
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2018) Volume 3, Issue 2
Pain Neuroscience Education to Support Birth: A Feasibility Study
2Michael G. DeGroote School of Medicine, McMaster University, Canada
Received Date: Aug 10, 2018 / Accepted Date: Aug 14, 2018 / Published Date: Aug 30, 2018
Copyright: ©Sinead Dufour. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: This study explored the impact of a novel one-time workshop, aimed to empower women throughout their birth experience through the use of pain neuroscience education concepts.
Methods: A pre-post cohort study design involving a 90-minute workshop with pregnant women in their third trimester. Education related to physiologic birth principles with an emphasis on pain neuroscience education and recent associated best practice guidelines represented the focus of the workshop. In addition to the collection of feasibility data outcomes were measured pre and post workshop as well as within the first 6 weeks post-partum.
Results: A one-time workshop that focused on pain neuroscience education was feasible. All participants used pain modulating strategies based on the workshop content and 92% of participants reported they would recommend the workshop. Further the workshop and had a positive effect on outcomes. Specifically, significant improvements for selfefficacy were found post-workshop.
Conclusion: Pain neuroscience education appears to be feasible to delivered in a one-time workshop format and appears to have the potential improve birth outcomes. Future to be delivered fully powered trials are required to adequately test and confirm these preliminary findings.
Introduction
A physiologic birth constitutes a baby born vaginally following a labour that is not altered by medical interventions [1]. Specifically, this involves spontaneous onset and progression of labour at term, utilizing the woman’s innate hormone physiology [2]. Compared births involving common interventions such as synthetic oxytocin or epidural analgesia, physiologic births provide superior outcomes for both mother and baby [2]. Specifically, enhanced outcomes for the baby include increased breastfeeding rates and infant-maternal attachment, while the mother will also benefit from increased satisfaction as well as reduced labour duration and peripartum morbidity [1,3-5]. Moreover, a physiologic birth is protective for the perineum and pelvic floor [3]. The correlation between instrumental delivery, recumbent birth positions and directed Valsalva pushing strategies with pelvic floor injury is well-established [6-8].
The increasing rates of medical intervention in birth is discordant from current clinical practice guidelines (CPGs) [8-15]. Both the Society of Obstetricians and Gynecologists of Canada (SOGC) and the American College of Obstetricians and Gynecologists (ACOG) recently updated their CPGs surrounding labour management, advocating for practices in concordance with physiologic labour and birth, inclusive of non-pharmacological pain management [13-14]. Notably, the most recent SOGC CPGs highlights the importance of improving the mother understands of the physiology and complexity of neurophysiologic and endocrine resources, inclusive of pain during labour [15]. Specifically, concerning pain neuroscience education (PNE), this most recent CPG is the first to explicitly focus on the important issues of understanding and related to the pain output signals and associated hormone processes that support birth and maternal-infant attachment [15].
Pain science is an overarching team that describes the emerging multifaceted understanding of pain. In birthing practices, labour pain management continues to primarily focus on pharmacological means to diminish the sensory input of pain [19]. However, the neuromatrix theory recognizes pain experience to involve sensory, emotional and cognitive inputs, including aspects from past experiences, stress regulation, sense of safety and immune systems [20]. The current evolved understanding of pain is multi factorial and acknowledges the context dependent nature of the pain output from the brain. Various mechanisms of pain control have been described in the literature and have been utilized through education and training in health care. Three of these have been described in relation to birth processes. First, the Gate Control mechanism works by creating pleasant stimulations in the painful area, such as rubbing a toe after it has been stubbed [15]. Second, the Diffuse Noxious Inhibitory Control (DNIC) works by applying painful stimulations at any site on the body for the duration of each painful stimulus, releasing endogenous morphine to decrease experiences of pain [15]. Finally, the Central Nervous System Control (CNSC) mechanism utilizes the underlying knowledge of the context dependent nature of the produced pain output. Understanding the mindset and the physical and social environment as powerful modulators of context is key to this over arching mechanism [15]. The lack of utilization of PNE in perinatal care represents a clear care gap.
Pregnant women lack awareness regarding physiologic birth strategies and the associated risks of non-physiologic birth methods in part due to inadequate training and experience of related health care providers [2,15]. These findings support the necessity for research specifically devoted to enhancing a woman’s self-efficacy, knowledge and birth outcomes through education and empowerment, inclusive of PNE. Therefore, the objective of this pilot study was to examine the potential effect of a one-time workshop, aimed to empower women throughout their birth experience through specifically incorporating PNE within the context of knowledge translation related to physiologic birth best practices [16-18]. We hypothesized that including PNE within a group prenatal workshop would improve self-efficacy and coping in the birth process as well as improve physiologic birth outcomes. Specifically, we are interested to determine the impact of the intervention on: (1) understanding of pain; (2) understanding of physiologic birth; (3) self-efficacy prior to birth and (4) birth outcomes.
Methods
Study Design
A pre-post cohort study design was conducted. Participant’s baseline understanding of pain neuroscience, physiologic birth knowledge and perceived self-efficacy were assessed using three self-report measures immediately prior to the interactive workshop. All participants were assessed using the same three self-report measures immediately following workshop completion. Participants were then administered one self-report survey by phone or email two to six weeks post birth to track birth outcomes and assess the perceived utility of the workshop. Ethics approval was granted by the Hamilton Integrated Research and Ethics Board.
Participants
Women in the third trimester of pregnancy were invited to attend a one-time 90-minute interactive workshop. Women were recruited primarily through poster dissemination at various perinatal care settings in the Greater Toronto Area Ontario, Canada.
Intervention
A 90-minute interactive workshop was delivered in on two occasions in the Greater Toronto Area Ontario, Canada [21-27]. The objectives of the workshop were to educate and empower participants regarding their upcoming birth through knowledge translation of best evidence and CPGs and related PNE specific to the birth process.
Data collection
Outcome Measures The following self-report measure was administered at baseline and immediately post-workshop.
Pain Neurophysiology Questionnaire (Moseley 2003)
Participant’s understanding of pain science and their conceptualizations of pain were measured using the Moseley’s pain neuroscience questionnaire, which has been validated in chronic pain populations [30]. This questionnaire is made of 19 question items with respective responses of true, false or undecided [31]. Each correct response is given one point and incorrect or undecided responses are given zero points [31]. Participant’s total correct scores were recorded into an Excel spreadsheet as percentages.
Outcome Measure Development
The research team utilized a systematic four-step process, to develop self-report measures to be used pre-workshop, post-workshop and post-birth including a knowledge of physiologic birth questionnaire, self-efficacy questionnaire and a post-birth survey [32]. The first step is described as domain identification, which was accomplished through a systematic review of the literature. The second step, item identification, involved the generation of items from previously established content domains. The third step, instrument formation, consisted of writing components from item identification in a more suitable and practical format. The fourth step involved pilot testing questionnaires in this study cohort. Modifications to the questionnaires were made based on peer review and feedback provided, which included changes to items due to ambiguity and irrelevance, as well as rationalizations for measurement scales utilized.
Knowledge of Physiologic Birth Questionnaire
Participant’s understanding of concepts, processes, mechanisms and benefits of a physiologic birth was assessed using a constructed self-report measure with two multiple choice and seven true or false items. This questionnaire also measured participants’ understanding of common pain modulating strategies during labour and delivery, pain versus suffering distinctions, and available perinatal birth supports. Correct responses were give one point and incorrect responses were given zero points. Likewise, participants’ total correct scores were recorded into an Excel spread sheet as percentages.
Self-Efficacy Questionnaire
In order to measure constructs related to birth self-efficacy, items from the Coping Self-Efficacy Scale (CSES) and Childbirth Self-Efficacy Inventory (CSFI) were combined [33,34]. The CSES is a reliable and valid measure of self-efficacy in various cohorts [33,34]. The CSES has not been validated in pregnant women to date, whereas the CSFI has been validated in multiple perinatal populations [35,36]. However, the CSFI is time intensive because it incorporates 62 items [36]. Therefore, the CSES and CSFI were combined to develop a feasible self-reported measure of self-efficacy, the Self-Efficacy Questionnaire [35,36]. Specifically, in order to combine these measures, thematic analysis was conducted and produced three overlapping constructs with corresponding question items: (1) Use of problem-focused coping related to your upcoming birth (eight items), (2) Stop unpleasant emotions and thoughts related to your upcoming birth (three items), and (3) Get support from friends and family-related to your upcoming birth (two items). Finally, an 11-point Likert scale, adapted from the CSES, was applied, where one point signified “cannot do at all” and 10 points represented “certain can do”.
Pre- and Post-Workshop Packages
The pre and post workshop packages incorporated the three self-report measures outlined above: Pain Neurophysiology Questionnaire, Self-Efficacy Scale and Knowledge of Physiologic Birth Questionnaire. Participant demographic questions pertaining to age, due date, number of previous births, anticipated birth support, attending practitioner, and planned birth environment (home or hospital) were included in pre-workshop packages [30]. Pre- and Post-Workshop Packages were administered immediately before and after the workshop, respectively.
Post-Birth Survey
The Post-Birth Survey was developed to track birth outcomes and assess the utility of the workshop including knowledge of pain and suffering distinctions, implementation of self-efficacy and pain modulating strategies during birth, implementation of medical interventions as well as the participant’s overall experience related to the event of childbirth. This survey was informed by Childbirth Connections, recommendations from the SOGC CPGs and population specific meta-analyses [3,13,15,28,37]. Item responses included a seven point Likert Scale, which has been proven to be more accurate and easier to use compared to alternative ordinal scales [38]. This survey was administered within 6 weeks after the participant’s birth through email or phone.
Feasibility of the Intervention
Feasibility of the intervention relates to the degree to which the participants enroll in, complete, and comply with the intervention. The feasibility of the intervention was monitored through a research log and a post-intervention survey.
The research log determined:
The number of eligible participants who enrolled in the study, the reported reasons for non-participation, and the number of participants lost to follow-up in addition to the reasons for this. The characteristics of participants will also be determined through the research log.
a) The level of fidelity of the protocol (the extent to which the research team adhered to the components of the protocol), based on team meetings and collaborative follow-up through the study period.
b) The baseline characteristics of the participants who completed the intervention through to the follow-up survey and those who withdrew. The survey determined the following:
a) The reported reasons for compliance and non-compliance with the intervention, that is if knowledge learned in the workshop were applied or not.
Data Analysis
Descriptive statistics were calculated for all demographic items. To test for normality of pre- and post-workshop scores, the Shapiro-Wilk W-test was conducted, with a significance value of alpha 0.05. The Shapiro-Wilk W-test was selected as it is the most appropriate normality test for sample sizes less than 50 [37]. Two-tailed, paired sample t-tests were used to calculate mean difference, standard error, and 95% confidence intervals as well as test for statistically significant differences between pre- and post-Moseley Pain Neurophysiology Questionnaire, Knowledge of Physiologic Birth Questionnaire, and Self-Efficacy Questionnaire scores using STATA software (version 14.2). Clinically meaningful change was assessed using differences between means. Descriptive statistics were also calculated for Post-Birth Survey items.
Results
A total of 12 women completed this study, the majorities were nulliparous (67%), anticipated spousal birth support, and listed a midwife as their attending practitioner (Table 1). All pre and post self-report measures are displayed in. Questionnaire scores demonstrated parametric distribution (p > 0.05). Mean difference, standard error, and 95% confidence intervals for all pre- and post-workshop self-report measures. Pain Neurophysiology Questionnaire (Moseley) scores post-workshop did not significantly increase (t=-0.1173, degrees of freedom (DF)= 22, p=0.91), whereas Knowledge of Physiologic Birth Questionnaire scores slightly decreased, but not enough to reach statistical significance (t=0.1750, DF=22, p=0.86). However, Self-Efficacy Questionnaire scores post-workshop significantly increased (t=-2.2695, DF=22, p =0.03).
Table 1: Participant Demographics (n=12)
|
Age |
|
|
Mean (SD) |
34.3 (3.8) |
|
Range |
30 - 42 |
|
Number of Previous Births (%) |
|
|
Nulliparus |
8 (67) |
|
Multiparus |
4 (33) |
|
Due Date |
|
|
Range |
April 03, 2018- June 04,2018 |
|
Anticipated Birth Support (%) |
|
|
Spouse |
12 (100) |
|
Doula |
3 (25) |
|
Family |
4 (33) |
|
Friend |
1 (8) |
|
Attending Practitioner (%) |
|
|
Midwife |
10 (83) |
|
OB-GYN |
1 (9) |
|
Family Practitioner |
1 (9) |
|
Midwifery Delivery Setting (%) |
|
|
Home |
7 (58) |
|
Hospital |
3 (25) |
SD= standard deviation; OB-GYN = obstetrician- gynecologist
Table 2: Pre-Post Workshop Results (n=12)
|
|
Mean (SD) |
Range |
Mean Difference (SE) |
95% CI |
|
Pain Neurophysiology Questionnaire |
||||
|
Pre Workshop |
73.68 (8.64) |
63.16-89.47 |
-0.44 (3.74) |
(-8.19,7.31) |
|
Post Workshop |
78.51 (9.64) |
68.42-94.73 |
|
|
|
Knowledge of Physiologic Birth Questionnaire |
||||
|
Pre Workshop |
84.26 (15.32) |
55.55-100 |
0.93 (5.29) |
(-10.04,11.90) |
|
Post Workshop |
83.33 (10.05) |
66.66-100 |
|
|
|
Self-Efficacy Questionnaire |
||||
|
Pre Workshop |
7.29 (1.14) |
5.54-9.38 |
-0.89 (0.39) |
(-1.71,-0.08) |
|
Post Workshop |
8.19 (0.74) |
6.85- 9.69 |
|
|
SD= standard deviation; SE= standard error; CI = confidence interval
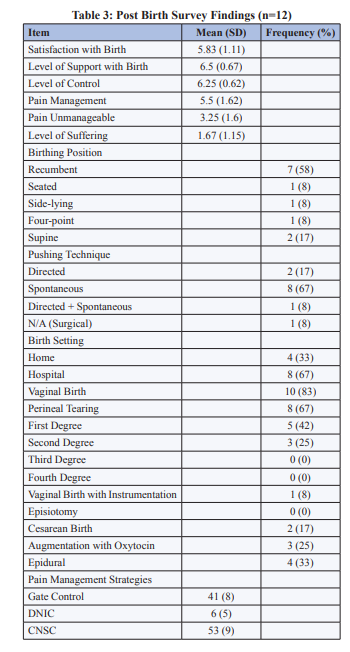
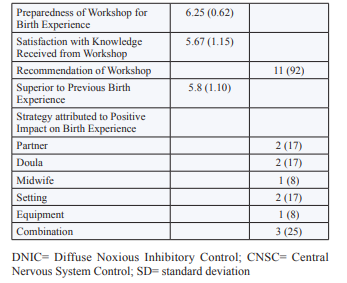
Post-Birth Survey descriptive statistics are summarized in Table 3. Participants felt they were in control of the birth (mean= 6.25, SD= 0.62), had adequate levels of support (mean= 6.5, SD= 0.67) and experienced minimal suffering (mean= 1.67, SD= 1.15). Most participants had a vaginal birth (83%) and were free to move during labour (83%). Recumbent birth positioning was the most common position reported (58%) as was the use of spontaneous pushing (67%). Eleven participants said they would recommend the workshop to other expecting mothers and their partners. All participants used at least one non-pharmacological pain-management strategy introduced in the workshop during their birth (Table 3). Specifically, participants on average used 10 (SD= 2.68) non-pharmacological pain management strategies during birth, the majority classified as CNSC (53%), followed by GCT (42%), and DNIC (5%). Generally, participants emphasized the role of their partner, doula, and/or midwife having the greatest positive impact on their birth experience.
Discussion
To the authors’ knowledge, this is the first study exploring the impact of a one-time workshop focused on PNE. In accordance to the SOGC CPGs, there are many benefits of physiologic labour and birth for both mother and baby, involving a significant increase in oxytocin, beta-endorphins, prolactin and other catecholamines. These hormones are essential in supporting labour and birth processes, such as high-intensity uterine contractions, pain modulating mechanisms as well as lactation and fetal development [13,15,38-41]. Therefore, disruption of these hormonal systems through common maternity care practices, can understandably increase the risk of complications and newborn morbidities such as less-frequent involuntary contractions [43,44].
Although we observe no significant change in participant knowledge of pain neuroscience and physiologic birth processes post-workshop, there was a statistically significant improvement in birth self-efficacy. However, the magnitude of improvement of self-efficacy was not clinically significant, as inferred from “rule-of-thumb” calculations of 30-36% change when no cut-off values exist in the literature [45]. These results could be due to a ceiling effect, as participants demonstrated high levels of baseline knowledge of pain neuroscience, physiologic birth processes and self-efficacy. Additionally, the small sample size also increases the chance of Type 2 error, limiting the chance of correctly identifying significant change [46].
Our results indicate that participants had positive birth experiences following participation in the workshop studied. Specifically, participants were able to cope with the experiences of birth, as reflected by high levels of reported control, ability to manage pain as well as minimal experiences of suffering and unmanageable pain during the birth process. This finding is corroborates the recommendations set out by the SOGC, which emphasize the utilization of any pain management mechanism to facilitate freedom of movement, improve self-efficacy and limit suffering during childbirth [13,15].
Additionally, the majority of participants experienced a physiologic birth. Our participants’ birth outcomes were notably different than the Ontario (Canada) average when compared with normative data from the Better Outcomes Registry and Network (BORN) database (2016-2017). According to BORN the frequency of vaginal births in Ontario is 71.6%, the frequency of epidurals is 73.8% and the frequency of instrumental vaginal births is 12.4%. In contrast among our participants the frequency of vaginal birth was 83%, the frewence of epidurals was only 33% and the frequency of instrumental vaginal births was 8%. The design of this study does not allow for us to conclude that the birth outcomes noted were a result of the workshop intervention used. However, our results congruent with those of a 2014 meta-analysis comparing birth outcomes when non-pharmacological strategies were used, compared with “usual care” [3]. Given the ratings of control and manageability pain throughout their birth, this pilot study does appear to supports PNE as an antenatal education strategy that warrants further study.
Suffering and pain represent two distinct constructs that are not mutually exclusive. Pharmacological interventions act to minimize sensation and pain, these interventions do not address the experience of suffering, or the distressing psychological state that may or may not be associated with pain (i.e. helplessness, anguish, fear, panic, or loss of control) [15, 28]. During the various stages of the birth process, a diverse set of needs must be met in order to prevent suffering, often including non-pharmacological approaches, such as: knowledge about pain and coping strategies, continuous labour support that is confident and caring, as well as a peaceful and safe environment [15]. As compared to use of epidurals, non-pharmacological approaches further benefit birth experiences and outcomes by decreasing pain intensity as well as the likelihood of invasive procedures (e.g. Cesarean-sections) and labour complications (e.g. fetal distress and severe vaginal tearing) [15,23-26]. Despite extensive research in support of non-pharmacological approaches, epidurals and other medical interventions are still widely used in current practice [29]. Our findings support the feseaility and potential effect of PNE.
Currently, there remains a disconnect between common birth practices and CPGs [2,13]. This pilot study highlights the potential role PNE and mobilizing physiologic birth evidence and associated recommended best practices to bridge this gap
Limitations
Although we were able to follow up with 100% of participants that enrolled in our study, a limitation of this pilot study was the small sample size [47]. Consequently, an acceptable level of power was not determined, reducing the probability of detecting significant differences between pre-post workshop outcomes. Second, in absence of a control group, inferences of workshop effectiveness could only be compared to normative data through BORN.
Conclusion
Pain neuroscience education and awareness of associated best practice guidelines that support physiologic birth practices have the potential to improve birth outcomes. Future fully powered trials are required to adequately test and confirm and extend these preliminary findings.
References
- ACNM, MANA, & NACPM (2013) Supporting Healthy and Normal Physiologic Childbirth: A Consensus Statement by ACNM, MANA, and NACPM. J Perinat Educ 22: 14-18.
- Mayberry LJ, Avery MD, Budin W, Shannon Perry (2017) Improving maternal and infant outcomes by promoting normal physiologic birth on hospital birthing units. Nurs Outlook 65: 240-241.
- Chaillet N, Beliad L, Crochetiere C, Roy L, Gagné GP, et al. (2014) Non pharmacologic approaches for pain management during labor compared with usual care: a meta-analysis. Birth 41: 122-137.
- Dozier AM, Howard CR, Brownell EA, Wissler RN, Glantz JC, et al. (2013) Labor epidural anesthesia, obstetric factors and breastfeeding cessation. Maternal Child Health J 17: 689-698.
- Hodnett ED (2002) Pain and women’s satisfaction with the experience of childbirth: a systematic review. Am J Obstet Gynecol 186: S160-172.
- Khooshide M, Mirzarahimi T, Akbari GA (2015) The Impact of Physiologic and Non-Physiologic Delivery on the Mother and Neonate Outcomes; A Comparative Study on the Primi Gravid Mothers. J Family Reprod Health 9: 13-18.
- Liebling RE, Swingler R, Patel RR, Verity L, Soothill PW, et al. (2004) Pelvic floor morbidity up to one year after difficult instrumental delivery and cesarean section in the second stage of labor: A cohort study. Am J Obstet Gynecol 191: 4-10.
- Gizzo S, Di Gangi S, Noventa M, Veronica Bacile, Alessandra Zambon, et al. (2014) Women’s Choice of Positions during Labour: Return to the Past or a Modern Way to Give Birth? A Cohort Study in Italy. BioMed Research International.
- Kainu JP, Sarvela J, Tiippana E, Halmesmäki E, Korttila KT (2010) Persistent pain after caesarean section and vaginal birth: a cohort study. Int J Obstet Anesth 19: 4-9.
- Torvaldsen S, Roberts CL, Simpson JM, Jane F Thompson, David A Ellwood (2006) Intrapartum epidural analgesia and breastfeeding: a prospective cohort study. Int Breastfeed J 1: 24.
- Harris SJ, Janssen PA, Saxell L, Carty EA, MacRae GS (2012) Effect of a collaborative interdisciplinary maternity care program on perinatal outcomes. CMAJ 184: 1885-1892.
- Chalmers B, Kaczorowski J, O’Brien B, Royle C (2012) Rates of Intervention in Labor and Birth across Canada: Findings of the Canadian Maternity Experiences Study. Birth IssPerinat C 39: 203-210.
- The Society of Obstetricians and Gynaecologists of Canada (SOCG) (2016) No.336- Management of Spontaneous Labour at Term in Health Women – SOGC Clinical Practice Guideline. Journal of Obstetrics and Gynecology Canada 38: 843-865.
- The Society of Obstetricians and Gynaecologists of Canada (SOGC) (2018) No. 355-Physiologic Basis of Pain in Labour and Delivery: An Evidence-Based Approach to its Management. J ObstetGynaecol Can 40: 227-245.
- American College of Obstetricians and Gynecologists (ACOG) (2017) Approaches to limit intervention during labor and birth. Committee Opinion No. 687. ObstetGynecol 129: e20-28.
- Escott D, Slade P, Spiby H (2009) Preparation for pain management during childbirth: The psychological aspects of coping strategy development in antenatal education. Clin Psychol Rev 29: 617-622.
- Mehdizadeh A, Roosta F, Chaichian S, Alaghehbandan R (2005) Evaluation of the impact of birth preparation courses on the health of1 the mother and newborn. Am J Perinatol 22: 7-9.
- Ip WY, Tang C, Goggins W (2009) An educational intervention to improve women’s ability to cope with childbirth. J ClinNurs 18: 2125-2135.
- Whitburn LY, Jones LE, Davey MA, Susan McDonald (2018) The nature of labour pain: An updated review of the literature. Women Birth. 2018. [PDF]
- Trout K (2010) The Neuromatrix Theory of Pain Implications for Selected Non pharmacological Methods of Pain Relief for Labor. J Midwifery Women’s Health 49: 482-88.
- Louw A, Diener I, Landers MR, Puentedura EJ (2014) Preoperative pain neuroscience education for lumbar radiculopathy: a multicentre randomized controlled trial with 1-year follow-up. Spine 39: 1449-1457.
- Semmons J (2016) The role of physiotherapy in the management of chronic pain. AnaesthIntens Care 17: 445-447.
- Heberlein EC, Picklesimer AH, Billings DL, Covington-Kolb S, Farber N, et al. (2016) Qualitative comparison of women’s perspectives on the functions and benefits of group and individual prenatal care. J Midwifery Women’s Health 61: 224-234.
- Johnston RG, Brown AE (2013) Maternal trait personality and childbirth: the role of extraversion and neuroticism. Midwifery 29: 1244-1250.
- Ruiz RJ, Gennaro S, O’Connor C, Nathan Marti, Amanda Lulloff, et al. (2015) Measuring coping in pregnant minority women. West J Nurs Res 37: 257-275.
- Rini CK, Dunkel-Schetter C, Wadhwa PD, Sandman CA (1999) Psychological adaptation and birth outcomes: the role of personal resources, stress, and socio cultural context in pregnancy. Health Psychol 18: 333.
- Smith CA, Levett KM, Collins CT, Armour M, Dahlen HG, et al. (2011) Relaxation techniques for pain management in labour. The Cochrane Library.
- Simkin P (2007) Comfort in Labor: How You Can Help Yourself to a Normal Satisfying Childbirth.
- Better Outcomes Registry and Network (BORN) Ontario. Years provided: 2016-2017. Resource Type: Extract data. Data Provided May 2017.
- Moseley GL (2003) Unravelling the barriers to reconceptualisation of the problem in chronic pain: the actual and perceived ability of patients and health professionals to understand the neurophysiology. J Pain 4: 184-189.
- Adillion A, Lozano E, Salvat I (2015) Comparison of pain neurophysiology knowledge among health sciences students: a cross-sectional study. BMC Res Notes 8: 592.
- Bernhardsson S, Larsson M (2013) Measuring Evidence-Based Practice in Physical Therapy: Translation, Adaptation, Further Development, Validation, and Reliability Test of a Questionnaire. PhysTher 93: 819-832
- Chesney MA, Neilands TB, Chambers DB, Jonelle M. Taylor, Susan Folkman A (2006) validity and reliability study of the coping self-efficacy scale. Br J Health Psychol. 11: 421-437.
- Lowe NK (1993) Maternal confidence for labor: Development of the childbirth self-efficacy inventory. Res Nurs& Health 16:141-149.
- Drummond J, Rickwood D (1997) Childbirth confidence: validating the childbirth self-efficacy inventory (CBSEI) in an Australian sample. J of AdvNurs 26: 613-622.
- Sinclair M, O’Boyle C (1999) The Childbirth Self-Efficacy Inventory: A replication study. J of AdvNurs 30: 1416-1423.
- D’agostino RB, Belanger A, D’Agostino Jr RB (1990) A suggestion for using powerful and informative tests of normality. Am. Stat 44: 316-321.
- Finstad K (2010) Response interpolation and scale sensitivity: evidence against 5-point scales. J Usability Stud 5: 104-110.
- Nathanielsz, PW (1998) Comparative studies on the initiation of labor. Eur J ObstetGynecolReprod Biol 78: 127-132.
- Terzidou V, Blanks AM, Kim SH, Steven Thornton, Phillip R (2011) Bennett Labor and inflammation increase the expression of oxytocin receptor in human amnion. BiolReprod. 84: 546-552.
- Yang J, Liang JY, Li P, Pan YJ, Qiu PY, et al. (2011) Oxytocin in the periaqueductal gray participates in pain modulation in the rat by influencing endogenous opiate peptides. Peptides 32: 1255-1261.
- Voogt JL, Lee Y, Yang S, Arbogast L (2001) Regulation of prolactin secretion during pregnancy and lactation. Prog Brain Res 133: 173-185.
- Anim-Somuah M, Smyth RM, Jones L (2011) Epidural versus non-epidural or no analgesia in labour. Cochrane Database Syst Rev (12) CD000331.
- Buckley, Sarah J (2015) Hormonal Physiology of Childbearing: Evidence and Implications for Women, Babies, and Maternity Care. Washington, D.C.: Childbirth Connection Programs, National Partnership for Women & Families.
- Riddle DL, Stratford PW (2013) Is this change real? interpreting patient outcomes in physical therapy. Philadelphia, PA: F.A. Davis Company; 99 p.
- Riddle DL, Stratford PW (2013) Is this change real? Interpreting patient outcomes in physical therapy. Philadelphia, PA: F.A. Davis Company; 47 p.
- Halpern S (2008) SOGC Joint Policy Statement on Normal Childbirth. J ObstetGynaecol Can 30: 1163-1165.