



Research Article - (2020) Volume 5, Issue 2
Prevalence and Associated Factors of Hypertension among Assosa town, Western Ethiopia, 2018
Received Date: Jun 03, 2020 / Accepted Date: Jun 10, 2020 / Published Date: Jul 21, 2020
Copyright: ©Lalisa M Gadisa. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Hypertension, the global first and third risk for mortality and disease burden respectively, is recording an increment in Sub-Saharan Africa countries. This study aimed to identify prevalence and its associated risk factor of Hypertension in the Assosa town.
Objective: To identify prevalence and factors associated with hypertension in the study area to increase it’s prevention and control methods.
Methods & materials: Institutional based cross sectional study design with quota non-probability sampling technique was conducted among patients visited OPD units of Assosa General Hospital (AGH) andAssosa Health Center(AHC) fromMarch to June 2018. All outpatients were included. To collect data, pre-tested structured questionnaire and face to face interviews were used. Components ofstatisticalresearch software SPSS version-21 like frequency table, chi-square test of independence & logistic regression was used to enter, analyze, summarize and characterize disease and associated factors data.
Result: The study was conducted among 194 participants(152 from AGH and 42 from AHC) with 102 males and 92 females. Prevalence of hypertension among patients visited outpatient units of Assosa General Hospital and Assosa Health Center was 17.5%, and was slightly highest in male than female. Associated factors for hypertension among patients visited OPD units of AGH & AHC were history of hypertension in the family (CI=95% and COR=4.497(1.133-17.844) and being private employee (CI=95% and COR=0.0017(0.001-0.407).
Conclusion & recommendation: Prevalence of HTN in the Assosa town, was low and influenced by some risk factors like work status and previousfamily history of hypertension. Even if usual usage ofsalt and using vegetable oil was not associated factor, being private employee were independent factor of HTN. In-depth study is recommended for further investigation. To increase preventative methods of HTN, health education supported by mass media, illustrative posters and anotherstrategies at every government & non government work sector are recommended.
Keywords
Prevalence, Hypertension, OPD, AGH, AHC
Abbreviations and Acronyms
AGH: Assosa General Hospital
AHC: Assosa Health Center
AOR: Adjusted Odd Ratio
B/G/R: Benishengul-Gumuz Region
CI: Confidence Interval
COR: Crude Odd Ratio
CVD: Cardio vascular disease
DM: Diabetes Mellitus
HTN: Hypertension
IESO: Integrated Emergency Surgical Officer
JUSH: Jimma University Referral Hospital
LMIC: Low Middle Income Countries
MMD: Major Depression Disorder
Mmhg: Millimeter of Mercury
MRFIT: Multiple Risk Factor Intervention trial
OPD: Out Patient Department
PHO: Public Health Officer
STEPs: Step wise approach to surveillance
USA: United States of America
WHO: World Health Organization
Introduction
Hypertension due to concomitant increment in its prevalence and risk of disease is global public health challenge. According to the 2010 data, global non-communicable disease reported that be- tween 1980 and 2008, number of hypertensive patient was hiked from six hundred million to one billion and it can be predicted to raise to 1.5 billion by the year 2025 [1]. Viewing from the angle of economic level, HTN is highly prevalent in the Low and Middle Income countries (LMIC). Globally, we lost about 9.4 million peo- ple by HTN every year [2]. Despite another fatal health risk and burden from high blood pressure is going upward across the world, impairing estimably around 1 billion, it is predicted to increases, especially in low, lower middle income countries than high income countries [3]. Among World Health Organization (WHO) coun- try-consideration for HTN based on tangible data, Africa scored highest prevalence with the prevalence of 46% which included combination of both sex groups. Blood pressure can be described by the two functionally interlinked fractional finding. These val- ues are called systolic blood pressure (SBP) and Diastolic blood pressure (DBP) which represents the upper and the lower value respectively.
The standard unit of blood pressure is millimeter mercury (mmhg). Though it has little insignificant difference based on dif- ferent reference, averagely blood pressure of between 90/60mmhg and 120/80mmhg is considered as normal; but, any record of below 90/60 and above 120/80 is abnormal and have high risk which may result death if not immediately controlled medically. Low arterial blood pressure is called hypotension; while high arterial blood pres- sure is called hypertension. Recording of blood pressure between 120/80 mmHg to 139/89 is termed as pre-hypertension and any record above 140/90 is considered high. An elevation of both blood pressure i.e, systolic and diastolic blood pressure increases the risk of developing heart disease, kidney disease, hardening of the arter- ies, eye damage, and a stroke which is called end organ damage as it is the end result of chronic high blood pressure. Sometimes HTN is called ‘Silent Killer’ by some clinicians because most of the time, it remains silence in the early stage and manifests symptoms only after damaging body organ and finally results with death. These symptoms are usually a result of end-organ damage and the pre- sentation depends on the organ that is affected [4]. Essential hyper- tension expresses another circumference of hypertension in which cause of hypertension is unknown and comprises 90% among total prevalence of the condition [5]. Cardiovascular diseases are group of diseases which are due to impairment of heart and veins of the body organ. They are major risk of death in the developed coun- try and Hypertension is their major risk factor. According to data of Multiple Risk Factor Intervention Trial (MRFIT), in the United States of America (USA), likelihood of mortality from coronary heart disease among mild to severe hypertensive patient was varied between 2.3-6.9 higher than among those who have normal blood pressure; and the likelihood of developing stroke among hyper- tensive patients were varied between 3.6-19.2 higher than those of normal blood pressure. And additionally, in general population of USA, 23% - 25.6% of death from coronary artery disease and 6.8%-40% of death from stroke could be preventable if hyperten- sion was prevented. Opposite to direct logical prediction, rather than developed countries, developing countries are more affected by non-communicable diseases.
WHO estimated that about 80% of chronic disease deaths occur in low and middle income countries and in Sub Saharan countries, hypertension causes to 7.5 million deaths, among about 12.8% of the total annual deaths [6,7]. In the developed countries, numerous studies have been conducted to estimate frequency of HTN but in the low incoming countries like Ethiopia due to more attention is given to communicable disease, there is data shortage on preva- lence and its associated factors in entire population and specifically among vulnerable groups who are more predisposed to HTN and other related disorders than general population. Previously, there was no study conducted on the Assosa general hospital (AGH) and Assosa health center (AHC) as well as in Assosa town community to represent the study population with the same topic. Thus the purpose of this study is to identify the prevalence and it’s associated risk factors of hypertension in Assosatown.
Materials and Methods
Study setting
Two study institution that were used to conduct this study were: AGH which have been serving population of more than 750,000 and AHC which have been serving more than 30,000 populations.
Since these health institutions are the only governmental health institutions that are found in Assosa town, capital city of Benis- hangul-Gumuz regional state, they were purposely selected to rep- resent prevalence and related risk factors of HTN among Assosa town population. Assosa town is located on the North western of Ethiopia by the 675km distance from Addis Ababa, capital of the Ethiopia.
AGH has now 22 Medical doctors, 96 nurses, 15 midwifes, 4 IE- SOs, 2 Anaesthesia’s, 2 Psychiatrics, 12 Pharmacicts and 3 general Specialists. And it has 4 wards namely, Medical ward (30 beds), surgical ward (24 beds), Pediatric ward (25 beds) and Maternity ward (26 beds). It has also 13 OPDs which is serving averagely 300- 500 outpatients daily. AHC has 31 Nurses, 9 Midwifes, 5 PHOs, 3 Pharmacists and 3 Medical doctors with 10 OPDs
Study design and sample size
An institution based cross sectional study was conducted at Assosa general hospital& Assosahealth center. Samplesizewas determined by using statistical formula, n =Z2Pq/â??2. taking confidence inter- val 95%(1.96), Proportion of hypertension 13.2% (0.132) which was taken from hospital based cross sectional study conducted on JUSH & margin of error as 0.05 and Assuming non-response rate as 10%, the final sample size would become, n=176+17.6=194 [8].
Sampling methodology
Proportional allocation was made for each health institution and quota non-probability sampling technique was used to include all patients visiting outpatient units of AGH and AHC to represent entire population of the town. Assosa general hospital and Assosa health center have 23,867 and 6,608 registered patients respectively within three months of the past year which have highest patient flow. Since 194 samples are required for this study, 152 samples from AGH and 42 from AHC were randomly selected using quo- ta nan-probability sampling method from all OPDs according to their willingness and eligibility criteria. Since all outpatients have different appointment duration, and time of this study is short, probability sampling method was not used. Prior to starting study question, the importance of the study was deeply informed and if they found difficult to participate they excluded from the study. If randomly selected patient was ineligible or not volunteer to par- ticipate, the next available patient was selected based on inclusion criteria until required sample size was met. The further illustration of used sampling methodology is shownbelow.
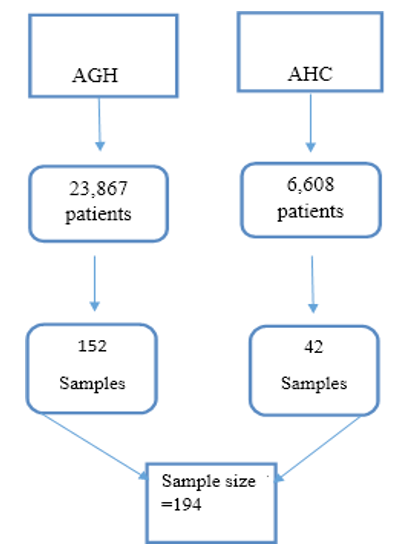
Figure1: Sampling methodolog
Selection of study subjects
Inclusion criteria
All out patients aged 18 years and above who were visiting outpa- tient units of AGH and AHC during the study period were enrolled in to study based on their willingness and eligibility to participate in the study.
Exclusion criteria
All outpatients who are presented with severe and critical medical conditions, mental disorder, traumatic and other emergency pa- tients were excluded from the study
Tools and techniques of the study
Face to face questionnaire was composed of open-ended and close- ended questions which was administered to collect data of socio- demography life style, genetic and family related factors & presence of other medical diseases or condition. The questionnaire was prepared by the English language and then translated to Am- haric version as the most respondents are speaker of Amharic lan- guage. Questions included in the questionnaire are adapted from World Health Organization STEP wise approach to surveillance (STEPS) instrument for collecting data on chronic diseases and their risk factors. After the interview, the study participant was al- lowed to rest (relax) for 15 minutes then two blood pressure mea- surements were taken three minutes apart in a sitting position and the average of the two reading was taken. The blood pressure was measured on the left upper arm. The participant was positioned in such a way that the left upper arm was at the same level with the heart. To minimize measurement and inter observer variability, digital BP machine was used throughout the study and all blood pressure measurements was done by one qualifiedperson.
Ethical consideration
Prior to data collection, formal ethical clearance letter was ob- tained from Assosa University, college of health science and re- search directorate bureau. Then as the request by the former let- ter, support letter was attained from B/G/R health bureau, Assosa, Benishangul-Gumuz region and from B/G health bureau. Final in- tegrated letter was sent to respective woreda health office and AGH and then to health center. In addition, before commencing data collection, informed consent was obtained from each participant after expressing objective the study purposely. For positively vol- unteered participants, it was also informed that they can terminate at anywhere in the face-to-face interview. All information collected from each respondent was kept confidential.
Definitions used
Hypertension: Is a condition in which arterial blood pressure is increased beyond it‘s normal value i.e., above 140/90mmhg and measured by mmhg.
Table 1: Classification of blood pressure
|
Classification |
Systolic value |
Diastolic value |
|
Hypotension |
<90 |
<60 |
|
Normal BP |
90-119 |
60-79 |
|
Prehypertension |
120-139 |
80-89 |
|
HTN stage 1 |
140-159 |
90-99 |
|
HTN stage 2 |
≥160 |
≥100 |
Physical activity: A condition in which body is move for the min- imum of at 10 minutes continuously to increase breathing rate and heart beat.
Prevalence: the number of all new and old cases of a disease or occurrences of an event during a particular period. Prevalence is expressed as a ratio in which the number of events is the numerator and the population at risk is the denominator.
Risk factor: is an independent variable which can associated with an increased risk of disease or infection. Sometimes, determinant is also used, being a variable associated with either increased or decreased risk
Data processing and analysis
Data was entered, cleaning & analyzing by using SPSS version-21. After raw data was entered in to SPSS, it was secured by comput- er password to save from losing. In order to check accuracy and missed value of data, frequency run procedure was performed on software. Lastly, data was coded to simplify for analysis.
Quantitative characteristics of data like frequency, mean, media and standard deviation were computed to quantify collected data. To test association between hypertension and independent vari- ables, binary logistic regression model was used. Degree of associa- tion was expressed using odds ratio using confidence interval 95%, and p-value less than 0.05 and final data description used the form of text, tables and figures.
Results
Socio demographic characteristics Out of the 194, 102(52.6%) are male & 92(47.4%) were females. Only 41(21%) was below 25 age and 79% were above 25 age with maximum and minimum age of 72 and 19 respectively. Median of the age is 33, mean age for the male and female are 39 and 34 respectively with the total mean of 37. Most study participant (58.8%) were married with the greater number of female (51.8%). All finding of socio- demographic was described on the following table.
Table 2: The socio-demographic characteristics sitting among patients visited outpatient units of Assosa General Hospital and Assosa Health Center(n=194)
|
S.N |
variable |
|
Frequency |
Percent |
|
1 |
Educational level |
1-8 |
13 |
6.7 |
|
|
|
9-12 |
39 |
20 |
|
|
|
University degree |
44 |
22.7 |
|
|
|
Masters degree |
11 |
5.67 |
|
|
|
Above masters degree |
4 |
2 |
|
|
|
None |
83 |
42.8 |
|
2 |
Religion |
Orthodox |
69 |
35.6 |
|
|
|
Protestant |
59 |
30.4 |
|
|
|
Catholic |
56 |
5.2 |
|
|
|
Muslim |
10 |
28.9 |
|
3 |
Sex |
Male |
102 |
52.6 |
|
|
|
Female |
92 |
47.4 |
|
4 |
Monthly income in |
100-1000 |
40 |
20.6 |
|
|
birr |
1100-2000 |
47 |
24.2 |
|
|
|
2100-3000 |
54 |
27.8 |
|
|
|
3100-4000 |
28 |
14.4 |
|
|
|
4100-5000 |
14 |
7.2 |
|
|
|
>5000 |
11 |
5.7 |
|
5 |
Marital status |
Single |
44 |
21.6 |
|
|
|
Married |
114 |
58.8 |
|
|
|
Divorce |
25 |
12.9 |
|
|
|
Separated-coexisted |
11 |
5.7 |
|
|
|
Widowed |
2 |
1 |
|
6 |
Work status |
Gov’t employee |
35 |
18 |
|
|
|
Non-gov‘t employee |
27 |
13.9 |
|
|
|
Self employee |
42 |
21.6 |
|
|
|
House wife |
34 |
17.5 |
|
|
|
Peasant |
27 |
13.9 |
|
|
|
Other |
29 |
14. |
|
7 |
Age |
18-25 |
41 |
21.1 |
|
|
|
26-33 |
57 |
29.4 |
|
|
|
34-41 |
31 |
16.0 |
|
|
|
42-49 |
24 |
12.4 |
|
|
|
≥50 |
41 |
21.1 |
Lifestyle
Alcohol consumption
Prevalence of alcohol consumption was 24.2% (47) with 33 males (70.2%) and 14 females (29.8%). 31 participants (66%) had min- imum of one heavy drinking episodes per month with the medi- an number of 2. where heavy drinking expressed as (≥5 standard drinks/day in males or ≥4 in females. The frequency of drinking alcohol was generally low.
Smoking
Prevalence of smoking was 2.6%. All smoker respondents were us- ing cigarettes. No evidence of smoking in female was occurred. For current smokers, the median duration of smoking was 3 years and the median number of duration of smocking was 1 hour.
Physical inactivity
The prevalence of current physical inactivity in Assosa town was 49.5% (96), with 45(46.9%) in male and 51(53.1% ) in female. Among 98(50.5%) that was physically active, 57(58.2%) was male and 41(41.8%) was female. Those 98 current physical active was doing vigorous vigorous intensity activity that increases heart rate such as carrying or lifting heavy loads building work, medium in- tensity activity such as, walking or carrying simple loads for at least 10 minutes per day continuously.
These physical activity was practicable during both regular work and recreation. Daily duration of the time spent was shown on the following table.
Table 3: Daily duration of time spent by sitting among patients visited outpatient units of AGH & AHC (n=194)
|
Total daily duration of time spent by sitting in hour |
Frequency |
Percent(%) |
|
1 |
27 |
13.9 |
|
2 |
75 |
38.7 |
|
3 |
69 |
35.6 |
|
4 |
15 |
7.7 |
|
5 |
1 |
0.5 |
|
6 |
2 |
1 |
|
7 |
3 |
1.5 |
|
8 |
2 |
1 |
Diet
Majority of the participant 120 (61.9%) was eating fruits and veg- etables 2 times/day .. Prevalence of of adding salt to the food was 90.2% (92 male) and (83 female). Regarding the type of usually us- ing oil, prevalence of usually using vegetable oil was high (63.9%). Frequency and percentage of diet with its type was described by the following table and pie chart
Table4:Frequencyofdailyeatingbothfruitandvegetableamong patients visited outpatient unit of AGH and AHC (n=194)
|
S.N |
Variable |
Daily fre- quency |
Frequency |
Per cent |
|
1 |
Daily frequency of eating table salt |
< 1 time/ day |
6 |
3 |
|
1 time/day |
65 |
33.5 |
||
|
2 time/day |
120 |
61.9 |
||
|
≥3 times/ day |
3 |
1.5 |
||
|
2 |
Number of days that table salt is used |
Always |
175 |
90.2 |
According to following pie chart, 164 participant or 84.5% of them were used vegetable oil, but 12.4% or 24 of them used both vegeta- ble oil and butter but, only 6 of them or 3% used only butter.
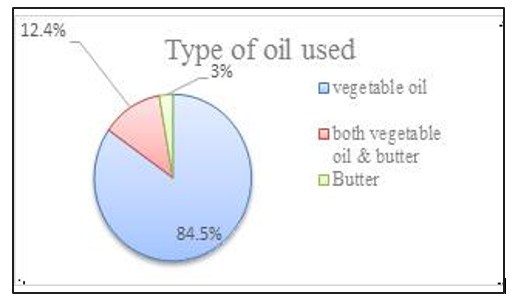
Figure 2: Type of oil used by Asossa population town, 2018.
Family History
Prevalence of family history of HTN was 35.1(68%) and prevalence of family history of DM was 17.1% (33). The following table shows prevalence and complication of Hypertension in thefamily.
Table 5: Prevalence of family history of HTN, complication of HTN in the family and prevalence of family history of DM among patients visited outpatient unit of Assosa General Hospital and Assosa Health Center 2018 (n=194)
|
S. no |
Variable |
Frequency |
Percent |
|
|
1 |
Family history of HTN |
Yes |
68 |
35.1 |
|
|
|
No |
126 |
64.9 |
|
2 |
Complication of HTN in the family |
Yes |
23 |
11.9 |
|
|
|
No |
171 |
88.1 |
|
3 |
Family history of DM |
Yes |
33 |
17.1 |
|
|
|
No |
61 |
83 |
|
4 |
Presence of complication diseases of HTN |
HF |
13 |
6.7 |
|
|
|
Stroke |
2 |
1 |
|
|
|
Kidneydisease |
7 |
3.6 |
|
|
|
Other |
1 |
0.5 |
|
5 |
Family member who have history of HTN |
Father |
14 |
7.7 |
|
|
|
Mother |
21 |
11.2 |
|
|
|
Sibling of father |
15 |
8.2 |
|
|
|
Sibling of mother |
11 |
6.2 |
|
|
|
Child |
1 |
0.5 |
|
|
|
Parent of father |
5 |
3.1 |
|
|
|
Parent of mother |
1 |
0.5 |
Prevalence of hypertension Prevalence of hypertension was 17.5%. Of these 17.5%, 18(52.9%) were male and 16(47.1%) were a female. 22(64.7%) were diagnosed two years back, 8(23.5%) were diagnosed three years back and 4(11.77%) were diagnosed in this year. Among hypertensive patients, Pre- hypertension stage 1 HTN and stage 2 HTN accounted 64.7%, 20.5% and 14.7% respectively. Out of these 34(17.5) hypertensive patients 12(35%) had some disease complication as follows. 2 of them or 1% have complication of heart failure, Another 2 of them had Type 1 Diabetic complication, and 6 of them (3%) had complication of acute gastritis. 1 patient had also complication of asthma and another 1 patient have psychotic disorder of Major Depression Disorder (MDD) which was assessed from medical chart of the patient. Risk factors for hypertension
Table 6: Multivariate association between Socio-demography, genetic & family related factors, life style and comorbidity among patients visited outpatient unit of AGH and AHC, (n=194)
|
s.no |
Variable |
Hyperte nsive |
Non- hypert ensive |
95% CI COR |
95% CI AOR |
P- val- ue |
|
|
1 |
Work Status |
Gov‘t employee Non-gov‘t employee Self-employee Housewife Peasant
Private employee |
5
2
11
6
5
5 |
30
25
31
28
22
24 |
1
2.083(0.377-11.676)
0.470(0.146-1.5141)
0.778(0.213-2.836)
0.733(0.189-2.846)
0.800(0.207-3.088) |
0.0017(0.001-0.407) |
0.415
0.783
0.681
0.996
0.012 |
|
2 |
Family history of HTN |
Yes
No |
20
14 |
112 |
0.300(0.204-1.178)
1 |
4.497(1.133-17.844) |
0.033 |
|
3 |
Marital status |
Single Married Divorced Separated & coexisting
widow |
3
23
5
2
1 |
39
91
20
9
1 |
1
0.304(0.086-1.073)
0.308(0.067-1.420)
0.346(0.050-2.386) |
|
0.251
0.779
0.364 |
|
4 |
Educati onal status |
1-8 grade
9-12 grade 1st Degree 2nd degree >masters degree
Illiterate |
9
2
9
4
1
9 |
44
37
35
7
3
34 |
1
3.784(0.769-18.618)
0.795(0.285-2.217)
0.385(0.086-1.484)
0.614(0.057-6.591)
0.773(0.277-2.157) |
|
0.996
0.239
0.559
0.254
0.337 |
|
5 |
Monthly income |
100-1000 1100-2000 2100-3000 3100-4000 4100-5000 >5000 |
5 9 9 3 3 5 |
35 38 45 25 11 6 |
1 0.603(0.184-1.974) 0.714(0.220-2.322) 1.190(0.260-5.446) 0.524(0.108-2.552) 1.171(0.038-0.778) |
|
0.531 0.315 0.330 0.413 0.116 |
|
6 |
Age |
19-25 26-33 34-41 42-49 ≥50 |
3 4 9 5 13 |
38 53 22 19 28 |
1 1.046(0.221-4.997) 0.193(0.47-0.787) 0.300(0.065-1.3991) 0.170(0.044-0.654) |
|
0.819 0.162 0.329 0.100 |
|
7 |
Using Salt |
Yes
No |
20
14 |
155
5 |
21.700(7.604-66.680) 1 |
|
0.996 |
|
8 |
Smoking |
Yes
No |
2 32 |
3 157 |
0.306(0.049-1.904) 1 |
|
0.127 |
|
9 |
Alcohol drinkin g |
Yes
No |
11
23 |
36
124 |
0.607(0.270-1.363)
1 |
|
0.909 |
|
10 |
Family history of DM |
Yes No |
9 25 |
24 136 |
0.490(0.204-1.178) 1 |
|
0.563 |
Discussion
This study shown prevalence of HTN in Assosa town (17.5%) is higher that of Cameroon which is 12.1% but comparable to Tan- zania which has prevalence of 23.7% [9]. This may be due to his- tory of the HTN in the family. Regarding the sex difference, Like Mozambique and unlike Turkey, it is higher in the male than in the female which was 52.9%, this slight difference may be due to physical activity [10]. Among Assosa town community, as their age increase, the prevalence of HTN increase, which is compara- ble to that of Turkey in which prevalence of HTN in 20-29 years and 60-69 years age group is 16.9% and 84.4% respectively [11]. In Africa the increment of prevalence of HTN with age was recorded in Egypt where the prevalence was 7.8% among young age group (25-34) years and 59.4% among old age group (65-74) years [12].
Biologically, the more we gets order, the more arterial pressure in- crease because, age positively affects thickening of artery. In this study, being private employee was one of the significant factor for hypertension which may be related to high monthly income which will be estimated to cause high consuming of vegetable oil and ta- ble salt. Private employees were 0.0017 times likely to be hyperten- sive than government employee But in this study, high salt intake, consuming vegetable oil and high monthly income were not statis- tically significant. Hence, there may be some linkage factors behind high work status and prevalence of hypertension. It should need another study. Even though it was not statistically significant, being married is another risk factor for HTN. This shown that there may be another variable (s) that was (were) not included in this study which may be psycho-social and stress which needs further study to dig it out. Though it is estimated that heavy alcohol drinkers i.e, those who drinks above two drinks per day have one and half to two high frequency of Hypertension than nondrinkers and nota- ble effect of hypertension is common when alcohol drinking ex- ceeds five drinks per day, in this study alcohol drinking associated to hypertension insignificantly [13]. Frequently and excessive use of alcohol increase obesity which gradually thickens blood arteries of the body in which blood flows to different parts and organs of the body; on the other hand it increases blood pressure and other cardiovascular diseases from complication of high blood pressure. Among Assosa town community, since number of alcohol con- sumer were small, it was impossible to stratify different categories of drinking to assess their association and effects on blood pres- sure. The effects of continuous dietary salt intake on blood pressure were identified using many and different study designs like experi- mental and interventional studies; however in this study the bivari- ate analysis effect of dietary salt intake was insignificant and shown salt intake is not independent predictor for hypertension [14]. This may be due to advice given for hypertensive patient to reduce salt in their daily food and for in-depth exploration further study with quantity of daily salt intake is demanded. Because even if quantity of salt intake at household level can be minimized, about 80% of salt is commercially available anywhere.
Though physical inactivity was not statistical significance of this study, more than half of physically inactive outpatients visited AGH and AHC was hypertensive. Accordingly, since magnitude of physical inactivity was greater than in female, it may beestimated that future prevalence of HTN in female will be greater than of male in that population.
According to study, among Assosa town population presence of HTN history in the family strongly affects prevalence of the HTN. In Assosa town population, the likelihood of developing hyperten- sion among those who have history of HTN in their family is 4.497 times higher than those who have not history of HTN in their fam- ily. This proves the relationship between genetics and hypertension and regular screening and follow up even in the non-hypertensive condition to prevent potential burden and complication. Among those who have family history of HTN, despite most of them have hypertensive mothers relatively, since it was insufficient number to compute stratified analysis other independent variables. So it was impossible to identify in which sex family history of hypertension is prevalent. In this case, another case study and case control study may identify and explore association between sex and history of HTN in the family to determine their effect on the prevalence of HTN.
Conclusion and Recommendation
The prevalence of hypertension among Assosa town was consis- tency with nearly one-fourth of that of U.S.A, nearly half of that of urban Varanasi, Hindia and of that of Gondor and also twice of that of Southern Ethiopia [9,15,16]. Prevalence of HTN in the Assosa town is higher in males, and increase as age increase. Prev- alence of hypertension in this study area is affected by history of hypertension in the family (mainly in the mother) and work status like being private employee.
The following recommendations were given to the Benishan- gul- Gumuz region and Assosa town health bureau health bureau to provide the following services in corporation with Assosa General Hospital and Assosa Health Center.
• To conduct further in-depth study using different study de- signs like case study and cohort to identify associated factors that increase susceptibility of high work status and relation- ship of HTN with sex difference, association between dietary salt intake and HTN and effects of other factors like smoking and other comorbidity diseases like DM.
• To provide health education on preventative methods of hy- pertension like decreasing salt in the food, not using smoking and having regular body exercise.
• To conduct a regular surveillance to identify and explore risk factors of hypertension which will be used for considering re- vision of current health policy specially at regional level based on the comprehensive finding and assist in, providing, mon- itoring and evaluating health education and promotion pro- grams.
• To initiate communities for screening and clinical follow up mainly for those who have history of HTN in their family.
• To provide the community with the recent information and update preventative strategy using various methods nlike mass media, announcements and posters and another means.
• Combining with the local NGOs, to focus on the problemand initiate employees of every sectors of work to direct their at- tention on associated risk factors of to prevent HTN and other related cardiovascular diseases and complication disease [17- 28].
Limitations of the Study
• Causal association of variables were not examined as it is cross sectional study.
• Lack of resource as previous conducted study on the same area and topic is unavailable.
• Number of alcohol drinkers and cigarrete smokers were not large enough to compare with dependent variable.
• Number of most reported family who have HTNin those who have family history of HTN was insufficient to associate with sex.
• Magnitude of complication disease of HTN was not large enough to compare with prevalence of HTN
Acknowledgements
Frist and foremost, I would like to express my deep & sincere grat- itude to creator of mine, scholar of heaven & earth, Almighty God for his infinite help and encouragement in all aspects of this study, from beginning to end. Next, I’m indebted to my academic super- visor, instructor Tesfu Zewdu (BSc, MSc) for his continuous com- ment, assistance, evaluation and advice. Indeed, this study bene- fited immeasurably from the input i got from Assosa University, College of health sciences & Department of Nursing. Lastly but not the least, every individuals, groups, institutions, departments and others those who are not mentioned here are pillars of my study through which I succeeded. It is my great pleasure to say you all thanks a most. Great is the exuded contribution in which you played a major role in improving your community healththrough!
References
- Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, et al. (2005) Global burden of hypertension: analysis of worldwide data. Lancet 365: 217-223.
- World Health Organization, Regional Office for South East Asia, World Health day (2013)
- Katherine T Mills, Joshua D Bundy, Tanika N Kelly, Jennifer E Reed, Patricia M Kearney, et al. (2016) Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-Based Studies from 90 countriesl. Circulation 134: 441-450.
- Hypertension. Wikipedia, the free encyclopedia. Available on URL http://en.wikipedia.org/wiki/Hypertension#cite_note- pmid7707630-121 (Accessed 6 February 2018)
- Fauci S, Braunwald E, Kasper DL, Hauser SL, Longo DL, et al. (2008) Harrison‘s principles Internal Medicine. 17th Ed. The McGraw-Hill Companies.
- Available on https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC5120816/ (Accessed 28 April 2018)
- WHO (2005) Preventing chronic diseases: a vital investment: WHO global report. Geneva, Switzerland.
- Esayas Kebede Gudina, Yadani Michael, Sahilu Assegid (2013) Prevalence of hypertension and its risk factors in southwest Ethiopia: a hospital-based cross-sectional survey. Integr Blood Press Control 6: 111-117.
- Addo J, Smeeth L, Leon DA (2007) Hypertension in sub-Saha- ran Africa: a systematic review. Hypertension. 50: 1012-1018.
- Damasceno A, Azevedo A, Silva-Matos C, Prista A, Diogo D, et al. (2009) Hypertension Prevalence, Awareness, Treatment, and Control in Mozambique Urban/Rural Gap During Epide- miological Transition. Hypertension 54: 77-83.
- Erem C, Hacihasanoglu A, Kocak M, Deger O, Topbas M (2009) Prevalence of prehypertension and hypertension and associated risk factors among Turkish adults: Trabzon Hyper- tension Study. Journal of Public Health 31: 47-58.
- 13. Amon Marwiro (2010) Prevalence and Risk Factors for Hypertension among Bulawayo City Council Employees, 2010.
- Blood pressure. Wikipedia, the free encyclopedia. Available on URL http://en.wikipedia.org/wiki/Blood_pressure (Accessed 6 February 2018).
- Factors that contribute to High Blood Pressure. The American Heart Association. Available on: http://www.americanheart. org/presenter.jhtml?identifier=4650 (Accessed 8 February 2018).
- Shikha Singh, Ravi Shankar, Gyan Prakash Singh (2017) Prev- alence and associated risk factors of hypertension: A cross sec- tional study in Urban Varanasi. Int J Hypertens 2017:5491838.
- Department of Health and Human Services (US). The Seventh Report of the Joint National Committee on Prevention, Detec- tion, Evaluation and Treatment of High Blood Pressure. NIH Publication No. 04-5230 August 2004 available on URL http:// www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf (Ac- cessed 5 February 2018).
- Sharma S,Kortas C (2018) Hypertension. Emedicine. Avail- able on URL http://emedicine.medscape.com/article/241381- overview (Accessed 5 February 2018)
- Ibrahim M, Rizk H, Appel LJ, Aroussy W, Helmy S, et al. (1995) Hypertension Prevalence, Awareness, Treatment, and Control in Egypt. Hypertension 26: 886-890.
- Wyatt SB, Akylbekova EL, Wofford WR, Coady SA, Walker ER, et al. (2008) Prevalence, Awareness, Treatment, and Con- trol of Hypertension in the Jackson Heart Study. Hyperten- sion. 51: 650-656.
- Jiang H, Muntner P, Chen J, Roccella EJ, Streiffer RH, et al. (2002) Factors Associated With Hypertension Control in the General Population of the United States. Archives of internal medicine 162: 1051-1058.
- Muntner P, Dongfeng G, Xiqui W, Duan X, Wenqi G, et al. (2004) Factors Associated With Hypertension Awareness, Treatment, and Control in a Representative Sample of the Chi- nese Population. Hypertension 43: 578-585
- Mufunda J, Mebrahtu G, Usman A, Nyarango P, Kosia A, et al. (2006) The prevalence of hypertension and its relationship with obesity: results from a national blood pressure survey in Eritrea. J Hum Hypertens 20: 59-65.
- Van de Vijver S, Akinyi H, Oti S, Olajide A, Agyemang C, et al. (2013) Status report on hypertension in Africa-consultative review for the 6th Session of the African Union Conference of Ministers of Health on NCD’s. Pan Afr Med J 16: 38.
- Misganaw A, Mariam DH, Ali A, Araya T (2014) Epidemiol- ogy of major non-communicable diseases in Ethiopia: A sys-tematic review. J Heal Popul Nutr 32: 1-13.
- Leung Ong K, Cheung BMY, Man YB, Lau CP, Lam KSL (2007) Prevalence, Awareness, Treatment, and Control of Hy- pertension Among United States Adults 1999–2004. Hyper- tension 49: 69-75.
- Lim SS, Theo Vos, Flaxman AD, Danaei G, Kenji Shibuya, et al. (2012) A comparative risk assessment of burden of dis-ease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2224-2260.