




Case Report - (2024) Volume 3, Issue 1
Papillary Thyroid Carcinoma Synchronous with High-Grade Non-Hodgkin's Lymphoma: A Case Report
2Faculte de medecine et de pharmacie /universite Mohamed V Rabat, Morocco
Received Date: Jan 23, 2024 / Accepted Date: Feb 15, 2024 / Published Date: Feb 26, 2024
Copyright: ©Â©2024 Zakaria El Hafi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Hafi, Z. E., Hjaouj, K., Bencheikh, R., Benbouzid, M. A., Oujilal, A., et al. (2024). Papillary Thyroid Carcinoma Syn-chronous with High-Grade Non-Hodgkin's Lymphoma: A Case Report. J Surg Care, 3(1), 01-03.
Abstract
Papillary thyroid carcinoma (PTC) is the most common thyroid carcinoma, accounting for up to 90% of all thyroid malignancies. The association with a hematological malignancy is very rare, representing an incidence of only 7%. We present a case of synchronous papillary thyroid cancer and non-Hodgkin's lymphoma (NHL) and discuss possible dilemmas in diagnosis and treatment. A 60-year-old woman with no medical or radiation history presented with a hard, immobile left supraclavicular swelling. Cervical ultrasound showed the presence of a suspicious-looking supraclavicular adenopathy with two right lobar thyroid nodules classified EU-TIRADS 4. We performed a total thyroidectomy with right central latero-cervical functional left curage and excision of the left supraclavicular adenopathy. Pathological examination revealed papillary thyroid carcinoma synchronous with high-grade non- Hodgkin's lymphoma. After a multidisciplinary consultation, the patient received six courses of chemotherapy before undergoing irratherapy. This article highlights the importance of a multidisciplinary approach in the absence of consensus, given the rarity of this case.
Keywords
Papillary Carcinoma, Thyroid, Non-Hodgkin's Lymphoma, A Case Report.
Introduction
Differentiated thyroid cancer (DTC) is the most common endocrine malignancy, and the most common is papillary thyroid carcinoma. This is the most indolent form of the disease, and its prognosis is excellent. The association of DTC with a hematological malignancy is very rare, representing an incidence of only 7% [1]. The literature review shows very few cases of this entity, which presents a diagnostic and therapeutic dilemma. We report the case of a patient presenting with papillary thyroid carcinoma synchronous with non-Hodgkin's lymphoma.
• Case history
Patient information: A 60-year-old woman, with no history including no previous cervical irradiation, who consulted for recent-onset left supraclavicular and right lateralized basi-cervical swelling with no other associated signs.
• Clinical findings
Presence of a mass of firm consistency on the right side of the thyroid lodge that ascends on swallowing without inflammatory signs opposite, and presence of a firm left supra-clavicular mass fixed to the deep plane. The rest of the clinical examination was normal.
• Chronology
In view of this clinical examination, pre-therapeutic and iconographic assessments were requested.
Diagnostic Approach
Ultrasound revealed an enlarged thyroid gland at the expense of its right lobe, which was the site of two contiguous nodules with the same characteristics: oval with regular contours, well defined, predominantly tissue echostructure, partially hypoechoic and surrounded by a thin hypoechoic halo, the larger measuring 14 x 22 mm, both classified as EU-TIRADS IV. The ultrasound revealed a left supraclavicular adenopathy, roughly oval in shape, with regular contours, a mixed echostructure, predominantly cystic with a hypoechoic fleshy portion, and an eccentric hilum measuring 19 mm in minor axis. Cytopuncture was performed on the largest nodule, showing a dense, undifferentiated cell population consisting of diffuse sheets of cells with ill-defined cytoplasms and anisokaryotic, hyperchromatic nuclei with dense, finely nucleolated chromatin, and a necrotic-hemorrhagic background. According to the Bethesda classification: Cytology classified as "suspicious of malignancy" category V.
Therapeutic Intervention
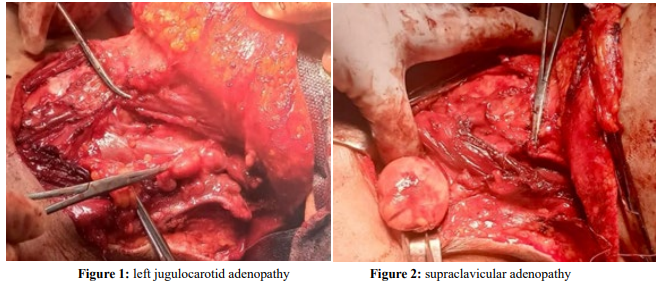
The patient underwent total thyroidectomy with central bilateral and left laterocervical lymph node dissection in view of several left jugulocarotid adenopathies (Figure 1) and excision of the left supra-clavicular adenopathy (Figure 2).
Histological study of the right thyroid lobe revealed a nodule well bounded by a thin capsule made up of vesicles of variable size with areas of round thyroidocyte nuclei displaying the nuclear criteria of papillary carcinoma, interstitial fibrosis and foci of calcifications, concluding in the presence of a non-invasive vesicular thyroid tumour with papillary-type nuclei (NIFT-P according to WHO 2022 terminology) measuring 3.7 cm in long axis. As for adenopathy, a smooth-surfaced nodule measuring 4.5x4x2.5 cm was found, with a pinkish-white <
Follow-up and Results of Surgery
Following a multidisciplinary consultation meeting, the patient was first referred to medical oncology, where she received six cycles of chemotherapy. R-CHOP, this protocol includes the administration of 04 molecules Rituximab - Cyclophosphamide -. Hydroxy Doxorubicin – Vincristine R-CHOP is based on immunochemotherapy, i.e. the combination of chemotherapy and immunotherapy to stimulate the body's immune defenses. The treatment combines a monoclonal antibody (R on day 1, D1), chemotherapy (CHO on D1) and corticosteroids (Prednisolone from D1 to D5). She was then referred to endocrinology and nuclear medicine for iratherapy followed by hormone replacement therapy. One year after surgery, the patient was in good general condition, with no haematological or other signs, and complete disappearance of cervical adenopathy with hormonal stabilization.
Discussion
The coexistence of papillary thyroid carcinoma and lymphoma is extremely rare. Few cases have been reported in the literature. [2,3] Numerous studies have reported the association of thyroid pathology with lymphoma in patients treated with radiotherapy [4]. Several other studies have attempted to explain the link between Thyroid Papillary Carcinoma and extra-thyroid malignancies, arguing that "the long-term carcinogenic effects of certain anti-cancer treatments could be responsible for a second cancer" [1]. However, our patient was diagnosed simultaneously with DTC and NHL. Up to 20-50% of patients with papillary thyroid carcinoma have cervical metastases at the time of diagnosis. The most common site for regional metastases is the central VI and rarely the lateral neck and anterior mediastinum [5]. Similarly, lymph node involvement is common in lymphoma [6].
In our patient, a fine-needle cytopunction of the supra-clavicular lymph node should also have been performed to confirm the diagnosis of lymphoma and exclude lymph node metastasis of the DTC. Due to the lack of a standard approach to synchronous tumors, it is still very difficult to manage these cases of synchronous tumors. Surgery is the mainstay of treatment for differentiated thyroid cancers, followed by iratherapy to improve outcome by treating residual or persistent disease, while in cases of lymphoma, chemotherapy is the first-line treatment [5].
In our case, given the good prognosis of DTC, we first started chemotherapy for NHL, in line with other authors. However, cervical lymph node dissection could have been avoided, as these nodes would have responded to chemotherapy.
Conclusion
The synchronous presence of DTC and NHL is a rare entity, which may pose a diagnostic and treatment dilemma. To date, there is no standardized approach due to lack of experience, we suggest the "lymphoma-first approach" with synchronized and tailored multidisciplinary efforts.
Patient Perspective
Before admission and in the operating room, the patient was given an explanation of the procedure in order to obtain her consent. Objective abnormalities and risks associated with anesthesia and surgery were explained to her.
Ethics Declarations
Informed Consent
A written informed consent, dated and signed, was obtained from the patient.
Conflict of Interest
The authors declare no conflict of interest.
Ethics Approval Obtained
This study was approved by: Mohammed V university in Rabat; morocco
Authors' Contributions
All authors have contributed to the management of the patient and have read and approved the final version of the manuscript.
Acknowledgements
To all authors who contributed to the realization of this work
References
- Prinzi, N., Sorrenti, S., Baldini, E., De Vito, C., Tuccilli, C., Catania, A., ... & Ulisse, S. (2015). Association of thyroid diseases with primary extra-thyroidal malignancies in women: results of a cross-sectional study of 6,386 patients.PloS one, 10(3), e0122958.
- Acosta-Ortega, J., Montalbán-Romero, S., García-Solano, J., Sánchez-Sánchez, C., & Pérez-Guillermo, M. (2004). Simultaneous medullary carcinoma of the thyroid gland and Hodgkin's lymphoma in bilateral lymph nodes of the neck: A potential pitfall in fine-needle aspiration cytology. Diagnostic Cytopathology, 31(4), 255-258.
- Xie, S., Liu, W., Xiang, Y., Dai, Y., & Ren, J. (2015).Primary thyroid diffuse large B-cell lymphoma coexistent with papillary thyroid carcinoma: A case report. Head & Neck, 37(9), E109-E114.
- Warren, S. (1932). Gates, 0.: Multiple primary malignant tumors. A survey of the literature and a statistical study. Am J Cancer, 16(1358), 414.
- Haugen, B. R., Alexander, E. K., Bible, K. C., Doherty,G. M., Mandel, S. J., Nikiforov, Y. E., ... & Wartofsky, L. (2016). 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid, 26(1), 1-133.
- Shanbhag, S., & Ambinder, R. F. (2018). Hodgkin lymphoma: A review and update on recent progress. CA: a cancer journal for clinicians, 68(2), 116-132.