
International Journal of Orthopaedics Research(IJOR)
ISSN: 2690-9189 | DOI: 10.33140/IJOR
Impact Factor: 1.6

Research Article - (2025) Volume 8, Issue 3
Pitfalls of MRI in Local Staging of Osteosarcoma of Appendicular Skeleton
2Professor of Radiology, NIMS, Hyderabad, India
3Professor of Pathology, NIMS, Hyderabad, India
4Additional Professor of Orthopedics, NIMS, Hyderabad, India
Received Date: Jun 04, 2025 / Accepted Date: Aug 05, 2025 / Published Date: Sep 11, 2025
Copyright: ©2025 Sujata Patnaik, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Anuhya, K. P., Patnaik, S., Uppin, S. G., Kumar, A. (2025). Pitfalls of MRI in Local Staging of Osteosarcoma of Appendicular Skeleton. Int J Ortho Res, 8(3), 01-06.
Abstract
Osteosarcoma is the most common primary malignant tumour with excess production of osteoid matrix. It accounts for 80% of primary bone Tumours and 2-4% of childhood sarcomas [1]. Triple diagnostic steps - clinical, radiological, and histopathological assessment are essential for appropriate diagnosis and management. Imaging plays a crucial role in the diagnosis, therapeutic planning and follow up. This is an observational study about role of MRI in the evaluation of Osteosarcomas of the appendicular skeleton.
Introduction
Osteosarcoma is the most common primary malignant tumour with excess production of osteoid matrix. It accounts for 80% of primary bone Tumours and 2-4% of childhood sarcomas [1]. Triple diagnostic steps - clinical, radiological, and histopathological assessment are essential for appropriate diagnosis and management. Imaging plays a crucial role in the diagnosis, therapeutic planning and follow up. This is an observational study about role of MRI in the evaluation of Osteosarcomas of the appendicular skeleton.
Material and Method
We analysed the imaging findings in 10 consecutive cases of osteosarcoma of appendicular skeleton which were diagnosed on MRI, operated and histopathologically confirmed. All these patients had undergone plain radiograph and MRI. All were males with average age of presentation at 20.2 years. Distal femur was the commonest site (n=6). Proximal femur was involved in one case. Rest of the tumours were in proximal tibia. 8 cases were conventional Osteosarcoma; there was one case of periosteal osteosarcoma and one case of telangiectatic osteosarcoma. Local staging was done based on MRI and this was correlated with surgical and histopathological findings.
Results
Epiphyseal involvement was noted 9 out of 10 cases (Figure 1). In this study, marrow involvement was missed on MRI in one case (Figure 2) and the rest had marrow involvement on MRI; 5 of the 10 patients, had intra-articular extension on MRI. On surgery there were 2 false positive for intra-articular extension. Seven had muscle- involvement on MRI; however, in 2 cases it was false positive in few of the muscles. Rest of the findings correlated well with histopathology. The details of the 10 patients and their MRI findings are enumerated.

Figure 1: 33 year old male; OS of proximal femur; on radiographs there was a large expansile lytic lesion with foci of calcification in metadiaphysis of femur extending to epiphysis. On axial T1, T2, STIR W MRI images there was no intra articular extension and there is pathological fracture. The lesion is infiltrating adjacent muscles and encasing profunda femoris.

Figure 2: 14 year old male; A case of periosteal OS (chondroblastic) in diaphysis of femur with Sunray spiculation on radiograph and coronal T1W and STIR W images. The intramedullary extent was missed on MRI.
Discussion
Osteosarcoma (OS) is broadly classified as intramedullary and juxtacortical types. Intramedullary tumours can be conventional, telangiectatic (TOS), high grade and small cell osteosarcomas. Juxtacortical tumours can be parosteal, periosteal or high-grade surface osteosarcoma. Conventional OS accounts for 80% of all OS [2]. It may be osteoblastic /chondroblastic /fibroblastic. TOS accounts for 4% of all OS [3]. Parosteal type accounts for 4-6% and periosteal tumours occur less than parosteal OS [4]. High grade surface OS is still rare accounting for less than 1%. Eight out of 10 of our cases were conventional OS, 1 telangiectatic and one was periosteal (Figures-1, 2 & 3). Osteosarcomas occur most commonly in the metaphysis of long bone around the knee (Figures- 4 & 5). Femur is the most involved followed by tibia and humerus, as in our case. All except one that is periosteal OS were metaphyseal. Lesion extends to epiphysis in 75-85% cases [5,6]. We also made a similar observation (Figures- 4 & 5).

Figure 3: 13 year-old male; Talengiectatic OS after chemotherapy. Radiograph reveals lytic lesion with solid periosteal reaction in distal femur. T1 W, STIR axial, coronal, axial T1W contrast images depict the involvement of vastus lateralis muscle. Tumor shows intense heterogenous enhancement

Figure 4: 23 year-old male; OS of upper tibia. Radiographs showing ill-defined sclerotic lesion in metaphysis with adjacent periosteal reaction. Extension to epiphysis and involvement of vastus lateralis and gastrocnemius muscle were noted in STIR W images in coronal and axial sections.
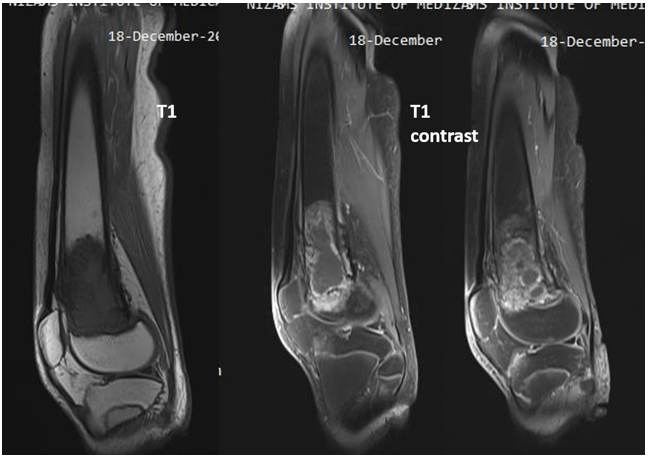
Figure 5: 14 year-old male; OS distal femur, transphyseal extension and no soft tissue involvement in contrast enhanced T1w sagittal images.
Tumors may be osteoblastic, chondroblastic or fibroblastic presenting as intramedullary lesion with cloud- like, Sunburst, Codmanâ??s triangle periosteal reaction (Figurea-2 & 6). Usually, permeative type of eccentric lysis may be seen which may have areas of sclerosis. Cortical destruction and soft tissue component are present. Low grade OS are well differentiated tumor and are less aggressive occurring 3rd or 4th decade or present in metaphysis as lytic /lytic plus sclerotic lesions mimicking fibrous dysplasia. Small cell OS occurs in 2nd and 3rd decades with slightly better prognosis compared to conventional OS. 14% occur in diaphysis. Small cell OS mimics Ewing's sarcoma. They are associated with large soft tissue mass and periosteal reaction in >50% cases.

Figure 6: 18 year old male; OS proximal tibia, radiograph of knee joint AP, Lateral view showing cloud like periosteal reaction. On surgery and MRI there was infiltration of tumor into tibialis anterior and extensor digitorum and popliteus muscles. MRI revealed T2 hyperintensity of vastus lateralis but on surgery, it was uninvolved.
Periosteal OS are chondroblastic with better prognosis. In them, there is cartilage forming into osteoid component. A close differential is myositis ossificans. Our single case of periosteal OS was in 14 years boy in distal femoral diaphysis with adjacent cortical thickening and sunray spiculation and small soft tissue component. Soft tissue component was T2 Hyperintense suggestive of chondroblastic element and was confirmed on HPE (Figure 2). Parosteal OS are low grade and arise from the surface. Most of them occur in 30-40 years of age. 90% occur in metaphysis. Close differential is osteochondroma.
High grade surface OS account for 0.4% of all OS, occurring commonly in diaphysis or metaphysis. Dense ossification, periosteal reaction, cortical thickening and medullary invasion are common. Extensive circumferential bone involvement helps to differentiate it from periosteal OS. MRI is helpful for assessing intramedullary involvement and extension of tumor to soft tissue. Presence of ill-defined enhancing soft tissue adjacent to ossified mass indicates area of dedifferentiation.
Telangiectatic OS occurs in metaphysis with a 10 year- survival in 60%. It occurs in 2nd decade. Extension to epiphysis is common. Fluid- fluid levels are diagnostic hall-mark of the disease. It appears as multiloculated expansile lesion with geographic area of lysis. Occasionally they have sclerotic rim with wide zone of transition, endosteal scalloping and bone destructions. MRI depicts thick, nodular enhancing septae and enhancing soft tissue component. In our study there is a case of TOS in 14-years male child with OS in distal femur. It was treated with chemotherapy and was having solid periosteal reaction and lytic sclerotic lesion. On MRI, it showed multiloculated with enhancing septae, FFL and soft tissue component (Figure 3). Role of chemotherapy in TOS is not well established. However, the survival has increased from 20 % to 60% with patients receiving neoadjuvant chemotherapy [7]. The post chemo-changes in TOS are not well described.
Plain radiograph is the initial investigation in all cases. Radiograph depicts the lesion, characterises it and helps in close differential [8]. All the cases could be diagnosed on radiograph as osteosarcoma except one which was diagnosed as chondrosarcoma because of age and expansile lesion with foci of calcification (Figure 1). In about 20% of cases of osteosarcoma have diagnostic dilemma on plain radiograph.
CT/MRI are meant for characterisation of lesion, local extent, tumor composition, extent of involvement in marrow and extraosseous soft tissue spread and finding skip lesions which are important for treatment planning. CT is helpful for detecting osteoid mineralisation and for guided biopsy. MRI is good for knowing the extent in adjacent soft tissue. PET-CT helps to detect the distant metastases. Advanced MRI techniques like DWI, ADC, DCE MRI, and Perfusion MRI have added advantage to know tumor cellularity and tumor vascularity which are essential for treatment response
Imaging PIT-FALLS on MRI IN Our Series
The main role of MRI is to know the bulk, local extent and the involvement of neuro-vascular bundle (NVB). MRI of entire extremities is advisable to delineate full extent and detect skip lesion if any. OS are heterogeneously hypointense in T1W and hyper-intense on T2W images and show brilliant enhancement. T1W images are helpful in knowing the tumor extent and intramedullary component and also to note the distance of tumor from joint. Intramedullary component appears hypointense in background of higher signal in healthy marrow [9].
Epiphyseal involvement said to be present when there is continuation of tumor hypointensity to epiphysis and show increased enhancement on contrast. It is observed that accuracy of DCE in detection of epiphyseal involvement is less than T1W images. MRI detected epiphyseal extent and cortical break in all our cases (Figures 4 & 5).
Joint involvement presents as nodular thickening of synovium, cruciate ligament involvement in knee and involvement of articular margin. Joint effusion is not specific for joint involvement. In 2 of our cases intra articular extension was suspected on MRI and at surgery there was no actual articular involvement (Figure 7).
There was cortical break with bulging of tumor into joint that has misled the diagnosis. In a study by Schima et al, 10 out of 46 patients, had intra articular extensions which were detected by MRI. Contrast enhanced MRI is better for detecting intra articular extension with a sensitivity of 100% with a specificity of 69% and transphyseal extension with 100% sensitivity and 100% specificity [10]. However, sometimes it may be misdiagnosed as in our case. The relation of extra osseous tumor to adjacent soft tissue and neurovascular bundle is best seen in T2W, fat supressed and STIR sequences. NVB is said to be free when there is clear fat plane between tumor and NVS, abutting when it is obliterated. NVB is said to be unequivocally involved when infiltration or encasement is present. When angle of contact of tumor and NVB is > 180 degree, it indicates encasement. There was a case having ATA; another case showed profunda femoris involvement on MRI and was proven surgically (Figure 1).

Figure 7: A, B, C: Radiograph reveals periosteal reaction in form of Codman triangle. Contrast enhanced T1W MRI sagittal sections reveal enhancing capsule in knee suggestive of intra articular extension. Cross sectional T1 contrast axial depicts enhancement of adductor magnus and vastus lateralis.
Five of the 10, had intraarticular extension on MRI; on surgery there were 2 false positive. 7/10 had muscles involvement on MRI, however 2 cases it was false positive. This is similar to the study by Namrita et al. In their study of 38 cases, 34 had intramedullary extension on MRI, but 35 had intramedullary extent on surgery. Similarly, 2 cases had false positive extra articular extension; 2 cases had false positive intra articular extension [11].
The involved muscles appear hyper intense on T2W images. T2W images are good for knowing tumor extent in muscles (Figure 8), involvement of NVB, and adjacent joint. However, they sometimes, overestimate as noted in 2 of our cases (Figures 7). DEC- MRI may be used to differentiate the tumor infiltration into muscle from oedema as tumor infiltration shows different enhancement compared to the uninvolved muscle.

Figure 8: 14 year-old male; OS of distal femur. Adductor and vastus muscle involvement as shown in T2W axial images
Conclusions
On MRI, though T1W images help in depicting epiphyseal extent and T2W images detect muscle, NVB, intra articular extent in most of cases. Contrast enhanced MRI may be needed to diagnose the extent. Despite contrast MRI, occasionally the diagnosis may be missed on certain situations.
References
- Durfee, R. A., Mohammed, M., & Luu, H. H. (2016). Review of osteosarcoma and current management. Rheumatology and therapy, 3(2), 221-243.
- Kager, L., Zoubek, A., Dominkus, M., Lang, S., Bodmer, N., Jundt, G., ... & COSS Study Group. (2010). Osteosarcoma in very young children: experience of the Cooperative Osteosarcoma Study Group. Cancer, 116(22), 5316-5324.
- Fletcher, C. D., Unni, K. K., & Mertens, F. (Eds.). (2002). Pathology and genetics of tumours of soft tissue and bone (Vol. 4). Iarc.
- Johnson, K., Davies, A. M., Mangham, D. C., & Grimer,R. J. (1999). Parosteal osteosarcoma of a metatarsal with intramedullary invasion. Skeletal radiology, 28(2), 111-115.
- Resnick, D. L., Jacobson, J. A., Chung, C. B., Kransdorf, M. J., & Pathria, M. N. (2024). Bone and joint imaging E-Book. Elsevier Health Sciences.
- Murphey, M. D., Robbin, M. R., MCRae, G. A., Flemming, D. J., Temple, H. T., & Kransdorf, M. J. (1997). The many faces of osteosarcoma. Radiographics, 17(5), 1205-1231.
- Angelini, A., Mavrogenis, A. F., Trovarelli, G., Ferrari, S., Picci, P., & Ruggieri, P. (2016). Telangiectatic osteosarcoma: a review of 87 cases. Journal of cancer research and clinical oncology, 142(10), 2197-2207.
- Casali, P. G., Bielack, S., Abecassis, N., Aro, H. T., Bauer, S., Biagini, R., ... & ESMO Guidelines Committee. (2018). Bone sarcomas: ESMO–PaedCan–EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology, 29, iv79-iv95.
- O'flanagan, S. J., Stack, J. P., McGee, H. M., Dervan, P., & Hurson, B. (1991). Imaging of intramedullary tumour spread in osteosarcoma. A comparison of techniques. The Journal of Bone & Joint Surgery British Volume, 73(6), 998-1001.
- Schima, W., Amann, G., Stiglbauer, R., Windhager, R., Kramer, J., Nicolakis, M., ... & Imhof, H. (1994). Preoperative osteosarcoma: imaging staging of efficacy of MR in detecting joint involvement. Am J Roentgenol, 163, 1171-1175.
- Sachdev N, Singh Y, Vani K, Jain R, Sethi D. (2020). Role of MRI in primary bone tumors and assessing their local Spread. Ind J Scient Research, 9: 47-48