



Research Article - (2020) Volume 5, Issue 1
Parasympathetic and Sympathetic Nervous System Monitoring and Anxiety Like Symptoms: Improved Differentiation and Improved Outcomes
2Director of Cardiac Research,The Heart and Vascular Institute, Germantown, Tennessee, USA
3Franklin Cardiovascular Associates, USA
4Department of Psychiatry, Rowan University School of Osteopathic Medicine, USA
5Medical Director, Franklin Cardiovascular Associates, PA., and Autonomic Dysfunction and POTS Center, Clinical Professor of Medicine, Hahnemann Hospital, Drexel University; Attending Cardiologist, Pennsylvania Hospital of the University of Pennsylvania Health System, USA
Received Date: Mar 25, 2020 / Accepted Date: Mar 30, 2020 / Published Date: Apr 09, 2020
Copyright: ©Joe Colombo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Anxiety disorders (DSM-5) and disorders having anxiety laden symptoms (e.g., PTSD and attention disorders) often include several physiologic symptoms which involve the Parasympathetic and Sympathetic nervous systems (P&S). Our research has identified four P&S disorders that are associated with these symptoms: 1) Sympathetic Excess (SE) secondary to Parasympathetic Excess (PE) as an abnormal stress response, 2) Sympathetic Withdrawal (SW) upon assuming headup posture (standing) associated with Orthostatic Dysfunction, 3) SE upon standing associated with Syncope, and 4) Autonomically mediated cardiac arrhythmia, including Sinus Arrhythmia. All four disorders involve poor brain profusion which is known to contribute to Anxiety-like symptoms. They also contribute to (sub-clinical) depression, another frequent co-morbidity. Resting and challenge P&S responses were assessed noninvasively using the ANSAR Medical Technologies, Inc. (Philadelphia, PA) software (ANX 3.0 autonomic function monitor). Patients diagnosed with Anxiety or Anxiety-like symptoms from a large cardiology practice serving both urban and rural areas were followed with more than one assessment over four years (an average of 3.3 assessments per patient; 50.5% Female; average age of 57 years). Patients diagnosed with Anxiety or Anxiety-like symptoms, with one of the four P&S disorders were also treated for their P&S disorder. Relieving P&S dysfunction within this cohort reduced Anxiety or Anxiety-like symptoms by over 45%. P&S guided therapy for patients with Anxiety or Anxiety-like symptoms, may reduce the burden of Anxiety, improve patient outcomes and quality of life, reduce the risk of suicide, aid the psychiatrist in focusing on the etiology of Anxiety, and reduce healthcare costs.
Introduction
The American Psychiatric Association’s (APA) Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5, copyrighted in 2013), is the APA’s text listing and describing all of the current recognized psychiatric disorders. Anxiety disorders and disorders having anxiety laden symptoms as part of their presentation affect millions of Americans at any given time. Such disorders cause significant interpersonal, occupational, and economic burdens for the patients afflicted, and society as a whole. Anxiety disorders proper include, separation anxiety disorder, selective mutism, panic disorder, agoraphobia, social anxiety disorder [social phobia], specific phobia, and generalized anxiety disorder. Posttraumatic stress disorder [PTSD] and obsessive-compulsive disorder [OCD] used to be classified as anxiety disorders, but now are listed as separate disorders. However, patients experiencing such disorders, including attention disorders, often experience anxiety, or anxiety like symptoms; the latter of which includes physical symptoms generated by their primary psychiatric disorder. Also note that a significant number of patient experiencing clinical depression have co-morbid anxiety symptoms as well. Anxiety disorders and their related disorders affect more patients than diabetes and heart failure combined [1]. Over 70% of patients attempting suicide have at least one anxiety disorder [2]. Local hospitals report ten to twenty Emergency Room visits a day of patients having anxiety or panic attacks, with up to half of them refusing to leave because they believe they are having a heart attack or stroke. Given the growing numbers of patients with anxiety disorder symptoms, it is taking up to six months for a newly diagnosed Anxiety disorders patient to see a qualified Psychiatrist. Some reports indicate that up to 12% of these patients are lost to suicide during these six months.
Anxiety disorders often include several physiologic symptoms, including: sleep difficulties, GI upset, heart palpitations, high blood pressure or difficult to control blood pressure, elevated or high heart rate, abnormal sweating, lightheadedness, and experiences of depersonalization and de-realization. These physiologic symptoms all involve the Parasympathetic and Sympathetic nervous systems (P&S). In fact, it is possible that this combination indicates that there are abnormalities (excesses) in both systems [3]. Stress plays a significant role in the pathology of anxiety disorders [4]. Stress includes Psychosocial stress at the systemic level and growing evidence of Oxidative Stress at the cellular level [5-9]. Oxidative Stress significantly affects the P&S and is associated with autonomic disorders such as Neurogenic Orthostatic Hypotension [6]. Orthostatic dysfunction is arguably one of the most debilitating of autonomic disorders [7,8]. The physiologic symptoms, above, plus lightheadedness, cognitive and memory difficulties, “Brain Fog,” sex dysfunction, shortness of breath, and persistent fatigue (not necessarily Chronic Fatigue Syndrome) help to define Anxiety- Disorder-Like (“Anxiety-Like”) symptoms.
P&S function includes proper tissue perfusion, especially brain perfusion. With poor brain perfusion, patients demonstrate sub- clinical depression. However, many also complain of anxiety-like symptoms. The latter may be associated with “adrenaline storms” that cycle anxiety as the brain attempts to regain proper perfusion. There are four P&S disorders that are associated with these anxiety- like symptoms:
• Sympathetic Excess (SE) secondary to Parasympathetic Excess (PE) as an abnormal stress response [3],
• Sympathetic Withdrawal (SW) upon assuming head-up posture (standing) associated with orthostatic dysfunction [6, 9],
• Sympathetic Excess (SE) upon standing associated with syncope [23] and
• Autonomically mediated cardiac arrhythmia, including Sinus Arrhythmia [10].
We discuss our findings in a large cardiology cohort. In general: 1) one or more of these P&S disorders, together with primary Anxiety, may all be co-morbid, and 2) all may be treated simultaneously, resulting in improved quality of life and reduced morbidity and mortality risk [1].
Methods
A database of 3670 consecutive, serial patients (50.5% Female; average age of 57 years; age range: 12 to 100 years) was followed in a large cardiology practice drawing from both urban and suburban populations. P&S function was assessed noninvasively using the ANSAR Medical Technologies, Inc. (Philadelphia, PA) software (ANX 3.0 autonomic function monitor). The ANX 3.0 computes simultaneous, independent measures of P&S activity based on continuous, time-frequency analysis of Heart Rate Variability (HRV) with concurrent, continuous, time-frequency analysis of respiratory activity (RA). Time-frequency analyses employ a normalized CMORL wavelet with a Q of 5 and a spectral update of 4 seconds.
This method facilitates reading P&S responses in the presence of arrhythmia [10]. Given that patients with anxiety-like symptoms often present with palpitations and possible arrhythmia (generally benign), arrhythmia patients were included in this analysis. However, the presence of arrhythmia may change the way in which P&S reports are interpreted. There are 943 patients presenting with a high burden of ectopy (a run of more than two consecutive arrhythmic heart beats). From standard HRV analysis ectopy may be corrected if they occur as singlets or doublets [11,12]. A run of three or more is considered significant and must be presented to the physician. If the arrhythmia is isolated as singlets or doublets, FDA cleared software is employed to normalize the ectopic beats, permitting the usual interpretation. With significant numbers of ectopic beats the interpretation changes, and the timing of the ectopy and Sympathovagal Balance at rest remain the only valid data upon which to base interpretation [11].
Patients were followed with more than one assessment over four (4) years (an average of 3.3 assessments per patient). The mean time between assessments is 442.7 days. At baseline, patients carry diagnoses of primary Anxiety (9.1%), Orthostatic Dysfunction (30.5%, including 15.7% with pre-clinical or clinical Orthostatic Hypotension and 1.5% with pre-clinical or clinical Postural Orthostatic Tachycardia Syndrome), (pre-clinical) Syncope (8.4%), cardiovascular disease (CVD) or a condition at high risk of future CVD, such as hypertension (32.7%), heart failure (35.2%), history of MI (16.2%), type 2 diabetes (36.2), renal disease (17%), or COPD (8.7%). Patients were on standard therapy [12].
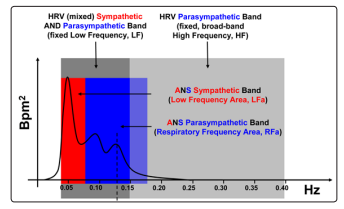
HRV-alone analyses compute mixed measures of P&S activity. For example, spectral HRV analyses result in a Low Frequency (LF) and a High Frequency (HF) term [13,14]. LF is a mix of both P&S activity (see Figure 1) unless the subject’s breathing rate is greater than about 13 breaths per minute [12,13]. HF is a broad-band term [12,13] (see Figure 1), more than twice as broad as the known Parasympathetic frequency range [15 -19]. Therefore, even if the subject’s breathing rate is > 13 breathes/min, the HF term is mixed with noise, including harmonics. Both LF & HF require assumption and approximation to specify P&S activity.
Figure 1: A spectral domain comparison of the LFa & RFa method [8] and the LF & HF method [12,13], see the Methods section for abbreviations. The vertical broken line represents the Respiratory frequency over the four second measurement period. The Respiratory frequency is independently computed in the Respiratory Activity spectrum (not shown) and then transferred here, to the HRV spectrum, to locate the RFa (Parasympathetic) spectrum. In this way, the RFa spectrum is based on the breathing rate of the subject. In this example, the Respiratory frequency is 0.125Hz (equivalent to 7.5 breathes per minute). The LF spectrum is represented in dark grey, from 0.04Hz to 0.15Hz [12,13]. The HF spectrum is represented in light grey, from 0.15Hz to 0.40Hz [12,13]. The RFa spectrum, in this example, is from 0.065Hz to 0.185Hz [8]. The RFa is computed from a frequency range centered on the Respiratory frequency (0.125Hz, see above) and moves as the Respiratory frequency moves [8]. The LFa spectrum, in this example, is from 0.04Hz to 0.065Hz. The LFa is computed as the (fixed) LF frequency range (0.04Hz to 0.15Hz) minus the portion of the RFa frequency range that overlaps the LF frequency range (in this example 0.065Hz to 0.15Hz) [8]. LFa, in (beats per minute)2 or bpm2, represents Sympathetic activity and RFa, in bpm2, represents Parasympathetic activity [8,14-16, 23].
In order to eliminate the need for assumption and approximation required by LF & HF, independent spectral analyses of RA are added to spectral analyses of HRV. This second independent P&S measure (RA) satisfies the algebraic requirement for a system with two independent components, fully characterizing the system, eliminating the need for assumption and approximation. Wavelet and analysis eliminates the time-frequency approximations required by Fourier Transforms and enables a significantly shorter data collection time to compute P&S activity. This enables autonomic transients and the dynamic activity of P&S interactions to be captured and analyzed. The resulting P&S terms are Respiratory Frequency area (RFa) and Low Frequency area (LFa), respectively, and Sympathovagal Balance (SB = LFa/RFa) is computed as a true ratio of independent parameters [8]. See the differences between LF & HF and LFa & RFa in Figure 1 [8].
The clinical study employed to determine P&S activity includes four well-known autonomic challenges, separated by resting baseline periods. These six periods are: A) resting Baseline, B) Deep Breathing, C) baseline, D) Valsalva maneuvers, E) baseline, and F) Stand (postural change). The stand challenge, in the clinical study used in this article is a postural change challenge, which is equivalent tilt-testing [9,16]. The stand challenge is a physiologic activity and therefore inherently safer and more comfortable for the patient, arguably leading to more reliable results [7, 23]. The stand challenge enables autonomic testing to be performed in smaller clinics, and in shorter time periods. From a safety point of view, the independent measures of P&S activity obviate the need for overt symptoms to be demonstrated, thereby inherently improving the safety of the study.
The time requirement, as well as the safety factor, is further improved with the implementation of a spectral analysis technique that eliminates the time-frequency compromise: the Wavelet Transform [18 -19]. P&S Monitoring employs the Wavelet Transform, along with the appropriate time and safety considerations. Non-invasive BPs were taken during each phase of the clinical study [9, 20]. This is an observational study. Patient testing and clinical outcomes measures were collected as an authorized part of the subjects’ care and treatment given their clinical history. All data were handled according to HIPPA regulations. Data were analyzed, statistically, with SPSS v 22.0, with the null hypothesis indicating significance at p ≤ 0.05.
Therapy Options Pharmaceutical Therapy Options
Pharmaceutical therapy options were prescribed based on patient history [21]. In general they included the following. For SW, 2.5mg Midodrine titrated as needed from qd to tid. The first dose was recommended around dinner, four hours before laying down, when BP tended to be lowest. However, morning doses were recommended for patients reporting significant symptoms at that time; typically POTS patients. Midodrine was contraindicated for patients with supine hypertension or those with BPs > 160/90. For PE (either Valsalva or Stand), 10.0 mg, qd, dinner Nortriptyline (primary) or 20mg, qd, dinner Duloxetine (secondary), titrated as needed. For (stand) SE, therapy depended on the differential. If SE was demonstrated with PE indicating (pre-clinical) Vasovagal Syncope, then PE therapy was followed [15]. If SE was demonstrated with a drop in Heart Rate from resting to stand indicating (pre-clinical) Neurogenic Syncope, volume building and often Midodrine helped to treat the stand SE. For autonomically mediated arrhythmia, the rest of the P&S test helped to determine whether the arrhythmia was due to P or S abnormality or not autonomic and treated accordingly [19].
Non-Pharmaceutical Therapy Options
In general, psychosocial stress reduction was recommended with history-specific antioxidant and supplement recommendations to reduce oxidative stress and improve blood flow. Non-Pharmaceutical therapy options were offer if patients were intolerant or unresponsive to the pharmaceutical options. For SW, 600 mg tid, Alpha-Lipoic Acid, titrated as needed and tolerated was recommended [6,11]. For PE, six months of walking at no more than two miles per hour for 40 contiguous minutes per day, for more than 5 days per week [17]. Often this was augmented, early in the therapy especially if the patient reported significant sleep difficulties, by 20 minutes of supine, 15° head-down posture around two hours before bed- time and up to three times per day, as needed given no supine hypertension, head pressure or additional headache. Head-down posture was also recommended to help with stand SE. Autonomically induced arrhythmia was treated based on underlying etiology.
This is an observational study. Patient testing and clinical outcomes measures were collected as an authorized part of the subjects’ care and treatment given their clinical history. All data were handled according to HIPPA regulations. Data were analyzed, statistically, with SPSS v 22.0, with the null hypothesis indicating significance at p ≤ 0.05.
Results
Table 1 presents the percentages of primary Anxiety or Anxiety- Like diagnoses with the percentages of the cohort that demonstrate P&S dysfunctions that may be associated with Anxiety and that underlie Anxiety-Like symptoms. Only 9.1% of this patient population was diagnosed with primary Anxiety, but 55.2% were diagnosed with Anxiety-Like symptoms or the risk of Anxiety- like symptoms. The majority of those with the risk of Anxiety- like symptoms demonstrated challenge PE (58.3%). A significant portion demonstrated SW (47.9%), which is associated with (pre- clinical) orthostatic dysfunction. Stand SE, associated with possible (pre-clinical) Syncope, was demonstrated by 4.2% of this cohort. Often with Anxiety-Like symptoms, these three P&S dysfunctions are co-morbid (41.3%). In the case of this cohort: Challenge PE and SW were concurrently demonstrated by 25.0% of the cohort, Challenge PE and Stand SE were concurrently demonstrated by 6.2%, and Stand SE and SW were concurrently demonstrated by 10.1%. Resting PE is associated with fatigue and (sub-clinical) depression, and is demonstrated by 12.5% of this cohort.
Note, these are difficult differentials to diagnose through symptoms. In the case of Challenge PE with SW, the PE often masks the SW. Here, the SW is implicated by a drop in BP from resting to stand. With Stand SE (a beta-adrenergic response) and SW (an alpha- adrenergic response), Stand SE is documented as an instantaneous result and SW is documented as an average result. In other words, the SE is documented as a peak Sympathetic response to standing that is comparable to, or greater than the peak Sympathetic response to Valsalva. Of course this makes no sense physiologically. The stand Sympathetic response should be significantly lower than the Sympathetic response to a series of short Valsalva maneuvers which are known to be very significant Sympathetic challenges. (Valsalva maneuvers > 20 seconds are the well-known, and significant, Parasympathetic challenges.) The SW is overtly demonstrated as a decrease in the average Sympathetic response at rest as compared with the average Sympathetic response to the postural change challenge (standing). Also, while both of these are Sympathetic responses, and it may be difficult to imagine how the Sympathetics could increase (SE) and decrease (SW) at the same time. The fact is that SE is a beta-adrenergic response and SW is an alpha-adrenergic response. In other words, these are two responses from two different sub-systems within the Sympathetic nervous system.
At baseline, most patients were prescribed either SSRIs or Benzodiazepines, these were typically high dose, and more than a fourth of the patients were prescribed multiple anxiolytics. While there was a noted reduction in the occurrences of Anxiety and Anxiety-Like symptoms, these symptoms still presented, especially with stress.
Upon the first follow-up P&S study (typically between 3 and 12 months after the baseline study) there is little change in the clinical condition of these patients; there is only a 5.1% decrease in the numbers of Anxiety-Like symptoms reported and no change in the primary Anxiety diagnoses (Table 1). The only exception is a significant reduction (65.1%) in the percent of the population that were diagnosed with multiple P&S dysfunctions. While the numbers of co-morbid conditions decreased, P&S dysfunctions persisted, and the persistent dysfunctions were often not treated until they were unmasked or if the patient seemed unresponsive to the first therapy. The persistent P&S dysfunctions seem to be the reason for the persistent Anxiety-Like symptoms.
The reason for the little change at this time is that the P&S itself takes time to change, and a change in the P&S is required before organ function changes, which then will change symptoms. Often the first follow-up (at 3 months) is an encouragement visit to demonstrate that the P&S is changing for the better.
Table 1: Percent of cohort with diagnoses of Anxiety or Anxiety-Like symptoms and underlying P&S dysfunction
|
Diagnoses (Dx) |
Primary Anxiety |
Resting PE |
Challenge PE* |
SW |
Stand SE |
Co-Morbid Dx |
Anxiety-Like Sx |
|
Baseline |
9.1 |
12.5 |
58.3 |
47.9 |
4.2 |
41.3 |
55.2 |
|
First Follow-up |
9.1 |
5.2 |
37.2 |
50.6** |
3.8 |
14.4 |
50.1 |
|
Final Follow-up |
7.1 |
2.2 |
8.9 |
12.4 |
0.6 |
4.3 |
13.5 |
* PE demonstrated during Sympathetic challenges: a series of short (< 15 sec) Valsalva maneuvers, or a quick postural change (standing from relaxed sitting) with five or more minutes of quiet standing.
** Stand PE often masks (stand SW). Treating the former often unmasks the latter.
The final follow-up P&S study was typically one to two years following the first follow-up study. This is when significant P&S changes were demonstrated. A reason for the significant amount of time between the first and final follow-up study is that patients reported that the number, and frequency, of symptoms has significantly decreased. This includes the primary Anxiety patients, suggesting that perhaps not all of these patients had primary Anxiety.
Therapy modification after the first follow-up study, in general, was not significant in terms of the type or number of different medications (Table 2), with Tri-Cyclics, SNRIs, and Hyoscyamine being increased; typically as a result of switching from a Benzodiazepine, SSRI or other medications with anti-cholinergic activity (e.g., Clonidine). However in many cases the dosages were reduced to prevent side- effects. By the final follow-up, many patients with Anxiety-Like symptoms had self-weaned from their anxiolytic medications. The remainder had their P&S therapies discontinued given that their P&S nervous systems had stabilized. Those remaining on medication required the low dosages to maintain.
Table 2: Percent of cohort prescribed anxiolytics (anti-cholinergics)
|
Medications |
SSRIs |
SNRIs |
TriCyclics |
Benzos |
Spiriva |
Hyoscyamine (prn) |
Other Anti- Cholinergics |
Multiples |
|
Baseline |
27.1 |
4.2 |
4.2 |
22.9 |
2.1 |
4.8 |
14.6 |
28.0 |
|
First Follow-up |
24.7 |
5.3 |
13.6 |
18.2 |
2.1 |
6.5 |
11.4 |
26.4 |
|
Final Follow-up |
5.4 |
0.8 |
5.5 |
0.4 |
1.8 |
5.7 |
2.6 |
3.1 |
Discussions
P&S Monitoring uniquely enables simultaneous, yet (mathematically) independent, measures of P&S activity. Other autonomic measures, measure total autonomic function and force assumption and approximation to theorize P&S activity. As a result, additional autonomic dysfunctions are identified which seem to provide more information to help diagnose and treat the complicated symptomatology of Anxiety. This additional information is especially helpful when some of the diagnoses are co-morbid.
PE in response to a stressor (Valsalva or stand challenge) is an abnormal stress response. It is usually assumed that the Parasympathetics decrease during the SE response. However, that happens only in healthier individuals. In these cases, SE secondary to (Challenge) PE, as often observed with P&S monitoring, is also an abnormal stress response [3]. This abnormal P&S response may help to further define conditions that involved both depression and anxiety. It helps to explain depression or fatigue (PE) with sympathetic symptoms: palpitations or arrhythmia, high or difficult to manage BP or HR, nighttime sleeplessness, etc. In these cases, SE should betreated as secondary to PE, given that the Parasympathetics establish the baseline around which the Sympathetics react. This is a case when the “see-saw” model of the autonomic nervous system fails. The Parasympathetics abnormally increase and force the Sympathetics to increase excessively. Unfortunately, the parameters measured (HR, BP, Cardiac Output, etc.) are Sympathetically mediated. As a result, the Sympathetics are treated (inhibited in some way) as the primary dysfunction. This only serves to exacerbate the PE, forcing the body to defeat the therapy by using some other Sympathetic pathway (there are more Sympathetic pathways than medicine can block). As a result, the patient seems to be unresponsive leading to excessive dosing, or non-compliance (which may be worse).
Challenge PE may be diagnostically helpful in other ways. If both PE & SE are demonstrated with standing, indicating possible (pre- clinical) Syncope, the PE differentiates the diagnosis as possible (pre-clinical) Vasovagal Syncope. In another way, Stand PE may mask SW, this is especially true if Stand PE is accompanied by a decrease in BP from rest to stand. In both of these cases treating both abnormal P&S states helps to relieve symptoms. In all of these ways, PE precipitates reduced blood flow and thereby poor brain and possibly coronary perfusion, which seems to trigger the Anxiety-Like symptoms.
SW upon assuming head-up posture (standing) is associated with orthostatic dysfunction [9]. Orthostatic Intolerance seems to underlie all neurogenic orthostatic dysfunctions, and may be considered the pre-clinical state prior to overt symptoms or clinically defined conditions. As overt symptoms present (e.g., lightheadedness and palpitations) significant changes in HR or BP also present helping to differentiate the sub-forms of orthostatic dysfunction: POTS as SW with an abnormal increase in HR with stand, and (Neurogenic) Orthostatic Hypotension as SW with a significant decrease in BP with stand. Orthostatic dysfunction is also known to reduce blood flow to the heart and brain thereby causing poor brain and coronary perfusion, and triggering Anxiety-Like symptoms.
As mentioned, Stand SE is associated with possible (pre-clinical) Syncope [23]. P&S Monitoring helps to differentiate the sub-forms of Syncope as well as provide a better differential between POTS and Vasovagal Syncope, or identify both when co-morbid. These and other (resting) P&S dysfunctions, may all also be associated with, or mediate, cardiac arrhythmias. Knowing which autonomic branch is abnormal may provide more information upon which to base therapy plans and thereby improve outcomes. For example, Atrial Fibrillation (AFib) may be associated with Anxiety in some cases [24]. It is well known that autonomic dysfunction is associated with AFib in approximately 80% of the patients and, in about 80% of those, the autonomic dysfunction is a Parasympathetic dysfunction. This indicates that only 64% of those with Anxiety and AFib treated with anti-cholinergics are actually being helped. A common autonomically mediated cardiac arrhythmia, is Sinus Arrhythmia, which, like AFib, may be Parasympathetically or Sympathetically induced. Either way, reducing arrhythmia, and its related sensations, and improving brain perfusion helps to reduce Anxiety-Like symptoms.
It is reported above that the first follow-up P&S study was often three to four months after the baseline study. This was recommended for two reasons. First it was an encouragement study. While the patient is believed to be compliant, there may be little evidence of symptom change. This is due to the fact that the organs demonstrate symptoms, the P&S nervous systems drive the organs, and they function collectively to maintain normal organ function, even if individually they are dysfunctional. In the absence of changes in symptoms, P&S Monitoring provides evidence of change. Second, it was an opportunity for the physician to further titrate therapy, specifically to the individual patient.
Limitations
P&S Monitoring is a non-invasive test. This cohort is limited to one region of the country from one private practice. A larger more diversified study is recommended.
Conclusion
Treating the etiology underlying Anxiety-Like symptoms generally normalizes patients’ physiology, thereby reducing morbidity and mortality risk. Relieving P&S dysfunction within this cohort reduced Anxiety or Anxiety-like symptoms by over 45%. While it seems to help to restore proper brain perfusion (as evidenced by a significant reduction in reported lightheadedness and “Brain Fog,” and reported improvements in cognitive and memory function, and sleep quality), it does not often treat primary Anxiety. Only 2% in this cohort were relieved of primary Anxiety with P&S guided therapy, see Table 1. However, it does seem to improve the quality of life for these patients by reducing lightheadedness, sleep and GI symptoms, BP & HR excesses, “Brain Fog,” persistent fatigue, shortness of breath,etc. It may also help to reduce the risk of suicide. As a result, it may help to focus the patient on the actual etiology under-lying the primary Anxiety. P&S guided therapy for patients with Anxiety or Anxiety-like symptoms, may reduce the burden of Anxiety, improve patient outcomes and quality of life, reduce the risk of suicide, aid the psychiatrist in focusing on the etiology of Anxiety, and reduce healthcare costs.
References
- https://www.cdc.gov/
- Nepon J, Belik SL, Bolton J, Sareen J (2010) The relationship between anxiety disorders and suicide attempts: findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Depress Anxiety 27: 791-798.
- Tobias H, Vinitsky A, Bulgarelli RJ, Ghosh-Dastidar S, Colombo J, etal. (2010) Autonomic nervous system monitoring of patients with excess parasympathetic responses to sympathetic challenges – clinical observations. US Neurology 5: 62-66.
- Bystritsky A, Khalsa SS, Cameron ME, Schiffman J (2013) Current diagnosis and treatment of anxiety disorders. P T 38: 30-57.
- Bouayed J, Rammal H, Soulimani R (2009) Oxidative stress and anxiety: relationship and cellular pathways. Oxid Med Cell Longev 2: 63-67.
- Murray GL Colombo J (2019) (R)Alpha Lipoic Acid is a Safe, Effective Pharmacologic Therapy of Chronic Orthostatic Hypotension Associated with Low Sympathetic Tone. Int J Angiol. 28: 188-193.
- Vinik AI, Maser RE, Nakave AA (2007) Diabetic cardiovascular autonomic nerve dysfunction. US Endocrine Disease 2: 66-74.
- Vinik A, Ziegler D (2007) Diabetic cardiovascular autonomicneuropathy. Circulation 115: 387-397.
- Arora RR, Bulgarelli RJ, Ghosh-Dastidar S, Colombo J (2008) Autonomic mechanisms and therapeutic implications of postural diabetic cardiovascular abnormalities. J Diabetes Science and Technology 2: 568-571.
- Nanavati SH, Bulgarelli RJ, Vazquez-Tanus J, Ghosh-Dastidar S, Colombo J, etal. (2010) Altered autonomic activity with atrial fibrillation as demonstrated by non-invasive autonomic monitoring. US Cardiology 7: 47-50.
- Colombo J, Arora RR, DePace NL, Vinik AI (2014) Clinical Autonomic Dysfunction: Measurement, Indications, Therapies, and Outcomes. Springer Science + Business Media pp 1-3.
- DePace NL, Bateman J, Yayac M, Oh J, Siddique M, etal. (2018) Improved patient outcomes by normalizing sympathovagal balance as measured by parasympathetic and sympathetic monitoring: the benefits of carvedilol. Cardiovascular Disorders and Medicine 3: 1-5.
- Malik M (1996) The Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability, standards of measurement, physiological interpretation, and clinical use. Circulation 93: 1043-1065.
- Malik M (1996) The Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability, standards of measurement, physiological interpretation, and clinical use. European Heart Journal. 17: 354-381.
- Akselrod S, Gordon S, Ubel FA, Shannon DC, Berger AC, etal. (1981) Power spectrum analysis of heart rate fluctuations: a quantitative probe of beat-to- beat cardiovascular control.Science 213: 213-220.
- Bloomfield DM, Kaufman ES, Bigger JT, Fleiss J, Rolnitzky L, etal. (1997) Passive head-up tilt and actively standing up produce similar overall changes in autonomic balance. Am Heart J 134: 316-320.
- Vinik AI, Bloom HL, Colombo J (2014) Differential effects of adrenergic antagonists (carvedilol vs. metoprolol) on parasympathetic and sympathetic activity: A comparison of measures. Heart International. Heart Int 9: 7-14.
- Xavier R, Laranjo S, Ducla-Soares E, Andrade A, Boto JP, etal. (2008) The Valsalva Maneuver Revisited by Wavelets. Rev Port Cardiol 27: 435-441.
- Piña IL, Di Palo KE, Ventura HO (2018) Psychopharmacology and Cardiovascular Disease. JACC 71: 2346-2359.
- DePace NL, Bateman JA, Yayac M, Oh J, Siddique M, etal. (2018) Acosta C, Pinales JM, Vinik AI, and Bloom HL. Improved Patient Outcomes by Normalizing Sympathovagal Balance: Differentiating Syncope-Precise Subtype Differentiation Leads to Improved Outcomes. Cardiology Research and Practice 8, pp .
- Thompson TS, Barksdale DJ, Sears SF, Mounsey JP, Pursell I, etal. (2014)The effect of anxiety and depression on symptoms attributed to atrial fibrillation. Pacing Clin Electrophysiol 37: 439-446.
- Akselrod S (1988) Spectral analysis of fluctuations in cardiovascular parameters: a quantitative tool for the investigation of autonomic control. Trends Pharmacol Sci 9: 6-9.
- Aysin B, Aysin E (2006) Effect of respiration in heart rate variability (HRV) analysis. Conf Proc IEEEEng Med Biol Soc 1: 1776-1779.
- Aysin B, Aysin E, Colombo J (2007) Comparison of HRV analysis methods during orthostatic challenge: HRV with respiration or without? IEEE Engineering in Medicine and Biology.
- Keissar K, Davrath LR, Akselrod S (2009) Coherence analysis between respiration and heart rate variability using continuous wavelet transform. Philos Transact A Math Phys Eng Sci. 367: 1393-406.
- Olivera MM, Santos-Bento M, Xavier R, Rocha I, Ducla- Soares J-L, et al. (2007) Wavelet analysis for the evaluation of cardiovascular autonomic nervous response to postural change in healthy subjects in relation to age. Second Joint Meeting of the European Federation of Autonomic Societies and the American Autonomic Society, Vienna, Austria. Clinical Autonom Res 17: 301.
- Olivera MM, Feliciano J, da-Silva N, Alves S, Xavier R, et al. (2007) Wavelet Analysis for the evaluation of autonomic nervous system during orthostatic stress in paroxysmal atrial fibrillation. Second Joint Meeting of the European Federation of Autonomic Societies and the American Autonomic Society, Vienna, Austria. Clinical Autonom Res. 17: 301.
- Olivera MM, da-Silva N, Timoteo AT, Feliciano J, Silva S, et al. (2009) Alterations in autonomic response during head-up tilt testing in paroxysmal atrial fibrillation patients: a wavelet analysis. Rev Port Cardiol 28: 243-257.
- Ducla-Soares JL, Santos-Bento M, Laranjo S, Andrade A, Ducla-Soares E, et al. (2009) Wavelet analysis of autonomic outflow of normal subjects on head-up tilt, cold pressor test, Valsalva manoeuvre and deep breathing. Exp Physiol 92: 677-686.
- Xavier R, Laranjo S, Ducla-Soares E, Andrade A, Boto JP, et al. (2008) The Valsalva Maneuver Revisited by Wavelets. Rev Port Cardiol 27: 435-441.
- Piña IL, Di Palo KE, Ventura HO (2018) Psychopharmacology and Cardiovascular Disease JACC 71: 2346-2359.