
Archives of Clinical and Medical Microbiology(ACMMJ)
ISSN: 2835-9968 | DOI: 10.33140/ACMMJ
Impact Factor: 1.0

Research Article - (2025) Volume 4, Issue 2
Prevalence and Predictors of Post-Partum Depression in Pakistan
2Revival Aesthetics, Islamabad, Pakistan
Received Date: Apr 18, 2025 / Accepted Date: May 14, 2025 / Published Date: Jun 03, 2025
Copyright: ©Â©2025 Anina Qureshi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Qureshi, A., Ahmad, S., Ain, Q. U., Ahmed, A., Javed, D., et al. (2025). Prevalence and Predictors of Post-Partum Depression in Pakistan. Archives Clin Med Microbiol, 4(2), 01-13.
Abstract
Background Postpartum depression is a severe mental health condition that affects a significant portion of women globally, with higher rates observed in developing countries. PPD hampers a mother's and child’s health but regular screening and support can reduce the risk of PPD. However, research on the prevalence and risk factors of PPD has been scarce in Pakistan.
Aim To assess the prevalence and risk factors associated with postpartum depression (PPD) among new mothers in Rawalpindi and Islamabad.
Methods A descriptive cross-sectional study was conducted among new mothers of twin cities over a period of three months. Sample size was 382 participants were recruited through convenience sampling. The Edinburgh Postnatal Depression Scale (EPDS) was employed to assess depression severity. Data were analyzed using SPSS v 25.0.
Results The mean postnatal period of the study population was 6.32 ± 2.724 weeks. All participants exhibited some degree of postpartum depression, with 75% experiencing severe symptoms. The incidence of severe depression was higher among women aged 26-35 years, having normal body weight, with three or more children, no daughters, and those with no miscarriage history. Lastly, occupational status and geographical location (urban vs. rural) were not significantly associated with depression severity.
Conclusion and Future Implications Post-partum depression is highly prevalent among women in Pakistan. Therefore, there is an urgent need for targeted interventions and support systems for vulnerable groups, particularly women in the 26-35 age group with normal BMI. Moreover, PPD screening must be integrated into routine maternal healthcare services in Pakistan. resistant genes was observed, including TEM, CTX-M, SHV, and VEB types. The bacterial isolates (S. scuri ssp. lentus, S. gallinarum, S. eqourum, and S. xylulosus) demonstrated high antimicrobial resistance to commonly prescribed antibiotics, particularly gentamicin, erythromycin, sulfamethoxazole, and tetracycline.
Introduction
Females are approximately two times as likely as males to encounter depression at some point in their lifetimes, making depression a serious public health concern. Several depressive disorders are prevalent globally. These are long-lasting and remain the main cause of disability among women. Every year, almost 12 million women in the US suffer from clinical depression [1]. The estimated frequency of depression among women in low- and middle-income countries in Asia and Africa ranges from 15 to 28% [1].
Two major life milestones for a woman are becoming pregnant and giving birth. The burden of responsibilities increases after childbirth that leads to postpartum depression among women. It is a serious psychological condition which establishes after the childbirth [2]. Postpartum depression (PPD), a debilitating condition that strikes a month after childbirth, is marked by feelings of hopelessness, sadness, guilt, low self-esteem, exhaustion, emptiness, anhedonia, social withdrawal, low or no energy, feeling inadequate to care for the baby, becoming easily frustrated, difficulty speaking or writing, outbursts of rage towards others, increased anxiety, or panic attacks [3]. It is important to differentiate PPD from "maternity/ baby blues," which account for up to 80% of women's moderate and transient moodiness [4]. The strength and length of symptoms in PPD vary from baby blues as PPD can persist for up to a year [4].
The frequency of PPD in moms varies from 0.5% to 60.8% worldwide. Women in developing nations have greater rates of PPD than women in wealthy nations. According to a systematic review involving 28 industrialized nations, the prevalence of PPD symptoms (PPDS) among women in high-income countries, they were ranged from 6 to 13% [5]. About 20% of women in underdeveloped countries had postpartum common mental disorders [6]. Asian nations have shown a frequency of depression incidence which encompasses between 3.5-63.3% [7]. According to research carried out in rural Bangladesh, approximately 18% and 35% of rural women had PPD [8].
According to Gulamani, it is challenging to find out the PPD chronicity rate in Pakistan as women experiencing this condition underreport their symptoms due to social norms. The unavailability of PPD measuring scales in hospitals and birth centers further exacerbates the issue of missed diagnosis. In a study Rukh et al. claimed that Pakistan has the highest PPD prevalence rate among Asian nations ranging between 28% and 63% [9].
PPD is a multifactorial disorder with varying impacts on women based on age, educational level, race, and ethnicity. The following factors may contribute to preterm or low birth weight babies: unemployment, financial difficulties, lack of social or emotional support, housing issues, first-born child, stress associated with childcare, infant temperament, high parity, complications from obstetrics, sleep disorders, low self-esteem, negative attitude towards pregnancy, prenatal depression or anxiety, history of depression, poor marital relationship, history of domestic abuse, and significant negative life events in the year prior [10]. Moreover, studies show that postnatal depression is more common in younger women (20–29 years old) than in older women [10].
Postpartum depression creates an unfavorable atmosphere for the personal development of mothers and their newborn offspring. Untreated postpartum depression in mothers can lead to weight difficulties, substance misuse, domestic troubles, and nursing complications later in life [11]. According to research, recurrent bouts of depression result in high levels of chronic stress later in life. Furthermore, PPD negatively impacts family and social life [8]. PPD is a significant public health concern but research on the impact of various demographic and social parameters on postpartum depression has been limited. A study showed that the incidence of PPD has been underreported in Pakistan due to cultural and social stigma [12]. Therefore, this research aims to investigate the prevalence of PPD in Pakistan, as well as the impact of various demographic and social parameters on the severity of Postpartum depression.
Methodology
Study Design
A descriptive cross-sectional study was conducted to evaluate the incidence and prevalence of Postpartum Depression among women in the twin cities of Pakistan.
Sampling and Participants
The survey covered all gynae clinics and tertiary care facilities. The participants were recruited via convenience sampling. The study respondents were new mothers who were attending clinics and hospitals in Pakistan's twin cities, Rawalpindi and Islamabad.
Sample Size
The sample size was calculated using an online sample size calculator Raosoft®. The Sample size was calculated to be 382 mothers to achieve a 95% confidence level with a 5% margin of error. As no updated list of new mothers in twin cities is available, a convenient sampling technique was used. According to this technique, all the available respondents present at the time of data collection were included in the study.
Ethical Approval
The study received ethical approval from the Research and Ethics Committee of the Margalla Institute of Health Sciences. While permission from Pakistan's Ministry of Health is not required for questionnaire-based research, prior data was submitted to the Ministry for review. Additionally, authorization was obtained from the relevant authorities at the various healthcare institutions involved in data collection. Informed consent was secured from all respondents, and measures were implemented to ensure confidentiality of their information.
Data Collection
The data was gathered by self-administering the questionnaires to the mothers of diverse age groups and backgrounds at different hospitals/clinics.
Data Collection Tool
A pre-validated instrument, the Edinburgh Postnatal Depression Scale (EPDS), was slightly modified to align with the study's objectives and the socio-demographic context of the country. The EPDS was specifically designed to assist healthcare professionals in identifying mothers experiencing postpartum depression (PPD), a significant mental health condition that often extends beyond the transient symptoms commonly referred to as the "baby blues," which may occur within the first week postpartum. This scale provides a systematic approach to screening for PPD, facilitating timely intervention and support for affected individuals.
It is a pre-validated tool to evaluate Postpartum depression. There are ten brief points on the scale. A mother selects the response from four options that best reflects her feelings over the previous seven days. In under five minutes, most mothers are able to complete the scale.Responses to the Edinburgh Postnatal Depression Scale (EPDS) are rated on a scale from 0 to 3, reflecting the severity of each symptom. Items 3 and 5 through 10 are reverse scored, assigning values of 3, 2, 1, and 0, respectively. The overall score is obtained by summing the scores of all 10 items. Mothers with total scores exceeding 12 or 13 are considered at risk for postpartum depression and are encouraged to seek medical evaluation. A comprehensive clinical assessment by a qualified healthcare professional is essential for confirming a diagnosis and developing an appropriate treatment plan. The scale assesses the mother's emotional state over the past week, and it may be beneficial to administer the scale again after two weeks to monitor changes in her mental health status.
Reliability and Validity of the Tool
To validate the face and content of the instrument, two focus group discussions were conducted with clinical research specialists at different intervals. Additionally, pilot testing was performed on a subset comprising 10% of the data to assess the reliability of the tool following data collection.
Data Collection Procedures and Analysis
Data was collected by the principal investigator trained by the supervisor. The questionnaire was hand-delivered to the respondents and collected on the same day to avoid bias. After data collection, data was cleaned, coded, and entered in SPSS version 25. The normality of data was assessed through the Shapiro-Wilk test. Descriptive statistics comprising frequency and percentages were calculated. The association between variables was analyzed through chi-squared tests and analysis of variance (ANOVA).
Results
Demographics
Most participants were aged between 26-35 (47%) and had weights ranging between 56-65 (50%). A detailed overview of the demographic parameters of the study population is given in Table 1.
|
Demographic parameters |
n |
N % |
|
|
Age in years |
15-25 |
31 |
22.8% |
|
26-35 |
60 |
44.1% |
|
|
36-45 |
45 |
33.1% |
|
|
Weight in Kg |
45-55 |
23 |
16.9% |
|
56-65 |
69 |
50.7% |
|
|
66-75 |
37 |
27.2% |
|
|
Above 75 |
7 |
5.1% |
|
|
Number of Children Already Have |
0 |
9 |
6.6% |
|
1 |
47 |
34.6% |
|
|
2 |
37 |
27.2% |
|
|
3 or Above |
43 |
31.6% |
|
|
Number of Sons |
0 |
43 |
31.6% |
|
1 |
62 |
45.6% |
|
|
2 |
21 |
15.4% |
|
|
More than 2 |
10 |
7.4% |
|
|
No. of Daughters |
0 |
43 |
31.6% |
|
1 |
45 |
33.1% |
|
|
2 |
22 |
16.2% |
|
|
More than 2 |
.26 |
19.1% |
|
|
Body Mass Index |
18.0-20.9 |
29 |
21.3% |
|
21.0-23.9 |
62 |
45.6% |
|
|
24-25.9 |
37 |
27.2% |
|
|
Above 25.9 |
8 |
5.9% |
|
|
Number of Miscarriages |
0 |
71 |
52.2% |
|
1 |
37 |
27.2% |
|
|
2 |
12 |
8.8% |
|
|
|
More than 2 |
16 |
11.8% |
|
Area |
Urban |
107 |
78.7% |
|
Rural |
29 |
21.3% |
|
|
Occupation |
House-Wife |
92 |
67.6% |
|
Working-Woman |
41 |
30.1% |
|
|
Any Other |
3 |
2.2% |
Table 1: demographic parameters of study population
The mean postnatal period of study participants was 6.32 ± 2.724 weeks. The participants aged between 36-45 years and with more than two miscarriages had the longest mean postnatal period with mean days of (7.76 ± 1.59) and (7.58 ± 2.39), respectively. The detailed overview of mean postnatal weeks on which data was collected from different demographic groups is given in Table2.
|
Demographic Parameters |
Postnatal week |
||||||||||||
|
|
Mean |
S.D |
95% CI: (Lower bound- Upper Bound) |
Mean |
S.D |
95% CI: (Lower bound- Upper Bound) |
Mean |
S.D |
95% CI: (Lower bound- Upper Bound) |
||||
|
Age |
15-25 |
26-35 |
36-45 |
||||||||||
|
|
5.35 |
2.15 |
4.57-6.14 |
5.73 |
3.21 |
4.90- 6.56 |
7.76 |
1.59 |
7.28-8.24 |
||||
|
Weight in Kg |
45-55 |
56-65 |
66-75 |
||||||||||
|
6.04 |
2.07 |
5.15-6.94 |
6.51 |
2.57 |
5.89- 7.12 |
3.435 |
6.08 |
4.94-7.23 |
|||||
|
Number of Children |
0 |
1 |
2 |
||||||||||
|
4.67 |
2.23 |
2.95-6.39 |
6.04 |
3.41 |
5.04- 7.04 |
5.78 |
2.250 |
5.03-6.53 |
|||||
|
Number of Sons |
0 |
1 |
2 |
||||||||||
|
5.93 |
2.44 |
5.18-6.68 |
6.55 |
3.22 |
5.73- 7.37 |
6.43 |
1.81 |
5.61-7.25 |
|||||
|
No. of Daughters |
0 |
1 |
2 |
||||||||||
|
5.56 |
3.38 |
4.52-6.60 |
5.96 |
2.47 |
5.21- 6.70 |
6.59 |
1.92 |
5.74-7.44 |
|||||
|
Body Mass Index |
18.0-20.9 |
21.0-23.9 |
24-25.9 |
||||||||||
|
6.24 |
2.502 |
5.29-7.19 |
6.24 |
2.546 |
5.60- 6.89 |
6.41 |
3.27 |
5.32-7.50 |
|||||
|
Number of Miscarriages |
0 |
1 |
2 |
||||||||||
|
6.25 |
2.136 |
5.75-6.76 |
4.78 |
2.405 |
3.98- 5.59 |
7.58 |
2.392 |
6.06-9.10 |
|||||
|
Area |
Urban |
Rural |
|||||||||||
|
6.39 |
2.907 |
5.84-6.95 |
6.03 |
1.918 |
5.31-6.76 |
||||||||
|
Occupation |
Housewife |
Working Women |
Any Other |
||||||||||
|
6.57 |
2.44 |
6.06-7.07 |
5.7 |
3.30 |
4.69- 6.77 |
6.67 |
1.16 |
3.80-9.54 |
|||||
Table 2: Mean Postnatal Week of Study Participants During Data Collection
EPDS Depression Scores
All women enrolled in this study had some degree of PPD elaborated in the next sections. The mean EPDS depression score of participants was 14.26 ± 5.335. The mean EPDS score was higher for women aged between 26-35 as compared to those aged 36-45 and 15-25 (15.01 ± 5.29 vs 12.14 ± 6.36 and 14.74 ± 2.91). However, the difference was not significant. Similarly, no significant differences existed for total depression score between various demographic groups Table 3.
|
Demographic parameters |
EPDS total Score |
P-Value |
||||||||
|
Age |
Mean |
S.D |
95% CI: (Lower Bound- Upper Bound) |
Mean |
S.D |
95% CI: (Lower Bound- Upper Bound |
Mean |
S.D |
95% CI: (Lower Bound- Upper Bound) |
|
|
|
15-25 |
26-35 |
36-45 |
|
||||||
|
|
14.74 |
2.91 |
13.48- 16.00 |
15.01 |
5.29 |
13.74- 16.29 |
12.14 |
6.36 |
10.01- 14.26 |
0.544 |
|
Number of Children |
0 |
1 |
2 |
|
||||||
|
|
14.22 |
6.28 |
9.39-19.05 |
13.36 |
6.05 |
11.58- 15.14 |
14.30 |
5.80 |
12.36- 16.23 |
0.585 |
|
Number of Sons |
0 |
1 |
2 |
|
||||||
|
|
14.70 |
5.46 |
13.02- 16.38 |
13.42 |
5.62 |
11.99- 14.85 |
15.29 |
4.91 |
13.05- 17.52 |
0.998 |
|
No. of Daughters |
0 |
1 |
2 |
|
||||||
|
|
13.42 |
6.38 |
11.45- 15.38 |
13.76 |
5.52 |
12.10- 15.41 |
15.00 |
4.01 |
13.22- 16.78 |
0.998 |
|
Body Mass Index |
18.0-20.9 |
21.0-23.9 |
24-25.9 |
|
||||||
|
|
13.66 |
2.91 |
12.54- 14.77 |
15.21 |
5.46 |
13.82- 16.60 |
12.59 |
6.41 |
10.46- 14.73 |
0.465 |
|
Number of Miscarriages |
0 |
1 |
2 |
|
||||||
|
|
15.06 |
4.69 |
13.94- 16.17 |
12.03 |
6.86 |
9.74-14.31 |
15.50 |
3.23 |
13.45- 17.55 |
0.151 |
Table 3: The EPDS Score of Study Participants with Respect to Demographic Parameters
EPDS Depression Stage
Most of the study participants had severe depression 102 (75%) followed by short lived distress 20 (14.7%) and mild to moderate depression 14 (10.3%). There were significant differences in the depression stages based on age, weight, number of children, number of daughters, BMI and number of miscarriages (p<0.05). The incidence of severe depression was higher in women aged between 26-35 vs. 35-45 and 15-25 [43 (31.6%) vs. 37 (27.2%) and 12 (8.8%), p<0.05]. Similarly, severe depression was more prevalent among women having weight in the range of 55-65 kg as compared to 66-75 , 45-55kg and above 75kg [55 (40.4%) vs. 20 (14.7%), 20 (14.7%), and 7 (5.1%), p<0.05]. Women having more than three children had higher incidence of PPD as compared to women having one and two children or no children at all [34 (25%) vs. 33 (24.3%) and 28 (20.6%) or 7 (5.1%), p<0.05]. Additionally, women having one or no daughter had higher incidence of severe PPD as compared to those with more than two and two daughters [31 (22.8%) or 30 (22.1%) vs. 23 (16.9%) and 18 (13.2%), p<0.05]. Moreover, the incidence of severe depression was highest in women with BMI 21-23.9 followed by 24-25.9 and 18-20.9 while the least was observed in women with BMI above 25.9 [53 (39.0%) vs. 22 (16.2%) and 20 (14.7%), and 7 (5.1%), p<0.05]. Lastly, the incidence of severe PPD was higher in women with no miscarriages compared to those with one miscarriage, followed by more than two and two miscarriages [59 (43.4%) vs. 22 (16.2%) and 11 (8.1%), and 10 (7.4%), p<0.05]. There were no significant differences between depression stage among women of different occupation and area Table 4.
|
|
EPD |
EPDS depression stage |
Count |
n % |
X2 |
p-value |
|
Age in years |
15-25 |
Short-Lived Distress |
7 |
5.1% |
9.567 |
0.048 |
|
Mild to Moderate Depression |
2 |
1.5% |
||||
|
Severe Depression |
22 |
16.2% |
||||
|
26-35 |
Short-Lived Distress |
12 |
8.8% |
|||
|
Mild to Moderate Depression |
5 |
3.7% |
||||
|
Severe Depression |
43 |
31.6% |
||||
|
36-45 |
Short-Lived Distress |
1 |
0.7% |
|||
|
Mild to Moderate Depression |
7 |
5.1% |
||||
|
Severe Depression |
37 |
27.2% |
||||
|
Weight in Kg |
45-55 |
Short-Lived Distress |
2 |
1.5% |
14.412 |
0.025 |
|
Mild to Moderate Depression |
1 |
0.7% |
||||
|
Severe Depression |
20 |
14.7% |
||||
|
56-65 |
Short-Lived Distress |
7 |
5.1% |
|||
|
Mild to Moderate Depression |
7 |
5.1% |
||||
|
Severe Depression |
55 |
40.4% |
||||
|
66-75 |
Short-Lived Distress |
11 |
8.1% |
|||
|
Mild to Moderate Depression |
6 |
4.4% |
||||
|
Severe Depression |
20 |
14.7% |
||||
|
Above 75 |
Short-Lived Distress |
0 |
0.0% |
|||
|
Mild to Moderate Depression |
0 |
0.0% |
||||
|
Severe Depression |
7 |
5.1% |
||||
|
Number of Children Already Have |
0 |
Short-Lived Distress |
1 |
0.7% |
13.342 |
0.038 |
|
Mild to Moderate Depression |
1 |
0.7% |
||||
|
Severe Depression |
7 |
5.1% |
||||
|
1 |
Short-Lived Distress |
12 |
8.8% |
|||
|
Mild to Moderate Depression |
2 |
1.5% |
||||
|
Severe Depression |
33 |
24.3% |
||||
|
2 |
Short-Lived Distress |
6 |
4.4% |
|||
|
Mild to Moderate Depression |
3 |
2.2% |
||||
|
Severe Depression |
28 |
20.6% |
||||
|
3 or Above |
Short-Lived Distress |
1 |
0.7% |
|||
|
Mild to Moderate Depression |
8 |
5.9% |
||||
|
Severe Depression |
34 |
25.0% |
||||
|
Number of Sons |
0 |
Short-Lived Distress |
6 |
4.4% |
6.252 |
0.396 |
|
Mild to Moderate Depression |
2 |
1.5% |
||||
|
Severe Depression |
35 |
25.7% |
|
|
1 |
Short-Lived Distress |
12 |
8.8% |
|
|
|
Mild to Moderate Depression |
8 |
5.9% |
||||
|
Severe Depression |
42 |
30.9% |
||||
|
2 |
Short-Lived Distress |
2 |
1.5% |
|||
|
Mild to Moderate Depression |
2 |
1.5% |
||||
|
Severe Depression |
17 |
12.5% |
||||
|
More than 2 |
Short-Lived Distress |
0 |
0.0% |
|||
|
Mild to Moderate Depression |
2 |
1.5% |
||||
|
Severe Depression |
8 |
5.9% |
||||
|
No. of Daughters |
0 |
Short-Lived Distress |
11 |
8.1% |
11.206 |
0.082 |
|
Mild to Moderate Depression |
2 |
1.5% |
||||
|
Severe Depression |
30 |
22.1% |
||||
|
1 |
Short-Lived Distress |
7 |
5.1% |
|||
|
Mild to Moderate Depression |
7 |
5.1% |
||||
|
Severe Depression |
31 |
22.8% |
||||
|
2 |
Short-Lived Distress |
1 |
0.7% |
|||
|
Mild to Moderate Depression |
3 |
2.2% |
||||
|
Severe Depression |
18 |
13.2% |
||||
|
More than 2 |
Short-Lived Distress |
1 |
0.7% |
|||
|
Mild to Moderate Depression |
2 |
1.5% |
||||
|
Severe Depression |
23 |
16.9% |
||||
|
Body Mass Index |
18.0-20.9 |
Short-Lived Distress |
2 |
1.5% |
19.092 |
0.004 |
|
Mild to Moderate Depression |
7 |
5.1% |
||||
|
Severe Depression |
20 |
14.7% |
||||
|
21.0-23.9 |
Short-Lived Distress |
8 |
5.9% |
|||
|
Mild to Moderate Depression |
1 |
0.7% |
||||
|
Severe Depression |
53 |
39.0% |
||||
|
24-25.9 |
Short-Lived Distress |
10 |
7.4% |
|||
|
Mild to Moderate Depression |
5 |
3.7% |
||||
|
Severe Depression |
22 |
16.2% |
||||
|
Above 25.9 |
Short-Lived Distress |
0 |
0.0% |
|||
|
Mild to Moderate Depression |
1 |
0.7% |
||||
|
Severe Depression |
7 |
5.1% |
||||
|
Number of Miscarriages |
0 |
Short-Lived Distress |
8 |
5.9% |
16.141 |
0.013 |
|
Mild to Moderate Depression |
4 |
2.9% |
||||
|
Severe Depression |
59 |
43.4% |
||||
|
|
1 |
Short-Lived Distress |
11 |
8.1% |
|
|
|
Mild to Moderate Depression |
4 |
2.9% |
|
|
|
Severe Depression |
22 |
16.2% |
||||
|
2 |
Short-Lived Distress |
0 |
0.0% |
|||
|
Mild to Moderate Depression |
2 |
1.5% |
||||
|
"Severe Depression" |
10 |
7.4% |
||||
|
More than 2 |
Short-Lived Distress |
1 |
0.7% |
|||
|
Mild to Moderate Depression |
4 |
2.9% |
||||
|
Severe Depression |
11 |
8.1% |
||||
|
Area |
Urban |
Short-Lived Distress |
18 |
13.2% |
4.262 |
0.119 |
|
Mild to Moderate Depression |
13 |
9.6% |
||||
|
Severe Depression |
76 |
55.9% |
||||
|
Rural |
Short-Lived Distress |
2 |
1.5% |
|||
|
Mild to Moderate Depression |
1 |
0.7% |
||||
|
Severe Depression |
26 |
19.1% |
||||
|
Occupation |
House-Wife |
Short-Lived Distress |
10 |
7.4% |
6.493 |
0.165 |
|
Mild to Moderate Depression |
12 |
8.8% |
||||
|
Severe Depression |
70 |
51.5% |
||||
|
Working- Woman |
Short-Lived Distress |
10 |
7.4% |
|||
|
Mild to Moderate Depression |
2 |
1.5% |
||||
|
Severe Depression |
29 |
21.3% |
||||
|
Any Other |
Short-Lived Distress |
0 |
0.0% |
|||
|
Mild to Moderate Depression |
0 |
0.0% |
||||
|
Severe Depression |
3 |
2.2% |
Table 4 : EPDS Depression Stage of Study Participants with Respect to Demographic Parameters
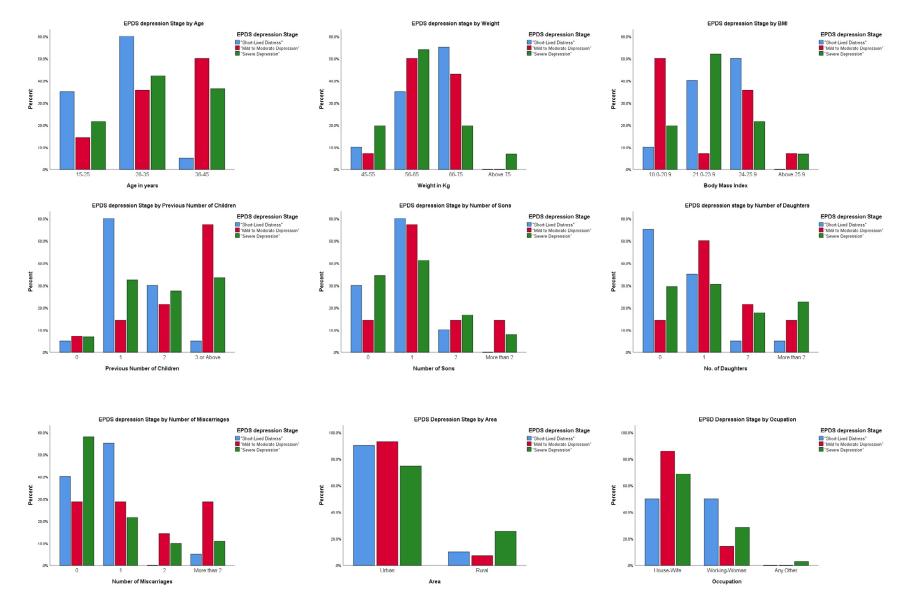
Figure 1 : Association of Post-Partum Depression with Demographic Parameters
Association between EPDS total score and Postnatal week
A statistically significant relationship existed between postnatal week of women and EPDS total score where EPDS total score increased by 0.382 points with each passing postnatal week (p = 0.023). Based on the identified prevalence of depression stage among various demographic groups a risk stratification tool has been created and is given in Table 5.
|
Demographic Factor |
Low Risk |
Moderate Risk |
Severe Risk |
|
Age (Years) |
36-45 |
15-25 |
26-35 |
|
Weight (Kg) |
Above 75 |
45-55, 66-75 |
56-65 |
|
Number of Children |
0 Children |
1 Child, 2 Children |
3 or More Children |
|
Number of Sons |
More than 2 |
0 Sons |
1 Son |
|
Number of Daughters |
More than 2 |
0 Daughters, 1 Daughter |
2 Daughters |
|
Body Mass Index (BMI) |
Above 25.9 |
18.0-20.9, 24-25.9 |
21.0-23.9 |
|
Number of Miscarriages |
More than 2 |
1 Miscarriage |
0 Miscarriages |
|
Area |
Rural |
Urban |
- |
|
Occupation |
Any Other |
Working Women |
Housewife |
Table 5 : Risk Stratification for Post-Partum Depression Based on Demographic Factors
Discussion
This study investigated the impact of demographic factors on postpartum depression among women of Rawalpindi and Islamabad. All of the women were at some stage of post-partum depression. The results indicated that demographic factors had a significant association with the depression stage. For instance, the incidence of severe depression was higher among women aged 26- 35 years of age, 56-65 kg weight, having three or more children, with one or no daughters, and BMI 21-23.9. Additionally, there was no significant association between occupation, geographic location (urban vs. rural), and the stage of depression. These findings led to the creation of a risk stratification tool to predict highly vulnerable groups more likely to have postpartum depression symptoms and should be counseled in both pre natal and post natal periods.
The Edinburgh Postnatal Depression Scale (EPDS) is a widely recognized screening tool used to assess the severity of depressive symptoms in postpartum women. In this study, a high percentage of participants experienced severe depression, which aligns with previous research suggesting that rates of postpartum depression vary significantly between locations but often remain alarmingly high [11,13,14]. It is a significant public health concern as PPD not only affects the well-being of mothers but also has profound implications for child development and family dynamics [15]. Research indicates that untreated PPD can lead to negative outcomes for children, including emotional and behavioral problems, as well as disruptions in mother-child bonding [16,17].
The higher incidence of post-partum depression among women aged 26-35 may be attributed to higher societal challenges among this group. The mental health challenges are exacerbated in this group due to societal pressure to excel in both career and managing family responsibilities alongside the physical demands of childbirth [18]. Additionally, women in this age range are often at a peak period for establishing long-term personal and professional identities which leads to increased vulnerability to emotional distress when these expectations clash with the realities of motherhood [19]. Further, studies suggest that younger women, particularly those under 25, may have stronger social support networks, either from family or peers, which can mitigate the risk of PPD [20]. On the other hand, older women (above 35) might benefit from greater emotional maturity and potentially fewer societal pressures regarding childbearing [21]. Therefore, psychosocial pressure makes women 26-35 years a vulnerable age group for experiencing severe postpartum depression symptoms.
The women with normal body weight and BMI experienced a higher incidence of post-partum depression which aligns with the findings of various studies [22-24]. However, studies conducted in America suggest the reverse relationship between postpartum depression and BMI with obese women having a higher likelihood of severe depression [25-27]. This may be attributed to geographical and cultural differences between western and eastern regions. In a study by Silverman et al., the higher post-partum anxiety and depression levels among women of normal BMI were attributed to increased body dissatisfaction and higher pressures to regain pre pregnancy weight [23]. A few meta-analyses showed that women on a lower spectrum of normal weight had lower self-esteem and higher anxiety about conforming to societal standards of body image [28,29]. Therefore, body negativity can be directly linked to a higher incidence of PPD and vice versa. However, social support can mediate the effect of BMI. According to a study by Cho et al., women who reported strong support systems during the postpartum period experienced less severe depressive symptoms, regardless of their BMI [30]. Thus, women having a normal BMI before pregnancy are likely to experience severe depression due to body image issues, but they can be mediated by enhanced social support.
Research indicates that the risk of severe postpartum depression increases with the number of children a mother has. A study conducted across different nations suggested that women with multiple children are more likely to experience severe depressive symptoms postpartum due to the cumulative stress associated with caring for several children [31]. The demands of parenting can lead to feelings of being overwhelmed, particularly if support systems are lacking [13]. A study by Segre et al. found that mothers with larger families reported higher levels of stress and depression, attributing this to time constraints and the difficulty of providing individualized care to each child [32]. Further, mothers with several children may find it challenging to engage socially, leading to reduced opportunities for emotional support, which is vital for mental health [30].
The relationship between the gender of children and the incidence of postpartum depression (PPD) is a complex issue influenced by cultural, societal, and psychological factors. In the context of South Asian societies, including the twin cities of Pakistan, distinct gender norms and societal expectations can significantly impact maternal mental health. This phenomenon may be linked to various factors, including societal expectations surrounding gender roles and the perceived value of daughters versus sons. Research by Bhat and Zavier (2003) suggests that the cultural preference for sons can lead to feelings of inadequacy and depression in mothers who do not meet this expectation [33]. However, our study provided contradictory results with a higher incidence of PPD among women having one or no daughter. This finding suggests that gender roles and societal expectations might be shifting in the recent era.
Moreover, the results of this study suggested that women with no history of miscarriage had a higher incidence of experiencing severe depression. Several studies highlight that women who have had successful births after miscarriages often experience a reduction in anxiety and depressive symptoms, indicating a positive psychological shift [34,35]. Another study by supports this notion, suggesting that first-time mothers may face intense pressure to succeed in their new roles, leading to increased anxiety and depressive symptoms [36]. However, another recent study suggested that women undergone miscarriages can experience chronic grief, which can exacerbate the risk of developing PPD after a subsequent birth [37]. The relationship between pregnancy loss and subsequent mental health can vary between different regions with higher chances of women having no miscarriage to experience severe PPD.
The absence of significant differences in PPD rates among housewives, working women, and others suggests that occupational status may not be a primary determinant of postpartum mental health. This aligns with another research conducted in Pakistan by Ramji et al., which found that factors beyond occupation such as individual coping mechanisms, social support, and personal circumstances play a more critical role in determining the risk of PPD [38]. Similarly, the absence of significant differences in PPD rates between urban and rural women suggests that both groups may face similar mental health challenges postpartum. This finding aligns with the findings of Aliani and Khuwaja, which indicated that while geographical location may influence certain aspects of maternal health, the psychological impacts of childbirth can transcend these boundaries [39].
Access to healthcare in both regions can also significantly affect levels of PPD. For instance, urban areas typically offer greater access to healthcare resources, however, this advantage does not necessarily translate into lower rates of PPD. Urban women may have access to a wider range of mental health services, but they may also encounter higher levels of stress related to living in densely populated environments, such as increased financial burdens or lack of social support [40]. Conversely, rural women might experience limited access to specialized care but benefit from close-knit communities and social networks that provide emotional support [40]. These variations in social support systems between urban and rural areas make PPD incidence less differentiated based on geographical location.
PPD poses significant public health challenges, affecting not only mothers but also child development, family dynamics, and healthcare systems. Therefore, early detection should be ensured through screening tools like the EPDS during prenatal and postnatal visits for timely intervention. These interventions should focus on enhancing social support and access to mental health resources for mothers in both urban and rural areas. The American College of Obstetricians and Gynecologists (ACOG) recommends routine screening for perinatal depression at least once during the perinatal period, particularly for high-risk groups, including mothers of multiple children [41]. Further, comprehensive support systems including community-based programs for screening and counseling should be initiated for new mothers. Moreover, community education programs that promote awareness of gender equality, and address societal norms can significantly improve maternal mental health. A research study suggested that community-based interventions focusing on gender sensitization and mental health support can help alleviate the stigma associated with having daughters and reduce the incidence of postpartum depression [42].
This study was conducted only in Rawalpindi and Islamabad, and it does not apply to the whole Pakistani population. Therefore similar studies should be conducted across other regions of Pakistan. However, it provides a comprehensive overview of risk factors for postpartum depression. Future research should analyze the relationship between social support, body image concerns, and PPD severity among women with normal BMI. Moreover, there is a need for longitudinal studies to explore the role of healthcare providers in identifying and addressing PPD, including barriers to care and potential solutions.
Conclusion
The prevalence of PPD remains high with 100% of participants experiencing some degree of depression. Further, demographic factors have a significant impact on the severity of postpartum depression (PPD) among women in Rawalpindi and Islamabad, Pakistan. The incidence of severe depression remains high concerning age (26-35 years), normal body weight (BMI 21- 23.9), having three or more children, and having one or no daughters. Contrary to expectations, occupation and geographical location (urban vs. rural) did not significantly impact PPD severity. A complex interplay exists between cultural, societal, and psychological factors influencing maternal mental health in Pakistan. There is an urgent need for targeted interventions and support systems for vulnerable groups, particularly women aged 26-35 with normal BMI. Lastly, future research should explore the relationships between societal norms or cultural beliefs and PPD.
References
- Zeleke, T. A., Getinet, W., Tadesse Tessema, Z., & Gebeyehu,K. (2021). Prevalence and associated factors of post-partum depression in Ethiopia. A systematic review and meta- analysis. PloS one, 16(2), e0247005.
- Slomian, J., Honvo, G., Emonts, P., Reginster, J. Y., & Bruyère, O. (2019). Consequences of maternal postpartum depression: A systematic review of maternal and infant outcomes. Women's health, 15, 1745506519844044.
- Stewart, D. E., & Vigod, S. (2016). Postpartumdepression.375(22), 2177-2186.
- Tarar, A., Ijaz, M., Tarar, M., & Batool, M. (2021). Postpartum depression: Assessment of cultural risk factors. Pakistan Armed Forces Medical Journal, 71.
- Shakeel, N., Sletner, L., Falk, R. S., Slinning, K., Martinsen, E. W., Jenum, A. K., & Eberhard-Gran, M. (2018). Prevalence of postpartum depressive symptoms in a multiethnic population and the role of ethnicity and integration. Journal of Affective Disorders, 241, 49-58.
- Bener, A., Gerber, L. M., & Sheikh, J. (2012). Prevalence of psychiatric disorders and associated risk factors in women during their postpartum period: a major public health problem and global comparison. International journal of women's health, 191-200.
- Peng, L., Zhang, J., Li, N., Jin, Y., & Zheng, Z. J. (2023). Depressive symptoms occurring after stroke by age, sex and socioeconomic status in six population-based studies: Longitudinal analyses and meta-analyses. Asian Journal of Psychiatry, 79, 103397.
- Rashidul Azad, R. A., Rukhshan Fahmi, R. F., Shrestha, S.Joshi, H., Mehedi Hasan, M. H., Khan, A. N. S., ... & Billah,S. M. (2019). Prevalence and risk factors of postpartum depression within one year after birth in urban slums of Dhaka, Bangladesh.
- Gulamani, S. S., Shaikh, K., & Chagani, J. (2013). Postpartum depression in Pakistan. Nursing for women's health, 17(2), 147-152.
- Mokwena, K., & Masike, I. (2020). The need for universal screening for postnatal depression in South Africa: Confirmation from a sub-district in Pretoria, South Africa. International journal of environmental research and public health, 17(19), 6980.
- Yadav, T., Shams, R., Khan, A. F., Azam, H., Anwar, M., Anwar, T., ... & Sukaina, M. (2020). Postpartum depression: prevalence and associated risk factors among women in Sindh, Pakistan. Cureus, 12(12).
- Adil, A., Shahbaz, R., Ameer, S., & Usama, M. (2021). Influence of parental competence on postpartum depression mediated via negative thoughts: Moderating role of type of delivery. Women & Health, 61(6), 591-598.
- O'hara, M. W., & Swain, A. M. (1996). Rates and risk of postpartum depression—a meta-analysis. International review of psychiatry, 8(1), 37-54.
- Shorey, S., Chee, C. Y. I., Ng, E. D., Chan, Y. H., San Tam,W. W., & Chong, Y. S. (2018). Prevalence and incidence of postpartum depression among healthy mothers: A systematic review and meta-analysis. Journal of psychiatric research, 104, 235-248.
- González, G., Moraes, M., Sosa, C., Umpierrez, E., Duarte, M., Cal, J., & Ghione, A. (2017). Maternal postnatal depression and its impact on child neurodevelopment: a cohort study. Rev. Chil. Pediatr, 88(3), 360-366.
- Opie, R. S., Zheng, M., Torres, S., & Campbell, K. (2021). The impact of maternal post-partum depressive symptoms on child diet at 18 months. Maternal & Child Nutrition, 17(4), e13187.
- Eitenmüller, P., Köhler, S., Hirsch, O., & Christiansen,H. (2022). The impact of prepartum depression and birth experience on postpartum mother-infant bonding: A longitudinal path analysis. Frontiers in Psychiatry, 13, 815822.
- Muraca, G. M., & Joseph, K. S. (2014). The association between maternal age and depression. Journal of obstetrics and gynaecology Canada, 36(9), 803-810.
- Meczkowska-Christiansen, A., Królikowska, I. J. M. P. I. (2023). Perspectives. The Role of Discursive Contexts in Constructing the Identity of Women at Sea: Towards Informal Dimensions of Maritime Adult Education,2:93.
- Pao, C., Guintivano, J., Santos, H., & Meltzer-Brody, S. (2019). Postpartum depression and social support in a racially and ethnically diverse population of women. Archives of women's mental health, 22, 105-114.
- Mehta, C. M., Arnett, J. J., Palmer, C. G., & Nelson, L. J. (2020). Established adulthood: A new conception of ages 30 to 45. American Psychologist, 75(4), 431.
- Bliddal, M., Pottegård, A., Kirkegaard, H., Olsen, J.,Jørgensen, J. S., Sørensen, T. I., ... & Nohr, E. A. (2015). Mental disorders in motherhood according to prepregnancy BMI and pregnancy-related weight changes—A Danish cohort study. Journal of affective disorders, 183, 322-329.
- Silverman, M. E., Smith, L., Lichtenstein, P., Reichenberg, A., & Sandin, S. (2018). The association between body mass index and postpartum depression: A population-based study. Journal of affective disorders, 240, 193-198.
- Solorzano, C. S., Porciello, G., Violani, C., & Grano,C. (2022). Body image dissatisfaction and interoceptive sensibility significantly predict postpartum depressive symptoms. Journal of Affective Disorders, 311, 239-246.
- Getahun, D., Oyelese, Y., Peltier, M., Yeh, M., Chiu, V. Y., Takhar, H., ... & Fassett, M. J. (2023). Trends in postpartum depression by race/ethnicity and pre-pregnancy body mass index. American Journal of Obstetrics & Gynecology, 228(1), S122-S123.
- de Los Reyes, S., Dude, A., Adams, M., Castille, D., Ouyang, D. W., & Plunkett, B. A. (2023). The association between maternal body mass index and the risk of perinatal depression. American journal of perinatology, 40(02), 222- 226.
- Dayan, F., Javadifar, N., Tadayon, M., Malehi, A. S., & Komeili Sani, H. (2018). The relationship between gestational weight gain and postpartum depression in normal and overweight pregnant women. Journal of pregnancy, 2018(1), 9315320.
- Griffiths, A., Shannon, O. M., Brown, T., Davison, M., Swann, C., Jones, A., ... & Matu, J. (2024). Associations between anxiety, depression, and weight status during and after pregnancy: A systematic review and meta-analysis. Obesity Reviews, 25(3), e13668.
- Dachew, B. A., Ayano, G., Betts, K., & Alati, R. (2021). The impact of pre-pregnancy BMI on maternal depressive and anxiety symptoms during pregnancy and the postpartum period: A systematic review and meta-analysis. Journal of affective disorders, 281, 321-330.
- Cho, H., Lee, K., Choi, E., Cho, H. N., Park, B., Suh, M., ...& Choi, K. S. (2022). Association between social support and postpartum depression. Scientific reports, 12(1), 3128.
- Bradshaw, H., Riddle, J. N., Salimgaraev, R., Zhaunova, L., & Payne, J. L. (2022). Risk factors associated with postpartum depressive symptoms: A multinational study. Journal of Affective Disorders, 301, 345-351.
- Segre, L. S., O’Hara, M. W., Arndt, S., & Stuart, S. (2007). The prevalence of postpartum depression: the relative significance of three social status indices. Social psychiatry and psychiatric epidemiology, 42, 316-321.
- Bhat, P. M., & Zavier, A. F. (2003). Fertility decline and gender bias in. Demography, 40, 637-657.
- Chojenta, C., Harris, S., Reilly, N., Forder, P., Austin, M. P., & Loxton, D. (2014). History of pregnancy loss increases the risk of mental health problems in subsequent pregnancies but not in the postpartum. PLoS One, 9(4), e95038.
- Reardon, D. C., & Craver, C. (2021). Effects of pregnancy loss on subsequent postpartum mental health: A prospective longitudinal cohort study. International journal of environmental research and public health, 18(4), 2179.
- Kahalon, R., Yanushevsky Cnaani, G., Preis, H., & Benyamini,Y. (2022). The complex effects of maternal expectations on postpartum depressive symptoms: when does a protective factor become a risk factor?. Journal of Psychosomatic Obstetrics & Gynecology, 43(1), 74-82.
- Cuenca, D. (2023). Pregnancy loss: Consequences for mental health. Frontiers in global women's health, 3, 1032212.
- Ramji, R. S., Noori, M. Y., & Faisal, A. (2016). POSTPARTUM DEPRESSION (PPD) AMONG WORKING AND NON- WORKING MOTHERS/WOMEN IN KARACHI,PAKISTAN. i-Manager's Journal on Nursing, 6(3).
- Aliani, R., & Khuwaja, B. (2017). Epidemiology of postpartumdepression in Pakistan: a review of literature. National journalof health sciences, 2(1), 24-30.
- Zarghami, M., Abdollahi, F., & Lye, M. S. (2019). A comparison of the prevalence and related risk factors for post- partum depression in urban and rural areas. Iranian journal of psychiatry and behavioral sciences, 13(2).
- ACOG Committee. (2018). ACOG Committee Opinion No. 757: screening for perinatal depression. Obstet Gynecol, 132(5), e208-e212.
- Maselko, J., Sikander, S., Turner, E. L., Bates, L. M., Ahmad, I., Atif, N., ... & Rahman, A. (2020). Effectiveness of a peer- delivered, psychosocial intervention on maternal depression and child development at 3 years postnatal: a cluster randomised trial in Pakistan. The Lancet Psychiatry, 7(9), 775-787.