
Journal of Clinical Pediatrics and Child Care Research(JCPCCR)
ISSN: 2832-2584 | DOI: 10.33140/JCPCCR
Impact Factor: 1.10



Case Report - (2025) Volume 6, Issue 1
Neonatal Hydrometrocolpos Complicated by Obstructive Uropathy: A Case Report
2Department of Obstetrics and Gynaecology, Orotta College of Medicine and Health Sciences, Asmara, Eritrea
3Orotta National Referral Maternity Hospital, Ministry of Health, Asmara, Eritrea
4Department of Radiology, Orotta College of Medicine and Health Sciences, Asmara, Eritrea, Eritrea
5Department of Pediatrics, Orotta College of Medicine and Health Sciences, Asmara, Eritrea
Received Date: Aug 20, 2024 / Accepted Date: Jan 15, 2025 / Published Date: Feb 13, 2025
Copyright: ©2025 Okbu Frezgi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Yassin, R., Ghirmay, R., Sereke, D., Zain, H., Teckle, H., et, al. (2025). Neonatal Hydrometrocolpos Complicated by Obstructive Uropathy: A Case Report. J Cli Ped Chi Res, 6(1), 01-04.
Abstract
The most common congenital urogenital anomalies causing hydrometrocolpos is imperforate hymen. In the neonatal period, the development of hydrometrocolpos can rarely cause obstructive uropathy due to compression of the lower urinary tract. Here we report a neonate came with a history of abdominal distention, and failure to pass urine. The neonates was irritable with a firm, mobile abdomino-pelvic mass of 10 ×12 cm size and imperforate bulged hymen. Magnetic resonance imaging of abdomen showed hydrometrocolpos with bilateral hydronephrosis. She was successfully managed with hymenectomy under sedation, and hydronephrosis resolve postoperatively. Future fertility issues warrant assessment of tubal patency. Proper perinatal and postnatal evaluation for possible congenital urogenital anomalies are needed in early diagnosis and mitigating their complications.
Keywords
Imperforate Hymen, Neonatal Hydrometrocolpos, Hydronephrosis, Hymenectomy
Introduction
Hydrometrocolpos is accumulation of fluid and/or mucus secretions in vagina and uterus due to distal vaginal obstruction caused by congenital urogenital anomalies or acquired etiologies [1-3]. It's a rare clinical condition with estimated incidence of ~0.006% per year in full-term newborns [1,2]. In the neonatal period, the development of hydrometrocolpos or pyometrocolpos can rarely cause obstructive uropathy due to compression of the lower urinary tract [4,5]. The most common cause in childhood and adolescence is congenital anomalies, most being an imperforate hymen with estimated worldwide incidence of at 0.014-0.1% [4, 6-9].
Development of female genital tract begins at 3rd week of pregnancy and completes during second trimester. The upper part of vagina is formed from MUllerian ducts and lower third from urogenital sinus and both structures contact at MUllerian tubercle [1,3]. Imperforate hymen in female fetuses or neonates leading to hydrometrocolpos may be incidentally discovered during the prenatal obstetrics ultrasound. After delivery neonates often present nonspecific symptoms dominated by suprapubic mass, vulvoperineal mass, tenderness and compression of adjacent structures, commonly the urinary bladder and ureters that results in urinary retention and obstructive uropathy respectively [1-3,5,10,11]. Early diagnosis and treatment is crucial to prevent complications such as tubal infection, adhesion, pelvic endometriosis, infertility, and renal failure secondary to hydronephrosis [3,10]. Imaging techniques like ultrasonography, and magnetic resonance imaging (MRI) are used to evaluate patients with hemato/hydrocolpos and particularly MRI with high-resolution and soft tissue contrast, provides useful information for the differential diagnosis of obstructive causes and management decisions [2, 3]. Generally imperforate hymen is managed by hymenotomy (surgical incision of the hymen) or hymenectomy (surgical removal of the hymen) [1,3,12,13].
Case Report
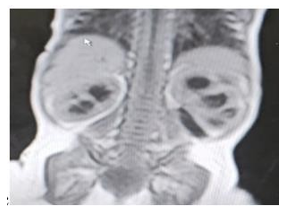
This 26 days old neonate presented to hospital with history of progressive abdominal distention, , difficulty in breastfeeding and which later accompanied by failure to pass urine which forced them to seek help. She has no history of vomiting or fever and passes stool three times a day. She was born from a 29 years old primgarvida mother at term with normal Apgar score and birth weight of 3.9 kilograms. Early neonatal period was uneventful until her comeback with the above mentioned complaint. On physical examination she was in mild distress with vital signs were blood pressure 80/40 mmHg, pulse rate-149 beats / minute, respiratory rate- 44 breaths/minute, oxygen saturation of 95%, temperature -36.5 ° C in the left axilla. Abdomen was grossly distended and a firm, mobile, tender abdominopelvic mass of 10 ×12 centimeters in size was identified. On genital examination there was no gross malformation and the hymen was bulged with no opening. Her hemoglobin 10.47 mg/dl, albumin 3.3, AST 67, ALT 97, ALP 72, creatinine 0.6, BUN 45, NA 115, Cl 112, K 4.2. Trans-abdominal ultrasonography showed 10× 7.7 cm hypoechoic wall defined pelvic mass with bilaterally dilated renal pelvises. MRI showed a structure with a configuration of a distended uterus and vagina that extends downward to vulvar region with bilateral moderate uretero- hydronephrosis. (Figure 1)


A B
C
Figure 1: Imaging Results (A) Trans-abdominal USG showing 10× 7.7 cm hypoechoic wall defined pelvic mass and both renal pelvis dilated. (B.C) MRI showing irregular, well circumscribed, pelvic-abdominal structure that shows low TI and high T2 signals, denoting its cystic nature with a measurement of 8.4×11.7× 9.5 cm. The structure has the configuration of a distended uterus and vagina that extends downward to vulvar region with bilateral moderate uretero- hydronephrosis.
A.  B.
B. 
C. 
Figure 2: (A) Grossly Distended Abdomen in Operating in Operating Room (B) Bulged Hymen with No Opening (C) Cruciate Incision at Center of Hymen Under Sedation.
With the diagnosis of hydromucometrocolpos secondary to imperforate hymen, a cruciate incision at center of hymen was performed under sedation and 500ml of fluid, milky mixed with blood was drained and four stitches were applied. During her follow up the uterine size and hydronephrosis progressively resolved.
Discussion
Normally hymen ruptures usually in utero due to degeneration of central epithelial cells and persists due to abnormalities in the degeneration of the central epithelial cells [3]. Imperforate hymen is the most common congenital malformation of the female genital tract, rarely leads to obstructive uropathy [1]. Due to its non-specific symptoms and rare incidence, diagnosis of congenital hydrometrocolpos requires high index of suspicion with careful history and perineal examination [4]. The diagnosis of congenital hydrometrocolpos can be made both postnatal and antenatal period in which detection has been reported as early as 25 gestational weeks [1,10,12]. In our case, imperforate hymen causes hydrometrocolpos, bilateral hydronephrosis and acute urinary retention.
The clinical presentation depends on the degree of compression to the surrounding structure commonly, the urinary tract, causing varying degrees of hydronephrosis [4,5]. In addition, patients with hydrometrocolpos may manifest as abdominal distention, and palpable, tender intra-abdominal mass or vulvoperineal mass [4,11]. On severe cases, the neonates can be presented with acute urinary retention and intestinal obstruction [2]. Similarly our patient presented with abdominal distention, difficulty to breast feeding and failure to pass urine which dictates the severity of the mass related compression. In hydrometrocolpos two types of fluids accumulates: mucus, secreted by the glands of the uterus and cervix, and urine, secondary to urogenital or cloacal malformation. [5,9]. In our case the color of the fluid milk mixed with blood probably due to the tearing of small blood with in the uterine wall or withdrawal of maternal estrogen.
Postnatally, careful perineal inspection, could help early suspicion of distal vaginal occlusion. Diagnosis can be confirmed using ultrasonography and MRI being of particular use in the presence of other congenital abnormalities due to its superior soft-tissue resolution [1,2]. The earlier the diagnosis of hydrometrocolpos, the lower risk of complications such as urinary tract infection, hydroureternephrosis, urinary retention, constipation, bowel obstruction, renal failure, rupture of hydrometrocolpos, peritonitis, and sepsis [1,2,4,8]. The surgical approach in managing patients with hydrometrocolpos and its complications, depend on the causes for developing hydrometrocolpos. [5,8] It has both short and long goals, in which short goals are alleviating the obstruction of the vagina and long terms are preserving satisfactory cosmesis, sexual function and fertility [11]. The surgical options for imperforate hymen are two, i.e., hymentomy and hymenectomy. In our case, the surgical option used, was cruciate incision of hymentomoy.
Conclusion
Obstructive uropathy complicated by Hydrometrocolpos in neonate can simply reversed by hymentomoy under sedation. A high index of suspicion during prenatal ultrasound and careful perianal examination after delivery helps early detection and intervention to prevent related complications.
Ethical Approval and Consent to Participate
The Ministry of Health does not require ethical approval for case reports or case series. Written informed consent was obtained from the patient to share her case details and any accompanying images published globally.
Acknowledgement
We like to Acknowledge to Dr. Essaias radiology department, and staff of Orotta national referral hospital.
References
- Tegene, D., Assefa, T., & Edris, A. (2023). Neonatal Hydrometrocolpos Secondary to Imperforate Hymen Presented with Acute Urinary Retention: Case Report. Research and Reports in Neonatology, 23-28.
- Osman, N. M., Hamza, A. M., & Elamin, H. A. M. (2019). Congenital vaginal obstruction in a newborn. Sudanese Journal of Paediatrics, 19(2), 145.
- Tanitame, K., Tanitame, N., Urayama, S., & Ohtsu, K. (2021).Congenital anomalies causing hemato/hydrocolpos: imaging findings, treatments, and outcomes. Japanese Journal of Radiology, 39(8), 733-740.
- Dahal, G. R., Phuyal, S., & Agrawal, P. (2020). Symptomatic imperforate hymen in early infancy: a case report. JNMA: Journal of the Nepal Medical Association, 58(226), 433.
- Chen, M. C., Chang, Y. L., & Chao, H. C. (2022).Hydrometrocolpos in infants: etiologies and clinical presentations. Children, 9(2), 219.
- El-Messidi, A., & Fleming, N. A. (2006). Congenital imperforate hymen and its life-threatening consequences in the neonatal period. Journal of pediatric and adolescent gynecology, 19(2), 99-103.
- Aljahdali, E. A., & Kurdi, M. O. (2022). Hymen-saving hymenotomy of imperforate hymen in neonates and adolescents: tertiary medical center experience. Annals of Pediatric Surgery, 18(1).
- Ramphul, M., Perry, L., & Bhatia, C. (2016). Neonatal imperforate hymen with hydrocolpos. Case Reports, 2016, bcr2016215434.
- Wróblewska-Seniuk, K., Jarzabek-Bielecka, G., & Kedzia,W. (2021). Gynecological problems in newborns and infants.Journal of Clinical Medicine, 10(5), 1071.
- Kwache, I., Meher, S., Balogun, M., Ewer, A. K., & Toldi,G. (2021). Fetal ultrasound diagnosis allows effective early postnatal treatment of hematometrocolpos. Clinical Case Reports, 9(5), e04088.
- Saxena, A. K., & Zuckerman, A. L. (2022). Pediatric imperforate hymen: Clinical presentation. J Pediatr Surg, 57(10), 2031-2034
- Nicassio, L. N., Cheng, J. W., & Cain, M. P. (2022). Bedside intervention for neonatal hydrometrocolpos and imperforate hymen. Urology, 160, 191-194.
- Salhan, B., Omisore, O. T., Kumar, P., & Potter, J. (2013). A rare presentation of imperforate hymen: a case report. Case Reports in Urology, 2013(1), 731019.