
Journal of Gynecology & Reproductive Medicine(JGRM)
ISSN: 2576-2842 | DOI: 10.33140/JGRM
Impact Factor: 1.247

Research Article - (2025) Volume 9, Issue 2
Prevalence and Associated Factors of Severe Degree Perineal Tear at Mekelle Public Hospitals, Tigray, Northern Ethiopia: A Seven Years Review
2Mekelle University College of Health, Depart- ment of Obstetrics and Gynecology, Mekelle, Ethiopia
3Mekelle University College of Health Science, Department of pharmacy, Mekelle, Ethiopia
Received Date: Mar 05, 2025 / Accepted Date: May 17, 2025 / Published Date: Jun 06, 2025
Copyright: ©©2025 Musie Negasi Gebreslase, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Gebreslase, M. N., Guesh, H., Negash, D., yeman. A., Berhe. Y. et al. (2025). Prevalence and Associated Factors of Severe Degree Perineal Tear at Mekelle Public Hospitals, Tigray, Northern Ethiopia: A Seven Years Review. J Gynecol Reprod Med, 9(2), 01-09.
Abstract
Introduction and Objectives: Obstetric anal sphincter injuries (OASIS) from perineal trauma during vaginal delivery result in poor maternal health outcomes and are common in low-resource settings and unattended births. Despite skilled hospital staff, some women still experience these injuries. This study evaluates the incidence and risk factors of third and fourth-degree perineal tears at Mekelle Public Hospitals in Tigray, Northern Ethiopia, from July 2016 to June 2023, aiming to fill gaps in understanding in resource-limited environments.
Methodology: An unmatched case-control study was conducted at Mekelle public hospitals in Ethiopia from July 1, 2016, to June 30, 2023. The study compared mothers who experienced severe perineal lacerations during vaginal delivery (cases) with those who did not (controls). All eligible cases from the seven-year period were included, and three controls per case, who delivered on the day of severe laceration repair, were selected. Data on sociodemographic, maternal, fetal, labor, delivery, and health provider characteristics were collected using structured questionnaires. Data were analyzed with epi-Data Management version 4.6 and SPSS version 23, employing bivariate and multivariate logistic regression. Statistical significance was determined with a p-value of <0.05, and associations were measured using odds ratios.
Results: The study included 361 participants (88 cases and 273 controls) with mean maternal ages of 26.2 and 26.9 years, respectively. The prevalence of severe perineal tears over seven years was 0.157% (1.57 per 1,000 vaginal deliveries). Risk factors for severe tears included rural residence, primiparity, gestational age ≥40 weeks, birth weight ≥3.5 kg, and instrumental delivery, while episiotomy was associated with a reduced risk.
Conclusion and Recommendation: At Mekelle Public Hospitals, severe perineal tears during vaginal delivery were linked to primiparity, instrumental delivery, fetal weight ≥ 3.5kg, gestational age ≥ 40 weeks, and rural residence. Mediolateral episiotomy reduced the risk. Regular monitoring and continuous training for birth attendants are essential to improve outcomes.
Keywords
Ai-Driven Renewable Energy, Smart Grid Optimization, Energy Forecasting, Sustainable Power Systems, Grid Resilience, Machine Learning in EnergyIntroduction
Vaginal delivery is well known to be associated with anal sphincter injury. Soft tissue organs in the genital tract and the adjacent organs can be traumatized during childbirth due to an episiotomy, spontaneous laceration or both [1]. A perineal tear is defined as a break in the continuity of either the perineal skin, mucosa, muscles/ connective tissues, anal sphincter complex and or rectal mucosa [2]. The perineal tear is classified according to the Royal College of Obstetrics and Gynecology as the first degree, which involves only the perineal skin and mucosa, a second degree, which involves the perineal muscles, third degree, which involves internal and external anal sphincter muscles and fourth degree involving the anal epithelium and rectal mucosa. Third-degree perineal is further subdivided into 3A if less than 50% of the external anal sphincter is involved, 3B if more than 50% and 3C if the internal anal sphincter is involved. First and second perineal tears are considered mild degree perineal tears, however, third and fourth are severe degree perineal injury or obstetric anal sphincter injury complex (OASI) [3]. Failure to appropriately distinguish between the degrees of perineal tears will result in deficient management [4] and hence result in short-term morbidities like perineal pain, which could result in acute urinary retention and difficulty of defecation in the immediate postpartum period, abscess formation, and wound breakdown, and long-term morbidities like rectovaginal fistula, chronic perineal pain, dyspareunia, and delayed sexual intercourse, as mentioned in various studies [5, 6]. Anal incontinence is the most worrisome complication associated with a two-fold to three- fold greater risk of having subsequent anal incontinence, which occurs in 7 to 61% of cases [7].
According to a WHO global retrospective study the prevalence of third-degree and fourth-degree perineal tear was found to range from 0.1% to 15% at the country level [8].
The risk factors for perineal tear consistently highlighted in previous studies are: -duration of the second stage of labor>1hours null parity fetal weight ≥ 3.5kg fetal weight ≥4.0 Kg assisted vaginal delivery occiput posterior position precipitate labor and Episiotomy has been linked to occurrence of perineal tear [5,6,8,9,12-14-22]. Generally, there are limited data on risk factors for severe degree perineal tears in our setting. Our study aimed at determining the risks factors for perineal tear among women having vaginal delivery at Mekelle Public Hospitals, Tigray Ethiopia. The findings will inform policy formulation and clinical practices geared to enhance better management and prevention of obstetric perineal tear.
Methods
Study Design and Setting
A retrospective unmatched case-control study reviewed records from mothers who delivered vaginally at Ayder Comprehensive Specialized Hospital and Mekelle General Hospital between July 1, 2016, and June 30, 2023, to examine the prevalence and risk factors of severe perineal tears. Ayder serves over 8 million people, with approximately 5,000 annual deliveries and facilities for low- and high-risk mothers, three operating rooms, and a neonatal care unit. Mekelle, one of the oldest regional hospitals, averages 400 deliveries per month, staffed by 30 midwives and 6 delivery couches, with rotating residents from Ayder. Both hospitals are crucial for maternal and neonatal health in their regions.
Study Population
The study population were records of all mothers delivered vaginally who were managed for severe degree perineal tear at Mekelle public hospital during the study period (July 1, 2016 to June 30, 2023).
Eligibility Criteria
All mothers who delivered vaginally after 28 weeks of gestation and were managed for severe perineal tear at Mekelle public hospitals between July 1, 2016, and June 30, 2023, were included in this study. Charts of mothers with severe perineal tears that had incomplete documentation or were lost were excluded from the study.
Sample-Size and Sampling Techniques
Sample Size Determination and Statistical Methods
The sample size was calculated using Epi-Info version 7 Statically for an unmatched case-control study, based on previous research in Ethiopia that identified birth weight of 3.5 kg and above as a risk factor for severe perineal laceration. The calculation assumed an 80% power (1 - β), an odds ratio of 2.11, 27.5% exposure among controls, a 3:1 control-to-case ratio, and a 95% confidence level. Ultimately, a total of 361 participants were included, consisting of 88 cases and 273 controls. A seven-year record from operating rooms and delivery registration books was reviewed to identify cases of severe perineal tear. Out of 95 medical records, 88 cases were eligible for the study. For each case, three controls who delivered vaginally on the same day as the severe perineal tear occurred and met the inclusion criteria were selected.
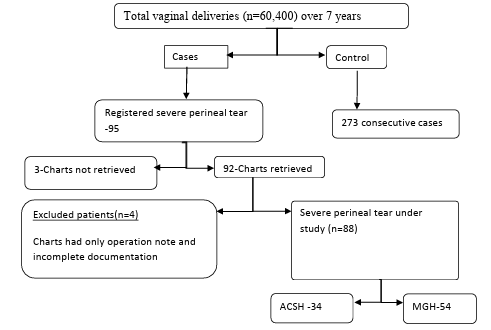
Figure1: Flow Diagram of Study Participants, Ayder Comprehensive Specialised Hospital and Mekelle General Hospital, Mekelle, Northern Ethiopia, 2016–2023
Variables and Measurements
The dependent variable in this study was severe perineal laceration, coded as (yes = 1, no = 0). The independent variables included maternal age, address, religion, length of the second stage of labor, precipitated labor, parity, gestational age, birth weight, instrumental delivery (forceps or vacuum), induction of labor, shoulder dystocia, persistent occiput posterior position, episiotomy, and the qualification of the birth attendant.
Case Definition
A case is defined as a mother who delivered vaginally at or beyond 28 weeks of gestation and experienced a severe perineal tear involving the anal sphincter muscle and anorectal mucosa. In contrast, a control is defined as a mother who delivered vaginally at or beyond 28 weeks of gestation without severe perineal laceration.
The diagnosis of severe perineal tear was made by a senior resident, with confirmation by a gynecologist or obstetrician for final diagnosis and repair, typically performed in the operating room. Data collection involved two Bachelor of Science midwives and two third-year senior residents, with the principal investigator (PI) overseeing the entire process. Variables were extracted using a pretested structured questionnaire and analyzed with Epi Data version 4.6, drawing information from patient cards, partographs, delivery logbooks, and operating room logbooks. Data quality was ensured through training and a pilot study.
Data Analysis
Data was entered into Epi Data Management version 4.6 and exported to SPSS version 23 for analysis. Frequency distribution was used to describe participant characteristics, while comparisons for categorical variables were made using the Chi-square test. Bi- variable logistic regression identified candidate variables, with those significant at p ≤ 0.25 included in the multivariable analysis. The final model was determined using multivariable binary logistic regression, where variables with p < 0.05 were considered significant. Model fit was assessed using the Hosmer-Lemeshow goodness-of-fit test (p > 0.05 indicating a good fit), and odds ratios with 95% confidence intervals were reported to measure the strength of association.
Operational Definitions and Terminologies
• Severe Perineal Tear/Laceration: Refers to third and fourth- degree perineal tears.
• Mekelle Public Hospitals: Includes Ayder Comprehensive Specialized Hospital and Mekelle General Hospital.
• Prolonged Second Stage of Labor (SSOL): Defined as primipara (first-time mothers) having labor lasting 2 hours or more, and multipara (women who have had more than one baby) lasting 1 hour or more.
• Precipitated Labor: Delivery occurring within three hours of the onset of regular uterine contractions.
• Multiparity: Refers to the delivery of more than one baby.
• Incomplete Chart: Charts that contain only an operation note or only a delivery summary.
• Mediolateral Episiotomy: A surgical incision made at an angle to the vaginal towards the side to facilitate delivery.
Ethical Clearance
Ethical approval was obtained from the Institutional Review Board (IRB) of Mekelle University, College of Health Sciences, and the ethical approval number is MU-IRB 2051/2023. Since this was a retrospective study, consent from patients could not be obtained. However, the patient’s profile and patient data were fully anonymized. After reviewing the protocol for this study, the IRB waived the requirement of informed consent.
Results
Out of the total delivery for the last 7 years in Mekelle Public Hospitals, 60,400 were vaginal deliveries (25,250 at ACSH and 35,150 at MGH). 95 cases of severe degree perineal tears were recorded in the operation registration book over the course of the 7-year study period at the Ayder Comprehensive Specialized Hospital and College of Health Science as well as the Mekelle General Hospital. A total of 88 charts were collected, 34 (38.6%) from ACSH and 54 (61.4%) from Mekelle General Hospital, after excluding mothers who did not meet the inclusion criteria. Three of the remaining seven charts couldn't be located, and four charts had to be removed due to inadequate documentation. Mothers who gave birth vaginally on the day that a severe degree perineal tear was repaired were included as controls. The prevalence of severe degree perineal tear over a 7 years study in both hospitals was 0.157 % (1.57/1000 vaginal deliveries).
Socio-Demographic Characteristics of Participants
The majority of women were identified in the 17–30 age range in both groups. The mean maternal age of cases and controls was 26.2 ± 5 (SD) years and 26.9 ± 5.6 (SD) years, respectively. The majority of cases, 68 (77.3%), and controls, 245 (89.7%), were urban dwellers from the Tigray region. (Table 1).
Maternal, Fetal, And Delivery-Related Characteristics of Cases and Controls
Out of 361 participants, 32.4% were nulliparous. About 85 (96.6%) cases and 267 (97.8%) controls had antenatal care, with more than half of the controls having their ANC follow-up at their nearby health center. The pattern of gestational age at delivery: 35 (39.8%) of cases and 175 (64.1%) controls were at 37 to 39 weeks, whereas 45 (51.1%) cases and 58 (21.2%) were delivered at 40-42 weeks. 8 cases had unknown gestational age even from the third trimester.
Labor was initiated with induction in 6 (6.8%) cases and 14 (5.1%) controls. Episiotomy was performed in 110 (30.5%) of the mothers in the study, with a much higher incidence in the control group in 92 (33.7%) patients compared with the severe degree perineal tear group. Instrumental delivery was done in 10 (11.4%) cases and 14 (5.1%) controls. About 40 (45.5%) of cases and 68 (24.9%) of control neonates were between 3.5 and 3.99 kg, whereas 14 (15.9%) cases and 32 (11.7%) control neonates were 4 kilograms and above. Labor was not attended on 9 (10.2%) of cases and 20 (7.3%) controls; from the attended labor most of the cases (83.3%) and controls (85.4%) were attended by midwifery, whereas the rest were attended by Residents. In 61 (69.3%) of the cases and 169 (61.9%) of the controls, labor was at nighttime (Table 2).
The Risk Factors Associated with Severe Perineal Tear
Both bivariate and multivariate logistic regression analyses revealed that rural dwelling, primiparity, and birth weight of 3.5 kg and above and gestational age of 40 weeks and above were associated with severe perineal tear, whereas mediolateral episiotomy on current delivery was associated with reduced risk in severe perineal tear (Table 3).
|
Variable |
|
Cases (N, %) |
Controls (N, %) |
|
Address |
Urban |
68(77.3%) |
245(89.7%) |
|
Rural |
20(22.7%) |
28(10.3%) |
|
|
Religion |
Christian |
86(97.7%) |
263(96.3) |
|
Muslim |
2(2.3) |
10(3.7%) |
|
|
Age |
17-24 |
37(42%) |
102(37.4%) |
|
25-30 |
33(37.5%) |
99(36.3%) |
|
|
>30 |
18(20.5%) |
72(26.4%) |
|
|
Institution |
ACSH |
34(38.6%) |
105(38.50%) |
|
MGH |
54(61.4%) |
168(61.50% |
Table 1 : Socio demographic characteristics of women with cases and controls, ACSH and MGH, July 2016- June, 2023
|
Characteristics |
Cases (N, %) |
Controls (N, %) |
|
|
Parity |
Primipara |
44(50.0%) |
73(26.7%) |
|
Multipara |
44(50.0%) |
200(73.3%) |
|
|
Gestational Age |
37-39 Weeks |
35(39.8%) |
175(64.1%) |
|
≥40 Weeks |
45(51.1%) |
58(21.2%) |
|
|
Unknown |
8(9.1%) |
40(14.7%) |
|
|
ANC |
Yes |
85(96.6%) |
267(97.8%) |
|
|
No |
3(3.4%) |
6(2.2%) |
|
Place of ANC |
ACSH |
14(16.3%) |
26(9.7%) |
|
MHG |
16(18.6%) |
73(27.2%) |
|
|
H/C |
50(58%) |
148(55.2%) |
|
|
Private |
5(5.8%) |
20(7.5%) |
|
|
History of Tear |
Yes |
8(9.1%) |
0 |
|
No |
80(90.9%) |
273(100%) |
|
|
Labor initiation |
spontaneous |
82(93.2%) |
259(94.9%) |
|
induction |
6(6.8%) |
14(5.1%) |
|
|
Labor Augmentation |
Yes |
4(4.5%) |
21(7.7%) |
|
No |
84(95.5%) |
252(92.3%) |
|
|
Precipitated labor |
Yes |
9(10.2%) |
22(8.1%) |
|
No |
66(75%) |
224(82.1%) |
|
|
unknown |
13(14.8%) |
27(14.8%) |
|
|
Prolonged SSOL |
Yes |
9(10.2%) |
31(11.4%) |
|
No |
48(54.5%) |
117(42.9%) |
|
|
unknown |
31(35.2%) |
125(45.8%) |
|
|
Episiotomy |
Yes |
19(21.6%) |
92(33.7%) |
|
No |
69(78.4%) |
181(66.3%) |
|
|
Instrumental delivery |
yes |
10(11.4%) |
14(5.1%) |
|
No |
78(88.6%) |
259(94.9%) |
|
|
Type of Instrumental delivery |
forceps |
7(70.0%) |
4(26.7%) |
|
vacuum |
3(30%) |
11(73.3%) |
|
|
Fetal head position |
Occipitoanterior |
40(45.5%) |
192(70.3%) |
|
Occipitoposterior |
7(8.0%) |
16(5.9%) |
|
|
Unknown |
41(46.6%) |
65(23.8%) |
|
|
Was labor attended |
Yes |
79(89.8%) |
253(92.7%) |
|
No |
9(10.2%) |
20(7.3%) |
|
|
Who attended labor |
Resident |
13(16.5%) |
36(14.2%) |
|
Midwifery |
66{83.5%} |
217(85.4%) |
|
|
Timing of SSOL |
at night |
60{68.2%} |
166(60.8%) |
|
day time |
24(27.3%) |
104(38.1%) |
|
|
Unknown |
4(4.5%) |
3(1.1%) |
|
|
Birth weight |
2500-3500 gram |
34(38.6%) |
173(63.4%) |
|
3500-3999 gram |
40(45.5%) |
68(24.9%) |
|
|
≥4000 gram |
14(15.9%) |
32(11.7%) |
|
|
Neonatal gender |
Male |
55(62.5%) |
128(46.9%) |
|
female |
33(37.5%) |
145(53.1%) |
|
|
Neonatal status |
Alive |
87(98.9%) |
271(99.3%) |
|
Stillbirth |
1(1.1%) |
2(0.7%) |
|
|
1st min APGAR |
<7 |
7(8%) |
24(8.9%) |
|
|
≥7 |
80(92%) |
247(91.1%) |
|
5th min APGAR |
<7 |
4(4.6%) |
14(5.2%) |
|
|
≥7 |
83(95.4%) |
257(94.8%) |
|
Abbreviations: SSOL-Second stage of labor, APGAR-A-Appearance, P-Pulse rate, G-Grimace, A-Appearance, RR-Respiratory Rate, N, % = number and percentage |
|||
Table 2: Maternal, fetal and delivery related characteristics of cases and controls, ACSH and MGH, July 2016- June, 2023
|
Characteristics |
Cases (N, %) |
Controls (N, %) |
COR (95%CI) |
AOR (95%CI) |
P-value |
|
|
Address |
Urban |
68(77.3%) |
245(89.7%) |
1 |
1 |
|
|
Rural |
20(22.7%) |
28(10.3%) |
2.7(1.4-5.1) |
5.302(2.118-13.275) |
<0.001 |
|
|
Place of ANC |
ACSH |
14(16.3%) |
26(9.7%) |
2.5(1.06-5.7) |
3.270(0.852-12.551) |
0.084 |
|
MHG |
16(18.6%) |
73(27.2%) |
1.6(0.777-3.3) |
1.858(0.606-5.702) |
0.279 |
|
|
H/C |
50(58.1%) |
148(55.2%) |
1.9(0.62-5.75) |
0.811(0.191-3.437) |
0.776 |
|
|
private |
6(7.0%) |
21(7.8%) |
1 |
1 |
|
|
|
Parity |
Primipara |
44(50.0%) |
73(26.7%) |
2.7(1.67-4.5) |
4.7(2.2-9.8) |
<0.001 |
|
Multipara |
44(50.0%) |
200(73.3%) |
1 |
1 |
|
|
|
Gestational Age |
37-39 wk |
35(39.8%) |
175(64.1%) |
1 |
|
|
|
40-42 wk |
45(51.1%) |
58(21.2%) |
3.88(2.3-6.6) |
5.1(2.5-10.3) |
<0.001 |
|
|
Unknown* |
8(9.1%) |
40(14.7%) |
|
|
|
|
|
Precipitated labor |
yes |
12(13.6%) |
19(7.0% |
2.14(0.98-4.65) |
2.9(0.98-8.5) |
0.053 |
|
No |
64(72.7%) |
217(79.5% |
1 |
1 |
|
|
|
unknown* |
9(10.2%) |
40(14.7%) |
|
|
|
|
|
Episiotomy |
yes |
19(21.6%) |
92(33.7%) |
0.54(0.307-0.95) |
0.266(0.109-0.649) |
0.004 |
|
No |
69(78.4%) |
181(66.3%) |
1 |
1 |
|
|
|
Instrumental delivery |
yes |
10(11.4%) |
14(58.3%) |
2.36(1.01-5.53) |
5.07(1.2-15.9) |
0.024 |
|
No |
78(88.6%) |
258(94.9%) |
1 |
1 |
|
|
|
Timing of SSOL |
at night |
60{68.2%} |
166(60.8%) |
1.5(0.92-2.7) |
1.4(0.67-3.2) |
0.35 |
|
day time |
24(27.3%) |
104(38.1%) |
1 |
1 |
|
|
|
Unknown |
4(4.5) |
3(1.1%) |
|
|
|
|
|
Birth weight |
2500-3499gram |
34(38.6%) |
173(63.4%) |
1 |
1 |
|
|
>3499 gram |
54(61.4%) |
100(36.6%) |
2.7(1.68-4.5) |
2.23(1.14-4.5) |
0.02 |
|
|
Neonatal gender |
Male |
55(62.5%) |
128(46.9%) |
1.8(1.15-3.1) |
1.640(0.82-3.3) |
|
|
female |
33(37.5%) |
145(53.1%) |
1 |
1 |
|
|
Table 3: Bivariate and Multivariate Analysis Results of Maternal, fetal and delivery related characteristics of cases and control, ACSH and MGH, July, 2016- June, 2023
Discussion
There were 95 severe perineal tears out of 60,400 vaginal deliveries, representing 0.157 percent of all vaginal deliveries. Bivariate and multivariate analyses identified rural residence, gestational age ≥40 weeks, primiparity, male neonates, instrumental delivery, and birth weight ≥3.5 kg as risk factors. mediolateral episiotomy was found to be protective. The outcome of this study revealed that out of total vaginal deliveries, the percentage of third- and fourth-degree perineal tears was 0.157%. Our finding is not only lower than other African countries like southwest Uganda (6.6%) but also from developed countries like Germany (1.8%) [5,23]. This implies a problem of documentation and underdiagnosis of our cases. This report may be misleading, because the lower prevalence is not due to better preventive measures we use in our setup. This calls for better examination of all patients after delivery and proper grading and documentation of all patients with severe perineal lacerations.
Our study found that being primiparous was significantly associated with severe degree perineal tear, which is 4.7 times compared to control groups. Indeed, parity is a well-known risk factor for third- and fourth-degree perineal tears in different studies (10, 19, 53, 54, 55, 56). The possible explanation for this increased risk could be due to the lack of elasticity of the perineal tissue in primiparas, which is the main factor, as previous deliveries may make the perineal tissues more stretchable and less susceptible to injury during delivery, and others speculated that the biomechanical stress of parturition, which can produce micro-rupture or rupture, decreases with parity (19, 57, 58). In contrast to our finding, a study done in Debremarkos, Ethiopia, did not show a significant association between parity and severe degree perineal tear [6]. This finding calls for a high index of suspicion for OASIS among prime gravidas to prevent their occurrence and/or facilitate their early recognition and prompt repair.
Instrumental delivery, particularly forceps delivery, is significantly associated with severe perineal tear, like previous studies from various centers [24-26]. Forceps are designed to widen the birth canal to accommodate the foetal presenting part while increasing the risk of injury to the pelvic floor, and it is important to note that instrumental deliveries are likely performed in labour dystocic or for immediate foetal extraction, where both could increase the risk of severe perineal trauma. Abdominal delivery is better than instrumental deliveries that do not fulfil the prerequisites of instrumental deliveries. The acquisition of appropriate skills and the performance of generous mediolateral episiotomy might be mentioned as important preventive strategies.
Gestational ages of 40 weeks and above were associated with a 5.1-fold risk of third- and fourth-degree perineal tears compared to 37-39 weeks of gestation, which is comparable with other studies [27,16]. Al-Ghamdi et al. 2018 have found gestational age above 40 weeks is associated with severe degree perineal tear (28), and it was reported that gestational age might be directly related to perineal injuries with an increase in the risk of OASIS of 77% each week of gestation [27]. The possible explanation for the risk of severe degree perineal tear with increased gestational age could be due to increased birth weight as gestational age advances. In contrast to this, a case-control study from Cape Town Tertiary Hospital (SA) showed no relationship between gestational age and severe degree perineal tears [29]. Particular attention should be given to mothers who are primigravida and postdate; labour should be strictly attended, and strict assessment of the perineum after delivery is advisable.
Birth weight ≥3.5 kg was associated with a significantly higher chance of severe perineal tear. This study is in line with a study done in Riyadh, Saudi Arabia, Madrid, Spain and Debre Markos, Ethiopia [16,26,28]. This could be explained by the biochemical stress imposed by the unproportioned foetal size to the maternal birth canal outlet. Contrary to our finding, in a study conducted at Tygerberg Hospital in Cape Town, birth weight was not significantly associated with severe degree perineal tear [29]. This might be due to a difference in foetal weight categorisation or might be due to low infant birth weight. The finding reminds us that birth weight assessment before labour is important to select patients regarding the mode of delivery. This may call for a particular selection of birth weight for abdominal delivery that suits our setup. And also, the knowledge of foetal weight helps to perform appropriate episiotomy at the appropriate time to prevent severe perineal lacerations.
Out of the mothers with severe degree perineal tears, 20 (22.7%) of them were from rural residences compared to the control group's 28 (10.3%). Mothers from rural areas are at high risk of severe degree perineal tear, which is 5.3 times riskier compared to mothers from the control group. 4 (44.4%) of severe degree laceration cases from rural areas had prolonged second stage of labour compared to 7 (22.6%) of controls, although 35.5% of cases had unknown duration of the second stage in which prolongation is possible.
The Possible expiation could be that laboring mothers from rural areas are more likely to come with the prolonged second stage of labour in which the increase of genital tract oedema can prevent optimal perineal tissue distention and compliance during the descent of the presenting part [30]. This finding highlights that mothers referred from remote distances with prolonged labour not only have their perinatal conditions compromised, but they are also at risk of severe degree perineal laceration with known long-term morbidities. A case-control study in Ethiopia showed no significant association between residence and severe degree perineal tear lacerations [6].
Almost half of mothers in Ethiopia will undergo episiotomy during childbirth [31]. The finding of our study showed the protective effect of episiotomy for severe degree perineal tear with an aOR of 0.26 and a 95% CI of 0.13-0.7. This finding is similar to a study done in Poland by Grażyna Gebuza et al. (2018) and to a systematic review by Verghese et al. (2016) on mediolateral episiotomy [32- 33]. At our institution, we perform a mediolateral episiotomy, and we believe that in women with a background risk of severe perineal laceration, episiotomy may play a role in reducing the trauma by the foetal head on the integrity of perineal tissue and prevent severe perineal lacerations. Our finding is in contrast to studies in Debremarkos, Ethiopia and Southwestern Uganda [5,6]. This could be explained by the method of episiotomy used, the angle of episiotomy, and the indications for the episiotomy, like difficulty in deliveries, rather than the episiotomy itself.
Strength and Limitations of The Study
The strength of this study is that it is an extended 7-year study that included cases and was a case-control study to see the association of risk factors with severe degree perineal tear. The limitations of this study are the fact that it is retrospective in nature, and poor diagnosis and documentation of cases underestimate the real information of cases.
Conclusion
The risk factors for perineal tear among women delivering at Mekelle Public Hospitals are being primiparous, assisted vaginal delivery, foetal weight ≥3.5 kg, mothers from rural areas, and gestational age ≥40 weeks. Our study found that mediolateral episiotomy is protective against severe degree perineal tear, which means for those at higher risk, like operative vaginal delivery, primiparous, and macrosomia babies, it is good to lower our threshold for mediolateral episiotomy.
Abbreviations
N, % - Number and Percentage
COR-Crude Odd Ratio
AOR-Adjusted Odd Ratio
CI-Confidence Interval
ACSH- Ayder Comprehensive Specialized Hospital
MGH- Mekelle General Hospita
References
- Groutz, A., Hasson, J., Wengier, A., Gold, R., Skornick- Rapaport, A., Lessing, J. B., & Gordon, D. (2011). Third- and fourth-degree perineal tears: prevalence and risk factors in the third millennium. American journal of obstetrics and gynecology, 204(4), 347-e1.
- Kettle, C., & Tohill, S. (2008). Perineal care. BMJ clinical evidence, 2008.
- THe management of third- and fourth-degree perineal tears. .Green-top guideline ,RCOG,. 2015;29:1905-11.
- Ah, S. (1993). Anal-sphincter disruption during vaginal delivery. N Eng J Med, 329, 1905-1911.
- Ali, M., Migisha, R., Ngonzi, J., Muhumuza, J., Mayanja, R., Joe Lapat, J., ... & Kayondo, M. (2020). Risk factors for obstetric anal sphincter injuries among women delivering at a tertiary hospital in Southwestern Uganda. Obstetrics and Gynecology International, 2020(1), 6035974.
- Worede, D. T., Alemu, S., & Tsegaye, T. B. (2020). Risk factors for severe perineal laceration among vaginally delivered mothers in public hospitals in Ethiopia: Unmatched case control study. Primary Health Care, 10(5), 350.
- Antonakou, A. (2018). The long-term physical, emotional and psychosexual outcomes related to anal incontinence after severe perineal trauma at childbirth. European Journal of Midwifery, 2.
- Hirayama, F., Koyanagi, A., Mori, R., Zhang, J., Souza, J. P., & Gülmezoglu, A. M. (2012). Prevalence and risk factors for third-and fourth-degree perineal lacerations during vaginal delivery: a multi-country study. BJOG: An International Journal of Obstetrics & Gynaecology, 119(3), 340-347.
- No, G. T. G. (2015). The management of third-and fourth- degree perineal tears. MIDIRS, 2, 9.
- Smith, L. A., Price, N., Simonite, V., & Burns, E. E. (2013). Incidence of and risk factors for perineal trauma: a prospective observational study. BMC pregnancy and childbirth, 13, 1-9.
- Cola, A., Frigerio, M., Manodoro, S., Verri, D., Interdonato,M. L., Nicoli, E., ... & Milani, R. (2016). Third and fourth degree perineal tears: incidence and risk factors in an Italian setting. European Journal of Obstetrics and Gynecology and Reproductive Biology, 206, e27.
- Hsieh, W. C., Liang, C. C., Wu, D., Chang, S. D., Chueh, H. Y., & Chao, A. S. (2014). Prevalence and contributing factors of severe perineal damage following episiotomy-assisted vaginal delivery. Taiwanese Journal of Obstetrics and Gynecology, 53(4), 481-485.
- Al-Ghamdi, T., Al-Thaydi, A. H., Chamsi, A. T., & Mardawi,E. A. (2018). Incidence and Risk Factors for Development of Third-and Fourth-Degree Perineal Tears: A Four-Year Experience in a Single Saudi Center. J Women's Health Care, 7(2), 423.
- Hoque, A. M., Hoque, M. E., & Hal, G. V. (2021). Incidence, trends and risk factors for perineal injuries of low-risk pregnant women: Experience from a midwife run obstetric unit, South Africa. African Journal of Reproductive Health, 25(4), 52-62.
- Gebuza, G., Kazmierczak, M., Gdaniec, A., Mieczkowska, E., Gierszewska, M., Dombrowska-Pali, A., ... & Malenczyk, M. (2018). Episiotomy and perineal tear risk factors in a group of 4493 women. Health care for women international, 39(6), 663-683.
- Barca, J. A., Bravo, C., Pintado-Recarte, M. P., Cueto- Hernández, I., Ruiz-Labarta, J., Cuñarro, Y., ... & De León- Luis, J. A. (2021). Risk factors in third and fourth degree perineal tears in women in a tertiary centre: An observational ambispective cohort study. Journal of Personalized
- Medicine, 11(8), 685.Smith, L. A., Price, N., Simonite, V., & Burns, E. E. (2013). Incidence of and risk factors for perineal trauma: a prospective observational study. BMC pregnancy and childbirth, 13, 1-9.
- Harmanli MD, O. (2006). Is severe perineal damage increased in women with prior anal sphincter injury?.
- Groutz, A., Cohen, A., Gold, R., Hasson, J., Wengier, A., Lessing, J. B., & Gordon, D. (2011). Risk factors for severe perineal injury during childbirth: a case–control study of 60 consecutive cases. Colorectal Disease, 13(8), e216-e219.
- Sultan, A. H., Kamm, M. A., Hudson, C. N., & Bartram, C. I. (1994). Third degree obstetric anal sphincter tears: risk factors and outcome of primary repair. Bmj, 308(6933), 887-891.
- Fouelifack, F., Essiben, F., Kemadjou, L., Fouedjio, J., Fouogue, J., & Mbu, R. (2017). Risk Factors of Genital Tract Lacerations at Yaoundé Central Hospital—Cameroon: A Case Control Study. British Journal of Medicine and Medical Research, 20, 1-8.
- Melamed N GO, Eisne M, Wiznitzer A, Wasserberg N, Yogev Y,, . Third and Fourth degree Perineal Tears-Incidence and and Risk Factors, Tel Aviv, Israel. j Maternal Fetal Neonatal Medicine, . 2013;26 (7):660-4.
- Blondel, B., Alexander, S., Bjarnadóttir, R. I., Gissler, M.,Langhoff-Roos, J., Novak-Antolic, Z., ... & Macfarlane,A. (2016). Variations in rates of severe perineal tears and episiotomies in 20 European countries: a study based on routine national data in Euro-Peristat Project. Acta obstetricia et gynecologica Scandinavica, 95(7), 746-754.
- Anglim, B., Kelly, L., & Fitzpatrick, M. (2019). Risk factors and outcome of repair of obstetric anal sphincter injuries as followed up in a dedicated perineal clinic. International urogynecology journal, 30, 1649-1655.
- Simic, M., Cnattingius, S., Petersson, G., Sandström, A., & Stephansson, O. (2017). Duration of second stage of labor and instrumental delivery as risk factors for severe perineal lacerations: population-based study. BMC pregnancy and childbirth, 17, 1-8.
- Gommesen, D., Nohr, E. A., Drue, H. C., Qvist, N., & Rasch,V. (2019). Obstetric perineal tears: risk factors, wound infection and dehiscence: a prospective cohort study. Archives of gynecology and obstetrics, 300, 67-77.
- Beckmann, M. M., & Garrett, A. J. (2006). Antenatal perineal massage for reducing perineal trauma. Cochrane Database of Systematic Reviews, (1).
- Al-Ghamdi, T., Al-Thaydi, A. H., Chamsi, A. T., & Mardawi,E. A. (2018). Incidence and Risk Factors for Development of Third-and Fourth-Degree Perineal Tears: A Four-Year Experience in a Single Saudi Center. J Women's Health Care, 7(2), 423.
- Juul, L., & Theron, G. B. (2011). Risk factors for third-and fourth-degree perineal tears during vaginal delivery. Urogynaecologia, 25(1), e2.
- Fouelifack, F., Essiben, F., Kemadjou, L., Fouedjio, J., Fouogue, J., & Mbu, R. (2017). Risk Factors of Genital Tract Lacerations at Yaoundé Central Hospital—Cameroon: A Case Control Study. British Journal of Medicine and Medical Research, 20, 1-8.
- Deyaso, Z. F., Chekole, T. T., Bedada, R. G., Molla, W., Uddo,E. B., & Mamo, T. T. (2022). Prevalence of episiotomy practice and factors associated with it in Ethiopia, systematic review and meta-analysis. Women's Health, 18, 17455057221091659.
- Gebuza, G., Kazmierczak, M., Gdaniec, A., Mieczkowska, E., Gierszewska, M., Dombrowska-Pali, A., ... & Malenczyk, M.(2018). Episiotomy and perineal tear risk factors in a group of 4493 women. Health care for women international, 39(6), 663-683.
- Verghese, T. S., Champaneria, R., Kapoor, D. S., & Latthe, P.M. (2016). Obstetric anal sphincter injuries after episiotomy: systematic review and meta-analysis. International urogyne- cology journal, 27, 1459-1467.