

Research Article - (2026) Volume 11, Issue 2
Poliscience: A Randomized Experimental Study on the Effects of a Standardized Narcotics Identification Card for ADHD Patients in Ambiguous Police Control Situations in Germany
Received Date: Mar 10, 2026 / Accepted Date: Apr 07, 2026 / Published Date: Apr 21, 2026
Copyright: ©2026 Emily Klose. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Klose, E. (2026). Poliscience: A Randomized Experimental Study on the Effects of a Standardized Narcotics Identification Card for ADHD Patients in Ambiguous Police Control Situations in Germany. Int J Psychiatry, 11(2), 01-08.
Abstract
Background: ADHD in adulthood affects approximately 2.5% of the population. Treatment in accordance with guidelines often involves stimulants that are subject to narcotics regulations. In ambiguous police control situations, carrying these medications can lead to suspicion, seizure, and investigation, despite legal prescription. This study examined whether a standardized narcotics identification card (ADHS-Ausweis®) reduces suspicion and intervention tendencies among German police officers.
Method: 74 active police officers participated in a two-armed, randomized online vignette study (ID+ vs. ID-). Standardized control scenarios were evaluated; 11 perceptions and intentions to act (POL-11) were recorded. Analysis was performed using MANOVA and univariate follow-up tests.
Results: Compared to the control condition, the identification card led to fewer negative intentions toward patients, including suspicion of drug trafficking/abuse, further control measures, contact with physicians, and securing medication. At the same time, credibility and health- related attributions increased. The effects were evident across various behavioral scenarios and remained detectable even in the case of risky behavior (e.g., refusal to answer questions, unfriendliness, pupil dilation/trembling).
Conclusion: The examined narcotics identification card shows a de-escalating effect in police control situations by reducing suspicion and strengthening patient-related attributions. Replication studies should examine its generalizability in other regions and legal contexts.
Keywords
ADHD, ADHD ID, Narcotics Identification Card, Police, Psychostimulants, Lisdexamfetamine, Methylphenidate
Introduction
Attention deficit hyperactivity disorder (ADHD) is a neurobiological developmental disorder that usually manifests in childhood and whose symptoms generally persist into adulthood [1]. Current studies report adult prevalence rates of between 2.8% and 4.4% [2]. The disorder is characterized by the key symptoms of motor hyperactivity, impulsivity, and inattention. ADHD is associated with cognitive impairments, including impairments in attention, problem solving, vigilance, inhibition control, language processing, memory performance, and cognitive flexibility. In addition, other functions such as sensory processing, motor skills, and emotion regulation may be affected, with nearly all disorder-related impairments also affecting social skills and social reception. The standard treatment for ADHD involves medication with prescription stimulants such as lisdexamfetamine (e.g., Elvanse®) or methylphenidate (e.g., Medikinet® adult), with prescription psychostimulants being among the most commonly prescribed ADHD medications. Possession of these substances without a physician's prescription is a criminal offense. Even if possession is legal and there is a proven medical indication, those affected are still at risk of coming into conflict with the Narcotics Law during police checks. The relevant provision in Germany is § 29 of the German Narcotics Act (Betaubungsmittelgesetz; BtMG), which provides for ''imprisonment of up to five years or a fine'' for unauthorized ''possession without being in possession of a written permit for acquisition.''
The impairments associated with ADHD affect many areas of life, including encounters with people in authoritative roles such as the police in everyday life. The key issue here is less the occurrence of manifest violations of the law than the increased risk of subtle violations of informal social norms due to ADHD symptoms, as a result of which those affected—for example, due to motor restlessness, impulsivity, pronounced impatience, low frustration tolerance, delayed implementation of requests, or ambiguous nonverbal and paraverbal signals—are quickly perceived as potentially uncooperative or disrespectful in interactions with authority figures and are accordingly stigmatized [3].
In practical terms, suspicion-independent checks can lead to the confiscation of medication, the initiation of criminal investigations, and lengthy, stressful proceedings, even if no unlawful behavior has occurred at any point. With the expansion of Section § 42c of the German Weapons Act (Waffengesetz; WaffG) in 2025, the possibility of such suspicion- independent checks on individuals in public spaces was greatly expanded in Germany. Since the law does not contain any specific criteria for carrying out such checks, there is a lot of discretion left to the officers doing the checking. In such contexts, there is a fundamental risk that individual neurodivergent behavioral characteristics—such as motor restlessness, irregular eye contact, overcompensatory self-regulation efforts, taciturnity, or avoidant behavior—will be misinterpreted as indications of suspicious behavior [4].
In this context, it is relevant that symptoms of ADHD often become more pronounced under acute psychosocial stress [5]. In addition, impulsivity in particular can lead to a tendency toward aggressive behavior or passive-aggressive refusal [6]. As a result, there may be an increased likelihood of interaction dynamics arising during a check in which the stress-induced suspicious social behavior of the person being checked is perceived by the police officers as confirmation of their initial suspicion (stereotype threat) [4]. As a result, there is an empirical increase in the risk of further measures being taken against the will of the person being checked [4]. These may include physical searches or the seizure of medically prescribed medication. Such measures can result in considerable psychosocial stress for those affected, as well as subsequent judicial and economic consequences, including the initiation of criminal investigations.
Empirical findings suggest that references to existing mental illness systematically influence the attribution behavior of police officers. Watson, Corrigan, and Otatti showed that police officers attributed greater need for assistance to people with schizophrenia and, at the same time, attributed less responsibility for the delinquent situation [7]. Furthermore, the presence of state empathy among officers in training was associated with a reduction in rejection and distrustful attitudes toward individuals with mental disorders. This suggests that state empathy enables police officers to distinguish between delinquency and disorder-related exceptional behavior.
However, these findings apply only to a limited extent to people with ADHD, as possession of any narcotic-containing medication can bring them more quickly into the focus of police investigations. From a police perspective, carrying such substances could raise concerns that a reported diagnosis is merely being used as a protective claim to conceal a potential crime. In the case of ADHD patients, it therefore seems likely that informal verbal reference to the existing narcotics indication alone will not lead to less suspicious attribution patterns and increased state empathy towards the patient.
Within this context, the present study aimed to examine the effects of a narcotics identification card on perceived suspicious circumstances as well as on action tendencies and attribution patterns of German police officers within the framework of a randomized case vignette design. It was expected that, regardless of the behavior of the person being checked, the ID would (1) have a mitigating effect on police officers' tendencies to act in a manner disadvantageous to the patient and (2) have an exonerating effect on negative attribution tendencies, including credibility, sincerity, and the assessment that the drugs serve the health and well-being of the person being checked.
Method and Material
Study Design
A two-arm, randomized online case vignette design was implemented as part of this study. Participants were randomly assigned to one of two experimental conditions: an experimental condition involving the presentation of an ID (ID+) and a control condition without an ID (ID-). The study was conducted at the Department of Psychology at a university in Hesse, Germany in compliance with the ethical guidelines of the Declaration of Helsinki and in accordance with the minimum ethical requirements of the university's internal ethics committee.
Inclusion criteria were age > 18 years and current employment as a police officer. Out of N = 365 prospective study participants who opened the survey link, n = 74 completed the survey in full (see Figure 1).
With their digitally transmitted informed consent, participants received standardized information about the study design, procedure, and data protection aspects, in particular the anonymity of the data collected and the voluntary nature of participation. Participants were informed that this was a computer-based vignette study aimed at investigating the psychological mechanisms of police decision-making.
Exerimental Procedure
The study included a preliminary screening followed by an experiment. The preliminary screening involved the collection of sociodemographic parameters and the assessment of anger tendencies using the scale of the State-Trait-Anger-Expression Inventory [8]. This was followed by randomized transfer to the experimental part.

Figure 1: CONSORT diragram (Consolidated Standards of Reporting Trials) showing recruitment, group assignment, and final number of participants. The sample consisted of 74 subjects. Group assignment was randomized to the ID- and ID+ groups. Randomization was performed using simple random assignment without block formation, which resulted in an uneven distribution
|
|
ID- |
ID+ |
p |
|
Ntotal (%female) |
45 (8.9) |
29 (13.7) |
.06 |
|
Age M / SD / Mdn years |
29.1 / 6.01 / 28 |
31.2 / 6.64 / 29 |
.16 |
|
STAXI-2 T M / SD / Mdn |
22.7 / 3.88 / 23 |
21.4 / 4.09 / 20 |
.19 |
|
Anmerkung. ID+ = with ID. ID- = without ID. P-values refer to the respective Chi2- or t-test for group differences per variable. |
|||
Table 1: Descriptive Sample Data
Stimulus Material
Standardized photographs of the ADHS-Ausweis® narcotics identification card in six versions served as stimulus material. The ADHS-Ausweis® product is a document form developed in accordance with legal requirements and specifications, which the patient has filled out and countersigned by the treating specialist. The document consists of a total of six pages and can be folded into itself using a triple fold, with dimensions of approximately 95 x 56 mm per page. The outside pages contain fields for handwritten medical information about the treating/signing physician, as well as fields for the date of issue, practice stamp, and the physician's signature.
For the present experiment, fictitious information about the respective treating physicians was placed in the designated fields. The stamp contained complete (real) address data as well as fictitious contact details and a fictitious business location number (Betriebsstattennummer; BSNR). Elvanse® (Takeda Pharmaceutical) was entered in a dosage of 70 mg with the times of administration 1-0-0, and Medikinet® (MEDICE Arzneimittel Putter GmbH & Co. KG) 10 mg with randomly varying information (such as ''as needed'' or ''as needed 1 x per day''). The prescriptions were each confirmed by a physician line by line. In addition to the prescription details, there was also information on the patient's identity, including their date of birth and narcotics indications (always ICD-10 code F.90.0), as well as their address.
Questionnaire for Surveying Police Behavioral Tendencies (POL-11)
Eleven items were developed to assess situational behavioral tendencies, which were designed to measure the participants' situation-related perception tendencies and intentions to act. The items were developed exploratively based on relevant experiences from everyday police work and typical decision-making situations involving ADHD-typical conspicuous (''neurodivergent'') behavior and medication carried in public spaces. They were intended to reflect realistic assessments and typical considerations for action in police encounters with ambiguous behavior. The aim was to operationalize the cognitive assessment processes of police officers in such situations as authentically as possible. Theoretically, the development was based on theories of attribution-based perception processes according to Kelley on the one hand, and on concepts of heuristic judgment formation according to Tversky and Kahneman on the other, which describe typical simplified, intuitively formed judgments in uncertain situations [9,10]. The responses were given on a five-point Likert scale from 1 = not at all applicable to 5 = fully applicable. An internal consistency of ![]() = .90 was determined with the present sample. The items were as follows:
= .90 was determined with the present sample. The items were as follows:
• The person seems suspicious to me. (Person is suspicious)
• I wonder if the person is dealing with the medication. (Suspicion of trafficking)
• I am considering whether further checks are necessary. (Carry out further checks)
• I am considering confiscating the medication. (Confiscate medication)
• I am considering whether it would be useful to ask the attending physician whether the medication carried is actually prescribed. (Consider consulting the physician)
• I consider it necessary to consult with my superiors to clarify how to proceed. (Consult with superiors)
• The medication carried is important for this person. (Meds are important for person)
• The person makes a credible and sincere impression on me. (Is credible/sincere)
• The medication is for the person's health. (Meds are for their well-being)
• I wonder if the person is abusing the medication. (Suspicion of abuse)
• I assume that the person's behavior is due to their illness. (Behavior is due to illness)
Case Vignettes
In the experimental part, participants worked on six standardized case vignettes involving police checks in public spaces, in which controlled substances used to treat ADHD were found on the person being checked. The vignettes differed only in terms of one dominant behavioral characteristic of the index person that could be interpreted in potentially ambivalent ways: nervousness, lack of eye contact, speech abnormalities, and behaviors that could be interpreted as risky, such as refusal to answer questions, unfriendliness, and pupil dilation/trembling. All other situational information was kept constant.
The study followed a between-subjects design with two experimental conditions. In the ID+ condition, the index person presented a standardized narcotics identification card. A photo of the ID was displayed for this purpose. In the ID- condition, no narcotics identfication card was presented; instead, the person being checked simply stated verbally that they were an ADHD patient and that the medication had been prescribed by a physician. The text, medication, and procedure of the check were otherwise identical. After each vignette, the police officers' perceptions and intended actions were assessed using the POL- 11.
The T-scale (trait anger) of the STAXI-2 anger expression inventory was used to check the equivalence of the groups in terms of dispositional anger response [8]. The scale measures a person's dispositional tendency to feel anger persistently and across situations. The measurement was used exclusively to control for potential initial differences between the experimental groups and was not part of the research questions or hypotheses. It consists of the two subscales ''anger temperament'' (general readiness to experience spontaneous and frequent anger; e.g., ''I get upset easily'') and ''anger reaction'' (tendency to feel anger in response to specific provocations or perceived injustice; e.g., ''It upsets me when I am treated unfairly''). The T-scale thus measures interindividual differences in the habitual intensity and frequency of anger experiences. The internal consistency is between rtt = .79 and .91, and the retest reliability is between rtt = .67 and .78.
Statistical Analyses
The statistical analyses were conducted using Jamovi analysis software (version 2.5.3.0; The jamovi Project,) [11]. Sociodemographic characteristics were compared between groups using t-tests and chi-square tests.
To test for group-related differences across the entire set of outcome variables, a one- factor MANOVA was performed, in which group was modeled as a two-level between factor.
The analysis included the items of the POL-11 averaged across all six case vignettes as eleven dependent variables. Significance levels were set at p < .05 (one-tailed).
In order to capture differences in police officers' behavior depending on the behavior of the persons being checked, the overall sample means (without group division) of the eleven police behavior tendencies (person is suspicious, suspicion of trafficking, carry out further checks, confiscate medication, consider consulting the physician, consult with superiors, meds are important for person, is credible/sincere, meds are for their well-being, suspicion of abuse, behavior is due to illness) were calculated separately for each control scenario. These were compared in descriptive analyses between the six control scenarios (nervousness, lack of eye contact, speech abnormalities, refusal to answer questions, unfriendliness, pupil dilation/trembling).
Results
Sample
Refer to Table 1 for detailed sample characteristics. The ID+ and ID- groups did not differ in terms of gender, age, and trait anger (STAXI-2).
Analysis of Group Differences
A multivariate analysis of variance (MANOVA) was performed to test whether the groups differed in the eleven dependent variables. A significant overall effect was found for group, Pillai's = 0.481, F(11, 62) = 5.22, p < .001. In univariate follow-up tests, with the exception of behaviour is due to illness significant differences between the groups were found for all action and attribution tendencies (see Figure 2 and Table 2). Descriptively, the aggregated behavioral tendencies vary significantly between the control scenarios, with the highest values for refusing to answer questions and pupil dilation/trembling (see Figure 3).
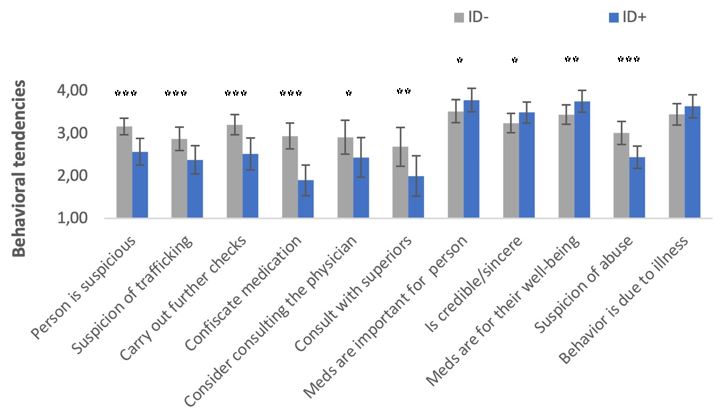
Figure 2: The Eleven Perceptions and Intentions to Act Across All Scenarios Depending on The Presence of the Identification Card. ID-= without ID, ID+ = with ID. Significant Univariate follow-up tests are marked with * p < .05, ** p < .01 und *** p < 001.
|
|
Group |
M |
SD |
F |
p |
|
Person is suspicious |
ID+ |
2.57 |
0.31 |
|
< .001 |
|
ID- |
3.16 |
0.19 |
25.67 |
||
|
Suspicion of trafficking |
ID+ |
2.38 |
0.33 |
12.08 |
< .001 |
|
ID- |
2.87 |
0.28 |
|||
|
Carry out further checks |
ID+ |
2.52 |
0.38 |
23.54 |
< .001 |
|
ID- |
3.21 |
0.24 |
|||
|
Confiscate medication |
ID+ |
1.90 |
0.36 |
45.43 |
< .001 |
|
ID- |
2.94 |
0.30 |
|||
|
Consider consulting the physician |
ID+ |
2.44 |
0.46 |
5.49 |
< .05 |
|
ID- |
2.91 |
0.40 |
|||
|
Consult with superiors |
ID+ |
2.00 |
0.48 |
9.61 |
< .01 |
|
ID- |
2.69 |
0.46 |
|||
|
Meds are important for person |
ID+ |
3.79 |
0.27 |
4.19 |
< .05 |
|
ID- |
3.52 |
0.27 |
|||
|
Is credible/sincere |
ID+ |
3.49 |
0.24 |
5.06 |
< .05 |
|
ID- |
3.24 |
0.23 |
|||
|
Meds are for their well-being |
ID+ |
3.76 |
0.23 |
7.61 |
<0.1 |
|
ID- |
3.44 |
0.26 |
|||
|
Suspicion of abuse |
ID+ |
2.44 |
0.26 |
25.76 |
< .001 |
|
ID- |
3.01 |
0.27 |
|||
|
Behavior is due to illness |
ID+ |
2.36 |
0.27 |
2.41 |
.125 |
|
ID- |
2.55 |
0.25 |
|||
|
Note. N = 74. ID+ = group with ID (n = 29). ID- = group without ID (n = 45). |
|||||
Table 2: Group Differences in Police Action and Attribution Tendencies
The results are based on univariate analyses of variance (F-Tests) with df(1, 72). Values in bold indicate statistical significance at the level of p < .05.
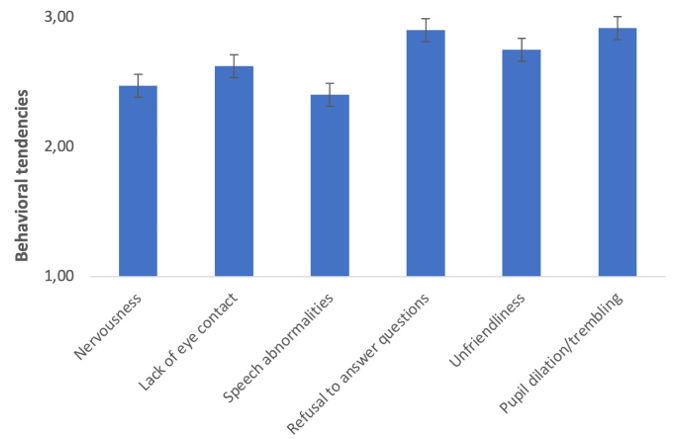
Figure 3: Descriptive Differences in Behavioral Tendencies (Across All Action and Attribution Tendencies) According to Control Scenario, Regardless of Group
Discussion
This study is the first empirical investigation to examine, within the framework of a randomized online case vignette design, the extent to which a medical narcotics identification card for patients (ADHS-Ausweis®) influences the perceptions and decision-making tendencies of police officers in typical control scenarios. The results indicate that the ID has a spontaneous effect in police check situations by reducing the risks typically associated with such checks for patients.
Participants in the ID+ condition reported a higher conviction that the medication found during the check was beneficial to the well-being of the person being checked. In addition, the person concerned was judged to be generally more credible, and there was a stronger conviction that the behavior that was conspicuous from the police's point of view was due to a disorder. These results align well with the work of Corrigan and Ottati and suggest that the presentation of the ID card facilitates a shift in participants' attributional patterns—moving from a perception of delinquency toward the categorization of the individual as a patient [7]. This shift could in turn be accompanied by less suspicious patterns of interpretation and greater tolerance of aversive behavior. The latter seems plausible, as it was consistently shown across all six control scenarios that participating police officers in the ID+ group classified persons checked in the same scenarios as less generally suspicious and also less suspicious in terms of narcotics abuse and trafficking. In addition, there was less tendency to take further measures that were disadvantageous to the patient than in the ID-group. In the action domains of carry out further checks, confiscate medication, consult with superiors, and consider consulting the physician, even in cases of high-risk behavior on the part of the patient, such as refusal to answer questions, unfriendliness, and pupil dilation/trembling, there were consistent significant reductions in all dependent variables for the ID+ condition. These effects thus occurred regardless of which specific characteristic was present.
The effectiveness of the ID demonstrated here is likely to be limited by the interaction dynamics that can arise in police control situations in conjunction with the specific behavioral profiles of people with ADHD, making them particularly vulnerable to adverse outcomes.
This becomes particularly clear in the scenarios involving refusal to answer questions and unfriendliness: Here, the highest levels of police behavior detrimental to patients were observed across both groups (see Figure 3). This indicates that, especially in situations where symptom-related stress reactions turn into behavior that is interpreted as oppositional or disrespectful, the de-escalating effect of even a medical certificate that is perceived as valid is limited. The protective effects of the ID examined here thus seem to unfold primarily when the patient's behavior, as interpreted by the police, falls within a certain tolerance range of cooperative, ambivalent, or potentially pathological behavior.
With regard to behavior perceived as confrontational, the use of psychoeducational interventions that specifically prepare those affected for situations of control appears to be useful. These could include patient-oriented educational offerings that highlight typical risks of escalation and at the same time teach simple, spontaneously accessible heuristic strategies (e.g., standardized self-instructions or short communication scripts). One objective could be to promote cooperative behavior in encounters with the police despite high levels of inner tension, which can be more easily attributed to illness by officers.
An integrative intervention concept that systematically combines psychoeducational content, practical heuristic strategies, and basic, situation-specific legal context information (e.g., on typical powers of intervention and the rights of those affected) seems conceivable in order to reduce the risk of unfavorable outcomes in control situations. The GIVE and FAST skills described in the context of dialectical behavioral therapy (Linehan, 2016) appear to be conceptually compatible here. These skills aim to promote clearly structured, cooperative, and respectful communication behavior even in highly stressful interactions with authority figures, while at the same time maintaining one's own self-respect.
The present findings can be evaluated using stereotype threat-based models such as those developed by Najdowski, Bottoms, and Goff [4]. The present study showed that ambiguously attributable behaviors in the ID+ condition were consistently associated with lower suspicion of narcotics drug dealing, reduced willingness to take potentially escalating measures (further checks, confiscation, consultation, contact with physician) and, at the same time, higher attributions of credibility and health benefits of the medications carried. The presentation of the ID appears to shift attribution patterns from delinquency to a patient role, as indicated by the significantly higher scores for is credible/sincere, meds are for their well- being, and meds are important for person. This indicates a shift in the stereotype threat- related escalation cycle by offering a plausible alternative explanation (medically certified ADHD) for ambiguous behavior (nervousness, restlessness, speech abnormalities).
Limitations
Although the aim of this study was to recruit participants nationwide, the sample was in fact concentrated in the federal states of North Rhine-Westphalia, Hesse, and Bavaria. The generalizability of the results to the entire federal territory is therefore limited. This is particularly relevant in light of the fact that state regulations on police powers—for example, with regard to suspicion-independent identity checks or the designation of weapon-free zones—vary significantly across the federal states. Such legislative differences systematically influence the frequency and procedure of control situations, which may suggest a regional bias in the respondents' answers [12]. In order to make valid statements for the entire federal territory and to be able to differentiate between state-specific effects, it would be useful to increase the number of cases in follow-up studies, fully including all 16 federal states.
Further possible limitations arise from the item characteristics of the POL-11. For example, item 6 (''I consider it necessary to consult with my superiors to clarify how to proceed'') could be interpreted either as escalatory (in the sense of clarifying whether further intervention measures should be initiated) or, on the contrary, as an expression of a more cautious approach oriented toward hierarchies and official routines, in which one's own decision-making activity is deliberately limited and reinsured. Accordingly, it is unclear whether high scores on this item actually reflect an increased willingness to intervene or rather a generalized need for security and reassurance in the face of uncertainty, which makes it difficult to interpret the associated effects.
With regard to other jurisdictions, it should also be noted that this study is anchored in a criminal and police law context that applies to the Federal Republic of Germany: The vignette material, the control scenarios described, and the operationalization of potentially patient-disadvantageous intentions implicitly refer to the regulations applicable in Germany under the Narcotics Law (BtMG), the Weapons Law (WaffG), and the relevant state police laws, which, among other things, the scope and form of suspicion-independent identity checks. In other countries, there are sometimes different criminal, regulatory, and police law frameworks, for example with regard to the classification and conditions for carrying medically prescribed psychostimulants, the powers of intervention during identity checks, or the formal significance or psychological attribution of medical documents certifying a narcotics indication. In addition, there are local differences in police education, de-escalation culture, and organizational routines. Against this background, it is not possible to directly transfer the observed effects of the narcotics identification card examined here to perception, attribution, and decision-making processes in other countries. Replication studies specific to the legal area and country would be necessary to test generalizability [12-15].
Study Funding: The author did not receive any financial support from public, commercial, or non-profit institutions for conducting this study.
Potential Conflicts of Interest: None.
References
- Song, P., Zha, M., Yang, Q., Zhang, Y., Li, X., & Rudan,(2021). The prevalence of adult attention-deficit hyperactivity disorder: A global systematic review and meta-analysis. Journal of global health, 11.
- Praus, P., Moldavski, A., Alm, B., Hennig, O., Rösler, M., & Retz, W. (2023). Epidemiologie, Diagnostik und Therapie der Aufmerksamkeitsdefizit-Hyperaktivitäts-Störung (ADHS) im höheren Lebensalter. Der Nervenarzt, 94(11), 1043-1049.
- Mueller, A. K., Fuermaier, A. B., Koerts, J., & Tucha, L. (2012). Stigma in attention deficit hyperactivity disorder. ADHD attention deficit and hyperactivity disorders, 4(3), 101-114.
- Najdowski, C. J., Bottoms, B. L., & Goff, P. A. (2015). Stereotype threat and racial differences in citizens’ experiences of police encounters. Law and human behavior, 39(5), 463.
- Combs, M. A., Canu, W. H., Broman-Fulks, J. J., Rocheleau,C. A., & Nieman, D. C. (2015). Perceived stress and ADHD symptoms in adults. Journal of attention disorders, 19(5), 425-434.
- Tuente, S. K., Bogaerts, S., & Veling, W. (2019). Hostile attribution bias and aggression in adults-a systematic review. Aggression and violent behavior, 46, 66-81.
- Watson, A. C., Corrigan, P. W., & Ottati, V. (2004). Police officers' attitudes toward and decisions about persons with mental illness. Psychiatric services, 55(1), 49-53.
- Rohrmann, S., Hodapp, V., Schnell, K., Tibubos, A. N., Schwenkmezger,P.,&Spielberger,C.D.(2013).DasState-Trait-Ärgerausdrucks-Inventar-2 (STAXI-2). Deutschsprachige Adaptation des State-Trait Anger Expression Inventory-2 (STAXI-2) von Charles D. Spielberger. Bern: Hans Huber.
- Kelley, H. H. (1973). The processes of causal attribution. American psychologist, 28(2), 107.
- Tversky, A., & Kahneman, D. (1974). Judgment under Uncertainty: Heuristics and Biases: Biases in judgments reveal some heuristics of thinking under uncertainty. science, 185(4157), 1124-1131.
- The jamovi project. (2025). jamovi (Version 2.6) [Computer Software]. https://www.jamovi.org
- Keitzel, S. (2020). Varianzen der Verselbstständigung der Polizei per Gesetz:„Gefährliche Orte “im bundesweiten Vergleich. Kriminologisches Journal, 52(3).
- Fuermaier, A. B., Tucha, L., Koerts, J., Mueller, A. K., Lange,K. W., & Tucha, O. (2012). Measurement of stigmatization towards adults with attention deficit hyperactivity disorder. Plos one, 7(12), e51755.
- Linehan, M. (2016). Dialektisch-Behaviorale Therapie (DBT): Therapiebuch und Handbücher (2 Bände): DBT-Therapiebuch, DBT Handbuch Bd. 1, DBT Handbuch.
- World Medical Association. (2024). WMA Declaration of Helsinki – ethical principles for medical research involving human participants.