
Archives of Clinical and Medical Microbiology(ACMMJ)
ISSN: 2835-9968 | DOI: 10.33140/ACMMJ
Impact Factor: 1.0

Research Article - (2024) Volume 3, Issue 3
Prevalence of Onychomycosis among Diabetic Population of District Doda (UT of J&K, India) -a Five Year Survey
2Department of Botany, University of Jammu, Jammu, 180006, India
3Medical Officer, Sub-District Hospital, Bhadarwah, Doda, J&K HME Department, India
Received Date: Jun 01, 2024 / Accepted Date: Aug 03, 2024 / Published Date: Aug 03, 2024
Copyright: ©©2024 Sandeep Kotwal, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Kotwal, S., Sumbali, G., Chauhan, M. (2024). Prevalence of Onychomycosis among Diabetic Population of District Doda (UT of J&K, India) -a Five Year Survey. Archives Clin Med Microbiol, 3(3), 01-10.
Abstract
Onychomycosis, which is the chronic fungal infection of finger and toe nails, is too prevalent in persons suffering with diabetes mellitus. Diabetes generally make a person more prone to a number of diseases due to their weakened immune system. Diabetics are almost three times more likely to develop onychomycosis than non-diabetics. In our present study, out of the 370 detected diabetic patients (190 males and 180 females), a total of 45 cases were found to be positive for onychomycosis, which showed a prevalence percentage of 12.16%. 35 onychomycotic male patients with a prevalence percentage of 9.46% and 10 onychomycotic female patients with a prevalence percentage of 2.70% with different clinical symptoms viz., Distal lateral subungual onychomycosis (DLSO), Proximal subungual onychomycosis (PSO), White superficial onychomycosis (WSO) and Total dystrophic onychomycosis (TDO) were reported. A total of 5 dermatophytes, 12 non-dermatophytes (yeast-like fungi) and 28 non-dermatophytes (filamentous fungi) were isolated from the nails of detected diabetic patients. The study also indicates that diabetic males are 3.5 times more prone to onychomycosis than diabetic females. This high prevalence of onychomycosis in diabetics is attributed to a combination of host factors including impaired glycaemic index, ischaemia, neuropathy and local immune-suppression. Onychomycosis can be especially important for some specific occupational groups because of their regular contact with soil, dirt and dust. Such people of the society, which depend upon physical labour for earning, such as, the farmers, gardeners, sweepers, maidservants, labourers, miners, etc., may be more prone to dermatophytic and non-dermatophytic onychomycosis and if they are diabetic then situation will become more complicated for them. This study also found that among detected diabetic patients highest prevalence rate of onychomycosis was found in employees (35.6%), farmers (24.4%), house-wives (17.8%), business-men (11.1%) and labourers (11.1%). Onychomycosis is a significant predictor for the development of secondary infections and foot ulcers in diabetes. Since, diabetics have vascular and nerve impairment, any minor injury to feet including a nail fungal infection can lead to more serious complications. Diabetics may have increased difficulty in doing regular foot check-ups due to obesity or retinopathy or cataracts, which may contribute to higher risk of developing complications from onychomycosis. In addition, symptoms go away very slowly and may take a year or more for the entire replacement of the old and infected nail. The study also found a correlation between the increasing age, diabetes and onychomycosis.
Keywords
Diabetes Mellitus, Onychomycosis, Dermatophytes, Non-Dermatophytes
Introduction
Onychomycosis is the chronic fungal infection of finger and toe nails, which may be caused by dermatophytes or non-dermatophytes including filamentous and yeast-like fungi. It is known to be associated with physical and psychological morbidity that affects the quality of life in a significant proportion of the world population. Onychomycosis occurs worldwide and affects approximately 5% of the population globally [1]. It appears to be a variable entity present in different forms in different parts of the world with every country and every region of a country having its own characteristic presentation [2]. Onychomycosis is among the most common nail disorders in adults, accounting for 15-40% of all nail diseases [3]. According to Richardson and Warnock (2012), approximately 20% of the population aged over 60 years, and up to 50% of subjects aged over 70 years have onychomycosis [4].
Onychomycosis can cause permanent damage to nails and may lead to other serious infections if the immune system is suppressed. Many risk factors are responsible for onychomycosis and some of them have been identified as diabetes, immune-compromised patients, avid sports participants, genetic defects and recently the COVID-19 SARS-CoV-2 infection [5-10]. As the population ages, there are corresponding chronic health problems that emerge, such as, diabetes, hypertension, thyroid and poor peripheral circulation. The risk is most serious for people with diabetes as they have vascular and nerve impairment and thus any minor injury to feet including a nail fungal infection can lead to more serious complications. In addition, symptoms go away very slowly and may take a year or more for the entire replacement of the old infected nail. Onychomycosis can also be important for some specific occupational groups of people because of their regular contact with soil, dirt and dust [11]. Such diabetic people of the society, which depend upon physical labour for earning, such as, the farmers, gardeners, sweepers, maidservants, labourers, miners, etc., may be more prone to dermatophytic and non-dermatophytic onychomycosis.
Diabetics are almost three times more likely to develop onychomycosis than non-diabetics [12]. High prevalence of onychomycosis among the diabetics is attributed to a combination of host factors including impaired glycaemic index, ischaemia, neuropathy and local immune-suppression. Onychomycosis is a significant predictor for the development of foot ulcers in diabetes [5]. Diabetics may have increased difficulty in doing regular foot check-ups due to obesity or retinopathy or cataracts, which may contribute to higher risk of developing complications from onychomycosis. Usually diseased nails have thick sharp edges, which can injure the surrounding skin tissue and result in pressure erosion of the nail bed. Such injuries usually may go unnoticed in diabetics due to sensory neuropathy [3]. The injury may act as an entry point for bacteria, fungi or other pathogens, leading to limb-threatening complications or even possible amputation of the lower extremities [3]. Approximately, 34% of all diabetics have fungal nail infections, as they show many of the risk factors that are associated with the increased prevalence of this disease [13]. Reports show that the most common causative agent for tinea pedis and onychomycosis in diabetic patients is Trichophyton rubrum, followed by T. mentagrophytes and then by other onychomycotic fungi [14,15].
Survey of literature shows few reports of isolated cases of onychomycosis from UT of Jammu and Kashmir [16,17]. So far, district wise survey for onychomycosis has been done only for Jammu and Rajouri [18-20]. In view of this, work was undertaken to study the prevalence of onychomycosis among diabetes mellitus population of District Doda, which is in the eastern part of Jammu province. District Doda lies within the middle and outer Himalayan ranges at 32° 53´ and 34° 21´N latitude and 75° 1´ and 76° 47´E longitude at an average elevation of 1107 meters (3631 feet) asl with temperature variation of -7oC to 37oC. The total area of district Doda is 2,985 Km2 and its population according to 2011 census is 4,09,936, out of which, 2,13,641 are males and 1,96,295 are females (http://doda.gov.in). Administratively, District Doda has been divided into 4 tehsils (Doda, Bhaderwah, Gandoh and Thatri) and 8 blocks viz., Doda, Bhaderwah, Gandoh, Thatri, Marmat, Bhagwah, Assar and Gundna (http://censusindia.gov.in).
Materials and Methods
During the five year survey period (2018-2022), samples of dystrophied fingernails and toenails were collected from the confirmed diabetic patients residing in District Doda of Union Territory of Jammu & Kashmir (India). Their fasting blood sugar level was estimated with the help of a Standard Digital Automatic Glucometer (blood glucose monitor) to confirm their sugar level in the blood. A detailed data sheet of each patient specifying history of occupation, personal habits, duration of infection, predisposing factors, different clinical patterns of onychomycosis, etc were recorded. All procedures performed in this study which involved human participants were in accordance with the ethical standards of the Institutional Ethical Committee. The standard procedure was applied for collecting the nail scrapings and nail clippings [21]. The dystrophied nail was first cleaned with 70% ethanol and a part of it was collected with a surgical blade in sterilized polythene bags. Direct microscopic observations were conducted by placing them in 2-3 drops of 20% potassium hydroxide (KOH) prepared in 36% dimethyl sulfoxide (DMSO) to detect any fungal hypha or spore. The samples irrespective of the negative or positive direct microscopic examination were then kept on dermatophyte test medium (DTM) and Sabouraud dextrose agar (SDA) medium supplemented with Chloramphenicol (0.040 g/L) and Cycloheximide (0.500 g/L) and incubated at 28±2oC for 7-14days. If the same fungus was isolated in culture on more than two consecutive occasions then it was taken as the criterion to consider the fungus as a probable pathogen. On the basis of the colouration, colony morphology, growth rate and lactophenol cotton bluemounts, the pathogens were identified mycologically by following the relevant literature. Identity of some of the fungal species was confirmed from National Fungal Culture Collection of India (NFCCI), Agharkar Research Institute (ARI), Pune, India.
Results and Discussion
During the period of survey, 370 diabetic patients from all the four tehsils of district Doda were scanned for the prevalence of onychomycosis. Of these, total of 45 individuals were found to be suffering with onychomycotic nails, thus showing a prevalence percentage of 12.16%. Data obtained during the survey were processed and statistically analysed using IBM SPSS version 24 under the platform of Microsoft windows XP. The different performance tests were compared using the Pearson chi-square test. P value less than 0.05 (P< 0.05) was considered statistically significant. Further, as shown in table 1, among the 45 diabetics showing onychomycosis, 35 were males and 10 were females. This shows that diabetic males of District Doda were more prone to onychomycosis (9.46%) than the diabetic females (2.70%) with a ratio of 3.5:1. Earlier, few other researchers have also reported diabetic males to be 2.5 to 3 times more prone to onychomycosis than the diabetic females, whereas others have found no significant difference in gender distribution among diabetic patients suffering from onychomycosis [22-25].
In the present study, more prevalence of onychomycosis among the diabetic males than the diabetic females is attributed to the fact that males are generally more engaged in outdoor physical activities like farming, sporting, social life, etc and hence their nails are more exposed to trauma and invasion by the invading fungi. In addition, they wear shoes for long hours, which create warm and humid conditions around the feet, thus making them more susceptible to the growth of fungal species causing onychomycosis. Many other researchers have also reported male onychomycosis to be more prevalent than female onychomycosis [23,26]. As depicted in Plate 1 & 2, both the toe and finger nails of the diabetic patients from Doda District were observed to be dystrophied due to fungal pathogenesis and they showed different patterns of onychomycosis like Distal lateral subungual onychomycosis (DLSO), Proximal subungual onychomycosis (PSO), White superficial onychomycosis (WSO) and Total dystrophic onychomycosis (TDO). Among the observed 45 diabetic patients, 90 finger and toe nails were onychomycotic, which included 56 onychomycotic toenails samples (6.2%) and 34 onychomycotic fingernails (3.8%) (Table 2). High incidence of toenail onychomycosis in diabetic patients has been reported earlier also by Manzano-Gayosso et al. and Leelavathi et al. [27,28]. During the present investigation, big toenails of the diabetics were more affected by fungal infection than other toenails (Table 2). This may be due to occlusive footwear pressure, defective blood circulation, peripheral vascular disease and neuropathy. In addition, use of public facilities like bathing ghats, swimming pools, community halls and also visiting the places of worship bare footed increase the risk of nail injuries, trauma and thus onset of onychomycosis [29]. Infact, such injuries usually go unnoticed in diabetics due to sensory neuropathy and may act as important sites for entry of fungal pathogens that cause onychomycosis [30,31]. The risk factors of preponderance of onychomycosis in diabetic patients are its duration, occupation, maturing age, subclinical atherosclerosis, obesity, triglyceride levels, metabolic syndrome and glycosylated haemoglobin [15].

Plate 1: Clinical Representation of Onychomycotic toe Nails of Diabetic Patients

Plate 2: Clinical Representation of Onychomycotic toe Nails of Diabetic Patients
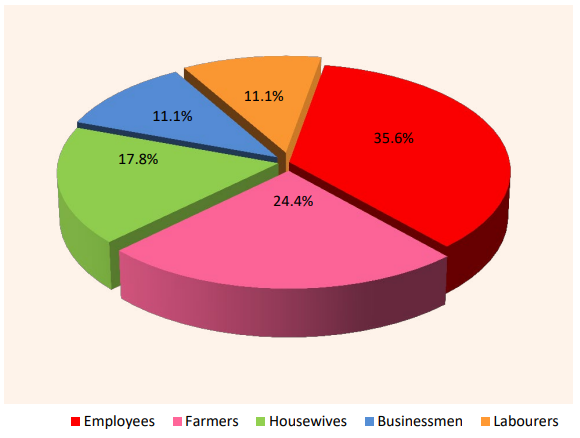
Figure 1: Prevalence (%) of Onychomycosis Among Diabetics with Different Occupational Groups
As depicted in table 2, out of the 45 diabetic patients with onychomycosis, 16 were employees, 11 were farmers, 8 were housewives and 5 each were businessmen and labourers. Therefore, highest prevalence rate of onychomycosis (35.6%) was detected among the diabetic employees (Figure 1). This study suggests that diabetic employees are at high risk of onychomycosis due to their continuous sitting for long hours, no exercises and wearing shoes for the whole day, which increases the disorders in their soles, toes, nails and provides condition that induces pressure necrosis of skin, thus increasing the chances of fungal infection. In our study, diabetic farmers and housewives formed the next onychomycotic risk groups with 24.4% and 17.8% prevalence respectively. This was probably due to their repeated contact of the finger nails and toe nails with water and soil, which influences the growth of nail infecting fungi. In our investigation, the diabetic businessmen and labourers were at minimum risk of onychomycosis, each showing 11.1% prevalence (Figure 1).
As shown in table 2 and depicted in figure 2, a total of 5 dermatophytic fungal species were isolated from the infected nails of diabetic patients, thus showing a prevalence percentage of 11.1%. Among the non-dermatophytes, 12 yeast-like fungal species and 28 filamentous fungal species were isolated from the dystrophied nails of diabetic patients, thus showing a prevalence rate of 26.7% and 62.2% respectively. This indicates that non-dermatophytes, which are keratinophilic soil-borne opportunist fungal species invade the nails of a person whose body immune system is compromised, become pathogenic and cause dystrophies by invading fresh keratinized tissues of the nail [11,32-35]. During the present investigation, it was also observed that the diabetic patients having onychomycosis were above the age of 33 years (Table2). Further, a correlation between the increasing age of diabetic patients and onychomycosis was observed. Perusal of data given in table 2 shows that within the age group (31-45 years), only 13 cases of diabetic patients with onychomycosis were detected, whereas in the age group (46-60 years), 15 cases were found and above 60 years, 17 cases were detected. Earlier, Gupta et al. and Leelavathi et al. also reported that the incidence of onychomycosis is more frequent among diabetic elders [13,28]. In fact, diabetes mellitus is considered as one of the major predisposing factors for onychomycosis [36]. According to Gupta et al., diabetic patients are three times more prone to onychomycosis than non-diabetic patients [13]. Moreover, due to obesity, retinopathy, cataracts and sensory neuropathy, they have lots of difficulty in going for regular foot check-ups [3]. Further, if onychomycosis is left untreated for longer period in these patients, their toenails can become thick with sharp edges, which may cause pressure and irritation of the surrounding skin tissue and thus result in erosion of the nail bed [3]. This injury may act as an entry point for other harmful microbial pathogens, thus making these patients more likely to develop limb cellulitis, foot ulceration and even amputation of the lower extremities [31,37,38].
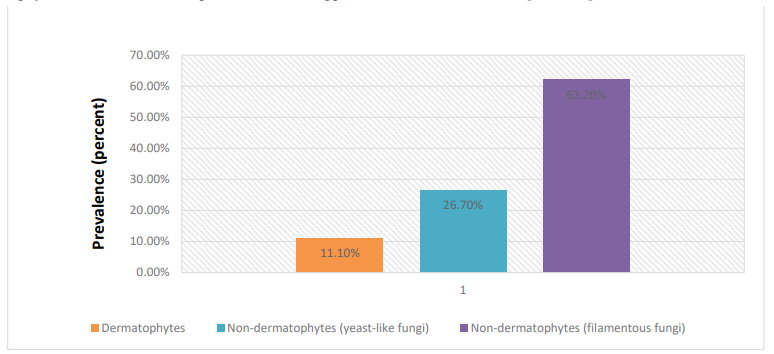
Figure 2:Prevalence (%) of onychomycotic Species Detected from Dystrophied Nails of Diabetic Patients
Currently, the world is facing COVID-19 pandemic since 2019 due to Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Diabetic patients suffering with onychomycosis can be more prone to COVID-19 and the response to medicines is also poor in these patients. Recently, Rakita et al. in their study also suggested that diabetic patient with onychomycosis is an indicator of more severe COVID-19 and poor out-comes [10]. In their experiment they found that the onychomycosis was a significant independent risk factor for COVID-19 severity, hospitalization and receiving supplementary oxygen therapy. Diabetes mellitus is always considered as a predisposing factor for a number of diseases viz., onychomycosis, skin diseases, mucormycosis, cardiovascular diseases, cataracts, etc [6,39,40-43].
|
Gender |
No. of diabetic patients scanned |
No. of diabetic patients with onychomycosis |
Prevalence (%) |
|
Males |
190 |
35 |
9.46% |
|
Females |
180 |
10 |
2.70% |
|
Total |
370 |
45 |
12.16% |
Table 1: Prevalence (%) of Onychomycosis among Diabetic Patients
|
Diabetic case with onychomycosis |
Gender |
Age (in years) |
Site of infection (nails infected) |
Occupation of patient |
Isolated fungal pathogen |
|
Case 1 |
M |
80 |
Left toenails (1,2,3) |
Employee |
Microsporum sp. |
|
Case 2 |
M |
45 |
Left toenail (1) |
Employee |
Microsporum sp. |
|
Case 3 |
M |
36 |
Left fingernail (1) |
Farmer |
Epidermophyton sp. |
|
Case 4 |
M |
45 |
Right fingernails (3,4) |
Businessman |
Aureobasidium sp. |
|
Case 5 |
M |
35 |
Left toenails (1,2,3) |
Farmer |
Aureobasidium sp. |
|
Case 6 |
M |
34 |
Left fingernail (1) |
Farmer |
Syncephalastrum sp. |
|
Case 7 |
F |
34 |
Left toenails (1,3,4) |
Housewife |
Sarocladium sp. |
|
Case 8 |
F |
68 |
Right fingernails (1,3) |
Housewife |
Acremonium sp. |
|
Case 9 |
M |
47 |
Left fingernails (2,3,4) |
Farmer |
Alternaria sp. |
|
Case 10 |
F |
42 |
Right fingernails (3,4) |
Housewife |
Cladosporium sp. |
|
Case 11 |
M |
53 |
Right fingernails (2,3,4,5) |
Employee |
Cladosporium sp. |
|
Case 12 |
M |
36 |
Left toenails (1,2) |
Farmer |
Nigrospora sp. |
|
Case 13 |
F |
62 |
Right fingernail (2) |
Housewife |
Curvularia sp. |
|
Case 14 |
M |
65 |
Right fingernail(1) |
Employee |
Penicillium sp. |
|
Case 15 |
M |
65 |
Right toenail (1,2) |
Employee |
Penicillium sp. |
|
Case 16 |
M |
82 |
Right toenails (1,2) & Left toenails (1,2) |
Employee |
Aspergillus sp. |
|
Case 17 |
M |
56 |
Right toenails (1,2) & Left toenails (1,4) |
Labourer |
Aspergillus sp. |
|
Case 18 |
M |
65 |
Left fingernail (4) |
Farmer |
Aspergillus sp. |
|
Case 19 |
M |
64 |
Right toenail (1) & Left toenail (1) |
Farmer |
Aspergillus sp. |
|
Case 20 |
M |
56 |
Right toenails (1,2,3,5) & Left toenails (1,2) |
Employee |
Aspergillus sp. |
|
Case 21 |
M |
70 |
Left toenails (1,2) |
Employee |
Candida sp. |
|
Case 22 |
M |
62 |
Left fingernails (2,3,4) |
Employee |
Candida sp. |
|
Case 23 |
M |
57 |
Right toenail (1) & Left toenail (1) |
Employee |
Candida sp. |
|
Case 24 |
M |
62 |
Right fingernail (4) |
Farmer |
Candida sp. |
|
Case 25 |
F |
57 |
Left fingernail (3) |
Employee |
Fusarium sp. |
|
Case 26 |
M |
66 |
Right fingernails (1,5) |
Employee |
Fusarium sp. |
|
Case 27 |
M |
64 |
Right toenail (1) & Left toenails (1,3) |
Businessman |
Fusarium sp. |
|
Case 28 |
M |
53 |
Right fingernail (1) |
Businessman |
Trichosporon sp. |
|
Case 29 |
M |
64 |
Left toenail (1) |
Farmer |
Paecilomyces sp. |
|
Case 30 |
M |
56 |
Right toenails (1,3,4) |
Labourer |
Aspergillus sp. |
|
Case 31 |
F |
37 |
Left fingernail (1) |
Housewife |
Aspergillus sp. |
|
Case 32 |
M |
56 |
Left toenail (1) |
Labourer |
Aspergillus sp. |
|
Case 33 |
F |
53 |
Right fingernail (1) & Left fingernail (1) |
Housewife |
Aspergillus sp. |
|
Case 34 |
M |
50 |
Left fingernail (1) |
Employee |
Microsporum sp. |
|
Case 35 |
F |
71 |
Right toenail (1) & Left toenail (1) |
Employee |
Epidermophyton sp. |
|
Case 36 |
M |
52 |
Right fingernail (4) |
Employee |
Trichosporon sp. |
|
Case 37 |
F |
64 |
Right toenail (1) & Left toenail (1,2) |
Housewife |
Trichosporon sp. |
|
Case 38 |
M |
46 |
Right toenail (1) & Left toenail (1) |
Labourer |
Paecilomyces sp. |
|
Case 39 |
M |
56 |
Right fingernail (3) |
Businessman |
Aspergillus sp. |
|
Case 40 |
M |
39 |
Right toenail (1) & Left toenail (1) |
Businessman |
Rhizopus sp. |
|
Case 41 |
M |
56 |
Right fingernail (1) & Left fingernail (1) |
Farmer |
Candida sp. |
|
Case 42 |
F |
36 |
Left toenail (1) |
Housewife |
Candida sp. |
|
Case 43 |
M |
62 |
Right toenails (1,2) |
Farmer |
Candida sp. |
|
Case 44 |
M |
38 |
Right toenail (1) |
Employee |
Penicillium sp. |
|
Case 45 |
M |
42 |
Right toenail (5) |
Labourer |
Penicillium sp. |
|
Total cases-45 |
M (males)=3 5 F (females)= 10 |
31-45y=13 cases 46-60y=15 cases 61-90y=17 cases |
Infected toenails-56 Infected fingernails-34 Total nails infected-90 |
Employees-16 Farmers-11 Housewives-8 Businessmen-5 Labourers -5 |
Dermatophytes= 05
Non-dermatophytes (yeast-like fungi) = 12 Non-dermatophytes (filamentous fungi)= 28 |
Table 2: Significant Details of Diabetic Cases Suffering with Onychomycosis
Conclusion
Among the 370 cases of detected diabetic patients from district Doda, 45 cases were found to be positive for onychomycosis also, thus showing a prevalence percentage of 12.16%. Of these, 35 onychomycotic males and 10 onychomycotic females were suffering with diabetes, thereby showing that diabetic males were more prone to onychomycosis (9.46%) than diabetic females (2.70%) with a prevalence ratio of 3.5:1. This may be due to the defective carbohydrate metabolism, testosterone hormone, more social activities of males, and more chances of trauma and low immunity, which are predisposing factors for onychomycosis. Both the toe and finger nails of the diabetic patients were observed to have fungal infection. A total of 90 onychomycotic nail samples of 45 diabetic patients were collected from this district. During the present investigation, big toenails of the diabetics were found to be more affected by fungal infection than other toenails. This may be due to occlusive footwear pressure, more surface area, defective blood circulation, peripheral vascular disease and neuropathy. In addition, the diabetic patients frequently use public facilities like bathing ghats, community halls and also visit places of worship bare footed, which increases the risk of nail injuries, trauma and thus onychomycosis. Such injuries usually go unnoticed in diabetics due to sensory neuropathy and may act as important sites for entry of fungal pathogens that cause onychomycosis. Among the 45 onychomycotic patients having diabetes, 16 were employees, 11 were farmers, 8 were housewives and 5 each were businessmen and labourers. This study suggests that diabetic employees are at higher risk of onychomycosis (35.6%) due to their continuous sitting for long hours, no exercises and wearing shoes for the whole day, which increases the disorders in their soles, toes, nails and provide conditions that induce pressure necrosis of skin, thus increasing the chances of fungal infection and thus they have to change their habits for the prevention of onychomycosis. In our study, diabetic farmers and housewives formed the next onychomycotic risk group with 24.4% and 17.8% prevalence respectively, whereas diabetic businessmen and labourers were detected with minimum onychomycosis, each showing least prevalence of 11.1%. This study also suggests that diabetic patients are always at higher risk for the invasion by onychomycotic fungi, so they should regularly visit the doctor to control their diabetes and they should regularly have their foot check-ups, which help them to lower down the risk of developing complications from onychomycosis viz., secondary infections, gangrene and even amputation of the lower extremities, if their body is invaded by any onychomycotic fungi. The clinicians should be extra observant in their diagnosis and its treatment because patients cannot be relied solely on discomfort or pain because of decreased sensation and neuropathy.
Author’s Contributions
First two authors were involved in designing the study, experimentation, data collection, data analysis, manuscript preparation, typing, reading and final approval. The third author help in the investigation of diabetic patients and onychomycosis. All the authors read and approved the final manuscript.
Acknowledgements
The authors are thankful to the HOD Botany, University of Jammu for providing laboratory facilities. The first author is also thankful to the University Grant Commission, New Delhi and JK Higher Education Department for providing an opportunity under UGC-FIP scheme for completing Ph.D.
Conflict of Interest
The authors have no conflicts of interests to declare.
References
- Murray, S. C., & Dawber, R. P. (2002). Onychomycosis of toenails: orthopaedic and podiatric considerations. Australasian journal of dermatology, 43(2), 105-112.
- Lungran, P., Mate, H., Pukhrambam, P. D., & Golmei, A.(2014). Prevalence and Etiological Agents of Onychomycosis.
- Ameen, M., Lear, J. T., Madan, V., Mohd Mustapa, M. F.,Richardson, M., Hughes, J. R., ... & Exton, L. S. (2014). British Association of Dermatologists' guidelines for the management of onychomycosis 2014. British Journal of Dermatology, 171(5), 937-958.
- Richardson, M. D., & Warnock, D. W. (2012). Fungal infection: diagnosis and management. John Wiley & Sons.
- Boyko, E. J., Ahroni, J. H., Cohen, V., Nelson, K. M., & Heagerty, P. J. (2006). Prediction of diabetic foot ulcer occurrence using commonly available clinical information: the Seattle Diabetic Foot Study. Diabetes care, 29(6), 1202-1207.
- Borba, O. S. A. M., Ogawa, M. M., Kirsztajn, G. M., & Tomimori, J. (2023). Onychomycosis in immunocompromised population: Phenotypic and molecular identification. Mycoses, 66(11), 1018-1024.
- Field, L. A., & Adams, B. B. (2008). Tinea pedis in athletes.International journal of dermatology, 47(5), 485-492.
- Odom, R. B. (1994). Common superficial fungal infections in immunosuppressed patients. Journal of the American Academy of Dermatology, 31(3), S56-S59.
- Gao, Y. D., Ding, M., Dong, X., Zhang, J. J., Kursat Azkur, A., Azkur, D., ... & Akdis, C. A. (2021). Risk factors for severe and critically ill COVID-19 patients: a review. Allergy, 76(2), 428-455.
- Rakita, U., Kaundinya, T., Guraya, A., Nelson, K., Maner, B., Manjunath, J., ... & Silverberg, J. I. (2021). Associations between onychomycosis and COVID-19 clinical outcomes: a retrospective cohort study from a US metropolitan center. Archives of dermatological research, 1-6.
- Kotwal, S., & Sumbali, G. (2016). Preferential utilization and colonization of keratin baits by different myco-keratinophiles. Springerplus, 5, 1-6.
- Al-Mutairi, N., Eassa, B. I., & Al-Rqobah, D. A. (2010). Clinical and mycologic characteristics of onychomycosis in diabetic patients. Acta Dermatovenerologica Croatica, 18(2), 0-0.
- Gupta, A. K., Konnikov, N., MacDonald, P., Rich, P., Rodger, N., Edmonds, M. W., ... & Summerbell, R. C. (1998). Prevalence and epidemiology of toenail onychomycosis in diabetic subjects: a multicentre survey. British Journal of Dermatology, 139(4), 665-671.
- Romano, C., Massai, L., Asta, F., & Signorini, A. M. (2001). Prevalence of dermatophytic skin and nail infections in diabetic patients. Mycoses, 44(3-4), 83-86.
- Ekeng, B. E., Kibone, W., Itam-Eyo, A. E., & Bongomin, F. (2023). Onychomycosis in patients with diabetes mellitus in Africa: a global scoping review, 2000–2021. Mycopathologia, 188(3), 173-182.
- Ahmad, M., Gupta, S., & Gupte, S. (2010). A clinico-mycological study of onychomycosis. Egypt Dermatol Online J, 6(4).
- Jandial, S., & Sumbali, G. (2012). Fusarial onychomycosis among gardeners: A report of two cases. Indian Journal of Dermatology, Venereology and Leprology, 78, 229.
- Bhou, R., & Sumbali, G. (2015). Fusarial onychomycosis-an unrecorded report from Jammu district (India). American International Journal of Research in Formal, Applied & Natural Sciences, 12, 21-26.
- Kanth, F., Wani, T., Manzoor, S., Shah, I., Bashir, G., Bali, N., & Mohiuidin, G. (2016). An epidemiological study of onychomycosis in Kashmir Valley. British Microbiology Research Journal, 15(1), 1-6.
- Sharma, A., & Sumbali, G. (2022). First Record of Aspergillus brunneus Causing Fingernail Aspergillomycosis in a Primary Schoolchild. Indian Journal of Paediatric Dermatology,23(2), 153-155.
- Gupta, A. K., Jain, H. C., Lynde, C. W., MacDonald, P., Cooper, E. A., & Summerbell, R. C. (2000). Prevalence and epidemiology of onychomycosis in patients visiting physicians’ offices: a multicenter Canadian survey of 15,000 patients. Journal of the American Academy of Dermatology, 43(2), 244-248.
- Chang, S. J., Hsu, S. C., Tien, K. J., Hsiao, J. Y., Lin, S. R.,Chen, H. C., & Hsieh, M. C. (2008). Metabolic syndrome associated with toenail onychomycosis in Taiwanese with diabetes mellitus. International journal of dermatology, 47(5), 467-472.
- Akkus, G., Evran, M., Gungor, D., Karakas, M., Sert, M., & Tetiker, T. (2016). Tinea pedis and onychomycosis frequency in diabetes mellitus patients and diabetic foot ulcers. A cross sectional–observational study. Pakistan journal of medical sciences, 32(4), 891.
- Kafaie, P., & Noorbala, M. T. (2010). Evaluation of onychomycosis among diabetic patients of Yazd diabetic center. Journal of Pakistan association of dermatologists, 20(4), 217-221.
- Gulcan, A., Gulcan, E., Oksuz, S., Sahin, I., & Kaya, D. (2011). Prevalence of toenail onychomycosis in patients with type 2 diabetes mellitus and evaluation of risk factors. Journal of the American Podiatric Medical Association, 101(1), 49-54.
- Hassab-El-Naby, H. M., Shaheen, I. M. I., Abdo, H. M., & El-Shafey, H. A. M. (2011). Comparative study for the reliability of potassium hydroxide mount versus nail clipping biopsy in diagnosis of onychomycosis. The Gulf Journal of Dermatology and Venereology, 18, 14-22.
- Manzano-Gayosso, P., Hernández-Hernández, F., Méndez-Tovar, L. J., Palacios-Morales, Y., Córdova-Martínez, E., Bazán-Mora, E., & López-Martinez, R. (2008). Onychomycosis incidence in type 2 diabetes mellitus patients. Mycopathologia, 166, 41-45.
- Leelavathi, M., Azimah, M. N., Kharuddin, N. F., & Tzar,M. N. (2013). Prevalence of toenail onychomycosis among diabetics at a primary care facility in Malaysia. Southeast Asian J Trop Med Public Health, 44(3), 479-483.
- Thomas, J., Jacobson, G. A., Narkowicz, C. K., Peterson, G. M., Burnet, H., & Sharpe, C. (2010). Toenail onychomycosis: an important global disease burden. Journal of clinical pharmacy and therapeutics, 35(5), 497-519.
- Brem, H., Sheehan, P., & Boulton, A. J. (2004). Protocol for treatment of diabetic foot ulcers. The American journal of surgery, 187(5), S1-S10.
- Winston, J. A., & Miller, J. L. (2006). Treatment of onychomycosis in diabetic patients. Clinical Diabetes, 24(4), 160-166.
- Kotwal, S., Sumbali, G., Sharma, S., & Kaul, S. (2018). Detection of some new Trichosporon species from the dystrophied nails of three female members of a family from North Indian State of Jammu and Kashmir. Mycoses, 61(8), 534-542.
- Kotwal, S., & Sumbali, G. Mycokeratinophiles: pathogens of onychomycosis. Kavaka. 2016b, 47, 83-94.
- Kotwal, S., Sumbali, G., & Jaglan, S. (2019). Documentation of yeast-like pathogens causing onychomycosis from Doda Region of Jammu and Kashmir (India). Kavaka, 53, 72-79.
- Higuchi, S., Noguchi, H., Matsumoto, T., Yaguchi, T., Kubo, M., Kashiwada-Nakamura, K., ... & Fukushima, S. (2023). Onychomycosis caused by Talaromyces muroii successfully treated with efinaconazole. Mycopathologia, 188(5), 825-827.
- Eba, M., Njunda, A. L., Mouliom, R. N., Kwenti, E. T., Fuh,A. N., Nchanji, G. T., & Atashili, J. (2016). Onychomycosis in diabetic patients in Fako Division of Cameroon: prevalence, causative agents, associated factors and antifungal sensitivity patterns. BMC research notes, 9, 1-8.
- Cathcart, S., Cantrell, W., & Elewski, B. E. (2009). Onychomycosis and diabetes. Journal of the European Academy of Dermatology and Venereology, 23(10), 1119-1122.
- Mayser, P., Freund, V., & Budihardja, D. (2009). Toenail onychomycosis in diabetic patients: issues and management.American journal of clinical dermatology, 10, 211-220.
- Abdi, A., Jalilian, M., Sarbarzeh, P. A., & Vlaisavljevic, Z. (2020). Diabetes and COVID-19: A systematic review on the current evidences. Diabetes research and clinical practice, 166, 108347.
- Shinkai, K., & Bruckner, A. L. (2020). Dermatology and COVID-19. Jama, 324(12), 1133-1134.
- Nassar, M., Daoud, A., Nso, N., Medina, L., Ghernautan, V., Bhangoo, H., ... & Misra, A. (2021). Diabetes mellitus and COVID-19. Diabetes & Metabolic Syndrome: Clinical Research & Reviews, 15(6), 102268.
- Cho, S. I., Kim, Y. E., & Jo, S. J. (2021). Association of COVID-19 with skin diseases and relevant biologics: a cross-sectional study using nationwide claim data in South Korea. British Journal of Dermatology, 184(2), 296-303.
- Lim, S., Bae, J. H., Kwon, H. S., & Nauck, M. A. (2021).COVID-19 and diabetes mellitus: from pathophysiology to clinical management. Nature Reviews Endocrinology, 17(1), 11-30.