
Advancements in Journal of Urology and Nephrology(AJUN)
ISSN: 2689-8616 | DOI: 10.33140/AJUN
Impact Factor: 1.0



Case Report - (2020) Volume 2, Issue 1
Nephron sparing surgery for giant renal angiomyolipoma; a viable option?
2Resident, Department of Urology, St John’s Medical College, Bengaluru, Karnataka, India
3Resident, Department of Urology, St John’s Medical College, Bengaluru, Karnataka, India
4Assistant Professor, Department of Urology, St John’s Medical College, Bengaluru, Karnataka, India
5Resident, Department of Urology, St John’s Medical College, Bengaluru, Karnataka, India
Received Date: Jan 20, 2020 / Accepted Date: Feb 03, 2020 / Published Date: Feb 13, 2020
Copyright: ©Zaffar K Sayed. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Angiomyolipomas (AML) are most common benign tumors of the Kidney. It may be an incidental diagnosis or in symptomatic patients it may cause flank pain,hematuria or renal mass. Also, sometimes renal AML may present initially as spontaneous retroperitoneal hemorrhage secondary to rupture (Wunderlich syndrome). AML >10 cm in size is known as giant AML and the data available on this entity is sparse. Herein, we report a case of a 28-year-old homemaker who had left flank pain for 3 months, on evaluation elsewhere, Ultrasonography, and Contrast Computed Tomography Scan - Kidney Ureter Bladder showed a left giant renal AML. This patient came to our centre for further management. Subsequently, this patient underwent left open Partial Nephrectomy; specimen was 21.5 cm x 16 cm x 14 cm in size and weighed 1330 g. Histopathological analysis showed AML. It is important to contemplate a primary nephron sparing approach even in a case of giant renal AML, as it may turn out to be a correct choice with a positive outcome.
Keywords
Giant AML, Nephron Sparing Surgery, Partial Nephrectomy, Simple Nephrectomy, Viable Option.
Introduction
Angiomyolipomas (AML) are the most common benign tumors of the Kidney, also known as renal hamartoma, and are sporadic in 80% of the cases. Renal AML have mesenchymal origin with autosomal dominant inheritance [1, 2]. Histologically, these lesions contain varying proportions of blood vessels, smooth muscle, and fat [3]. Further, any renal AML of >10 cm in size is known as giant AML which is a rare manifestation [4]. While managing these giant AML, primary Nephron Sparing Surgery (NSS) is not always the preferred approach. However, as this patient population is young, and may be having multiple/bilateral lesions or AML in the presence of Tuberous Sclerosis (TS), it will be prudent to preserve maximum functional renal parenchyma to the extent possible. Herein, we report our experience with a case of giant AML with successful open Partial Nephrectomy (PN) even without the advantage of pre-operative selective angioembolization.
Case Presentation
This patient, 28-year-old homemaker, who experienced left flank pain of 3 months duration, and underwent evaluation in her hometown. Ultrasonography (USG) and Contrast Computed Tomography Scan - Kidney Ureter Bladder (CT-KUB) was advised, which showed a left renal giant AML, and patient was referred to our centre for further management. After taking complete history, detailed clinical examination was performed; a palpable lump was noted in the left upper quadrant of the abdomen. There were no stigmata of Tuberous Sclerosis. We discussed with the patient, and her husband about the diagnosis, the available options for the management of this giant AML, and the possibility of need for Nephrectomy. Finally, due to their limited financial backup we took collective decision to go ahead with Left Partial/Simple Nephrectomy and excision of the mass. It was a challenge to plan the approach in this case with no advantage of pre-operative selective angioembolization to minimize the chances of intra-operative bleeding. Subsequently, after examining the available imaging studies, we planned it as a Nephron Sparing Surgery (NSS).
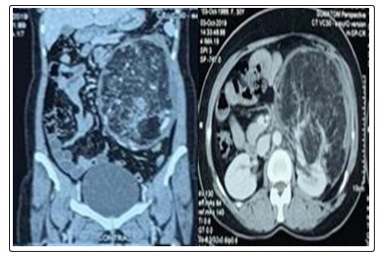
Figure 1: CT-Scan images showing left renal giant AML in coronal view (a) & axial view (b).
With trans-peritoneal approach by Chevron incision, we did Left PN along with tumor removal. Intra-operatively, the mass measuring 21.5 cm × 16 cm × 14 cm in size was arising from the anterior surface of the left kidney from the inter-polar region extending towards the lower pole. Further, it was pushing the kidney posteriorly with the colon, small bowel, and aorta pushed medially. Adhesions were released till we could reach the anterior surface of the kidney without compromising the oncological clearance. After ligating the feeder vessels, the mass was lifted off the anterior surface of the kidney with blunt and sharp dissection only to have <20% of the renal parenchyma adherent to the base of the mass. We delivered the specimen out, it weighed 1330 g. Drain tube placed in the left para-colic gutter after confirming hemostasis, and closure done in layers. Post-operative period was uneventful. Functional assessment showed 38 % function on the left side. We discharged the patient with advice to follow-up.
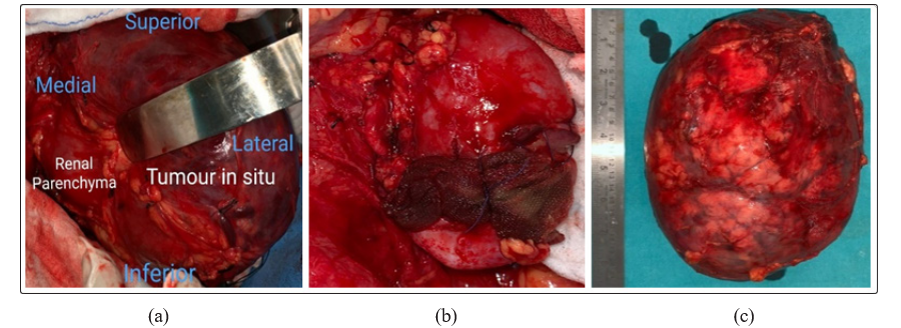
Figure 2: Showing images of intra-operative specimen with tumor in situ (a), Left kidney after removal of the tumor (b), tumor specimen21.5 cm × 1 6 cm × 14 cm post retrieval (c).
Discussion
Renal AML are the most common benign mesenchymal lesions with variable proportions of vascular, smooth muscle and fat. Sporadic cases of AML, which are more commonly seen (80%) usually have small size (<4 cm) and are solitary tumors [1, 2]. But, these tumors when they grow >10 cm in size, they are labelled as Giant AML. The data available in relation to this entity is sparse [4]. Taneja R et al. in 2013 reported a sporadic case of giant AML measuring 39 cm × 25 cm × 9 cm and weighing 7500 g in a 49-year-old female patient. This patient underwent Simple Nephrectomy (SN) as intra-operatively it was noted that the entire kidney was replaced by fat containing tumour [5]. Similarly, another case reported in 2016 by Albersheim-Carter et al. of a 61-year-old woman who presented with large retroperitoneal bleed, and was diagnosed to have a giant, sporadic AML of 30 cm × 26.5 cm × 18 cm in size for which the patient underwent segmental arterial embolization, followed by an open left PN [6]. Likewise, Chen et al. in 2017 described a case of 34-year-old patient having sporadic giant AML with lesion of 29 cm × 20 cm × 10 cm. This patient was taken up for diagnostic laparoscopy followed by Laparotomy with SN, as it was a non-functioning kidney [7]. Furthermore, in 2018, Arya A et al. documented a case of 35-year-old female patient with lesion measuring 40 cm × 20 cm × 15 cm in size and 7000 g in weight. This case with large AML of 40 cm was managed by nephron-sparing surgery without prior angioembolization [8]. The index case reported here had a tumor size of 21.5 cm × 16 cm × 14 cm , weighed 1330 g, and is not as large as in cases reported earlier. But it was also managed in the same way as described by Arya et al. Well, with the cases described above in the background, and in the absence of any defined protocol for the surgical approach for these rare cases of giant renal AML. It would be prudent to take it on case to case basis with the primary aim of NSS wherever possible making it a practical choice.
Sporadic cases of AML are commonly seen in fifth or sixth decade of life with female preponderance [9]. It can be deduced from the above description; the uniqueness of our case report is that the age of the patient is such that it is probably the youngest female patient with documented giant renal AML who underwent successful PN. Although, the incidence of renal AML is <0.2% in general population with a prevalence of 0.3% to 3% of all surgically resected renal tumors, making it a rare entity. It looks like the incidence of giant AML is under-estimated due to under-reporting. In addition, due to the rampant use of imaging studies for the evaluation of various abdominal disorders, giant AML is being diagnosed more often as compared to earlier. Now, it would not be logical to attribute this increased incidence of giant AML to only one factor like commonly used imaging and there may be one or more other factors contributing to it which needs further evaluation. Also, another point that we want to highlight here is that more and more patients are being diagnosed with giant AML at an early stage in life which is in contrast with the age group in which it is commonly known to occur. This opens one more avenue for further studies to shed some light on the reason for this change in the demographics of the affected patients.
The treatment options for sporadic renal AML with various presentations like lesion >4 cm, symptomatic patients, bilateral/ multiple tumors, recurrent masses, in patients with high risk of bleeding and giant AML includes selective angioembolization, Exploratory Laparotomy with SN/PN, Laparoscopic/Robotic SN/ PN. One of the approaches described even includes Diagnostic Laparoscopy in certain indeterminate cases as discussed above. The characteristic feature of these lesions is that they usually arise only from a small area over the surface of the kidney [10, 11]. It is this peculiarity of these lesions which can be exploited to the maximum, as it makes them amenable to resection with the intention to preserve renal parenchyma by NSS even in cases of giant AML by Open/Laparoscopic/Robotic method. Lastly, given the variety of approaches followed to tackle these cases, there is an urgent need to have a defined treatment protocol for this not so uncommon entity thereby leading to an improvement in delivery of patient care and outcome in an evidence based manner.
Conclusion
In view of the benign nature of this condition and the possibility of bilateral, multiple tumours or risk of recurrence as seen in Tuberous Sclerosis – The primary goal should be to safeguard the renal function to the maximum by Nephron Sparing approach thereby delaying the need for renal replacement therapy and leading to an improved quality of life.
Authors Contributions
Surya Kant Choubey - The conception and design of the study, acquisition of data and final approval of the version to be submitted.
Zaffar Karam Sayed - Acquisition of data, its analysis and interpretation. Drafting of the article and revised it critically for important intellectual content.
Rahul Yogesh Saboo - Acquisition of data, its analysis and interpretation. Drafting of the article.
Conflict of Interest: Declared none.
Acknowledgement: We thank the patient for permitting us to use her details and images.
Funding: No source
Institutional Review Board Approval and Informed Consent: Obtained
References
- Seyam RM, Bissada NK, Kattan SA, Mokhtar AA, Aslam M, et al. (2008) Changing trends in presentation, diagnosis, and management of renal angiomyolipoma: Comparison of sporadic and tuberous sclerosis complex associated forms. Urology 72:1077 1082.
- Ewalt DH, Sheffield E, Sparagana SP, Delgado MR, Roach ES, et al. (1998) Renal lesion growth in children with tuberous sclerosis complex. J Urol 160: 141 145.
- Garg PK, Jain BK, Kumar A, Bhatt S, Vibhav V, et al. (2012) Fat poor angiomyolipoma with lymphadenopathy: Diagnostic dilemma. Urol Ann 4: 126-129.
- Chronopoulos PN, Kaisidis GN, Vaiopoulos CK, Perits DM, Varvarousis MN, et al. (2016) Spontaneous rupture of a giant renal angiomyoli¬poma Wunderlich’s syndrome: Report of a case. Int J Surg Case Rep 19: 140 143.
- Taneja R, Singh DV (2013) Giant Renal Angiomyolipoma: Unusual Cause of Huge Abdominal Mass. J Clin Imaging Sci 3: 56.
- Albersheim-Carter J, Klein M, Murugan P, Weight J C (2016) Partial Nephrectomy for a Massive Sporadic Renal Angiomyolipoma: Case Report and Review of the Literature. Case Reports in Urology 2016: 1-5.
- Peijie Chen, Lu Jin, Yu Yang, Zebo Chen, Yongqing Lai, et al. (2017) Giant renal Angiomyolipoma: A case report. Molecular and Clinical Oncology 7: 298-300.
- Arya A, Bhatyal H, Narang V, Agarwal S (2018) Nephron-sparing Surgery without Angioembolization in Giant Angiomyolipoma: Is it Feasible? J Urol Surg 5: 191-193.
- Weight CJ, Lieser G, Larson BT, Gao T, Lane BR, et al. (2010) Partial nephrectomy is associated with improved overall survival compared to radical nephrectomy in patients with unanticipated benign renal tumours. Eur Urol 58: 293-298.
- Nelson CP, Sanda MG (2002) “Contemporary diagnosis and management of renal angiomyolipoma”. Journal of Urology 168: 1315-1325.
- Ljungberg B, Hedin O, Lundstam S, Warnolf Å, Mandahl Forsberg A, et al. (2016) Nephron Sparing Surgery Associated with Better Survival than Radical Nephrectomy in Patients Treated for unforeseen Benign Renal Tumors. Urology 93: 117-121.
- Vitaly M, Surena FM, Christopher GW (2012) Benign renal tumors. In: Campbell-Walsh, Urology. 10th ed. Philadelphia: Saunders Elsevier 1498-501.