
Journal of Novel Physiotherapies Research Reviews(JNP)
ISSN: 2771-7739 | DOI: 10.33140/JNP

Research Article - (2022) Volume 3, Issue 2
Non-attendance to Mammography Screening: A Qualitative Study among Non-attendees in Malta
2University of Highlands and Islands, 12b Ness Walk, Inverness IV3 5SQ, UK
3Faculty of Economics, Management & Accountancy, University of Malta, Msida MSD 2080, Malta, UK
Received Date: Apr 28, 2022 / Accepted Date: May 05, 2022 / Published Date: May 24, 2022
Copyright: ©Copyright: ©2022 Danika Marmara, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Danika Marmara, Gill Hubbard, Vincent Marmara .(2022). Non-attendance to Mammography Screening: A Qualitative Study among Non-attendees in Malta. J Nov Psy, 3(2), 54-64.
Abstract
Background: There is limited qualitative research exploring reasons for underutilisation of breast screening and the broader contexts that affect health-seeking behaviour among women who do not respond to breast screening invitations. This study aims to advance understanding of factors that influence breast screening non-attendance among lifetime nonattendees in Malta.
Methods: Twenty face-to-face qualitative interviews were conducted with women in Malta. These explored women’s illness perceptions regarding breast cancer, knowledge on screening, mammography beliefs, past health-related experiences, medical help seeking behaviour, health and social interactions, and effective interventions that would facilitate mammography attendance. Data were analysed using thematic analysis.
Results: Four themes emerged: 1) attitudes, feelings, beliefs and perceptions; 2) knowledge; 3) social network experiences and 4) perceived effective interventions. Fear of breast cancer and screening emerged as barriers to mammography. The majority of participants had not received physician advice. Previous familial cancer diagnosis prompted lifestyle changes in women, but it was not the primary motivator to attendance. Participants talked about fear of death and traumatic histories from experiences of relatives with cancer or personal traumas. Practical and emotional support are important to non-attendees.
Conclusions: The impact of physical and psychosocial variables on personal resilience and self-confidence should inform the planning of screening interventions. Professionals must refer to patients’ wider support networks and make the necessary referrals, while policy makers should ensure services providing psychological, social and emotional support are accessible.
Keywords
Mammography, Non-Attendance, Qualitative, Malta
Background
Despite the availability of breast screening (BS), many women struggle to access or respond to screening invitations [1-3]. Our previous work suggests non-attendees are more likely to be women with a lower family income, widowers, non-drivers, without a breast condition, without relatives or friends with cancer, less encouraged by a physician, unsure of the screening frequency, and more anxious and fearful [4-8]. However, there is limited qualitative research exploring reasons for underutilisation of BS and the broader contexts, such as psychosocial, economic and structural issues, that affect health-seeking behaviour among lifetime non-attendees. Gaining a more detailed understanding of women’s beliefs and perceptions may help explain why mammography uptake does not appear to be sustained at a population level. In addition, determining women’s sources of information may help explain gaps in knowledge or misconceptions about breast cancer (BC) and BS. Hence, the recognition of these facilitating factors and barriers is the first step in persuading lifetime non-attendees to make better decisions about preventive self-care [9]. This study aims to: 1) Gain a better understanding of beliefs, perceptions, attitudes, barriers and knowledge regarding BS among lifetime non-attendees in Malta and 2) Determine which interventions and channels are appropriate for communicating with women about BC and BS.
Methods
Design
This qualitative study is reported according to Standards for Reporting Qualitative Research (SRQR) [10]. A qualitative methodology was chosen as it was well-suited to capture individual stories. Face-to-face semi-structured interviews were used to explore in-depth issues and understand women’s behaviour [11, 12].
Sampling strategy
Purposeful sampling was adopted by selecting a small number of cases that maximize the diversity of women (heterogeneous sample). Participants were recruited from a larger quantitative study of 404 women, where 13.9% of women (n=56) had never attended for mammography (‘lifetime non-attendees’) [6]. These participants had responded in the population-based survey that they were willing to be contacted further for research purposes. The eligibility criteria were: women aged 50-60 at the time of their first screening invitation, residents in Malta or Gozo with a valid identity card number, able to communicate in English or Maltese, and with no severe co-morbidities. Women were excluded if they had been diagnosed with BC (n=200), if they were invited to the second screening cycle (n=12,210), if registered as deceased at the time of the sample selection (n=71) and if incorrect information existed at the Malta Breast Screening Programme (MBSP) (n=209). From 56 lifetime non-attendees, at least three women were selected per sociodemographic/health status group as these factors are associated with lifetime mammography practices [6]. Women were selected from, but not limited to, the following groups: ‘low family income’, ‘widowers’, ‘non-drivers’, ‘no breast condition/disease’, and ‘no relatives or close friends with cancer’. Figure 1 shows the flow of participants through the study.
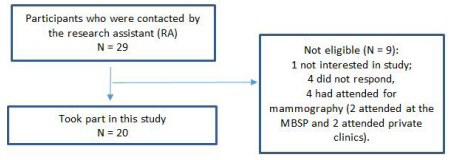
Figure 1: Flow of participants through the study
Context and Data Collection
A research assistant (RA) i.e., a senior nurse and researcher in Malta, contacted potential participants by telephone to confirm they meet eligibility criteria, give them study information and invite them to participate. Those, interested in taking part were invited for a face-to-face interview at a time that suits them, and were given a choice of locations. The RA mailed the information sheet to the participant at least 48 hours before the interview and before signing the consent form.
Interviews were conducted between December 2017 and February 2018. They were carried out in Maltese by a Maltese, bilingual female researcher, with over 10 years’ experience of conducting qualitative research in cancer care. All interviews were conducted privately with only the researcher and the participant present.
Sociodemographic data were collected to describe the sample characteristics. A semi-structured topic guide (Table 1) was developed after consultation with existing literature [9, 12-18]. This guide explored illness perceptions regarding BC, BC prevention and knowledge of screening, mammography beliefs, past health-related experiences, medical help seeking behaviour, interactions with healthcare providers, friends and relatives, BS facilitators and barriers, and effective interventions to facilitate mammography attendance. The guide was piloted with two women of eligible screening age. These pilot data were not included in the main analysis. Interviews continued until data saturation was reached.
Following completion of the interview, participants were given a debrief providing a summary of the study and information on the MBSP.
Table 1: Interview topic guide
|
Interview guide with Maltese women (English version) |
|
|
|
|
|
|
|
|
|
mammogram? Do you think that the quality of the mammogram differs? |
|
in which you have made decisions which you think were risky. |
|
|
|
you to screen regularly? What can we do from our end to help you attend? |
|
Data Analyses
Interviews were transcribed verbatim by the primary author and codes were assigned to each participant to protect their identity. Interviews were translated from Maltese to English by a qualified translator and checked for accuracy by the primary author.
The analysis followed a six-phase guide to thematic analysis [19]: (i) familiarisation, (ii) generation of codes, (iii) searching for themes, (iv) reviewing themes, (v) defining the themes and (vi) writing the report. This qualitative method was chosen due to its flexibility and potential to provide a detailed, and complex data [19].
Familiarisation and initial coding were done by the primary author and discussed with the RA. A selection of transcripts (n = 5) was also coded by RA to verify their consistency. Discrepancies were resolved through discussion. Broad themes were pre-set based on our previous work [20]. These included: (i) attitudes, feelings, beliefs and perceptions, (ii) knowledge, (iii) social network experiences and (iv) perceived effective interventions. Sub-themes emerged from this qualitative study and were strongly influenced by the interview topic guide and pre-set study objectives. Once the coding was completed, the coded transcripts were reviewed independently by two researchers to search for common sub-themes that reflected the pre-set themes. The final list of sub-themes was developed through discussion and checked against the transcripts.
Trustworthiness
Credibility and conformability of data were established in three ways [9]. First, the researcher summarised the interview before ending it and gave participants the opportunity for comments. Participants were also invited to comment on a summary of emergent sub-themes. As a further validity check, the RA interpreted the raw data of these transcripts independently by searching for emerging sub-themes, which ultimately were congruent with that of the researcher. The results were also checked by two women (the same two women who participated in pilot-testing the topic guide) to confirm the aptness of the sub-themes.
Results
Participants
Twenty women took part in the interviews, which lasted between 55 and 77 minutes. Their characteristics are shown in Table 2.
Table 2: Participants characteristics
|
Code |
Age (years) |
Marital status |
Education |
Occupation |
Income |
Do you drive? |
Do you have a family physician (GP) who provides medical care and advice to you? |
Do you have a family history or close friends with cancer? |
Have you ever had any type of breast condition or disease? |
|
NA1 |
58 |
Married |
Secondary |
Housewife |
Between €10,737 – €16,113 |
No |
Yes |
No |
No |
|
NA2 |
64 |
Widowed |
Primary |
Pensioner |
Less than €10,737 |
No |
Yes |
No |
No |
|
NA3 |
61 |
Married |
Primary |
Housewife |
Less than €10,737 |
No |
Yes |
Yes |
No |
|
NA4 |
60 |
Married |
Secondary |
Housewife |
Between €10,737 – €16,113 |
No |
Yes |
Yes |
No |
|
NA5 |
58 |
Married |
Secondary |
Housewife |
Less than €10,737 |
No |
Yes |
Yes |
No |
|
NA6 |
62 |
Separated/ Divorced |
Secondary |
Housewife |
Less than €10,737 |
No |
Yes |
No |
No |
|
NA7 |
56 |
Married |
Primary |
Housewife |
Between €10,737 – €16,113 |
Yes |
Yes |
No |
No |
|
NA8 |
58 |
Widowed |
Secondary |
Pensioner |
Less than €10,737 |
No |
Yes |
Yes |
No |
|
NA9 |
61 |
Married |
Secondary |
Housewife |
Between €10,737 – €16,113 |
No |
Yes |
Yes |
No |
|
NA10 |
59 |
Married |
Secondary |
Housewife |
Less than €10,737 |
No |
Yes |
Yes |
No |
|
NA11 |
60 |
Married |
Secondary |
Housewife |
Between €10,737 – €16,113 |
Yes |
Yes |
No |
Yes |
|
NA12 |
59 |
Married |
Secondary |
Housewife |
Between €10,737 – €16,113 |
No |
No |
Yes |
No |
|
NA13 |
61 |
Married |
Primary |
Housewife |
Less than €10,737 |
No |
Yes |
No |
No |
|
NA14 |
64 |
Married |
Primary |
Housewife |
Less than €10,737 |
No |
Yes |
Yes |
No |
|
NA15 |
59 |
Married |
Secondary |
Private employee |
Between €10,737 – €16,113 |
No |
Yes |
Yes |
No |
|
NA16 |
57 |
Married |
Secondary |
Housewife |
Between €10,737 – €16,113 |
No |
Yes |
Yes |
No |
|
NA17 |
59 |
Married |
Secondary |
Housewife |
Between €10,737 – €16,113 |
No |
No |
Yes |
No |
|
NA18 |
62 |
Married |
Secondary |
Housewife |
Less than €10,737 |
No |
Yes |
Yes |
Yes |
|
NA19 |
62 |
Married |
Secondary |
Housewife |
Between €10,737 – €16,113 |
No |
Yes |
Yes |
No |
|
NA20 |
58 |
Married |
Secondary |
Housewife |
Between €10,737 – €16,113 |
Yes |
Yes |
Yes |
No |
Findings
The findings are presented according to four themes, which include 8 sub-themes. These are illustrated in Table 3.
Table 3: Classification of subthemes expressed by non-attendees
|
Themes |
Subthemes |
Detected Elements |
Categories |
|
Personal beliefs, perceptions, attitudes and feelings |
Perceived severity |
Feeling well Lack of perceived severity Optimism Spiritual beliefs |
Perception of good health Absence of symptoms |
|
Fear |
Fear of cancer diagnosis and its related treatment side effects Fatalism Mammography pain Radiation Mastectomy Embarrassment Experiences of relatives with cancer Not seeing children and grandchildren grow |
Fear of death Physical pain Altered body image Shame Not being there for the family |
|
|
Competing health priorities |
Other personal health problems Cancer in a family member |
Postponement |
|
|
Emotional distress |
Depression and Anxiety Low self-esteem |
Low self-confidence |
|
|
Negative health experiences |
Physical accidents Other surgical operations Late diagnoses Death of relatives/friends |
History of trauma Lack of trust in the health care system |
|
|
Knowledge and awareness |
Insufficient BC/BS information |
Misinformation |
Lack of knowledge |
|
Social network experiences |
Cultural factors Rejection |
Lack of physician-patient relationship Lack of family/partner support Loneliness and isolation |
Ineffective health communication Rejection |
|
Perceived effective interventions |
Able to attend through effective cues to action |
Lack of support Lack of cues to action |
One-to-one counselling GP and partner recommendations Sharing personal experiences |
Theme 1: Personal Beliefs, Perceptions, Attitudes and Feelings
Perceived Severity
Perceptions of good health and absence of symptoms were reported as reasons for not attending mammography:
“There is no need to go and search for it (BC) because I am sure that I am healthy.” (NA15, 59 years)
“I might do mammography only if I see BC, and if I see it, it means I can feel it. Only then will I go to my doctor.” (NA10, 59 years)
Some women described the word ‘cancer’ as a disease that ‘brings negativity’ and wanted to view life in an optimistic manner:
“I am a person that tries not to think negatively and I feel good about myself and positive. This disease (BC) brings sadness, so I just don’t think about it.” (NA10, 59 years)
While participants discussed how their faith in God helped alleviate fears about uncertainties in life, disease and death, four women abdicated their personal responsibilities in preventing BC by resorting to prayer:
“I am determined that when I get to know I have cancer, I will live that remaining year of my life in peace. I will be leaving it in God’s hands. He will take me when he wants to. I could die tomorrow; we all have to die some day or other. We weren’t created to be here.” (NA8, 58 years)
Fear
Perceptions of fear were common in women’s narratives. Women were worried about physical pain and potential radiation exposure during mammography:
“...the fact that I know that I am going to feel pain, I can’t take it. That is what I was told by other women. They press the breasts between two plates and squash them. It isn’t for me.” (NA14, 64 years)
“My husband was fine but after being treated for brain cancer he got worse. It’s about those X-rays they gave him. The cancer spread even more.” (NA9, 61 years)
Worries about exposing themselves in front of health professionals, especially male ones, were also reported:
“I already feel embarrassed about the thought of having to expose my breasts in front of them (radiographers) because they might find it awkward. I actually feel ashamed.” (NA11, 60 years)
“I wouldn’t accept having a male professional checking me. It’s a woman thing.” (NA20, 58 years)
Fear of a cancer diagnosis was another barrier to non-attendance, particularly among women whose relatives had died from the disease:
“I don’t want to have to face the possibility of having a positive result. I have seen my family suffer too much due to BC. My mother had intestinal cancer and died.” (NA5, 58 years)
The majority of participants perceived cancer as an unchangeable fate that cannot be changed:
“If cancer forms in the breasts, you cannot do anything about it. It is nature and no one can control it. There’s no reason to stay beating around the bush. You die anyway. That’s your fate.” (NA7, 56 years)
Women also spoke of how their relatives had suffered from physical pain during chemotherapy:
“My mother (with intestinal cancer) died of intense pain. Chemotherapy kills you literally.” (NA5, 58 years)
Some women spoke of fear of a mastectomy, associating it with a distorted body image:
“I fear having a mammogram because I cannot imagine losing my breasts and passing through that physical pain with drain pipes all over and long-term physiotherapy. This would mean not being a woman anymore, losing my role as a mother. Breasts are part of a woman’s beauty; it inflicts harm on something that symbolizes femininity and motherhood.” (NA11, 60 years)
Finally, women talked about fear of not seeing their children/ grandchildren grow up and how this fear led them to refuse BS attendance to spare the family from suffering:
“I want to see my children grow. It scares me not to see them get married and have their own children, because life is beautiful that way. But the fear is too big an obstacle for me. I don’t want my children to pass through suffering because of me.” (NA6, 62 years)
Competing Health Priorities
Competing health priorities and caretaking roles were reported as reasons for non-attendance:
“I have other health problems which are more important than having screening tests for something that may develop one day.” (NA1, 58 years)
“My husband has been suffering from brain cancer for nine years. (…) Since we have a family, I need to take care of him and all at the moment.” (NA13, 61 years)
Emotional Distress
Emotional distress, including low self-esteem and symptoms of depression and anxiety, featured in women’s narratives:
“Depression messes with your memory. I am on medication and feel very sluggish and nauseated every morning. Leaving the house is difficult and distressing. I’ve been very low to the point where I don’t even want to go out and I’m regularly missing health appointments. I worry that my legs will be amputated due to diabetes and no one will be there for me. It’s very depressing and it actually destroys my self-esteem.” (NA20, 58 years)
Losing one’s sense of control and fearing disease progression were also common concerns:
“I am always worrying about what’s coming next. Will I get cancer myself now after my husband? What will be my next limitations? Will I be disabled? I’m losing my focused frame of mind.” (NA9, 61 years)
Additionally, anxiety around anticipation of results was a barrier to BS screening:
“After experiencing a personal physical accident and passing through a lot, it is daunting for me to wait for a result. I get very anxious and so I don’t go for it (mammography).” (NA1, 58 years)
Negative Health Experiences
Prior negative health care experiences were mentioned by non-attendees:
“I passed through a very bad car accident and spent 14 days in ITU with a torn liver and an internal haemorrhage, and had to undergo many surgical operations, a nightmare, and also ended up diabetic. I don’t want to experience all those tests again. Going to hospital again gives me the shivers. You don’t experience trauma then; the trauma comes out afterwards and you carry it for life.” (NA1, 58 years)
Other dimensions of lifetime traumas arose from the experience of relatives who died of cancer. These experiences reflected issues of lack of trust in the health care system, due to concerns of ‘wrongful’ health care, physician incompetence, medical errors (unintentional harm) or unethical experimentation (intentional harm):
“That doctor killed my mum. It’s better if she hadn’t taken that treatment because she would still be alive. I blame it on them, on the hospital.” (NA20, 58 years)
Women also described negative associations between prevention and disease, relaying experiences of friends who were diagnosed with cancer despite attending mammography:
“Many do mammography, but the doctors do not always find it (BC). My friend did her mammogram and had the all-clear result but in reality, she had it. Eventually, she lost her breast and then her existence.” (NA13, 61 years)
Theme 2: Knowledge and awareness
Insufficient Information
All women identified the importance of receiving information about BC and BS. However, some women had incorrect knowledge about BC prevention:
“I do not need the test. I did a CT (computed-tomography) scan and my breasts were checked during that scan.” (NA6, 62 years)
“I’ve never thought about the possibility of having BC as I breast-fed my children.” (NA19, 62 years)
Women were aware of familial history as a risk factor for BC and also considered lifestyle as important:
“Any woman can get BC, but people with a history of BC in their family, like myself, can get it even more, and those having unhealthy lifestyles too.” (NA2, 64 years)
None of the women gave correct information about screening time frequency. Breast screening examination (BSE) knowledge and practice varied. Some women were worried that BSE may not detect breast lesions:
“I do worry when I check my breasts … that I do not detect what is really in there.” (NA2, 64 years)
Theme 3: Social Network Experiences
Cultural Factors
Thirteen women reported that their GP did not provide adequate recommendations about screening benefits:
“My doctor used to tell me that if I wasn’t up for it (mammography), I would be doing well not to go because he used to tell me… ‘I showed you how to check your breasts, so that’s enough’. And when I received the letter, he told me that I don’t need to go.” (NA8, 58 years)
Some women recognised the powerful role physicians play in encouraging screening compliance and that an ineffective physician–patient relationship may lead to women’s non-attendance to BS:
“I don’t speak to my doctor about breast tests. I don’t have that close relationship with him. And since I don’t ask, he hasn’t ever mentioned it (mammography). I would need to be really pushed to go for one. I would prefer if my GP spoke to me about it.” (NA2, 64 years)
Rejection
Women’s major concern was that having a mastectomy or further treatment would precipitate rejection by their partner. Lack of family support was also a common concern:
“I had a friend whose husband rejected her when she had her breast removed. If I had to have (a breast) removed, I’d think that he’d seek another woman and that I’m no longer attractive to him.” (NA10, 59 years)
“I’ve got four children, all married but none of them take me to health appointments or anywhere really. I feel rejected and alone. Let alone how much I will be able to cope if I found out that something was wrong.” (NA20, 58 years)
Theme 4: Perceived Effective Interventions
Cues To Action
Several women reported that a recommendation from a health professional or a close relative (e.g., partner) would prompt them to consider mammography:
“I would prefer if my doctor spoke to me about mammography. I would consider his recommendations seriously.” (NA2, 64 years) “My husband is my closest link to health care. If he says so, I would consider his advice.” (NA5, 58 years)
Listening to others (e.g., friends, relatives, television) who shared their personal experiences of cancer was also mentioned as a cue to action:
“Women who experience cancer often speak their hearts out. That’s very encouraging.” (NA18, 62 years)
Non-attendees were reluctant to receive brochures, pamphlets and listen to educational talks as these did not seem to increase knowledge and awareness of BC and BS or motivate them to attend:
“Once I receive them (brochures, pamphlets, booklets), they’re immediately discarded.” (NA7, 56 years)
Discussion
This is the first study to explore women’s reasons for non-attending BS in Malta, and their beliefs, perceptions, attitudes and knowledge of BC and BS. The study found women experience several barriers to BS attendance, with fear being the most common barrier. This included fear of cancer diagnosis, pain, death, radiation, embarrassment and of the medical establishment. This is in line with previous research [21-23]. The belief that “it is better not to know” has been reported as a barrier to screening among Hispanic [24] and Turkish women [25]. Women in our study described using neglect and postponement as coping strategies for tackling their fears. Similarly, in another study, around 25% of patients with breast symptoms delayed seeking medical help for more than 3 months [26]. Absence of symptoms as a reason for not attending BS screening has also been reported before [9]. This suggests that the benefits of screening are either poorly understood or that screening is rejected as a premature intervention.
This study found that women were not motivated to perform BS due to competing priorities, such as family responsibilities, and fear of not seeing their (grand)children grow up. This resonates with previous research, showing women prioritise family obligations over own health [27, 28], and supports the notion that women’s fear of not being present within the family supersedes women’s consideration of screening benefits.
Our findings are also consistent with previous studies, whereby social and emotional support from women’s immediate networks, specifically husband/partner and siblings, could motivate women to improve their BS practices [29 - 32]. Alternatively, lack of support may lead to perceptions of rejection, isolation and loneliness. Loneliness has been described extensively in relation to death [33] but not in relation to BS. Additionally, women’s low self-confidence in this study was similar to the effect of women’s low self-efficacy in cancer prevention practices in other studies [34, 35]. Social networks may be important for building self-confidence because they serve as a source of advocacy to increase the effectiveness of health information and aid understanding of cultural factors.
Women also spoke about embarrassment about exposing their breasts in front of others. This is related to privacy matters of sexual organs [31] and literature suggesting women tend to cover their breasts [36, 37] and only allow female professionals to touch them [31]. This is consistent with previous qualitative studies, which reported that physicians’ gender can affect whether women decide to attend screening tests, such as Pap smears and mammography [38, 39, 40]. This implies that the concept of ‘shame’ for women can be avoided through tailored cultural information [41].
Screening non-attendance can also be attributed to underlying spiritual beliefs (e.g., faith in God; [42]). Cancer-related fatalism (i.e., the perception that individuals have limited influence over a disease, [9]) may lead to BS non-attendance as some Maltese women equated mammography with an impending BC diagnosis. The impact of spirituality on health behaviours can be found in a significant body of literature within the African-American community [43, 44]. However, religious, cultural and spiritual beliefs can also be facilitating factors for screening [45], and can be used to tailor empowering messages for Maltese women to take responsibility for their health.
Women’s negative health care experiences and poor patient-provider communication were also reported as barriers to BS screening. Similarly, Partin and Slater [46] found that barriers to non-attendance include prior traumatic experiences in relation of relatives with cancer, and resulting lack of trust in clinicians and mammography. It is known that fear of the health care system and subsequent denial/repression is one mechanism (of many) by which negative health care experiences may facilitate delays in seeking health care [9], resulting in worse health outcomes such as late-stage diagnoses and higher mortality rates. Trauma exposure has also been associated with decreased routine or preventive health care [47, 48] and is tied to substantial health care system costs [49] due to negative mental [50] and physical health effects [51], and disability [52].
Effective health communication is an important motivating factor for BS behaviour [9, 42]. This study found that women would consider a recommendation by the GP to attend screening and improve their knowledge of BC and BS. However, most participants had not received advice from their physician while some had received negative advice towards screening. Insufficient information about screening may partly explain the discordance between women’s beliefs and scientific evidence, and could result in women absorbing incorrect information.
Participants in this study reported following information on the media, including social media, television and radio. Information obtained from these platforms may be unreliable, incomplete and not supported by sufficient evidence [53-56]. There is a need for women to be directed to appropriate and accurate information about cancer screening, possibly by health professionals. Non-attendees suggested various communication channels as facilitators to BS, such as one-to-one counselling, GP/partner recommendations and support, and listening to other women’s personal health experiences. Hence, effective interventions should focus on supporting personal strategies that build upon individual coping styles and preferences, for example counselling women to develop personalised care plans.
Strengths and Limitations
This study produced new knowledge on key factors to be addressed in interventions aiming to increase BS uptake in Malta. While previous research has relied on questionnaires to explore such factors [57-59], this study allowed for any misconceptions to be identified, which strengthens the case for providing BS education to non-attendees. A qualitative approach allowed the researcher to understand how non-attendees processed information about BC and BS. The thematic framework enabled the data to be explored in depth while maintaining a transparent audit trail, which enhances the rigour of the analytical processes and the credibility of findings [60].
This study has some limitations. First, the risk perceptions for non-attendees were not objectively measured, and women may have underestimated or overestimated their actual BC risk [61, 62]. Second, women’s health literacy and actual knowledge of BC and BS were not measured. Inadequate health literacy is strongly associated with lower mammography performance [63, 64]. Third, variation in relation to cancer-related health education beliefs, attitudes and behaviours is likely to exist between countries and regions, limiting generalizability of findings [65, 66].
Conclusions
This is the first study to provide in-depth insights into women’s beliefs, perceptions, knowledge and attitudes for lack of BS use in Malta. The study provides health care providers and policy makers in Malta with evidence specific to their local population for the future development of effective interventions to increasing BS uptake.
List of abbreviations
BS – breast screening
BC – breast cancer
SRQR - Standards for Reporting Qualitative Research
MBSP - Malta Breast Screening Programme
RA – Research Assistant
Declarations
Ethics Approval and Consent to Participate: This study was approved by the School Research Ethics Committee at the University of Stirling (SREC14/15-Paper No. 18v4) and from the Maltese Health Ethics Committee (HEC 02/2015). The authors confirm that all methods were performed in accordance with the relevant guidelines and regulations. Written informed consent was obtained from all participants.
Consent for Publication
No individual data that can identify participants are presented in this manuscript.
Availability Of Data and Materials
The datasets generated and analysed during the current study are not publicly available due to client confidentiality but are available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no competing interests.
Funding
The PhD program was part-financed by the Malta Government Scholarship Scheme (MGSS), Government of Malta (MEDE 96/2012/25).
Authors’ contributions
DM, GH, VM
Acknowledgements
We thank the National Screening Programme in Malta for providing access to participants and all the participants for taking part.
References
- Benoit, C. (2001). Marginalized voices from the downtown eastside: Aboriginal women speak about their health experiences. National Network on Environments and Women’s Health.
- Benoit, C., Carroll, D., & Chaudhry, M. (2003). In search of a healing place: Aboriginal women in Vancouver’s downtown eastside. Social science & medicine, 56(4), 821-833.
- Browne, A. J., Fiske, J. A., & Thomas, G. (2000). First Nations women’s encounters with mainstream health care services & systems. Vancouver, BC: British Columbia Centre of Excellence for Women’s Health.
- Marmarà, D., Marmarà, V., & Hubbard, G. (2017). Maltese translation and adaptation of Champion’s health belief model scale and the revised illness perception questionnaire for breast screening among Maltese women. Journal of Nursing Measurement, 25(3), 486-503.
- Marmarà, D., Marmarà, V., & Hubbard, G. (2017). Health beliefs, illness perceptions and determinants of breast screening uptake in Malta: a cross-sectional survey. BMC public health, 17(1), 1-19.
- Marmarà, D., Marmarà, V., & Hubbard, G. (2018). Lifetime utilization of mammography among Maltese women: a cross-sectional survey. BMC public health, 18(1), 1-14.
- Marmarà, D., Marmarà, V., & Hubbard, G. (2018). A national cross-sectional study of adherence to timely mammography uses in Malta. BMC cancer, 18(1), 1-12.
- Marmarà, D., Marmarà, V., & Hubbard, G. (2017). Predicting reattendance to the second round of the Maltese National Breast Screening Programme: a prospective cohort pilot study. BMC Women’s Health.
- Lamyian, M., Ahmadi, F., Faghihzadeh, S., & Aguilar Vafaie,M. E. (2007). Barriers to and factors facilitating breast cancer screening among Iranian women: a qualitative study. EMHJ-Eastern Mediterranean Health Journal, 13 (5), 1160-1169,2007.
- O’Brien, B. C., Harris, I. B., Beckman, T. J., Reed, D. A., & Cook, D. A. (2014). Standards for reporting qualitative research: a synthesis of recommendations. Academic medicine, 89(9), 1245-1251.
- Frankfort-Nachmias C, Nachmias D. (1992) Research Methods in the Social Sciences, 4th ed. New York: St. Martin’s Press.
- Farooqui, M., Hassali, M. A., Knight, A., Shafie, A. A., Farooqui, M. A., Saleem, F., ... & Aljadhey, H. (2013). A qualitative exploration of Malaysian cancer patients’ perceptions of cancer screening. BMC public health, 13(1), 1-7.
- Ferrat, E., Le Breton, J., Djassibel, M., Veerabudun, K., Brixi, Z., Attali, C., & Renard, V. (2013). Understanding barriers to organized breast cancer screening in France: women’s perceptions, attitudes, and knowledge. Family practice, 30(4), 445-451.
- Fort, J. G., & Ahmed, N. U. (2005). Empowering Factors Among Breast Cancer Screening Compliant Underserved Populations. MEHARRY MEDICAL COLL NASHVILLE TN.
- Lasser, K. E., Ayanian, J. Z., Fletcher, R. H., & Good, M. J. D. (2008). Barriers to colorectal cancer screening in community health centers: a qualitative study. BMC family practice, 9(1), 1-8.
- Markovic, M., Kesic, V., Topic, L., & Matejic, B. (2005). Barriers to cervical cancer screening: a qualitative study with women in Serbia. Social science & medicine, 61(12), 2528-2535.
- Mele, N., Archer, J., & Pusch, B. D. (2005). Access to breast cancer screening services for women with disabilities. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 34(4), 453-464.
- Todd, A., & Stuifbergen, A. (2011). Barriers and facilitators related to breast cancer screening: A qualitative study of women with multiple sclerosis. International Journal of MS Care, 13(2), 49-56.
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative research in psychology, 3(2), 77-101.
- Marmara, D. M. (2019). Improving Participation in Breast Screening Programmes: A mixed methods study to increase breast screening uptake in Malta.
- Borrayo, E. A., Buki, L. P., & Feigal, B. M. (2005). Breast cancer detection among older Latinas: Is it worth the risk? Qualitative Health Research, 15(9), 1244-1263.
- Ogedegbe, G., Cassells, A. N., Robinson, C. M., DuHamel, K., Tobin, J. N., Sox, C. H., & Dietrich, A. J. (2005). Perceptions of barriers and facilitators of cancer early detection among low-income minority women in community health centers. Journal of the National Medical Association, 97(2), 162.
- Young, R. F., & Severson, R. K. (2005). Breast cancer screening barriers and mammography completion in older minority women. Breast cancer research and treatment, 89(2), 111-118.
- Austin, L. T., Ahmad, F., McNally, M. J., & Stewart, D. E. (2002). Breast and cervical cancer screening in Hispanic women: a literature review using the health belief model. Women’s Health Issues, 12(3), 122-128.
- Kissal, A., & Beser, A. (2011). Knowledge, facilitators and perceived barriers for early detection of breast cancer among elderly Turkish women. Asian Pac J Cancer Prev, 12(4), 975-984.
- Montazeri, A., Ebrahimi, M., Mehrdad, N., Ansari, M., & Sajadian, A. (2003). Delayed presentation in breast cancer: a study in Iranian women. BMC women’s health, 3(1), 1-6.
- Payne, S. (2006). The health of men and women. Polity Press.
- Trigoni, M., Griffiths, F., Tsiftsis, D., Koumantakis, E., Green, E., & Lionis, C. (2008). Mammography screening: views from women and primary care physicians in Crete. BMC Women’s Health, 8(1), 1-12.
- Kaltsa, A., Holloway, A., & Cox, K. (2013). Factors that influence mammography screening behaviour: a qualitative study of Greek women’s experiences. European Journal of Oncology Nursing, 17(3), 292-301.
- Kawar, L. N. (2013). Barriers to breast cancer screening participation among Jordanian and Palestinian American women. European Journal of Oncology Nursing, 17(1), 88-94.
- Khazaee-pool, M., Majlessi, F., Foroushani, A. R., Montazeri, A., Nedjat, S., Shojaeizadeh, D., ... & Salimzadeh, H. (2014). Perception of breast cancer screening among Iranian women without experience of mammography: a qualitative study. Asian Pacific Journal of Cancer Prevention, 15(9), 3965-3971.
- Torres, E., Erwin, D. O., Trevino, M., & Jandorf, L. (2013). Understanding factors influencing Latina women’s screening behavior: a qualitative approach. Health Education Research, 28(5), 772-783.
- Sundström, M., Edberg, A. K., Rämgård, M., & Blomqvist,K. (2018). Encountering existential loneliness among older people: perspectives of health care professionals. International Journal of Qualitative Studies on Health and Well-being, 13(1), 1474673.
- Miller, S. M., Lazev, A., Wang, C., Shapiro, P., Diefenbach,M. A., Buzaglo, J. S., & Wise, J. (2005). Cognitive-social and biobehavioral research in cancer prevention and control. Fox Chase Cancer Center 2Ð?Ð?5 Scientific Report. Philadelphia, Fox Chase Cancer Center.
- Otero-Sabogal, R., Stewart, S., Sabogal, F., Brown, B. A., & Pérez-Stable, E. J. (2003). Access and attitudinal factors related to breast and cervical cancer rescreening: why are Latinas still under screened? Health Education & Behavior, 30(3), 337-359.
- Lee, M. C. (2000). Knowledge, barriers, and motivators related to cervical cancer screening among Korean-American women: A focus group approach. Cancer nursing, 23(3), 168-175.
- Suh, E. E. (2008). The sociocultural context of breast cancer screening among Korean immigrant women. Cancer Nursing, 31(4), E1-E10.
- Kwok, C., White, K., & Roydhouse, J. K. (2011). Chinese-Australian women’s knowledge, facilitators and barriers related to cervical cancer screening: a qualitative study. Journal of Immigrant and Minority Health, 13(6), 1076-1083.
- Kwon, H. T., Ma, G. X., Gold, R. S., Atkinson, N. L., & Wang,M. Q. (2013). Primary care physicians’ cancer screening recommendation practices and perceptions of cancer risk of Asian Americans. Asian Pacific journal of cancer prevention: APJCP, 14(3), 1999.
- Taha H, Al-Qutob R, Nyström L, Wahlström R, Berggren V. (2012) Voices of fear and safety women’s ambivalence towards breast cancer and breast health: a qualitative study from Jordan. BMC Women’s Health, 2012: 12.
- Wang, J. H. Y., Schwartz, M. D., Brown, R. L., Maxwell, A.E., Lee, M. M., Adams, I. F., & Mandelblatt, J. S. (2012). Results of a randomized controlled trial testing the efficacy of a culturally targeted and a generic video on mammography screening among Chinese-American immigrants. Cancer Epidemiology and Prevention Biomarkers, 21(11), 1923-1932.
- Bener, A., Honein, G., Carter, A. O., Da’ar, Z., Miller, C., & Dunn, E. V. (2002, October). The determinants of breast cancer screening behavior: a focus group study of women in the United Arab Emirates. In Oncology nursing forum (Vol. 29, No. 9).
- Guidry, J. J., Matthewsâ?Juarez, P., & Copeland, V. A. (2003). Barriers to breast cancer control for Africanâ?American women: the interdependence of culture and psychosocial issues. Cancer, 97(S1), 318-323.
- Mansfield, C. J., Mitchell, J., & King, D. E. (2002). The doctor as God’s mechanic? Beliefs in the Southeastern United States. Social science & medicine, 54(3), 399-409.
- Islam, N., Patel, S., Brooks-Griffin, Q., Kemp, P., Raveis, V., Riley, L., ... & Kwon, S. (2017). Understanding barriers and facilitators to breast and cervical cancer screening among Muslim women in New York City: perspectives from key informants. SM journal of community medicine, 3(1).
- Partin, M. R., & Slater, J. S. (2003). Promoting repeat mammography use: insights from a systematic needs assessment. Health education & behavior, 30(1), 97-112.
- Farley, M., Minkoff, J. R., & Barkan, H. (2001). Breast cancer screening and trauma history. Women & Health, 34(2), 15-27.
- Schnurr, P. P., & Green, B. L. (2004). Trauma and health: Physical health consequences of exposure to extreme stress. American Psychological Association.
- Walker, E. A., Katon, W., Russo, J., Ciechanowski, P., Newman, E., & Wagner, A. W. (2003). Health care costs associated with posttraumatic stress disorder symptoms in women. Archives of General Psychiatry, 60(4), 369-374.
- Consedine, N. S., Magai, C., Krivoshekova, Y. S., Ryzewicz, L., & Neugut, A. I. (2004). Fear, anxiety, worry, and breast cancer screening behavior: a critical review. Cancer Epidemiology and Prevention Biomarkers, 13(4), 501-510.
- Seng, J. S., Clark, M. K., McCarthy, A. M., & Ronis, D. L. (2006). PTSD and physical comorbidity among women receiving Medicaid: Results from serviceâ?use data. Journal of traumatic stress, 19(1), 45-56.
- Bala, M. M., Strzeszynski, L., & Toporâ?Madry, R. (2017). Mass media interventions for smoking cessation in adults. Cochrane Database of Systematic Reviews, (11).
- Chew, F., Palmer, S., Slonska, Z., & Subbiah, K. (2002). Enhancing health knowledge, health beliefs, and health behavior in Poland through a health promoting television program series. Journal of Health Communication, 7(3), 179-196.
- Korownyk, C., Kolber, M. R., McCormack, J., Lam, V., Overbo, K., Cotton, C., ... & Allan, G. M. (2014). Televised medical talk shows—what they recommend and the evidence to support their recommendations: a prospective observational study. bmj, 349.
- Marx, J. J., Nedelmann, M., Haertle, B., Dieterich, M., & Eicke, B. M. (2008). An educational multimedia campaign has differential effects on public stroke knowledge and care-seeking behavior. Journal of neurology, 255(3), 378-384.
- Anagnostopoulos, F., Dimitrakaki, C., Fitzsimmons, D., Potamianos, G., Niakas, D., & Tountas, Y. (2012). Health beliefs and illness perceptions as related to mammography uptake in randomly selected women in Greece. Journal of clinical psychology in medical settings, 19(2), 147-164.
- Okobia, M. N., Bunker, C. H., Okonofua, F. E., & Osime, U. (2006). Knowledge, attitude and practice of Nigerian women towards breast cancer: a cross-sectional study. World journal of surgical oncology, 4(1), 1-9.
- Sobani, Z. U. A., Saeed, Z., Baloch, H. N. U. A., Majeed, A., Chaudry, S., Sheikh, A., ... & Qadir, I. (2012). Knowledge attitude and practices among urban women of Karachi, Pakistan, regarding breast cancer. Journal of Pakistan Medical Association, 62(11), 1259.
- Ritchie, J., Lewis, J., Nicholls, C. M., & Ormston, R. (Eds.). (2013). Qualitative research practice: A guide for social science students and researchers. sage.
- Apicella, C., Peacock, S. J., Andrews, L., Tucker, K., Daly,M. B., & Hopper, J. L. (2009). Measuring, and identifying predictors of, women’s perceptions of three types of breast cancer risk: population risk, absolute risk and comparative risk. British journal of cancer, 100(4), 583-589.
- Fehniger, J., Livaudais-Toman, J., Karliner, L., Kerlikowske, K., Tice, J. A., Quinn, J., ... & Kaplan, C. P. (2014). Perceived versus objective breast cancer risk in diverse women. Journal of Women’s Health, 23(5), 420-427.
- Pagán, J. A., Brown, C. J., Asch, D. A., Armstrong, K., Bastida, E., & Guerra, C. (2012). Health literacy and breast cancer screening among Mexican American women in South Texas. Journal of Cancer Education, 27(1), 132-137.
- Rakhshkhorshid, M., Navaee, M., Nouri, N., & Safarzaii, F. (2018). The association of health literacy with breast cancer knowledge, perception and screening behavior. European journal of breast health, 14(3), 144.
- Livingston J. (2012). Improvising medicine: An African oncology ward in an emerging cancer epidemic. Durham, NC: Duke University Press, 2012: 1-52.
- Azubuike S, Okwuokei S. (2013). Knowledge, attitudes and practices of women towards breast cancer in Benin City, Nigeria. Ann Med Health Sci Res, 3: 155-160.