
World Journal of Otolaryngology Research(WJOR)


Research Article - (2022) Volume 1, Issue 1
Prevalence and Pattern of Cervical Nodal Metastasis of Upper Aerodigestive Tract Squamous Cell Carcinoma at The Time of Diagnosis in Patients Attending Tikur Anbessa Specialized Hospital from September 2015 to September 2020.
Received Date: Oct 13, 2022 / Accepted Date: Oct 19, 2022 / Published Date: Oct 28, 2022
Copyright: ©Melcol Yilala. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Citation: Melcol Yilala. (2022). Prevalence and Pattern of Cervical Nodal Metastasis of Upper Aerodigestive Tract Squamous Cell Carcinoma at The Time of Diagnosis in Patients Attending Tikur Anbessa Specialized Hospital from September 2015 to September 2020. World J Otolaryngol Res, 1(1),01-19.
Abstract
Background: UADT neoplasms is a heterogenous diseases entity which includes primaries arising from nose and paranasal sinuses, nasopharynx, oral cavity, oropharynx, hypopharynx and larynx. Squamous cell carcinoma is the predominant histologic type. The likelihood of having nodal diseases at presentation may have a wide range depending the size and site of the primary tumor with significantly higher risk for patients with nasopharyngeal primaries and advanced T stage of other sub-sites of upper aerodigestive tract. Chances of having multiple and bilateral nodes also have direct correlation with the size of the primary tumors. Positive cervical nodal status is one of the most reliable prognostic factors which drops cure rate significantly. It is also responsible for treatment failure, local recurrence and reduction of survival rate and it’s a reliable indicator of development of distant metastasis. The pattern of distribution of nodal involvement is different for each site. Thorough study of distribution of most likely involved lymph node levels for each sub site helps to customize the neck treatment accordingly by avoiding radical treatments with significant functional and aesthetic morbidity.
Objective: To define prevalence and pattern of nodal and distant metastasis of UADT-SCC patients at the time of diagnosis.
Method: Institution based retrospective cross-sectional medical chart review of patients from September 2015- September 2020 was conducted. 259 patients who fulfilled the inclusion criteria were selected using systematic random sampling technique and data was collected using questioner.
Result: A total of 259 medical records were reviewed. Mean age at presentation is 44.8. Male to female ratio is 2.6:1. Prevalence of positive nodal diseases at presentation is 71%. Site specific analysis showed 50% of nose and PNS, 86.1% nasopharyngeal, 73.2% oral cavity, 70% oropharyngeal, 66.7% hypo-pharyngeal and 57.2% laryngeal primaries had positive nodal diseases at presentation. Majority of late presentations had positive nodal diseases (p<0.05). Nasopharynx is the commonest site of primary tumor (30.5%). It is also the commonest site with higher percentage of positive nodal diseases (86.1%). Most patients had advanced stage at presentation (cTNM stage III and IV- 88.1%). Distant metastasis was found in 10.8% of patients and had strong association with T stage (p<0.05).
Conclusion and Recommendation: This study concluded that majority of patients fall in the age group of 31 to 40 with male predominance of 2.6 to 1. Late presentation is a rule since most patients with UADT-SCC has advanced disease at presentation with significant nodal neck diseases. Nasopharynx is the commonest site of primary tumor forboth males and females. It's also the commonest site of primaries with higher percentage of positive nodal diseases at presentation. Chances of having positive cervical nodal disease at presentation were very high in patients with advanced T diseases. Pattern of metastasis of most sites are in line with the current accepted knowledge of practice. Research designs with better strength should be used to study the clinicopathologic behavior of UADT-SCC both nationwide and in region specific setups. Institutional cancer registry should be improved and made easily accessible to researchers. Patient’s medical records should be complete. Policies on preventive measures and screening tools should be designed. Health seeking behavior of the community should be improved. Referral system should be made easy for patients with suspected cases.
Introduction
Upper aerodigestive tract neoplasm is a heterogenous diseases entity which includes primaries arising from nose and paranasal sinuses, nasopharynx, oral cavity, oropharynx, hypopharynx and larynx. Squamous cell carcinoma is the predominant histologic type responsible for 90% of UADT malignancies.
Primaries from each site of UADT has relatively predictable distinct pattern of lymph node drainage pattern [4]. A thorough knowledge of this distribution helps the clinician to predict the site of possible nodal metastasis and decide on the appropriate neck treatment with less functional and aesthetic morbidity. It is also important to trace the site of the primary tumor when the initial presentation is neck diseases.
Statement of the Problem
The presence of cervical nodal involvement in squamous cell car- cinomas of upper aerodigestive tract primaries is one of the most important prognostic factors that drops cure rate significantly Shah, [1]. Relevance of cervical nodal metastasis at the time of diagnosis has long been established and found to be responsible for treatment failure, local recurrence and reduction of survival rate by nearly 50%. It is also a reliable indicator of development of distant metastasis [2]. The 5- years survival rate of patients who have cervical nodal metastasis at the time of diagnosis reduces and it depends on the size and number of involved nodes and presence or absence of extra capsular spread [3]. Similar study reviewing 267 patient records undertaken in Liverpool demonstrated 5-yeras survival of patients who initially presented with cervical nodal me- tastasis to be 27% [4].
Its incidence may range from 1 to 85% depending on the site and size of the primary tumor and the risk in advanced T3 and T4 stage tumors is more than 50% [5]. The incidence of cervical nodal involvement at the time of diagnosis increases as the size of the primary tumor gets bigger in certain sub sites of upper aerodi- gestive tract like oral cavity, soft palate and tonsillar pillars. The likelihood of having multiple and bilateral nodes also have direct correlation with the size of the primary tumors arising from sites mentioned earlier [6].
Certain risk factors are identified as increasing the chance of hav- ing nodal involvement at presentation and these include site and size of primary tumor, degree of differentia tion, perineurial inva- sion and tumor thickness.
Significance of the Study
Since it's not uncommon to see patients with advanced HNSCC patients with initial presentation of nodal diseases at Otorhinolar- yngology and Oncology clinics, determin ing its prevalence and pattern has many significant benefits.
The study provides insight about the burden of loco-regionally ad- vanced UADT-SCC at presentation in our setup, provides basis on risk group analysis and help clinicians to focus on possible areas of metastasis during metastatic workup so as to shorten the time between the initial presentation and initiation of treatment.
It’s evident that management of the neck of UADT-SCC patients is still a matter of con troversy and to deliver the optimal treatment it needs an evidence-based study on the pattern of distribution of nodal disease for each primary site. Knowing the patterns of nodal metastasis for each site of upper aero-digestive tract helps design the appropriate plan of management, customize the neck treatment with respect to each primary site and decide on the type of neck dissection to be done.
There is no study done in the incidence and pattern of nodal me- tastasis in hand and neck cancer in our institution so this study also helps to enlighten the responsible health care works and patients on the seriousness of advanced UADT-SCC and paves the way for future studies intended to determine prognosis, survival and dis- tant metas tasis as presence of nodal diseases at presentation is the single most important factor that determines the aforementioned areas of studies.
Objectives
General Objective
• To define preverence and pattern of nodal metastasis of upper arodigestive tract SCC patients at the time of diagnosis.
Specific Objectives
• To determine the prevalence of nodal metastasis at initial presen- tation with respect to different sites of UADT-SCC.
• To depict topographical distribution of lymph node metastasis with respect to differ ent primary sites of UADT-SCC.
• To determine the impact of duration of symptoms, site of primary tumor and clinical stage of primary tumor on the development of advanced diseases.
Literature Review
The pattern of lymph node drainage varies for different sites of up- per aerodigestive tract. The location of lymph node metastasis has significant prognostic value explained by worse prognosis when lymph nodes beyond first echelon nodes are involved [4]. The presence of cervical nodal involvement in squamous cell car- cinomas of upper aerodigestive tract primaries is other most im- portant prognostic factor that drops cure rate significantly [1].
Cancer of Oral Cavity
Location, pattern and incidence of metastasis from Oral cavity SCC vary according to the respective sub sites even though most tumors from these subsites typically drain to level I, II and III cer- vical nodes and there is a high tendency of bilateral nodal involve ment for midline lesions. Tumors that are 1cm away from mid line has lower tendency of contralateral nodal involvement [5]. Sublev- el IIB involvement was also demonstrated in 10% of patients with OC SCC [7]. Tumor thickness and ad vanced T stage are reliable indicators of nodal involvement [5].
Lip- cervical nodal metastasis is infrequent in primaries arising from lower lip occurring in only 10% of patients while the risk increases for upper lip and oral commissure tumors (Cummings).
Aleveolar ridge tumors arising from Upper–alveolar ridge tends to metastasize to jugulodigastric lymph nodes, whereas lower–alve- olar ridge tumors drain to submandibular lymphatics (Cummings) also demonstrated similar result where level I and II are found to be the most frequently involved nodes in their study [1]. There is correlation between mandibular bone invasion and increased risk of cervical nodal metastasis at presentation [8]. A systematic re- view by demonstrated the over-all incidence of nodal metastasis at presentation to range from 11.5 to 29 percent for maxillary gin- gival SCC and 18 to4 6 percent for mandibular gingival SCC [9].
Oral tongue- At initial presentation, 40% of patients with oral tongue carcinoma demonstrate evidence of cervical metastases (Cummings). Level II, III and I are most frequently involved in that order [1]. In their 20 years retrospective review of 277 pa- tients’ card demonstrated there is a 15.8% risk of skip metastasis to level II and III cervical nodes [10].
Retromolar trigone- At the time of presentation, up to 50% of pa- tients have regional metastatic disease. Level I and II are the most common sites involved followed by level III and IV [1].
Floor of mouth- Risk of cervical nodal metastasis for this subsite increases with the T stage of the primary tumor reaching approx- imately 30% for T2 lesions and 50% for advanced T3 and T4 le- sions. Submandibular lymph nodes are most frequently involved, and bilateral metastases are common with lesions of the anterior floor of the mouth. (Cummings). In their retrospective study in- volving 501 patients in 1990 Shah et.al depicted level I, II and III are most frequently involved nodes in that order and they also find metastasis in level V occurring in 6% of the times.
Buccal mucosa-When compared to tumors arising from other sub sites, cervical nodal metastasis at presentation in buccal SCC pa- tients is less frequent rendering elective treatment of the region- al lymphatics is unnecessary. Majority of patients are No at pre sentation. Level one and two are the most frequent sites of nodal involvement. Shah, 5 years survival rate for those who presented with positive nodal diseases was 49% [1]. Diaz et.al. T stage and thickness of the primary tumor are the two reliable indicators of nodal metastasis [11]. Jing et.al (2006) Overall clinical nodal posi- tivity was seen in 31.1% of patients of which around 88% occurred in advanced T3 and T4 primary tumors.
Hard Palate- Clinically positive nodal diseases at presentation is significantly correlated with advanced T stage of primary hard pal- ate SCC as depicted by Lin et.al (2009) in their cross-sectional population analysis that showed 4.1% 14.9% 10.3% and 24.7% of patients with T1, T2, T3 and T4 tumor has positive nodal diseases respectively.
Cancer of Oropharynx
SCC of oropharynx is one of the most aggressive tumors of up- per aerodigestive tract with a high likelihood of early and exten- sive cervical nodal metastasis. Risk of nodal metastasis from such primaries has an overall incidence of 92%, Gross et.al. and most frequently involved nodal sites are level II and III cervical nodal groups Vartanian, et al. [3].
Oropharyngeal SCC frequently drain to level II, III, IV, parapha- ryngeal and Retrophin geal nodes. Most frequently involved nodes are level II (83%) and III (45%). Lim et.al 2006. Sublevel II B is rarely involved representing 2.5% and contralateral nodal in- volvement was 15%. Among 1,155 patients who presented with cervical nodal metastasis Lindberg, demonstrated the percentage of nodal metastasis at presentation for soft palate, tonsillar fos- sa, taste of tongue and posterior oropharyngeal wall is 44%, 76%, 78% and 59% respectively [6]. They also depicted the most fre- quently involved level of lymph nodes for each subsite to be level III followed by level II groups and bilateral nodal involvement was significant for tumors of soft palate, base of tongue and posterior pharyngeal wall. Another retrospective study done by Shah, also demonstrated the most likely lymph node levels to be involved are live [1]. II, III and IV in that order [1].
A retrospective analysis conducted by Chung et.al in 2011 depict- ed among 98 neck dissection specimens collected from tonsillar SCC, 65.3% had nodal metastasis, 72.4% ipsilateral and 11.8% contralateral [12]. Most frequently involved lymphnode levels in- volved where level IIA followed by level III for both ipsilateral and contralateral speci mens.
Another retrospective medical record review of 333 patients with oropharyngeal and hypopharyngeal primaries and showed a preva- lence of positive neck disease at initial visit to be 84%. This review also depicted the overall of occurrence of positive nodal diseases in level II, III and IV to be 25%,19% and 8% respectively and in- volvement of level I and V is rare and always found only with the involvement of most frequent levels [13].
Cancer of Larynx
The incidence and pattern of cervical nodal metastasis in patients with laryngeal cancer vary with respect to the sub site of the pri- mary tumor. In a retrospective record re- view undertaken by Shah, it was made evident that 84% of therapeutic and 37 % of eleven RND had histopathological confirmed metastatic nodal diseases. The same study also demonstrated the most frequent nodal in- volvement included level II, III and IV nodal groups with less rare involvement of level I and V nodes. Shah, another study conducted by Cole depicted an overall nodal positivity rate for supraglottic and glottic larynx to be 50% and 22% respectively [1]. Cole et.al. [14]. Similar retrospective study undertaken by Candela showed level II, III and IV to be at greatest risk to harbor metastatic diseas- es from laryngeal primaries with rare involvement of level I and V which indicates nodal involvement of other sites. Candela et.al. [13]. Contralateral nodal involvement was demonstrated in 37% of patients with clinically positive node. Buckley et.al. Paratracheal nodal involvement of 26% in patients with advanced laryngeal, hypopharyngeal and cervical esophageal cancer was made evident by a prospective study undertaken by Timon and colleagues [15]. This same study showed the overall prognosis of patients with paratracheal diseases to be low Timon, et.al. [16].
Supraglottic SCC- Because of its rich lymphatic drainage system tumors arising from here have a higher tendency of nodal metas- tasis, over 60% when compared to other sub sites rendering elec- tive neck treatment mandatory. The likelihood of having bilateral nodal metastasis is also common here and level II, III and IV are the most frequently involved nodes. In their retrospective review published in 1972 Lindberg revealed upper jugular nodes to be the most commonly involved nodes followed by mid jugular nodes with frequent bilateral nodal involvement. Level I and V are rarely involved, 6% for each lymph node group. Candela et.al. Similar retrospective study undertaken by Redaelli and colleagues un- veiled chances of nodal metastasis from Supraglottic SCC reaches 40% with increasing prevalence in higher T stages. This study also revealed that level II and III are the most frequent sites of involve- ment with occurrence rate of 82% and 41% with no isolated in- volvement of other lymph node levels. Same study depicted that there is higher chance of bilateral nodal involvement for tumors arising more centrally than peripherally accounting for 20% and 5% respectively Redaelli, et al. [17].
Glottic SCC- lymphatic spread here is rare, less than 20%, when compared with other sub sites due to lack of submucosal lymphat- ics in the area and if spread occurs it is usually to level II, III, Iv and VI nodal groups. Bilateral nodal involvement is uncommon in glottic cancer. Like most primaries of upper aerodigestive SCC, there is a strong correlation between the T stage of laryngeal can- cer and the likelihood of having nodal metastasis at presentation. Involvement of Delphian nodes is an indicator of advanced T3 and T4 stage tumors.
Subglottic SCC- primary tumors of subglottic larynx are very rare constituting less than 5% of all laryngeal cancer cases. Despite the aggressiveness of the subglottic SCC having clinically positive nodal diseases at presentation is rare ranging from 4 unto 14%. Dahm, et al. However, there is a higher chance of occult metas- tasis which makes these lesions demand elective neck treatment [18]. Level VI paratracheal nodes are most frequently involved with both ipsilateral and contralateral involvement and unlike the two sub sites involvement of level III, IV lymph node groups are rare here. Retrospective study undertaken by Dahm and colleagues revealed 78.6% of their patients had N0 at presentation while N1, N2 and N3 diseases at presentation constitute 10.7%, 7.1% and 3.6% respectively Dahm, et al. [18].
SCC of Hypo-pharynx
Primary tumors arising from hypopharynx has the highest propen- sity of cervical nodal metastasis at presentation when compared to tumors arising from other specific sites of upper aerodigestive tract T.R. Helliwell, Lefebvre et al. [19,20].
Neck lump is the second most presen presenting symptom occur- ring in 82% of patients. This only follow difficulty of swallowing which was apparent in almost all patients with hypopharyngeal SCC.
Clinically palpable node at presentation occurred in 86% of pa- tients out of which 68% had unilateral nodes and the rest 18% had bilateral. Another study by Million et al. revealed 79% of their subjects had clinically positive node at ad- mission and 15% had bilateral positive nodes. T.R. Helliwell, also showed 70% nodal metastasis at presentation with 18% of bilateral involvement [19].
Various studies depict the most likely involved lymph node levels and there are appar ent differences in pattern and frequency among the three subsites of hypo pharynx. Primaries of pyriform sinus frequently goes to level II, III and IV, post cricoid tumors goes to level II, III and paratracheal nodes whereas 40% patients with primaries arising from posterior pharyngeal wall had metastasis to retropharyngeal lymhnodes T.R. Helliwell [19]. In their study of pyriform sinus SCC Nishi et.al. found that almost all cervical nod- al metastasis was confined to level II and III nodes. Level II lymph nodes are the most involved groups followed by level III and IV and involvement of level V is always associated with nodal me- tastasis at other sites. Candela et. al [13]. Level VI nodal involve- ment is usually seen in advanced tumors arising from post-cricoid and pyriform apex areas or lower pharyngeal areas. Timon, et al. Lindberg in their study conducted in 1155 patients with SCC of upper aerodigestive tract and positive node at presentation depict- ed that bilateral nodal involvement for pyriform sinus tumors is rare [6,16].
Most patients at presentation had advanced diseases. In their study T.R. Helliwell, depicted 63% of their patients had T3 and T4 dis- eases and 87% were stage III and IV [19]. In another study con- ducted by Lefebvre et al. 70% of patients had T3 and T4 tumor at presentation [20].
Cancer of Nasopharynx
Palpable neck lump is the most common presenting symptom of NPC patients occur- ring in 60% of patients and clinically node patients at presentation are around 80% and one third of patients have bilateral nodal involvement.
The initial echelon lymph node for the nasopharynx is the retro pharyngeal nodal groups from which the drainage system ends up in upper jugular and upper posterior lymph node groups. Linde- berg in the article published in 1972 demonstrated most frequently involved nodes to be level II nodes both ipsilateral and contralat- eral with significant involvement of level V and supraclavicular nodes, the last one being an indicator of more advanced N3 stage. Systematic review by Ho et. Al also depicted retro pharyngeal and level II nodes are involved in 69.4% and 70.4% l of patients re- spective ly followed by level III, VA and IV. Less frequently in- volved nodes include level I, VI, parotid and supraclavicular nodes [21]. Skip metastasis at presentation is also very rare in NPC pa- tients occurring in 0.5% of cases. Ho et al. [21].
Aggressiveness of early T1 and T2 nasopharyngeal tumors can be explained by the simi lar distribution of cervical nodal involve- ment with more advanced T3 and T4 tumors Lindberg, [6]
Cancer of Nose and Paranasal sinuses
Paranasal and nose SCC are accounting only 3% head and neck SCC. Patients with primaries from these sites usually present with advanced diseases after long standing and nonspecific complaints. Clinically patients usually present with non-specific nasal and or- bital complaints and neck swelling is very rare at initial encoun- ter only accounting for 4% of presenting symptoms Jackson et al. [22].
Unlike the other sites of upper aerodigestive tract, cervical nodal metastasis at the time of diagnosis is rare in patients with SCC of nose and PNS. In their systematic review Dulguerov, et al. found only 2.3% of their patients had positive node at the time of diagno- sis where all patients had T3 and T4 diseases arising from maxil- lary sinus, ethmoid sinus and nasal cavities. Similar study done by Cantu et al. depicted nodal metastasis from SCC of ethmoid and maxillary sinuses to be 1.6%, and 10% respectively with a final recommendation of doing neck dissection for such patients [23]. An- other study by Lavertu, et al. showed 75% of their cases had T3 and T4 diseases at presentation [24].
Cervical metastasis either at the time of initial presentation or through the course of treatment is a strong indicator of unfavor- able outcome and patients who present with positive neck disease should undergo neck dissection even though elective treatment regarding node negative diseases still remains a matter of contro- versy Cantu, et al. [23].
Methodology
Study area and period
Study was conducted in Tikur Anbessa Specialized Hospital, On- cology Unit and Otorhinolaryngology- Head and Surgery depart- ment clinics from September 2015 to September 2020.
Study design
Retrospective chart review of patients seen at Oncology and ORL- HNS clinics
Source and study population
Source population
All patients with initial diagnosis of UADT-SCC seen at Oncology and ORL-HNS clinics of TASH in the given time frame
Study population
All patients with initial diagnosis of UADT-SCC seen at Oncology and ORL-HNS clinics of TASH who are included in the sample.
Inclusion criteria
• Patients with histologically confirmed squamous cell carcinoma of upper aerodigestive tract
Exclusion criteria
• Patients with histopathologic report other than SCC
• SCC arising from other sites of head and neck like skin, ear, thy- roid and salivary glands
• Patients with working diagnosis of CUP
• Patients who has received chemotherapy, radiation therapy or both elsewhere before presentation
• Patients with incomplete medical record
Study Variable
Dependent Variables
• Prevalence of nodal metastasis
• Pattern of lymph node metastasis
Independent variables
• Sociodemographic factors
• Duration of illness
• Site of primary tumor
• Stage of primary tumor
Sample size determination
• Sample size for this study was determined using the formula to estimate a single population proportion
n = (Zα/2)2 * P (1-P)/d2
Where,
P= expected prevalence of UADT-SCC patients [0.5]
(Zα/2)2 =critical value at 95% certainity [ (1.96)2= 3.84]
d= marginal error between samples and population 0.05
Therefore n= calculated sample size [384]
Since source population is <10,000 population correction formula is
nc= n/(1+n/N) = 384/ (1+384/603) = 235
Where,
nc= Corrected sample size [235]
n= Un corrected sample size [384]
N= Source population [603]
10% non-response rate will be added to the corrected sample size and final sample size will be 259.
Sampling procedure
Systematic random sampling technique was used to draw cards.
K value was calculated
K=N/n = 603/259= 2.3~ 2 which means every 2cards.
Where,
N is total number of head and neck patients in 4yrs n is the sample size calculated
Data collection technique
• Patients medical record numbers are obtained from Oncology and ORL-HNS clinics
• Charts were collected from the hospital store
• GPs, nurses and junior residents who are trained on data collec- tion used the ques tionnaire to collect data from each selected chart
• The investigator supervised the process of collection
Data management and analysis
• Data entry was checked manually by the investigator • SPSS version 23 was used for data analysis
Operational definition
• Upper Aerodigestive tract- Nose and paranasal sinuses, Naso- pharynx, Oropharynx, Oral Cavity, Larynx and hypo-pharynx
• Head and neck cancer
Dissemination of results
Final copy of the thesis was be submitted to the department of ORL-HNS, department Oncology and School of public health, College of Health Sciences of Addis Ababa University both in hard and soft copies. Also, manuscript was developed and submit- ted for publication on international journals.
Ethical consideration
Ethical clearance will be obtained from the Institutional Review Board (IRB) of College of Health Sciences of Addis Ababa Uni- versity. Approval will be obtained from department of ORL-HNS and department of Oncology.
Results
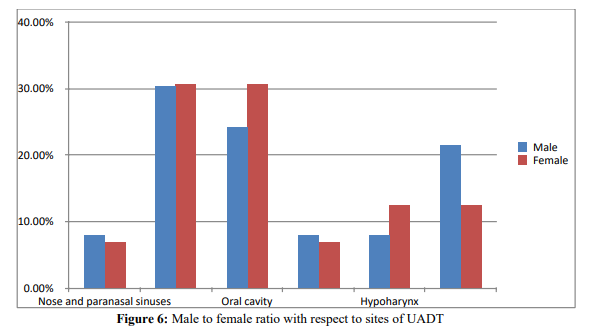
A review of 259 medical records of patients seen from Septem- ber 2015 to September 2020 at TASH were analyzed. Among the patients 72.2% were males and 27.8% were females with male to female ratio of 2.6 to 1.
The average age presentation is 44.8 +/- 15.8 years. Their age ranged from 13 to 85 with a median of 45 years. Majority of pa- tients fall in the age group of 41 to 50 years (22.8%), followed by the age range of 31 to 40 years (22%) and 51- to 60 years (20.5%) respectively.
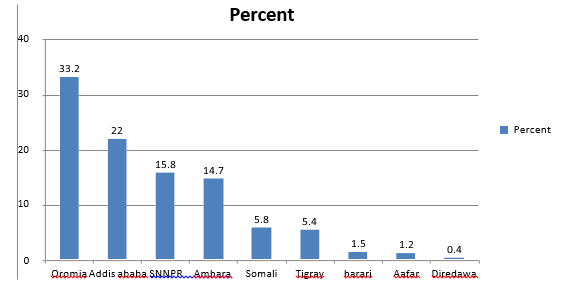
Most common regions where patients came from are Oromiya (33.2%), Addis Ababa (22%) and SNPPR (15.8%) respectively.
Nasopharyngeal and Oral cavity SCC were the two most primaries for both male and female patients (p=0.06).
Figure 1: Regional distribution of UADT SCC in percentage
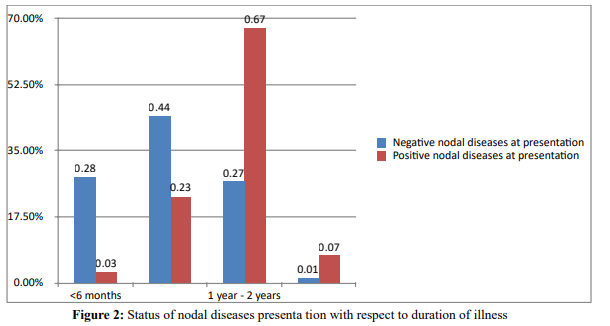
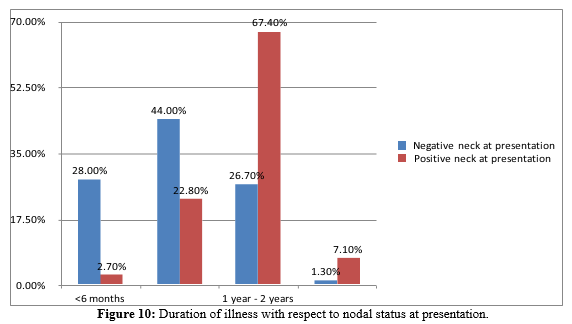
Most patients seek medical attention between one and two years since the onset of their initial symptom (55.6%) followed by 6 months upto one-year duration (29%) and only 10% of patients seek medical attention within 6 months since the onset of their ill- nesses. Majority of patients who come late have positive nodal dis- eases at presenta tion and this is statistically significant (P
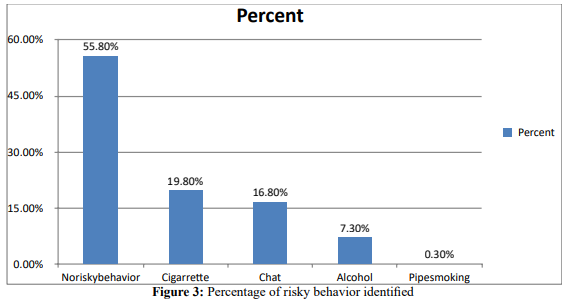
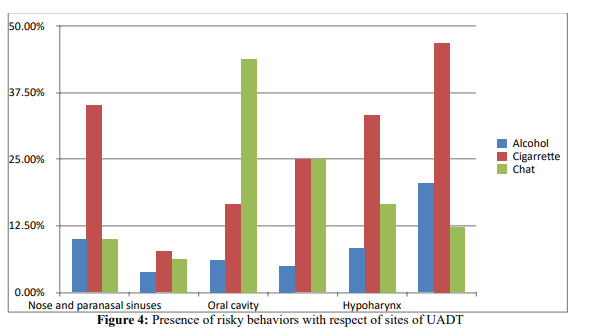
Cigarette smoking was the most common behavior identified followed by chat cheewing and alcohol use accounting for 19.8%, 16.8% and 7.3% cases respectively.
Smoking was the most common habit in patients with larynge- al (46.9%), hypopharyngeal (33.3%), nose and PNS (35%) and nasopharyngeal (7.6%) primaries. Chat cheewing was the most common in patients with oral cavity primaries (43.9%) and pa- tients with oropharyngeal SCC chat cheewing (25%) and smoking (25%) were equally identified. (P <0.05).
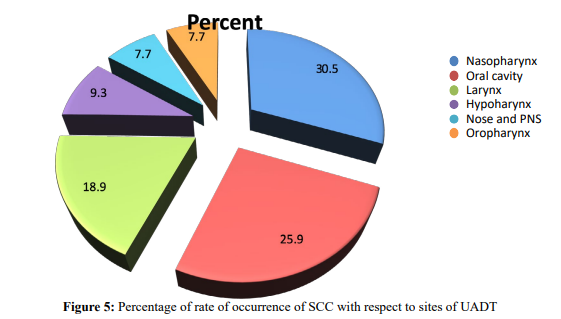
The primary tumors arise from the nasopharynx in 79 (30.5%), oral cavity in 67 (25.9%), larynx in 49 (18.9%), hypo pharynx in 24 (9.3%), nose and paranasal sinuses in 20 (7.7%) and oropharynx in 20 (7.7%) patients.
Nasopharyngeal and Oral cavity SCC were the two most primaries for both male and female patients (p=0.06).
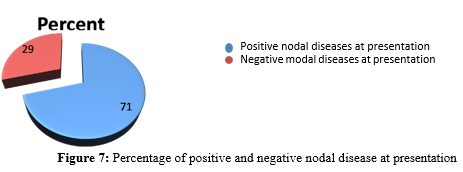
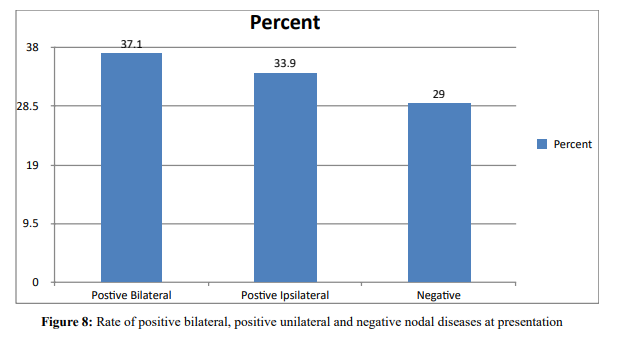
Only 75 patients (29%) had negative clinical nodal status at presentation and positive clinical cervical nodal diseases was confirmed in 184 of patients (71%) at initial presentation.
Among the positive nodal diseases at presentation 86patients (33.9%) had unilateral diseases and 96 patients (37.1%) had bilateral dis- eases.
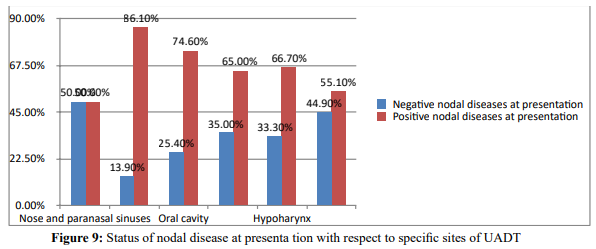
Site specific analysis revealed 68 patients with nasopharyngeal (86.1%), 50 patients with oral cavity (74.6), 27 patients with hypopha- ryngeal (66.7%), 16 patients with oropharyngeal (65%), 13 patients (55.1%) with laryngeal and 10 patients with nose and paranasal sinuses (50%) had positive nodal diseases at initial presentation (p<0.05).
Longer duration of illness is associated with higher chance of nodal diseases at pre sentation (P<0.05).
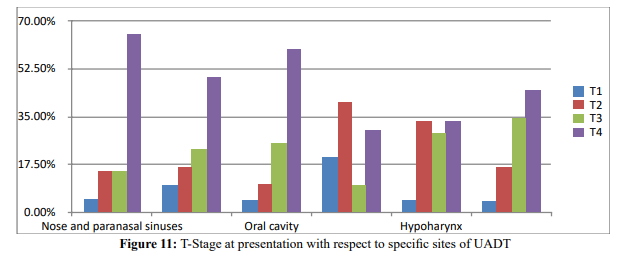
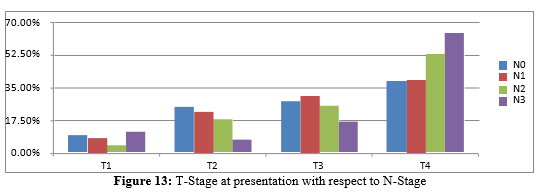
Overall analysis of T stage disease showed majority of patients come with advanced T4 and T3 diseases 49.4% and 24.7% respectively. Likewise, primary site-specific results showed advanced T stage at presentation (p<0.05).
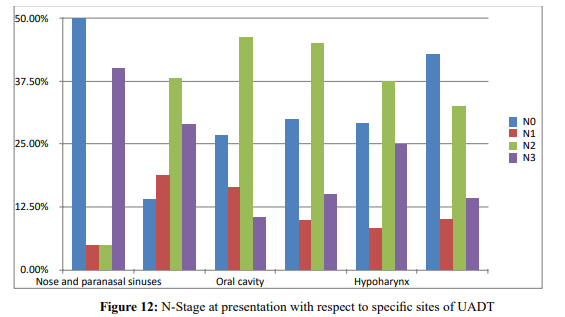
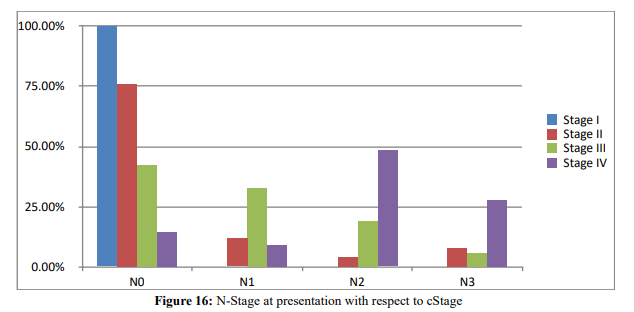
Most common nodal stage at presentation is N2 (31.7%) followed by N0 (28.2%), N3 (20.8%) and N1(13.5%). Site specific nodal stage analysis showed majority of patients with laryngeal and nose and PNS primaries present with NO diseases while patients with primaries from nasopharynx, oral cavity, hypopharynx and oropharynx had advanced nodal diseases (N3 and N2) at initial visit. (p<0.05).
The likelihood of having advanced nodal diseases at presentation is also evident in bigger T3 and T4 primaries(p<0.05).
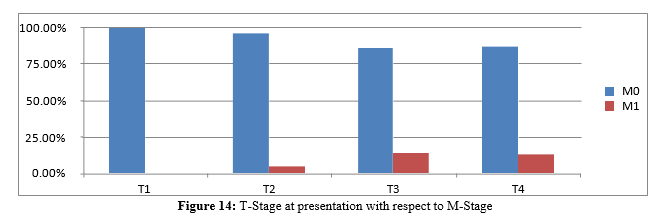
Distant metastasis at presentation were seen in 28 (10.8%) patients. Correlation of dis tant metastasis with site of primary tumor was not statistically significant while there was a statistically significant result when it comes to correlation with advanced T stage(p<0.05).
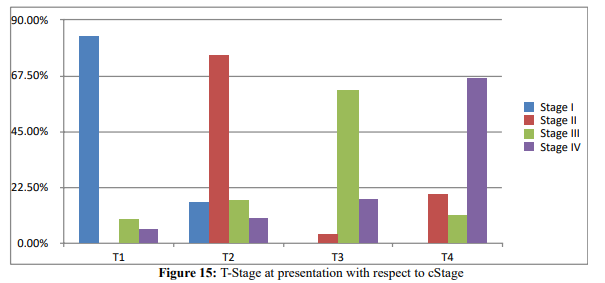
cTNM staging outputs revealed an overall late presentation with cTNM stage IV (68. %) and stage III (20.1%). There was a statistically significant association between cTNM and both T and N status of the tumor(p<0.05).
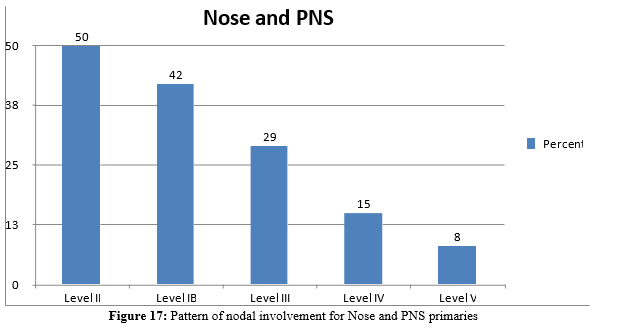
Pattern of lymph node metastasis was analyzed for each six sites of primaries with respect to the most frequent cervical nodal in- volved. Among patients with nose and paranasal sinuses primaries 50% had negative, 30% unilateral positive and 20% bilat eral pos- itive clinical nodal diseases at presentation (p<0.05). Majority of patients had advanced T and cTNM stage diseases at presentation (p<0.05). Level II (50%), IB (42%), III (29%) and IV (15%) are the most common involved nodes and level V is involved in only 8% of cases.
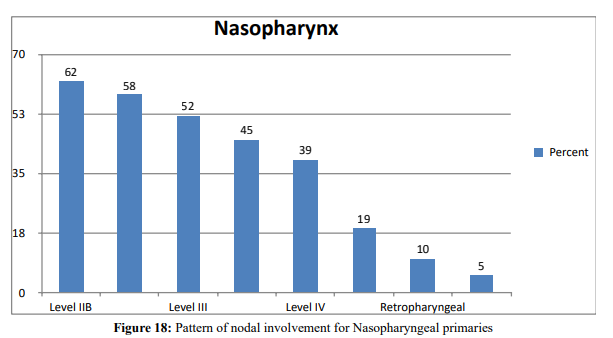
Among patients with nasopharyngeal primaries, negative, ipsilateral positive and bilater al positive nodal diseases account for 13.9%, 27.8% and 58.2% respectively(p<0.05). Level IIB (62%), IIA (58%), III (52%) and V (45%) are the most involved nodes.
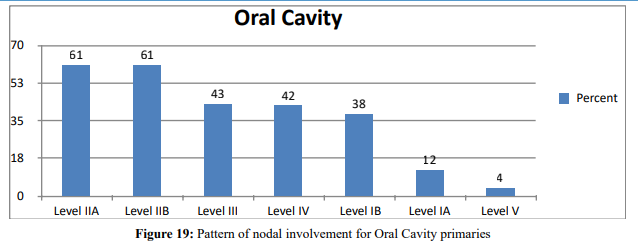
Among patients with oral cavity primaries negative, ipsilateral positive and bilateral positive nodal diseases account for 26.9%, 28.4% and 44.8% respectively (p<0.05). Level IIA (61%), IIB (61%), III (43%), IV (42%) and IB (38%) are most nodal levels involved and involvement of level IA is only 12%.
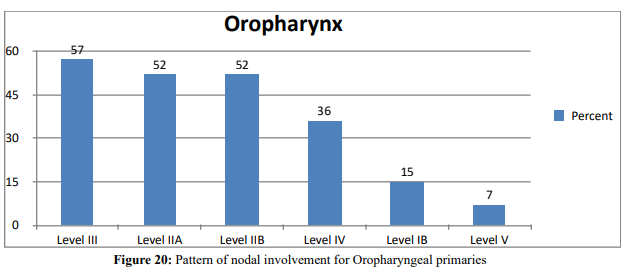
Among patients with oropharyngeal primaries negative, ipsilateral positive and bilateral positive nodal diseases account for 30%, 40% and 30% respectively(p<0.05). Level III (57%), IIA (52%), IIB (52%) and IV (36%) are most commonly involved and level I and V involvement is less than 20%.
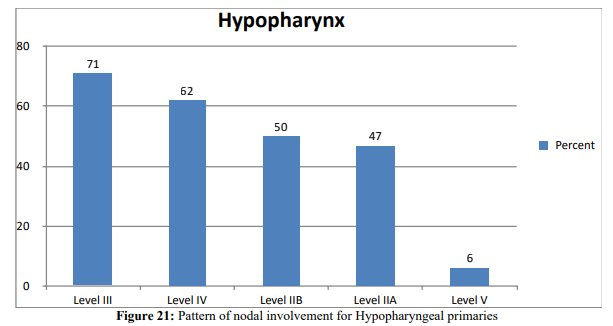
Among patients with hypopharyngeal primaries negative, ipsilateral positive and bilateral positive nodal diseases account for 33.3%, 29.2% and 37.5% respectively (p<0.05). Level III (71%), IV (62%), IIB (50%) and IIA (47%) are common sites of involvement while level V is involved in less than 10% of cases.
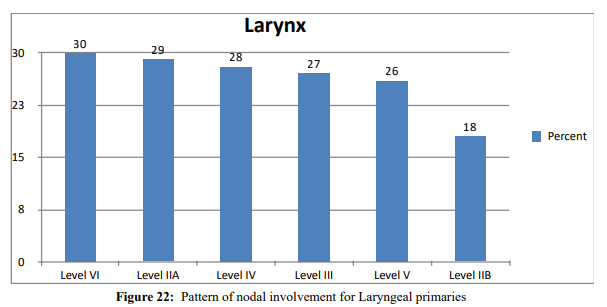
Among patients with laryngeal primaries negative, ipsilateral positive and bilateral positive nodal diseases account for 49.2%, 38.8% and 18.4% respectively (p<0.05). Level VI(30%), IIA(29%), IV(28%), III(27%), V(26%) and IIB(18%) were most common involved nodal levels.
Discussion
In this study the overall prevalence of positive clinical cervical nodal diseases at initial presentation is 71%. This finding is com- parable with other studies. Prevalence of positive nodal disease at presentation varies from 1% upto 85% with more than 50% chance of occurrence in T3 and T4 tumors. It’s also highly dependent on site of prima ry tumor and cTNM stage of the diseases [5, 1].
Late presentation in terms of advanced T stage (T3 and T4) of 74.1% at presentation, cTNM (stage III and IV) of 88.1% at pre- study done in Nigeria revealed chances of having stage III and IV disease at presentation is greater than 80% [25]. This could be due to lenient health seeking behavior, socioeconomic factors, lack of screening tools in primary health facilities and procrastinated re- ferral process.
Prevalence of positive nodal diseases for nose and PNS primaries was 50%. This result is significantly higher when compared with findings from a couple of literatures cited. Only 2.3% of patients were found to have positive nodal at presentation even though all participants had T3 and T4 diseases. Chances of having positive nodal disease were 1.6% and 10% for ethmoid and maxillary sinus SCC [26]. Only 29% of their patients had positive cervical nodal disease at presentation despite 75% had T3 and T4 diseases at pre- sentation [24]. Having positive nodal dis- ease at presentation is a rare encounter occurring in only 4% of cases. Having such a signif- icant proportion of patients with positive nodal diseases, where the rule elsewhere is advanced T stage with rare nodal disease can’t be sufficiently explained by only late presentation and further study should be pursued to study the Im pact of genetics, environmental factors, sun-cite and histologic type analysis. Pattern of nodal in- volvement is consistent with other literatures.
There is a very high chance of having positive nodal disease at presentation accounting for 85% of total cases with Level II (70%) and RPLNs (69.4%) being the most common sites of nodal dis- eases [21]. The percentage of positive cervical nodal at admission was 87% with significant bilateral disease, supraclavicular and retropharyngeal nodal involvement [6]. The likelihood of having bilateral lymphadenopathy was 81%. This study showed a prev- alence of positive nodal diseases for nasopharyngeal primaries (86.1%) and 68% chance bilateral involvement which is consistent with several articles reviewed. However, the percentage of retro- pharyngeal nodal involvement was way below expected and this might be due to inaccessibility of evaluation of this LN groups by physical examination and radiologic underreporting. The frequen- cy of occurrence in other lymph node groups was comparable with findings of different studies. In this study the prevalence of positive nodal diseases for oral cavity primaries was found to be 73.2% among which 61.2% had bilateral nodal diseases. This finding is higher than what is ex- pected based on different articles sited which showed a prevalence of 10-40% at initial presentation [1,8,10,11,27, 28]. This may be attributable to tumor degree of tumor differentiation, younger age at presentation or rising incidence of HPV related process which needs further investigation. It also depicted level IIA, IIB, III, IV and IB to be the most frequent levels involved which is in line with other citations that show similar results except there is higher fre- quency of level IV involvement in this study that might be due to more advanced diseases at presentation. Sublevel IIB involvement was less than 10%.
This study showed the prevalence of positive nodal diseases for oropharyngeal pri maries to be 70% out of which 42% had bilat- eral neck diseases at initial visit. This find ing is consistent with findings obtained from other studies. Prevalence of positive nodal diseases at presentation was 84%, 92%, 44-78% depend ing on dif- ferent subsites and 65% out of which 11.8 % had bilateral diseases [13,6,12]. The pattern of nodal involvement depicted in this study is also consistent with other studies findings which showed most frequent nodal levels involved to be level II and III followed by level IV [1,6,3,12,29].
Prevalence of positive nodal diseases for hypo pharyngeal prima- ries was 66.7%. This finding is in line with other studies done on similar topics. Positive cervical nodal dis- eases at presentation is the second common symptom occurring in 86% of the cases out of which 18% are bilateral. Hypopharyngeal SCC has a higher pro- pensity to nodal diseases at initial visit accounting for 79% with a 15%likelihood of bilateral neck diseases, also showed a 70% chance of positive nodal diseases at presentation among which 18% had bilateral neck diseases [19]. Findings regarding pattern of lymph node levels involved (level II, III and IV) were consistent with findings of similar studies [1,6,13,16].
The prevalence of positive nodal diseases for laryngeal at presen- tation is 57.2% out of which 32.8% had bilateral neck diseases at presentation This finding is not sub-site specific which is con- sistent only with supraglottic primaries (Redaelii) [13,14]. How- ever, glottic and subglottic primaries has lower (20-30%) risk of nodal diseases at presentation. Sub-site-specific prevalence study should be done to depict more reliable figures. Pattern of nodal involvement with level IV, II, III and IV being the most frequently involved is consistent with findings of other citations [1,6,13,16].
Strengths
• Large representative sample size.
• Cross tabulation analysis was done among various important variables and majority of outputs were statistically significant.
• First study in this institution.
Limitations
• Retrospective study
• Patient medical records don’t have sufficient information regard- ing sub-sites of pri mary tumors.
• Thorough radiologic report of lymph node sub-levels and retro- pharyngeal lymph nodes couldn’t be retrieved from patients’ med- ical records.
• There are no similar articles written in countries with similar set up like ours.
• Incomplete documentation of cases on logbooks.
Conclusion
This study concluded that majority of patients fall in the age group of 31 to 40 with male predominance of 2.6 to 1. Late presentation is a rule most patients with UADT- SCC has advanced disease at presentation with significant nodal neck diseases. Nasophariynx is the commonest site of primary tumor for both males and females. It’s also the comments site of primaries with higher percentage of positive nodal diseases at presentation. Chances of having positive cervical nodal disease at presentation are very high in patients with advanced T diseases. Pattern of metastasis of most sites are in line with the current accepted knowledge of practice.
Recommendations
• Research designs with better strength should be used to study the clinicopatholog ic behavior of upper aerodigestive tract SCC both nationwide and region specific.
• Institution based cancer registry should be improved and made easily accessible to researchers.
• Patient’s medical records should include through physical, intra- operative, radiologic and histopathologic reports.
• Nationwide policies on preventive measures and screening tools should be de- signed.
• Heart seeking behavior of the community should be improved by encouraging community bases awareness creation programs.
• Health care proffessionals should be trained to some basic office screening methods.
• Referral system should be made easy for patients with suspected cases.
References
- Shah, J. P. (1990). Patterns of cervical lymph node metastasis from squamous carcinomas of the upper aerodigestive tract. The American journal of surgery, 160(4), 405-409.
- Werner, J. A., Dünne, A. A., & Myers, J. N. (2003). Func- tional anatomy of the lymphatic drainage system of the upper aerodigestive tract and its role in metastasis of squamous cell carcinoma. Head & Neck: Journal for the Sciences and Spe- cialties of the Head and Neck, 25(4), 322-332.
- Vartanian, J. G., Pontes, E., Agra, I. M., Campos, O. D., Gonçalves-Filho, J., Carvalho, A. L., & Kowalski, L. P. (2003). Distribution of metastatic lymph nodes in oropharyn- geal carcinoma and its implications for the elective treatment of the neck. Archives of Otolaryngology–Head & Neck Sur- gery, 129(7), 729-732.
- Jones, A. S., Roland, N. J., Field, J. K., & Phillips, D. E. (1994). The level of cervical lymph node metastases: their prognostic relevance and relationship with head and neck squamous carcinoma primary sites. Clinical Otolaryngology & Allied Sciences, 19(1), 63-69.
- Kowalski, L. P., & Medina, J. E. (1998). Nodal metastases: predictive factors. Otolaryngologic Clinics of North America, 31(4), 621-637.
- Lindberg, R. (1972). Distribution of cervical lymph node me- tastases from squamous cell carcinoma of the upper respirato- ry and digestive tracts. Cancer, 29(6), 1446-1449.
- Villaret, A. B., Piazza, C., Peretti, G., Calabrese, L., Ansarin, M., Chiesa, F., ... & Nicolai, P. (2007). Multicentric prospec- tive study on the prevalence of sublevel IIb metastases in head and neck cancer. Archives of Otolaryngology–Head & Neck Surgery, 133(9), 897-903.
- Overholt, S. M., Eicher, S. A., Wolf, P., & Weber, R. S. (1996). Prognostic factors affecting outcome in lower gingival carci- noma. The Laryngoscope, 106(11), 1335-1339.
- Bark, R., Mercke, C., Munck-Wikland, E., Wisniewski, N. A., & Hammarstedt-Nordenvall, L. (2016). Cancer of the gingiva. European Archives of Oto-Rhino-Laryngology, 273(6), 1335-1345.
- Byers, R. M., Weber, R. S., Andrews, T., McGill, D., Kare, R., & Wolf, P. (1997). Frequency and therapeutic implications of “skip metastases” in the neck from squamous carcinoma of the oral tongue. Head & neck, 19(1), 14-19.
- Diaz Jr, E. M., Holsinger, F. C., Zuniga, E. R., Roberts, D. B., & Sorensen, D. M. (2003). Squamous cell carcinoma of the buccal mucosa: one institution's experience with 119 previ- ously untreated patients. Head & Neck: Journal for the Sci- ences and Specialties of the Head and Neck, 25(4), 267-273.
- Chung, E. J., Oh, J. I., Choi, K. Y., Lee, D. J., Park, I. S., KimJ. H., & Rho, Y. S. (2011). Pattern of cervical lymph node metastasis in tonsil cancer: predictive factor analysis of con- tralateral and retropharyngeal lymph node metastasis. Oral oncology, 47(8), 758-762.
- Candela, F. C., Kothari, K., & Shah, J. P. (1990). Patterns of cervical node metastases from squamous carcinoma of the oropharynx and hypopharynx. Head & neck, 12(3), 197-203.
- Cole, I., & Hughes, L. (1997). The relationship of cervical lymph node metastases to primary sites of carcinoma of the upper aerodigestive tract: a pathological study. Australian and New Zealand journal of surgery, 67(12), 860-865.
- Buckley, J. G., & MacLennan, K. (2000). Cervical node me- tastases in laryngeal and hypopharyngeal cancer: a prospec- tive analysis of prevalence and distribution. Head & Neck: Journal for the Sciences and Specialties of the Head and Neck, 22(4), 380-385.
- Timon, C. V., Toner, M., & Conlon, B. J. (2003). Paratracheal lymph node involvement in advanced cancer of the larynx, hypopharynx, and cervical esophagus. The Laryngoscope, 113(9), 1595-159
- Redaelli de Zinis, L. O., Nicolai, P., Tomenzoli, D., Ghizzardi, D., Trimarchi, M., Cappiello, J., ... & Antonelli, A. R. (2002). The distribution of lymph node metastases in supraglottic squamous cell carcinoma: therapeutic implications. Head & Neck: Journal for the Sciences and Specialties of the Head and Neck, 24(10), 913-920.
- Dahm, J. D., Sessions, D. G., Paniello, R. C., & Harvey, J. (1998). Primary subglottic cancer. The Laryngoscope, 108(5), 741-746.
- Helliwell, T. R. (2003). Evidence based pathology: squamous carcinoma of the hypopharynx. (Best Practice No 169). Jour- nal of Clinical Pathology, 56(2), 81-86.
- Lefebvre, J. L., Castelain, B., De Torre, J. L., Delobelleâ? Deroide, A., & Vankemmel, B. (1987). Lymph node invasion in hypopharynx and lateral epilarynx carcinoma: a prognostic factor. Head & Neck Surgery, 10(1), 14-18.
- Ho, F. C., Tham, I. W., Earnest, A., Lee, K. M., & Lu, J. J.(2012). Patterns of regional lymph node metastasis of naso- pharyngeal carcinoma: a meta-analysis of clinical evidence. BMC cancer, 12(1), 1-13.
- jackson1977.pdf. (n.d.).
- Cantù, G., Bimbi, G., Miceli, R., Mariani, L., Colombo, S., Riccio, S., ... & Rossi, M. (2008). Lymph node metastases in malignant tumors of the paranasal sinuses: prognostic val- ue and treatment. Archives of Otolaryngology–Head & Neck Surgery, 134(2), 170-177.
- Lavertu, P., Roberts, J. K., Kraus, D. H., Levine, H. L., Wood,B. G., Tucker, H. M., & Medendorp, S. V. (1989). Squamous cell carcinoma of the paranasal sinuses: the Cleveland Clin- ic experience 1977–1986. The Laryngoscope, 99(11), 1130-1136.
- Sowunmi, A. C., Ketiku, K. K., Olaniyi, P. A., Alabi, A. O.,Fatiregun, O. A., Asoegwu, N., ... & Blackson, K. A. (2015). Pattern of head and neck cancer in a tertiary institution in La- gos, Nigeria.
- Jing, J., Li, L., He, W., & Sun, G. (2006). Prognostic predic- tors of squamous cell carcinoma of the buccal mucosa with negative surgical margins. Journal of oral and maxillofacial surgery, 64(6), 896-901.
- Lin, H. W., & Bhattacharyya, N. (2009). Survival impact of nodal disease in hard palate and maxillary alveolus cancer. The Laryngoscope, 119(2), 312-315.
- Lim, Y. C., Koo, B. S., Lee, J. S., Lim, J. Y., & Choi, E. C(2006). Distributions of cervical lymph node metastases in oropharyngeal carcinoma: therapeutic implications for the N0 neck. The Laryngoscope, 116(7), 1148-1152.
- Calhoun, K. H., Fulmer, P., Weiss, R., & Hokanson, J. A. (1994). Distant metastases from head and neck squamous cell carcinomas. The Laryngoscope, 104(10), 1199-1205.
- Epidemiology, A., Anatomy, B., & Presentation, C. (n.d.). of the Mouth. 10–13.
- Huber, A. M., Mamyrova, G., Lachenbruch, P. A., Lee, J. A., Katz, J. D., Targoff, I. N., ... & Childhood Myositis Het- erogeneity Collaborative Study Group. (2014). Early illness features associated with mortality in the juvenile idiopathic inflammatory myopathies. Arthritis care & research, 66(5), 732-740
- Saxena, S., Sonkhya, N., Mishra, P., Yadav, R., & Bapna, A.S. (2001). Cervical node metastasis in Carcinoma of Pyriform Sinus: A prospective analysis of prevalence and distribution. Indian Journal of Otolaryngology and Head and Neck Sur- gery, 53(4), 273-276.
- McLaughlin, M. P., Mendenhall, W. M., Mancuso, A. A., Parsons, J. T., McCarty, P. J., Cassisi, N. J., ... & Million, R.R. (1995). Retropharyngeal adenopathy as a predictor of out- come in squamous cell carcinoma of the head and neck. Head & neck, 17(3), 190-198.