
Archives of Case Reports: Open Access(ACROA)
ISSN: 3065-7598 | DOI: 10.33140/ACROA


Research Article - (2024) Volume 1, Issue 1
Odontogenic Keratocyst Management Using Carnoy’s Solution: Our Experience
2Associate Professor, Department of Dentistry, India
3Department of ENT Senior Resident, India
4Department of ENT Senior Resident, India
5Department of Dentistry, India
Received Date: Feb 28, 2024 / Accepted Date: May 26, 2024 / Published Date: Apr 26, 2024
Copyright: ©Â©2024 Nilam U Sathe, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Sathe, N. U., Bhange, P., Rathod, I., Gupta, D., Kelkar, S. (2024). Odontogenic Keratocyst Management Using Carnoy
Abstract
Background Odontogenic keratocyst (OKC) is a benign intraosseous lesion relatively frequent in the oral cavity. It has a locally aggressive behaviour and exhibits a high propensity to recur after treatment.
Aim The present study aimed to study the demographic profile of the OKC and to investigate the clinicoradiographic presentations and outcomes of surgical treatment of OKC. Materials and methods: It is the descriptive Prospective Study done during the time period of January 2020 to December 2023, 18 cases of odontogenic keratocyst were admitted and treated under the care of Department of Otorhinolaryngology, Seth GSMC and KEM Hospital Mumbai. Patients came to the ENT OPD with history of swelling in the cheek region, nasal obstruction, numbness in the upper alveolar region. Enucleation with bone grafting & application of Carnoy’s solution (CS) was the most common surgical modality that was used in all patients.
Result Mean age of presentation was 34.39 years. Female predilection was more 61% compare to male 39%. most common presentation of the cases was third molar problem followed by pain. Mandibular odontogenic cyst is more common 13 cases (72%) than maxillary odontogenic cyst 5 cases (28%). No recurrence seen in this study. Conclusion-OKC is aggressive tumour for this timely intervention, complete enucleation and proper follow up require. Carnoys solution is the key for reducing recurrence of OKC.
Conclusion Odontogenic keratocyst is locally aggressive tumour. sometimes it occurs as incidental findings. Odontogenic keratocyst also associated with syndrome. For this timely intervention of swelling complete enucleation with proper follow up is required. Carnoy’s solution is the key for resolution of OKC & to prevent recurrence.
Keywords
Odontogenic Cysts, Keratocyst, Tumours of Mandible and Maxilla.
Introduction
The odontogenic keratocyst (OKC)-recently redefined as keratocystic odontogenic tumour (KCOT)-continues to be an interesting and challenging pathological entity for both clinicians and researchers. Phillipson (1956) described the lesion as a thin-walled cyst characterised by a cyst lining featuring keratinised epithelium. The lesion has gained much attention because of its potentially aggressive behaviour, significant recurrence rates following treatment, and its association with Basal Cell Naevus Syndrome. Pindborg and Hansen (1963) defined seven essential histopathological features of OKC [1]. These are summarised in Table 1.
|
Histological features of odontogenic keratocysts |
|
|
Sr. No |
Feature |
|
1 |
The lining epithelium is usually very thin and uniform in thickness, with little or no evidence of rete ridges. |
|
2 |
There is a well-defined basal layer, the component cells of which are cuboi-dal or columnar in shape and often in a palisaded arrangement |
|
3 |
There is a thin spinous cell layer that often shows a direct transition from the basal cell layer |
|
4 |
The cells of the spinous cell layer frequently exhibit intracellular oedema. |
|
5 |
Keratinisation is predominately parakeratotic, but it may be orthokeratotic* |
|
6 |
The keratin layer is often corrugated. |
|
7 |
The fibrous cyst wall is generally thin and usually uninflamed |
|
Note |
*ln the latest WHO classification (2005), only parakeratinisation is listed under Keratocystie odontogenic tumour. |
Table 1: Showing Histological Features of OKC
Odontogenic keratocytes (OKCs) are cystic lesions appearing in the jaws, classified as developmental cysts arising from the dental lamina [2]. They are more common in the mandible, with a predilection for the angle and ramus. This lesion may occur in association with an impacted third molar. Compared to other odontogenic cysts, OKC has an infiltrating growth pattern and aggressive biological behaviour. Moreover, the fact that OKC arises from the inactivation of the chromosome 9q patched gene (PTCH), a tumour suppressor gene. Odontogenic cysts are epithelial-lined pathological cavities that are encircled by fibrous connective tissue and arise from odontogenic tissues that are present in the maxilla and mandible’s tooth-bearing areas. Jaw cysts destroy the bone and may result in the resorption or displacement of neighbouring teeth [3]. The treatment modalities are divided into conservative and radical methods. The conservative methods include strict enucleation with or without surgical scraping or cleaning utilizing a curette or marsupialization decompression, with or without secondary therapeutic measures.
The aggressive techniques include peripheral ostectomy (PO), chemical curettage with Carnoy’s solution (CS), cryotherapy, electrocautery, and resection (en bloc or marginal). OKC are generally single, although they can present with multiple lesions, and are usually linked with nevoid basal cell carcinoma syndrome, which is a hereditary condition characterized by multiple basal cell skin cancers; other common signs include pits on the palms of the hands or soles of the feet, calcium deposits in the brain, developmental disability, and skeletal (bone) changes. Associated with Gorlin Goltz syndrome [4]. The delicate and fragile nature of its epithelial lining, weakly connected to the capsular connective tissue, makes these lesions prone to tearing, separating, and breaking during surgical excision, sparing some epithelial remains, which can lead to recurrence since they have high proliferative activity. Recurrence may also be due to the persistence of satellite cysts that would remain during surgery, the presence of cystic debris in the adjacent bone or mucosa, or the existence of epithelial islands in the lining of mucosa [5].
The maxillary sinus is a frequent site for pathologies of odontogenic origin due to its close anatomical relationship with teeth and periodontal tissues, inflammatory disease as well as neoplastic and tumorous lesions can occur in this area. Maxillary sinus involvement must be carefully assessed because orbital damage and the spreading of associated infections could lead to local and systemic compromise to the patient, present with pain, swelling and paraesthesia of lower lip or teeth. Displacement of tooth and destruction of the floor of the orbit, proptosis of eyeball when it involves maxilla are the most common features. Maxillary cysts cause buccal expansion but palatal expansion is rare [6].
Material and Method
It is descriptive Prospective Study done during the time period of January 2020 to December 2023, 18 cases of odontogenic keratocyst were admitted and treated under the care of Department of Otorhinolaryngology. Patient underwent thorough history taking and complete ear, nose and throat examination.
Aim and Objectives
1. To study demographic profile of odontogenic keratocyst.
2. To study clinicopathological aspects and management of odontogenic keratocysts (OKC).
Diagnostic nasal endoscopy, X-ray (Figure 1), CT scan of nose and paranasal sinuses and Cone beam CT scan of involved area (maxilla or mandible) done to confirm extend of the lesion and bony landmarks (Figure 2). After that patient sent for aspiration biopsy or incisional biopsy if required done in extensive lesions. After routine blood investigation and anaesthetic fitness patient posted for complete enucleation. Surgical excision done under general anaesthesia. Local infiltration given with the lignocaine with 2% adrenaline1:2lac concentration. Incision given with 15 no. blade (Figure 3) Mucoperiosteum flap elevated till good exposure of cystic swelling (Figure 4). Bony window is made with number 8 SS white carbide burr. Cystic swelling removed (Figure 5). Cystic lining removed in toto. Betadine wash given in cavity. Sharp margin of the cavity smoothened with round burr.
Carnoy’s solution applied to exposed bone surface to avoid the recurrence (Figure 6) Betadine wash given once again. Bone graft of demineralised bone granules (Figure 7) or synthetic bone graft kept for obliteration of cavity. Chorionic membrane placed over graft and mucoperiosteal flap sutured with 3-0 Vicryl (Figure 8). Excised specimen sent for histopathological examination. Follow up of the patient done weekly for 1 month, twice in month up to 6 months.
HPE shows H&E-stained soft tissue sections show Para keratinized squamous epithelium of uniform thickness with basal cell palisading and surface corrugation. The underlying connective tissue wall shows loose collagenous stroma with chronic inflammatory cell infiltration, cholesterol clefts and areas of haemorrhage (Figure 9).

Figure 1: Digital Xray Showing Mandibular OKC
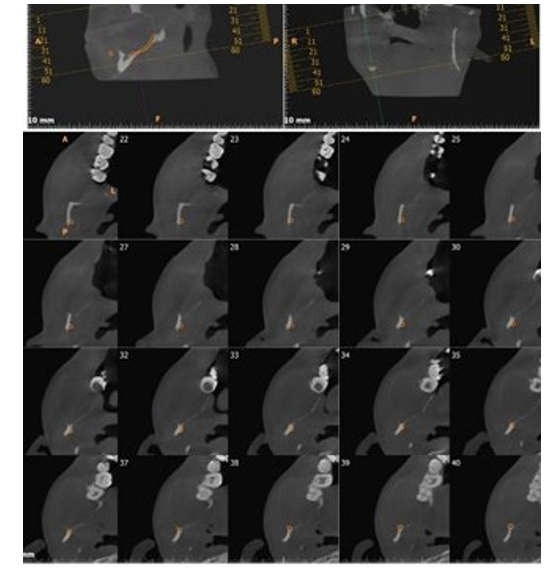
Figure 2: Cone Beam Ct Scan Showing Bilateral Mandibular OKC


Figure 3: Showing Mandibular OKC Figure 4: Showing OKC of Ramus of Mandible
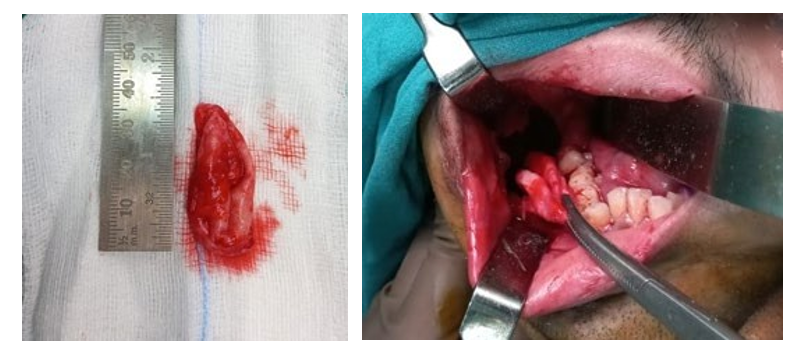
Figure 5: Showing in Toto Excision of OKC
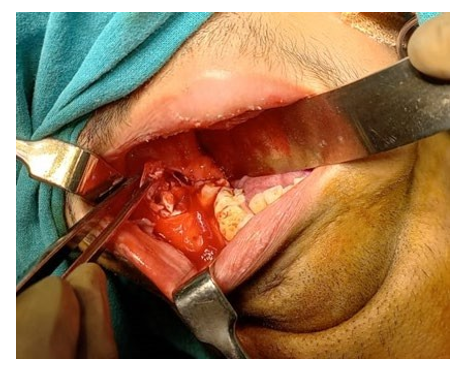
Figure 6: Showing Carnoy’s Solution Application


Figure 7: Showing Obliteration of Okc Cavity with Bone Granules Figure 8: Showing Chorionic Membrane Placed Over Graftand Mucoperiosteal Flap Sutured
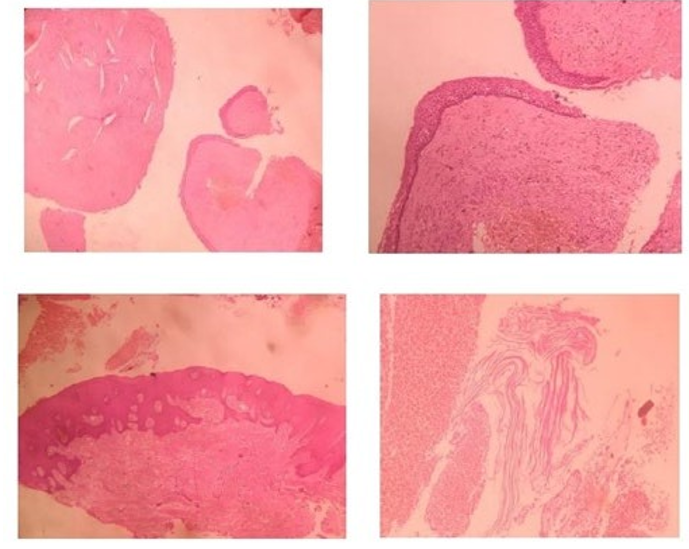
Figure 9: Histopathology Showing OKC
Results
In our study, out of 18 cases of OKC operated of which minimum age of the operated case was 18 year and maximum age of patient was 59 years. Maximum number of cases were of third decade 5 cases (28%) followed by fourth decade 4 cases (22%). Mean age of the patient was 34.39 years (Table 2). This study Shows slight female predilection of the disease as 11 cases were female (61%) and 7 cases were male (39%).
|
Age wise distribution of cases of OKC (n=18) |
||
|
Age group (yrs.) |
No. of cases |
Percentage |
|
1-10 |
0 |
0% |
|
11-20 |
3 |
14% |
|
21-30 |
5 |
28% |
|
31-40 |
4 |
22% |
|
41-50 |
3 |
17% |
|
51-60 |
3 |
17% |
|
Total |
18 |
100 |
|
Mean age 34.39 yr |
||
Table 2: Showing Age Distribution of OKC Cases
One patient diagnosed with Gorlin Goltz syndrome. Patient presented with most commonly with third molar problem were 6 cases. (i.e.,33%) followed by pain and swelling in 5 (28%) and 4 (22%) cases respectively (Table 3).
|
Symptomatologic distribution of cases of OKC |
|
|
Symptoms |
Percentage % |
|
Pain |
28% |
|
Swelling |
22% |
|
Discharge |
11% |
|
Third molar problem |
33% |
|
Sinus problem |
6% |
Table 3: Showing Symptomatological Distribution of OKC Cases
In our study most common site of for odontogenic cyst was mandible in 13 cases (72%) compared to maxilla in 5 cases (28%). Among the mandible most common site was posterior part of mandible including ramus in 9 cases (69%) followed by body of mandible in 3 cases (23%). Most common site affected was right side of mandible in 50% cases. Only one case (6%) with bilateral maxillary odontogenic cyst operated (Table 4). During surgical excision Carnoys solution used. Carnoy's solution is a substance used as a complementary treatment after the conservative excision of odontogenic keratocyst. The application of Carnoy's solution promotes a superficial chemical necrosis and is intended to reduce recurrence rates. However, the inferior alveolar vascular–nervous plexus can occasionally be exposed after the removal of a lesion. The safety of the application of Carnoy's solution over this plexus has been reported, but to date, no clinical report has been made. Carnoys solution, composed of 3 ml of chloroform, 6 ml of absolute ethanol, 1 ml of glacial acetic acid, and 1 g of ferric chloride, is often used as a complementary treatment of lesions with high recurrence rates, such as the keratocystic odontogenic tumour (KOT). In our study there is no any records of recurrence of the cases.
|
Distribution of cases of OKC cases by location |
||
|
Symptoms |
no. of cases |
Percentage |
|
Posterior Mandible |
9 |
50% |
|
Body of mandible |
3 |
17% |
|
Anterior maxillary |
2 |
11% |
|
Posterior maxillary |
3 |
17% |
|
Anterior mandible |
1 |
6% |
Table 4: Showing Distribution of Location of OKC Cases
Discussion
OKC is a benign cystic lesion of the tooth; it is usually asymptomatic and slow-growing. The widespread consensus is that these lesions, like the primordial cyst, develop from left over dental lamina [5].
The age at diagnosis and sex distributions of patients with OKC was (18-59) years, as in other studies shown by Ala et al and Myoung et al [2, 7]. Most OKCs reported they can appear at any age but more frequently in the third decade of life, as reported by Rojas et al [8]. In the present study, OKC was found to occur in patients of a wide age range, with a mean age of 34.39 years. By comparing the results, the most common age is the third decade. Which is similar with our study. In the study by Kammer et al. the results showed that the majority of patients were male (56.73%) [9]. Most OKCs report show a preference for males at a 1: 1.4 ratio, as shown in the study by Tarakaji et al [10]. Study clearly showed a preponderance of males over females at a ratio of 1.56:1 [1]. Findings of other studies of various populations Browne, 1971; Meningaudet al, 2006, suggesting that the male predominance is a universal phenomenon [11, 12].
In present study there is predilection for female 61% compared to male 39%. This might be due to the geographical area or small sample size these. There may be an association with third molar tooth eruption, which is supported by the peak incidence in the second and third decades and also the significant number of presenting complaints being related to third molar teeth. Such problems commonly manifest as pain; including those with those presenting with pain and swelling symptoms, means that the predominant presentation for OKC in the current study would be third molar problem, pain and swelling, in concordance with the findings of Chirapathomaskul et al (2006) [1, 13]. Clinical appearance varies greatly and is frequently characterized.
By soft tissue swelling without any discomfort, lesions can cause tooth displacement, aggressive growth through bone resorption, facial deformities, and spread into nearby structures in the literature review of a previous study of 256 patients by Myoung et al [14]. 118 (46.1%) â· experienced swelling at the time of the initial admission, 51(19.9%) reported pain, and 42 (16.4%) had both swelling and discomfort. Borghesi, et al. [15]. Reported that there were 17 patients (6.6%) with purulent discharge, 12 patients (4.7%) with discomfort, and 2 patients (2.1%) with paraesthesia (0.8%). Fourteen individuals (5.5%) had no symptoms [16]. Study reported that the most common clinical manifestations were bony swelling (54.9%), followed by pain (28.6%), tooth mobility (7.7%), expansion of the cortical plate (6.6%), and paraesthesia (2.2%) [2]. Both studies showed that the most common clinical manifestations were bony swelling followed by pain. So similar to the previously mentioned literature, our study also had a similar finding from the known fact that the OKC grows within the medullary spaces with pain and bony swelling in 5 cases (28%) and 4 cases (22%) respectively. Previous studies have reported that keratocysts occur more frequently in the mandible than the maxilla, with estimates ranging from 65% to 83% of lesions occurring in the former (Browne, 1970; Brannon, 1976) in present study also mandibular odontogenic cyst cases 72%are more common than maxillary odontogenic cyst cases 28% [17, 18]. which is similar with the above studies. Radiographically, odontogenic keratocysts (OKCs) present as a well-defined radiolucent lesion that is either unilocular or multilocular, with smooth and usually corticated margins, unless they have been secondarily infected (see the images below) [13]. In 25-40% of cases, there is an unerupted tooth involved with the lesion ¹³ adjacent teeth may be displaced, but root resorption is rarely seen. Maxillary lesions tend to be smaller than mandibular lesions; however, more extensive involvement can be appreciated in the maxilla because of the cancellous nature of the bone. Larger lesions can cause bony expansion with or without perforation of the cortical plates [13]. This is also similar with our Cone beam CT findings. There are cases presented with recurrence in study showed by Dias et al [16]. that recurrence rates have been estimated to be between 3% and 60%. In our study there is no any cases presented with recurrence.
This might be due to as we used Carnoys solution and also might be follow up duration is small. Various surgical options have been considered, including enucleation alone or associated with the adjunctive measures (Ostectomy, Carnoy’s solution, cryotherapy), marsupialization and decompression, marginal or segmental resection [19]. The effects of various adjunctive therapy on the peripheral lining and their ability to chemically cauterize it have been studied. After being applied for 3 min to reduce side effects, Carnoy’s solution, which contains 1 g of ferric chloride (FeCl3) mixed in 6 ml of alcohol, 3 ml of chloroform, and 1 ml of glacial acetic acid, has been used extensively as an adjuvant treatment with a recurrence rate of about 11%. However, the US Food and Drug. Administration has forbidden its use since 2013 after outlawing chloroform, which was found to be carcinogenic. Therefore, modified Carnoy’s solution (MCS) was developed with a 5-fluorouracil (5FU) was made available for topical usage due to its antimetabolic impact, which results in cell apoptosis.
Most KCOTs were treated with surgical enucleation, which is the traditional technique (to remove the lesion whole from within the bone) with Carnoy’s solution, as shown by Dias et al [14]. This result ties well with our study; All KCOTs were treated with surgical enucleation with, Carnoy’s solution of all surgical procedures, followed by curettage enucleation with bone skimming, cavity obliteration with bone graft demineralised bone granules followed by chorionic membrane placement over bone graft. Which may be key role for reducing recurrence [16].
Conclusion
• Odontogenic keratocyst is locally aggressive tumour. sometimes it occurs as incidental findings.
• Odontogenic keratocyst also associated with syndrome. For this timely intervention of swelling complete enucleation with proper follow up is required.
• Carnoy’s solution is the key for resolution of OKC & to prevent recurrence.
Conflict of Interest: There is no conflict of interest.
References
- Rakesh. (2011). A case series of odontogenic keratocysts from a New Zealand population over a 20-year period. New Zealand Dental Journal, 107(4), 112-116.
- Mohamed, A. A., Babiker, A. A., Khalfallah, M. S., & Eltohami, Y. I. (2023). Odontogenic Keratocysts: Presentation and Surgical Outcome in a Sample of Sudanese Patients. International Journal of Dentistry, 2023.
- Santosh, A. B. R. (2020). Odontogenic cysts. Dental clinics, 64(1), 105-119.
- Rathod, I. (2024). Keratocyst In Gorlin-Goltz Syndrome-A Case Report. British Journal of Medical and Health Research.
- Borrás-Ferreres, J., Sánchez-Torres, A., Alberdi-Navarro, J., Aguirre-Urizar, J. M., & Mosqueda-Taylor, A., et al. (2020). Therapeutic management of the odontogenic keratocyst. An energetic approach with a conservative perspective and review of the current therapeutic options. Journal of Clinical and Experimental Dentistry, 12(8), e794-e799.
- Priya, K. (2014). Odontogenic keratocyst: a case series of five patients. Indian Journal of Otolaryngology and Head & Neck Surgery, 66, 17-21.
- Myoung, H., Hong, S. P., Hong, S. D., Lee, J. I., & Lim,C. Y., et al. (2001). Odontogenic keratocyst: review of 256 cases for recurrence and clinicopathologic parameters. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 91(3), 328-333.
- Velazque Rojas, L., Alonso Claudio, C., Valenzuela Huamán, C. J., & Velazque Rojas, G. (2022). Diagnóstico y tratamiento conservador del queratoquiste odontogénico. Odontoestomatología, 24(39).
- Kammer, P. V., Mello, F. W., & Rivero, E. R. C. (2020).Comparative analysis between developmental andinflammatoryodontogenic cysts: retrospective study andliterature review. Oral and maxillofacial surgery, 24, 73-84.
- Tarakji, B., Baroudi, K., Hanouneh, S., Azzeghaiby, S. N., & Nassani, M. Z. (2013). Possible recurrence of keratocyst in nevoid basal cell carcinoma syndrome: A review of literature. European journal of dentistry, 7(S 01), S126-S134.
- Browne, R. M. (1971). The odontogenic keratocyst. Clinical aspects. British Dental Journal, 128, 225-231.
- Meningaud, J. P., Oprean, N., Pitak-Arnnop, P., & Bertrand,J. C. (2006). Odontogenic cysts: a clinical study of 695 cases. Journal of oral science, 48(2), 59-62.
- Chirapathomsakul, D., Sastravaha, P., & Jansisyanont, P. (2006). A review of odontogenic keratocysts and the behavior of recurrences. Oral surgery, oral medicine, oral pathology, oral radiology, and endodontology, 101(1), 5-9.
- Winters, R., Garip, M., Meeus, J., Coropciuc, R., & Politis,C. (2023). Safety and efficacy of adjunctive therapy in the treatment of OKC (odontogenic keratocyst): a systematic review. British Journal of Oral and Maxillofacial Surgery, 61(5), 331-336.
- Borghesi, A., Nardi, C., Giannitto, C., Tironi, A., & Maroldi, R., et al. (2018). Odontogenic keratocyst: imaging features of a benign lesion with an aggressive behaviour. Insights into imaging, 9, 883-897.
- Dias, G., Marques, T., & Coelho, P. (2017). Treatment options for keratocyst odontogenic tumour (KCOT): a systematic review. Oral Surgery, 10(4), 193-209.
- Browne, R. M. (1970). The odontogenic keratocyst: Histological features and their correlation with clinical behaviour. British Dental Journal, 131, 249-259.
- Brannon, R. (1976). The odontogenic keratocyst: A clinicopathologicstudy of 312 cases. Part 1. Clinical features. Oral Surgery, Oral Medicine, Oral Pathology 90, 205-217.
- Mendes, R. A., Carvalho, J. F., & van der Waal, I. (2010). Characterization and management of the keratocystic odontogenic tumor in relation to its histopathological and biological features. Oral oncology, 46(4), 219-225.