
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2023) Volume 8, Issue 1
Pregnant Women's Knowledge and Practice in Preventing Coronavirus Disease and its Associated Factors in the Dire Dawa Administration, Ethiopia
2School of Nursing and Midwifery, Haramaya University, Ethiopia
Received Date: Mar 31, 2023 / Accepted Date: Apr 20, 2023 / Published Date: Jun 02, 2023
Copyright: ©Ã???Ã??Ã?©2023 Aminu Mohammed, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Mohammed, A., Aliyi, A. (2023). Pregnant Women's Knowledge and Practice in Preventing Coronavirus Disease and Its Associated Factors in the Dire Dawa Administration, Ethiopia. Int J Women
Abstract
Background: Severe acute respiratory infections are a group of respiratory tract infections caused by a beta coronavirus (SARS-COV2).Corona Virus Disease ("COVID-19") is a family of SARS caused by a novel coronavirus that has recently spread rapidly throughout the world. The literature reveals gaps in preventive measures for specific groups, such as pregnant women. Thus, this study was aimed at assessing this gap to help with interventions.
Methods: A cross-sectional study was conducted from May 1 to 30, 2022, in the Dire Dawa city administration, Ethiopia. A systematic random sampling technique was employed to select participants, and data were collected through face-to-face interviews using a pre-tested structured questionnaire. Data were entered and cleaned by Epi DATA (Version 3.1) and analyzed using SPSS (Version 22). A P-value < 0.25 at bivariate to select variables for multivariate and ≤ 0.05 at multivariate with 95% confidence intervals was considered statistically significant.
Results: A total of 404 participants were included, for a response rate of 96.4%. About 60.6 percent and 46.3 percent of pregnant women attending antenatal care (ANC) were knowledgeable and had good practice against COVID-19 prevention measures, respectively. The predictors for knowledge were urban residence (AOR = 0.10, 95% CI: 0.06–0.17), media exposure (AOR = 2.0, 95% CI: 1.17–3.40), antenatal care visits (AOR = 2.70, 95% CI: 1.33-5.35), and parity (AOR = 0.40, 95% CI: 0.18–0.88). While urban residence (AOR = 6.60, 95% CI: 4.01–10.90), low income (AOR = 0.60, 95% CI: 0.37–0.93), and wanted pregnancy (AOR = 1.75, 95% CI: 1.01- 3.04) were predictors for practice.
Conclusion: Knowledge of pregnant women on COVID-19 was moderate compared to other studies, but their prevention practice was poor. Increased health education programs about COVID-19 were recommended for both urban and rural areas, as well as at hospital ANC wards.
Keywords
COVID-19, Knowledge, Practice, Pregnant, Women
Abbreviations
SARS: Sever Acute Respiratory Syndrome
COVID 19: Corona Virus Diseases 2019
ANC: Antenatal Care
AOR: Adjusted odds
CI: Confidence Interval
COR: Crude odds ratio
SPSS: Statistical Package for Social Sciences
Introduction
Severe acute respiratory infection (SARS) is a group of respirato¬ry tract infections caused by a beta coronavirus (SARS-COV2). Corona Virus Disease-2019 (“COVID-19”) is a family of SARS caused by Novel Coronavirus and was first detected in Decem¬ber 2019 in Wuhan, China. Since it has been declared a global pandemic by the World Health Organization (WHO), it has made the rapid spread across the world and causes high morbidity and mortality [1-3].While evidence for airborne transmission of COVID-19 is cur-rently incomplete, several hospital-based studies have performed air-sampling for SARS-COV-2, including one published paper [4]. Droplets, aerosol, and close contact are the significant factors to transfer the infection (COVID-19 pandemic) to the suspect [5,6]. Based on currently available data, neither absence nor presences of signs or symptoms are accurate enough to rule in or rule out COVIDâ?19 disease [7]. Worldwide, there is an estimated number of 5.8 million cases and nearly half a million deaths is occurred at the end of 2020 by COVID-19 [8]. COVIDâ?19 disease is not limit¬ed to the respiratory system and it affects other organs too like re¬nal dysfunction, gastrointestinal complications, liver dysfunction, cardiac manifestations, neurological abnormalities, and hemato-logical manifestations are among the reported extra pulmonary complications [9]. Moreover, according to studies in China and United States, on effects of COVID-19 on college students’ mental health show increased stress and anxiety due to the COVID-19 outbreak [10]. Increases in negative affect and symptoms of anx¬iety and depression are observed after 2 weeks of confinement in China [10]. And of the 195 students, 71% indicate increased stress and anxiety due to the COVID-19 outbreak in the United States [11].
Due to the long-lasting pandemic situation and onerous measures such as lockdown and stay-at-home orders, the COVID-19 pan-demic brings negative impacts on higher education [12,13]. Some of these negative impacts are psychological impacts vulnerabil¬ity to other diseases, burden of health care centers and workers politics and social interaction, leadership disturbance. Moreover, education process disturbances, Economic, social and political is-sues, the risks of sudden loss of income or access to social support have consequences that are difficult to estimate and constitute a challenge [14-23]. Another concern in African countries is that the response to COVID-19 will come at the expense of treating other diseases. So far, no definitive treatment for COVID-19 has been invented, and the disease has become a pandemic. Therefore, ob¬servation of hand hygiene, disinfection of high-touch surfaces, ob¬servation of social distance, and lack of presence in public places and wearing masks are recommended as preventive measures [24]. Currently, the principle fighting tool being promoted by the World Health Organization (WHO) is the prevention of acquiring SARS-COV-2 infection by following basic health hygiene rules and so¬cial distancing along with taking available COVID-19 vaccine [25]. Studies conducted across the globe, Africa including Ethi¬opia have been investigated the knowledge, attitude and practices toward the preventive measures of COVID-19 pandemic predomi¬nantly focused on health care workers and patients [26]. Currently most countries including Ethiopia have taken incredible preven tive measures including Vaccine. The severity of the COVID-19 pandemic has demanded the emergency use of COVID-19 preven¬tion methods including vaccines. However, there is still limited ev¬idence in COVID-19 vaccine acceptability and perceived barriers among some subgroups like pregnant women. In the study area, knowledge and practice to COVID-19 preventive measures among pregnant women, who constitute vulnerable groups, are yet to be assessed. Therefore, this study was aimed to investigate pregnant women's knowledge and practice in preventing coronavirus dis¬ease and its associated factors in the Dire Dawa administration, Ethiopia
Methods
Study Design and Setting
An institution based cross-sectional study was conducted from May 01 to 30, 2022 in Dire Dawa city administration 2 public and 2 private hospitals. These hospitals are found in Dire Dawa city which is located to the eastern part about 515 kilometers away from Addis Ababa, the capital city of Ethiopia. According to 2020 population projections, 506,000 people live in Dire Dawa city Ad¬ministration (68% estimated to be urban inhabitants) and have 38 rural and 9 urban kebeles (smallest administrative units). It has an estimated 37,142 households. Dire Dawa city has six hospitals (2 public and 4 private), 15 health centers and 34 health posts. Additionally there are a total of 58 different level clinics, 35 phar¬macy and 35 drug shops, Family Guidance Association and Marie Stopes International clinics [27].
Study Subjects
All pregnant women in Dire Dawa administration were the source population of this study. All pregnant women who had come to those hospitals for ANC follow-up in the study period were includ¬ed. However, pregnant women who were critically ill and admitted to the inpatient department were excluded.
Sample Size and Sampling Procedure
The sample size was determined by a single population propor-tion formula with assumptions: standard normal distribution (z=1.96), 95% level of significance, 5% margin of error (d), pro¬portion of knowledge and practice of preventive measures against COVID-19 54.84% and 76.2 %/ respectively and 10% consider¬ation of non-response rate and the final sample size became 419. The total sample size was deployed proportionally to each hospital according to their ANC flow. A systematic random sampling tech¬nique was employed in this study [28]. The intervals for subjects to be selected were calculated for each hospital in accordance with their case flow in Figure.
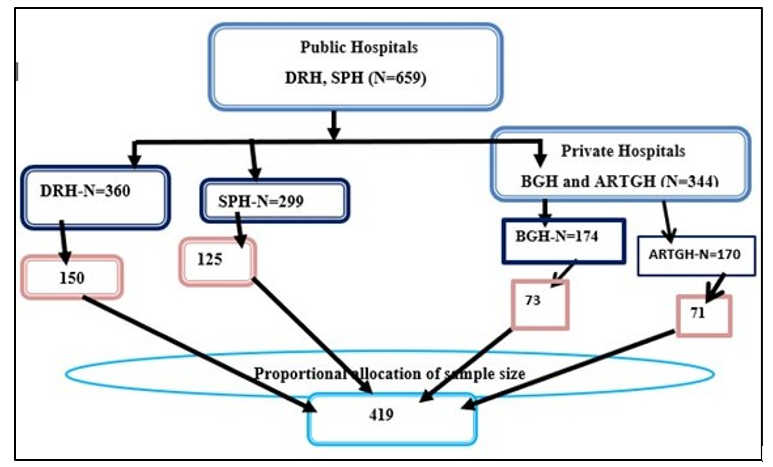
Figure: Diagrammatic Presentation of the Sampling Procedure for the Study in Public and Private Hospitals of the Dire Dawa Administration, Eastern Ethiopia, 2022
Both public hospitals (DRH, Dilchora Referral and SPH, Sabiyan primary) and 2 private hospitals (Bilal and ART General hospi-tals) were included by simple random techniques. According to the average information obtained from the 2-months record from the ANC registry books, each have DRH (720), SPH(598), BGH (348) and ARTGH (340) estimated number of ANC follower preg-nant women. Then the result is divided into two to get average number of ANC followers over one month. This results DRH=360 SPH=299, BGH=174 and ARTGH=170. Total ANC following pregnant women in four hospitals over a month equals to 1003. So, the sample size was proportionally allocated for each hospital (Figure).
Four Health professionals who have a Bachelor of Science (BSc) degree in midwifery working in ANC were data collectors and two supervisors were selected in their respective hospitals. One day training for supervisors and data collectors in each hospital was given on how to conduct data collection. The training discloses the possible benefit and purpose of the study to the study partic-ipants before the start of data collection. Orders of interview and intervals of selection were according to their ANC clinic entry. The objective of the study, how they are selected, and voluntary partic-ipation were clarified. The interview was conducted after routine services were given in ANC wards.
Data Collection Methods
The data was collected using pre-tested, interviewer guided, semi-structured questionnaire which was adapted from previous literatures designed for same study purpose and then variables were reviewed to suit the local context [29,30]. The questionnaire was developed in English language and translated into the local languages (Afan Oromo, Somali and Amharic) and then back to English to keep its consistency. The questionnaires have 15-item scale for knowledge assessment questions and an 8-item scale for practice questions. The scoring system of pregnant women’s knowledge and practice of preventive measures were either 1 (for correct answer) or 0 (for incorrect answer). The minimum score was 1, whereas the maximum score was 8 for each of knowledge and practice component of the questionnaire. The reliability of the questionnaire was checked by conducting a pretest among preg¬nant women (21=5% of sample size) in Hiwotfana Specialized University hospital ANC clinic.
Operational Definitions
The knowledge level of the study participants was determined using 15 knowledge assessing questions. A value of 1 and 0 was given for each correct and incorrect answer respectively and la¬beled as good and poor knowledge based on mean score. Those participants who scored greater than or equals to the mean score were considered as having a good knowledge whereas those who score less than the mean score labeled as poor knowledge [31]. Practice of participant was also determined based on 8 preventive measures. A value of 1 and 0 was given for each practiced and unpracticed preventive measures respectively and labeled as good and poor practice based on mean score. Pregnant women who scored greater than or equals to the mean score were considered as having good practice; while those who scored less than the mean score were considered as poor practice.
Data Quality Control
The principal investigators checked the completeness and consis¬tency of questionnaires filled by the data collectors to ensure the quality of data. To check the clarity, skipping pattern and order of questions, the questionnaire was pretested (5% of sample size at Haramaya) before the start of the actual data collection. After pre-test, questions were revised, edited, and those found to be un-clear were modified. The questionnaire was developed in English language and translated into the local languages (Afan Oromo, So-mali and Amharic) and then back to English to keep its consistency by experts. All data collectors and supervisors were selected based on their ability to speak local languages and experience of data collection and trained for one day. Questionnaires were prepared in three local languages for data collection and used according to the skills of the clients. Questionnaires-secured in a safe place for confidentiality and as a backup for later in case a need to check is necessary. Data-entered into EPI DATA software as part of data management. Double data entry was done by two data clerks, and consistency of the entered data will be cross-checked.
Data Management and Analysis
Data were checked manually for completeness. Data marked as complete were entered in to Epi Data (Version 3.1) software. For further analysis the data were exported to the SPSS (Version 22) software. Descriptive statistics were carried out as a frequency and percentage. Bivariate and multivariate analysis was used to see the effect of independent variable over dependent variable. Variables which were significant on bivariate analysis at a P-value less than 0.20 were taken to multivariate analysis. The fitness of model was checked by Hosmer and Lemeshow test (with the value >0.05). In multivariate analysis P-value of less than 0.05 and 95% confidence level was used as a cut-off point for the presence of association. Finally, results were compiled and presented using tables, graphs, charts, and texts.
Results
Socio-Demographic Characteristics
In this study, a total of 404 study participants were included, yield¬ing a response rate of 96.4%. The age of respondents was ranged from 18 to 40 (mean =26.5 years, SD±5.7 years). Majority of the participants 274 (67.8%) were married and house wife (47%) by occupation. More than half (58.4%) had primary level educa¬tion and 263 (65.1%) were urban dwellers Majority of husbands, 211(52.2%) had primary level education and 169 (41.8%) were merchant by occupation (Table 1).
|
Variables |
Category of variables |
Frequency (n=404) |
Percentage (%) |
|
Age (in complete years) |
≤19 |
34 |
8.4 |
|
|
20-24 |
111 |
27.5 |
|
|
25-29 |
125 |
30.9 |
|
|
30-34 |
81 |
20 |
|
|
35 and above |
53 |
13.1 |
|
Marital status |
Married |
274 |
67.8 |
|
|
Widowed |
89 |
22 |
|
|
Divorced |
41 |
10.1 |
|
Residence |
Urban |
263 |
65.1 |
|
|
Rural |
141 |
34.9 |
|
Religion |
Muslim |
168 |
41.6 |
|
|
Orthodox |
113 |
28 |
|
|
Protestant |
110 |
27.2 |
|
|
Catholic |
13 |
3.2 |
|
Occupation(women) |
House-wife |
187 |
47 |
|
|
Farmer |
99 |
24.9 |
|
|
Employee |
88 |
21.8 |
|
|
No job currently |
24 |
5.9 |
|
Occupation(husbands’) |
Merchant |
169 |
41.8 |
|
|
Farmer |
112 |
27.7 |
|
|
Employee |
110 |
27.2 |
|
|
No job currently |
13 |
3.2 |
|
Education level(women) |
No formal education |
42 |
10.4 |
|
|
Primary level(1-8th grade) |
236 |
58.4 |
|
|
Secondary and above |
126 |
31.2 |
|
Education level (husbands’) |
No formal education |
32 |
7.9 |
|
|
Primary level(1-8th grade) |
211 |
52.2 |
|
|
Secondary and above |
161 |
39.9 |
|
Media exposure |
Exposed more than one |
179 |
44.3 |
|
|
Exposed only one |
225 |
55.7 |
Table 1: Distribution of the Study Participants by their Socio-Demographics, Dire Daw Administration, Ethiopia, 2022 (n=404)
3.2. Reproductive Health and Obstetric Characteristics More than half (53.2%) of study participants were primipara and had more than half (65.8%) had more than three living children. Regarding the current pregnancy, majority (77%) was wanted and had more than three ANC visit. Only 86(21.3%) had reported pre¬vious adverse pregnancy outcomes (Table 2).
|
Variables |
Category of variables |
Frequency (n=404) |
Percentage (%) |
|
Parity |
Nulliparous |
78 |
19.3 |
|
|
Primipara |
215 |
53.2 |
|
|
Multipara |
111 |
27.5 |
|
Number of living children |
≤3 children |
138 |
31.2 |
|
|
>3 children |
266 |
65.8 |
|
Number of ANC visit (n=404) |
>3 |
311 |
77 |
|
|
≤3 |
93 |
23 |
|
Condition of current pregnancy |
unwanted |
93 |
23 |
|
|
Wanted |
311 |
77 |
|
Previous adverse pregnancy outcomes |
Yes |
86 |
21.3 |
|
|
No |
318 |
78.7 |
|
perceive that COVID-19 has a poor prognosis on people |
Yes |
281 |
69.6 |
|
with chronic disease |
No |
123 |
30.4 |
Table 2: Reproductive and Obstetrics Characteristics of Study Participants, Dire Daw Administration, Ethiopia, 2022 (n=404)
Pregnant Women's Knowledge about Preventive Measures against COVID-19
In this study a total of 404 participants were included with re-sponse rate of 96.4%. Pregnant women who were attending ANC in the hospitals were asked 15 questions to assess their knowledge in the preventive measures against COVID-19. Accordingly, 60.6 %( (95% CI: 55.9%-65.3%) of pregnant women were knowledge¬able. Great majority of study participants 398(98.5%) were up¬to-date that they had ever heard about COVID-19. Most common symptoms of COVID-19 mentioned by the pregnant women were headache 288 (71.3%), fever 249 (61.6%) and sore throat 212 (52.5%) (Table 3).
|
Variables |
Category |
Frequency [31] |
Percentage |
|
Ever heard about COVID-19 |
Yes |
398 |
98.5 |
|
No |
6 |
1.5 |
|
|
COVID-19 is contagious |
Yes |
279 |
69 |
|
No |
125 |
31 |
|
|
Respiratory droplets and close contact are the main transmission routes of COVID-19 |
Yes |
194 |
48 |
|
No |
210 |
52 |
|
|
Incubation period of COVID-19 is 2-14 days |
Yes |
373 |
92.4 |
|
No |
31 |
7.6 |
|
|
All peoples are generally susceptible for COVID-19 |
Yes |
259 |
64.1 |
|
No |
145 |
35.9 |
|
|
Fever is a symptom of COVID-19 |
Yes |
249 |
61.6 |
|
No |
155 |
38.4 |
|
|
Dry cough is a symptom of COVID-19 |
Yes |
133 |
32.9 |
|
No |
271 |
67.1 |
|
|
Headache is a symptom of COVID-19 |
Yes |
288 |
71.3 |
|
No |
116 |
28.7 |
|
|
Sore throat is a symptom of COVID-19 |
Yes |
212 |
52.5 |
|
No |
192 |
47.5 |
|
|
Runny nose is a symptom of COVID-19 |
Yes |
169 |
41.8 |
|
No |
235 |
58.2 |
|
Difficulty of breathing is a symptom of COVID-19 |
Yes |
177 |
43.8 |
|
No |
227 |
56.2 |
|
|
Stay at home and wearing face mask can prevent transmission of COVID-19 |
Yes |
162 |
40 |
|
No |
242 |
60 |
|
|
People with co-existing disease and smokers had poor prognostic outcomes if infected with COVID-19 |
Yes |
241 |
59.65 |
|
No |
163 |
40.35 |
|
|
Person with COVID-19 can transmit the virus to others without development of sign and symptoms |
Yes |
198 |
49 |
|
No |
206 |
51 |
|
|
pregnant women are at high risk than others if infected with COVID -19 |
Yes |
340 |
84.2 |
|
No |
64 |
15.8 |
Table 3: Pregnant Women's Knowledge about Preventive Measures against COVID-19 in Dire Dawa Administration, Ethiopia, 2022 (n=404)
Pregnant Women's Knowledge about Preventive Measures against COVID-19
A total of 404 pregnant women who were attending ANC in the hospitals were asked eight questions to assess their practice on what should be done to prevent against COVID-19. Consequent-ly, 46.3 % (95% CI: 41.3%-51.2%) of pregnant women had good practice in preventive measures against COVID-19. Participants were asked. Majority of the participants 295 (73%) were practiced preventive measure against COVID-19 by wearing face mask in public, 284 (70.3%) via avoiding handshaking, hugging and kiss¬ing, 203 (50.3%) were practiced by staying in-door if it is not must to get out and 194 (48%) by covering mouth and nose during coughing or sneezing (Table 4).
|
Questions |
category |
frequency |
percent |
|
Did you wash your hands frequently with soap and water or alcohol-based sanitizers? |
Yes |
201 |
49.75 |
|
No |
203 |
50.25 |
|
|
Did you maintaining at least 2 meter distance between yourself and others? |
Yes |
172 |
42.6 |
|
No |
232 |
57.4 |
|
|
Did you wear face mask in public? |
Yes |
295 |
73 |
|
No |
109 |
27 |
|
|
Have you stop going to public or crowded place after the COVID-19 pandemic confirmed in Ethiopia? |
Yes |
184 |
45.5 |
|
No |
144 |
54.5 |
|
|
Did you stay in-door if it is not must to get out? |
Yes |
203 |
50.3 |
|
No |
201 |
49.7 |
|
|
In order to prevent contracting and spreading COVID-19 do you avoid handshaking, hugging and kissing? |
Yes |
284 |
70.3 |
|
No |
120 |
29.7 |
|
|
Avoid touching eyes and mouth with unwashed hand. |
Yes |
203 |
50.3 |
|
No |
201 |
49.7 |
|
|
Cover mouth and nose during coughing or sneezing |
Yes |
194 |
48 |
|
No |
210 |
52 |
Table 4: Pregnant Women's Practices Regarding Preventive Measures against COVID-19 in Dire Dawa Administration, Ethiopia, 2022 (n=404)
Predictors of Pregnant Women's Knowledge of Preventive Measures against COVID-19
In binary logistic regression age (30-34), residence (urban), lev¬el of education (secondary and above) , occupation of pregnant women, husband level of education (secondary and above), media exposure parity, number of living children, number of ANC visit and previous adverse pregnancy outcomes had association with level of knowledge on preventive measures against COVID-19. Through multivariable logistic regression analysis after adjusting other co-variables by using backward likelihood stepwise method; residence/urban (AOR=0.10, 95% CI: 0.06- 0.17), media exposure (AOR=2.0, 95% CI: 1.17-3.39), number of ANC visit (AOR: 2.70; 95% CI: 1.33-5.35) and parity (AOR=0.40, 95% CI: 0.18-0.88) were found to have significant statistical association with knowl¬edge of COVID-19.
|
Variables |
Category |
Knowledge of COVID-19 |
COR (95% CI) |
AOR (95% CI) |
|
|
Good |
poor |
||||
|
Age |
≤19 |
21(61.8%) |
13(38.2%) |
1.20(0.50-2.95) |
1.75(0.57-5.40) |
|
20-24 |
71(64%) |
40(36%) |
1.09(0.55-2.18) |
1.22(0.52-2.86) |
|
|
25-29 |
79(63.2%) |
46(36.8%) |
1.13(0.58-2.22) |
0.86(0.37-1.96) |
|
|
30-34 |
39(48.1%) |
42(51.9%) |
2.09(1.02-4.29)* |
1.53(0.63-3.75) |
|
|
35 and above |
35(66%) |
18(34%) |
1 |
1 |
|
|
Residence |
Urban |
208(79%) |
55(20.9%) |
0.09(0.06-0.15)*** |
0.10(0.06-0.17)*** |
|
Rural |
37(26.2%) |
104(73.8%) |
1 |
1 |
|
|
Level of education |
Secondary and above |
57(45.2%) |
69(54.8%) |
2.42(1.16-5.03)* |
1.71(0.36-8.12) |
|
Primary level(1-8th grade) |
160(67.8%) |
76(32.2%) |
0.95(0.47-1.91) |
0.76(0.12-4.55) |
|
|
No formal education |
28(66.7%) |
14(33.3%) |
1 |
1 |
|
|
Occupation |
House-wife |
113(60.4%) |
74(39.6%) |
2.49(0.89-6.95)* |
2.20(0.66-7.30) |
|
Farmer |
60(60.6%) |
39(39.4%) |
2.47(0.85-7.16)* |
3.07(0.88-10.72) |
|
|
Employee |
47(53.4%) |
41(46.6%) |
3.31(1.14-9.67)* |
3.03(0.84-10.93) |
|
|
No job currently |
19(79.2%) |
5(20.8%) |
1 |
1 |
|
|
Level of educa-tion(husband) |
Secondary and above n |
79(49.1%) |
82(50.9%) |
3.11(1.32-7.34)** |
2.03(0.35-11.88) |
|
Primary level(1-8th grade) |
142(67.3%) |
69(32.7%) |
1.46(0.62-3.41) |
2.11(0.26-16.86) |
|
|
No formal education |
24(75%) |
8(25%) |
1 |
1 |
|
|
Media exposure |
Exposed more than one |
90(50.3%) |
89(49.7%) |
2.20(1.46-3.29)*** |
2.0(1.17-3.39)* |
|
Exposed only one |
155(68.9%) |
70(31.1%) |
1 |
1 |
|
|
parity |
Nulliparous |
56(71.8%) |
22(28.2%) |
0.43(0.23-0.80)** |
0.40(0.18-0.88)* |
|
Primipara |
131(60.9%) |
84(39.1%) |
0.70(0.44-1.11) |
1.04(0.60-1.86) |
|
|
Multipara |
58(52.3%) |
53(47.7%) |
1 |
1 |
|
|
Number of children |
≤3 children |
94(68.1%) |
44(31.9%) |
0.61(0.40-0.95)* |
0.67(0.38-1.18) |
|
>3 children |
151(56.8%) |
115(43.2%) |
1 |
1 |
|
|
Number of ANC visit |
>3 |
168(54%) |
143(46%) |
4.10(2.29-7.34)*** |
2.67(1.33-5.35)** |
|
≤3 |
77(82.8%) |
16(17.2%) |
1 |
1 |
|
|
Previous adverse pregnancy outcomes |
Yes |
42(48.8%) |
44(51.2%) |
1.84(1.14-2.98) |
1.02(0.50-2.08) |
|
No |
202(63.7%) |
115(36.3%) |
1 |
1
|
|
Significant at *p=<0.05, **p=<0.01, ***p=0.000, 1=reference
Table 5: Bivariate and Multivariable Analysis of Factors Associated with Pregnant Women’s Knowledge on Preventive Measures against COVID-19 in the Dire Dawa Administration, Ethiopia, 2022 (n = 404)
Predictors of Pregnant Women's Practice of Preventive Measures against COVID-19
In binary logistic regression age(30-34), residence(urban), media exposure parity, number of living children, number of ANC vis¬it, condition of current pregnancy and perceiving COVID-19 has a poor prognosis on people with chronic disease had association with level of practice on preventive measures against COVID-19. Through multivariable logistic regression analysis after adjusting other co-variables by using backward likelihood stepwise method; residence/urban (AOR=6.60, 95% CI: 4.01-10.90), media expo-sure (AOR=0.60, 95% CI: 0.37-0.93) and Condition of current pregnancy/wanted (AOR=1.75, 95% CI: 1.01-3.04) were predic¬tors for practice.
Urban resident pregnant women were almost seven times more likely to had good level of practice of preventive measures against COVID-19(AOR=6.60, 95% CI: 4.01-10.90) compared to rural residents. However, in this study pregnant women with unwanted pregnancy had almost two times more likely to had good level of practice of preventive measures against COVID-19 (AOR=1.75, 95% CI: 1.01-3.04) compared to pregnant women with wanted pregnancy (Table 6).
|
Variables |
Category |
Practice of COVID-19 |
COR (95% CI) |
AOR (95% CI) |
|
|
Good |
poor |
||||
|
Age |
≤19 |
16(47.1%) |
18(52.9%) |
0.70(0.28-1.63) |
0.51(0.19-1.35) |
|
20-24 |
49(44.1%) |
62(55.9%) |
0.77(0.39-1.50) |
0.61(0.28-1.30) |
|
|
25-29 |
57(45.6%) |
68(54.4%) |
0.72(0.37-1.40) |
0.73(0.35-1.56) |
|
|
30-34 |
45(55.6%) |
36(44.4%) |
0.48(0.24-0.98)* |
0.60(0.26-1.33) |
|
|
35 and above |
20(37.7%) |
33(62.3%) |
1 |
1 |
|
|
Residence |
Urban |
80(30.4%) |
183(69.6%) |
7.20(4.51-11.48)*** |
6.60(4.01- 10.90)*** |
|
Rural |
107(75.9%) |
34(24%) |
1 |
1 |
|
|
Media exposure |
Exposed more than one |
98(54.7%) |
81(45.3%) |
0.54(0.36-0.80)** |
0.60(0.37-0.93)* |
|
Exposed only one |
89(39.6%) |
136(60.4%) |
1 |
1 |
|
|
parity |
Nulliparous |
30(38.5%) |
48(61.5%) |
1.81(1.01-3.27)* |
1.54(0.78-3.06) |
|
Primipara |
98(45.6%) |
117(54.4%) |
1.35(0.86-2.14) |
1.10(0.63-1.81) |
|
|
Multipara |
59(53.2%) |
52(46.8%) |
1 |
1 |
|
|
Number of children |
≤3 children |
53(38.4%) |
85(61.6%) |
1.63(1.07-2.47)* |
1.61(0.99-2.62) |
|
>3 children |
134(50.4%) |
132(49.6%) |
1 |
1 |
|
|
Number of ANC visit |
>3 |
162(52.1%) |
149(47.9%) |
0.34(0.20-0.56)*** |
0.60(0.22-1.67) |
|
≤3 |
25(26.9%) |
68(73.1%) |
1 |
1 |
|
|
Condition of current pregnancy |
unwanted |
33(35.5%) |
60(64.5%) |
1.78 (1.10-2.88)* |
1.75 (1.01-3.04)* |
|
wanted |
154(49.5%) |
157(50.5%) |
1 |
1 |
|
|
Perception/COVID-19 has a poor prognosis on people with chronic disease |
Yes |
144(51.2%) |
137(48.8%) |
0.51(0.33-0.79)** |
0.85(0.34-2.10) |
|
No |
43(35%) |
80(65%) |
1 |
1 |
|
Significant at *p=<0.05, **p=<0.01, ***p=0.000, 1=reference
Table 6: Bivariate and Multivariate Analysis of Factors Associated with Pregnant Women’s Practice of Preventive Measures against COVID-19 in Dire Dawa Administration, Ethiopia, 2022 (n = 404)
Discussion
So far there is no definite treatment for COVID-19. Therefore, rec-ognizing the level of knowledge and practice of preventive mea-sures against it is critical to put prevention and controlling inter-vention particularly for low resources countries) like Ethiopia. This study presents pregnant women's knowledge and practice in pre¬venting coronavirus disease and its associated factors in the Dire Dawa administration, Ethiopia. Accordingly, this study shows that 60.6 percent (95% CI: 55.9%–65.3%) of pregnant women were knowledgeable on preventive measures against COVID-19. The finding of this study was in line with a study conducted in Ghana (62.7%) and Abakaliki, Nigeria (60.9%). higher than studies con¬ducted in South Africa (43.5%), in Guraghe Zone, southern Ethi¬opia (54.84%) and Debretabor town, northern Ethiopia (48.6%). lower than studies in Pakistan (85.7%), southwestern Iran (70%) and India (75.3%).This study is also lower than a study conducted in southwest Nigeria (87.2%).
This study shows that 46.3 % (95% CI: 41.3%-51.2%) of preg-nant women had good practice on preventive measures against COVID-19. The finding of this study was in line with studies conducted in Abakaliki, southeast Nigeria and Debretabor town, northern Ethiopia (47.6 %). However, it is lower than a finding of studies conducted in china (71.0%), India (92.7 %) and Pakistan (69.9%).The finding of this study is also lower than some studies in Africa and Ethiopia like South Africa (76%) Southwest Nigeria 79.2% and Guraghe Zone, southern Ethiopia (76.2 %). The finding of this study regarding the practice against COVID-19 by preg-nant women is higher than a study conducted in Abakaliki, Nigeria (30.3 %).
The findings of this study suggest significant knowledge and practice gaps between the amount of information available about COVID-19 and the depth of knowledge among the pregnant wom¬en. As the global threat of COVID-19 continues to emerge, it is critical to improving knowledge and practice in prevention and control against COVID-19 among pregnant women and the gener-al people in the Dire Dawa city administration.
Conclusions
In conclusion, this study showed that average number of pregnant women had knowledge and practice to prevent against COVID-19. The use of social media, antenatal care follow up, parity and res¬idence showed a significant association with pregnant women’s knowledge in prevention against COVID-19. While residence, media exposure and wanted pregnancy showed a significant as¬sociation with pregnant women’s practice in prevention against COVID-19 [32-38]. As per the finding promoting and increasing health education program regarding to the pandemic via different mass Medias and social Medias, promoting and increasing ANC follow up of pregnant women considering residence is recom¬mended to hospitals and community administrators and all other stakeholders. It is also recommended that mixed methods research, program evaluations, and longitudinal research efforts to be un¬dertaken to explore many other factors related to the knowledge and practice of pregnant women against prevention of COVID-19 and address effect of COVID-19 on pregnancy and pregnancy out¬comes too.
Strengths and Limitation
As this study is about the new devastating pandemic, it tried to de-termine the predictor of knowledge and practice of pregnant wom-en to prevent against COVID-19 and as there is scarcity of studied literatures on this specific study. The study focuses on risky groups (pregnant women) and included many study centers (study areas) which increase the external validity of the study.
Limitation of the Study
Since the study design was cross-sectional, cause and effect could not be identified. Social desirability bias is expecting in this study. But efforts were made to manage them through pre-testing the questionnaire, training of data collectors, and supervisors on how to approach respondents, interviewing privately, close supervision of data collectors, and explaining the purpose of the study for the study participants.
Availability of Data and Materials
The datasets used and analyzed during the current study are not available publicly due to privacy reasons, but are available from the corresponding author on reasonable request.
Acknowledgments
The author is grateful to the data collectors, supervisors, and study participants. Last but not least, my thanks go to hospital adminis¬trators (Both public hospitals (Dilchora Referral, Sabiyan, Bilal and ART General hospitals) and those individuals who directly or indirectly contributed their skills and knowledge toward the ac¬complishment of this study.
Funding
The research received no specific Grant from any funding agency in the public, commercial, or not-for profit sectors.
Author Information
Aminu Mohammed and Ahmedin Aliyi have contributed to this work.
Contributions
Aminu Mohammed: He was responsible for all aspects of this study, supervising data collectors along with supervisors, includ¬ing the study's design and implementation, analysis, interpretation of study results, and manuscript preparation, revision, writing and submission to the journal. Ahmedin Aliyi: Assisted in supervision, data analysis, draft revi¬sion, result interpretation, and writing manuscript
Ethics Declarations
Ethics Approval and Consent to Participate
Ethical approval was obtained on 19 March 2022 from Ethical Com¬mittee of Dilchora referral Hospital (File-DRH-2001/M/2022). Besides, an official letter of permission was obtained from the each hospital medical directors (Dilchora referral, Sabiyan, Bi¬lal and ART general hospitals). All protocols were carried out in accordance with relevant guidelines and regulations of Helsinki. Informed voluntary consent was obtained from all subjects and/or their legal guardian(s).
References
- Wu, D., Wu, T., Liu, Q., & Yang, Z. (2020). The SARS-CoV-2outbreak: what we know. International journal of infectious diseases, 94, 44-48.
- Zumla, A., Hui, D. S., & Perlman, S. (2015). Middle East respiratory syndrome. The Lancet, 386(9997), 995-1007.
- Lu, H., Stratton, C. W., & Tang, Y. W. (2020). Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle. Journal of medical virology, 92(4), 401.
- Ong, S. W. X., Tan, Y. K., Chia, P. Y., Lee, T. H., Ng, O. T.,Wong, M. S. Y. (2020). Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient, Jama. 323(16):1610-2.
- Lewis, D. (2020). Is the coronavirus airborne? Experts can’t agree. Nature, 580(7802), 175.
- Morawska, L., & Cao, J. (2020). Airborne transmission of SARS-CoV-2: The world should face the reality. Environment international, 139, 105730.
- Struyf, T., Deeks, J. J., Dinnes, J., Takwoingi, Y., Davenport, C., Leeflang, M. M., ... & Cochrane COVID-19 Diagnostic Test Accuracy Group. (2020). Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVIDâ?19. Cochrane Database of Systematic Reviews, (5).
- Organization WH. (2020). Coronavirus disease (ff COVID-19)ff:situation report, 166.
- Behzad, S., Aghaghazvini, L., Radmard, A. R., & Gholam-rezanezhad, A. (2020). Extrapulmonary manifestations of COVID-19: radiologic and clinical overview. Clinical imaging, 66, 35-41.
- Li, H. Y., Cao, H., Leung, D. Y., & Mak, Y. W. (2020). Thepsychological impacts of a COVID-19 outbreak on college students in China: a longitudinal study. International journal of environmental research and public health, 17(11), 3933.
- Son, C., Hegde, S., Smith, A., Wang, X., & Sasangohar, F. (2020). Effects of COVID-19 on college students’ mental health in the United States: Interview survey study. Journal of medical internet research, 22(9), e21279.
- Bettinsoli, M. L., Di Riso, D., Napier, J. L., Moretti, L., Bettinsoli, P., Delmedico, M. (2020). Psychological Impact and Contextual Factors Associated With Physical and Mental Health Conditions of Italian Healthcare Professionals During the Covid-19 Disease Outbreak.
- Li, S., Wang, Y., Xue, J., Zhao, N., & Zhu, T. (2020). Theimpact of COVID-19 epidemic declaration on psychological consequences: a study on active Weibo users. International journal of environmental research and public health, 17(6), 2032.
- Jordan, R. E., Adab, P., & Cheng, K. (2020). Covid-19: risk factors for severe disease and death. Bmj, 368.
- Sam, P. (2020). Redefining vulnerability in the era ofCOVID-19. Lancet, 395(10230), 1089.
- Bradley, N. L., DiPasquale, A. M., Dillabough, K., & Schneider, P. S. (2020). Health care practitioners’ responsibility to address intimate partner violence related to the COVID-19 pandemic. Cmaj, 192(22), E609-E610.
- Nepal, R., Sapkota, K., Adhikari, K., Paudel, P., Adhikari, B., Paudyal, N. (2020). Knowledge, attitude and practice regarding COVID-19 among healthcare workers in Chitwan, Nepal.
- Olum, R., Chekwech, G., Wekha, G., Nassozi, D. R., & Bon-gomin, F. (2020). Coronavirus disease-2019: knowledge, attitude, and practices of health care workers at Makerere University Teaching Hospitals, Uganda. Frontiers in public health, 8, 181.
- World Health Organization. (2020). COVID-19 and violence against women: what the health sector/system can do, 7 April 2020 (No. WHO/SRH/20.04). World Health Organization.
- Roesch, E., Amin, A., Gupta, J., & García-Moreno, C. (2020). Violence against women during covid-19 pandemic restrictions. Bmj, 369.
- Williamson, B., Eynon, R., & Potter, J. (2020). Pandemic politics, pedagogies and practices: digital technologies and distance education during the coronavirus emergency. Learning, Media and Technology, 45(2), 107-114.
- Bozkurt, A., Jung, I., Xiao, J., Vladimirschi, V., Schuwer, R., Egorov, G., & Paskevicius, M. (2020). A global outlook to the interruption of education due to COVID-19 pandemic: Navigating in a time of uncertainty and crisis. Asian Journal of Distance Education, 15(1), 1-126.
- Fekene, D. B., Bulto, G. A., and BEM, Gemeda, G. M. (2017). Male Partner’s Involvement and it’s Associated Factors in Promoting Skilled Birth Attendance among Fathers who have Children Less than One Year of Age in Ambo Town, Ethiopia. EC Gynaecology. 8.6(2019):465-74.
- Arefi, M. F., & Poursadeqiyan, M. (2020). A review of studies on the COVID-19 epidemic crisis disease with a preventive approach. Work, 66(4), 717-729.
- Sahu, K. K., & Kumar, R. (2020). Preventive and treatment strategies of COVID-19: from community to clinical trials. Journal of family medicine and primary care, 9(5), 2149.
- Jemal, B., Aweke, Z., Mola, S., Hailu, S., Abiy, S., Dendir, G.,... & Teshome, D. (2021). Knowledge, attitude, and practice of healthcare workers toward COVID-19 and its prevention in Ethiopia: A multicenter study. SAGE Open Medicine, 9.
- Dire Dawa Health Bereau Health Demographic Statistics. 2020.
- Fikadu, Y., Yeshaneh, A., Melis, T., Mesele, M., Anmut, W., & Argaw, M. (2021). Covid-19 preventive measure practices and knowledge of pregnant women in guraghe zone hospitals. International journal of women's health, 39-50.
- Amsalu, B., Guta, A., Seyoum, Z., Kassie, N., Sema, A., De-jene, W., & Belay, Y. (2021). Practice of COVID-19 prevention measures and associated factors among residents of Dire Dawa City, Eastern Ethiopia: Community-Based Study. Journal of multidisciplinary healthcare, 219-228.
- Ayele, A. D., Mihretie, G. N., Belay, H. G., Teffera, A. G., Kassa, B. G., & Amsalu, B. T. (2020). Knowledge and Practice to Prevent Against Corona Virus Disease (COVID-19) and Its Associated Factors Among Pregnant Women in De-bre Tabor Town Northwest Ethiopia: a Community Based Cross-Sectional Study.
- Serwaa, D., Lamptey, E., Appiah, A. B., Senkyire, E. K., & Ameyaw, J. K. (2020). Knowledge, risk perception and preparedness towards coronavirus disease-2019 (COVID-19) outbreak among Ghanaians: a quick online cross-sectional survey. The Pan African Medical Journal, 35(Suppl 2).
- Nwafor, J. I., Aniukwu, J. K., Anozie, B. O., & Ikeotuonye,A. C. (2020). Knowledge and practice of preventive measures against COVID-19 infection among pregnant women in a low-resource African setting. MedRxiv, 2020-04.
- Hoque, A. M., Alam, A. M., Hoque, M., Hoque, M. E., & Van Hal, G. (2021). Knowledge, attitudes, and practices towards COVID-19 of pregnant women at a primary health care facility in South Africa. European Journal of Medical and Health Sciences, 3(1), 50-55.
- Sajid, A., Sajid, A., Sajid, A., Hanif, A., Wazir, A., & Chee-ma, S. (2020). Knowledge Attitude and Practices towards COVID-19 among Pregnant Patients Coming in Lady Aitchi-son Hospital, Lahore. Journal of The Society of Obstetricians and Gynaecologists of Pakistan, 10(3), 153-158.
- Maharlouei, N., Asadi, N., Bazrafshan, K., Roozmeh, S.,Rezaianzadeh, A., Zahed-Roozegar, M. H., & Lankarani,K. B. (2020). Knowledge and attitude regarding COVID-19 among pregnant women in Southwestern Iran in the early period of its outbreak: a cross-sectional study. The American journal of tropical medicine and hygiene, 103(6), 2368.
- Kamal, D., Thakur, V. D., Swain, S. K., & Vikneshram, C. R. (2020). Knowledge, attitude, and practice toward COVID-19 among pregnant women in a tertiary care hospital during the COVID-19 outbreak. Journal of Marine Medical Society, 22(3), 66.
- Aduloju, O. P., Okunola, T. O., Adefisan, A. S., & Aduloju,T. (2019). Knowledge, attitude and practice of preventive measures against coronavirus disease 2019 among pregnant women in a tertiary health facility in southwest Nigeria. Int J Clin Obstet Gynaecol, 5(3), 101-7. Anikwe, C. C., Ogah,C. O., Anikwe, I. H., Okorochukwu, B. C., & Ikeoha, C. C. (2020). Coronavirus disease 2019: Knowledge, attitude, and practice of pregnant women in a tertiary hospital in Abakaliki, southeast Nigeria. International Journal of Gynecology & Obstetrics, 151(2), 197-202.
- Ding, W., Lu, J., Zhou, Y., Wei, W., Zhou, Z., & Chen, M. (2021). Knowledge, attitudes, practices, and influencing factors of anxiety among pregnant women in Wuhan during the outbreak of COVID-19: a cross-sectional study. BMC pregnancy and childbirth, 21(1), 1-9.