
Journal of Clinical Pediatrics and Child Care Research(JCPCCR)
ISSN: 2832-2584 | DOI: 10.33140/JCPCCR
Impact Factor: 1.10



Research Article - (2026) Volume 7, Issue 1
Multidisciplinary Perspectives of the Impact of Child Life Services in the Emergency Room and Radiology
2Radiology Child Life Specialist, Nemours Children’s Hospital, United States
3Supervisor of Child Life & Creative Arts Therapies, Nemours Children’s Hospital, United States
4Music Therapy Fellow, Nemours Children’s Hospital, United States
Received Date: Apr 25, 2026 / Accepted Date: Jan 08, 2026 / Published Date: Feb 09, 2026
Copyright: ©2026 Kristin Brown, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Brown, K., Tolland, M., Read, J., Thorn, A. (2026). Multidisciplinary Perspectives of the Impact of Child Life Services in the Emergency Room and Radiology. J Cli Ped Chi Res, 7(1), 01-06.
Abstract
Child life specialists focus on the psychosocial care of hospitalized children by assessing stress points and providing evidence- based interventions to promote coping. However, little is known about how clinical staff perceive child life interventions and responsibilities. The goal of this study is to add to the existing literature in the field of child life to better support child life specialists in understanding how various healthcare professionals’ views of the child life profession contributes to patient care. A total of 89 out of 154 eligible staff at Nemours Children’s Hospital Orlando responded to the survey, including nurses, radiology technologists, emergency physicians, paramedics, registration assistant, patient care technicians, nurse practitioners, and physician assistants. In the ED, the top three perceived responsibilities noted were procedural support, education and preparation, and nonpharmacological pain management. In radiology, the top three perceived responsibilities noted were education and preparation, procedural support, and providing toys/playing with patients. Limitations of this study are due to the limited sample size and the recent growth of this field of study. Future implications land on the desire of participants to have increased child life coverage in both units covered in this study. It is that child life specialists are essential and invaluable members of the healthcare team, but the lack of knowledge of the field of child life and the interventions and responsibilities within has caused child life specialists to be viewed as supplementary team members when compared with other health care professionals.
Keywords
Child Life Specialist, Multidisciplinary, Emergency, Radiology
Introduction
Everyday children and adolescents are hospitalized as a result of chronic, emergent, and even traumatic conditions, with these hospital experiences often being incredibly stressful life events for pediatric patients. Two of the units within pediatric hospitals that see a high volume of these patients are the emergency and radiology departments. According to the National Centre for Health Statistics, 18% of children under 18 years of age have had one or more emergency department visits in their life, with 6.7% having two or more visits a year. Within radiology, it is estimated that more than 62 million cat scans (CT) per year are currently obtained in the United States, with at least 4 million being done for children [1]. When children are uncooperative for these procedures, there is a need for increased sedative medications, staffing, time of subsequent appoints, and more, all which add to the rising healthcare costs.
Within both the pediatric radiology departments and emergency rooms, child life specialists work closely with the multidisciplinary team to address the psychosocial needs of patients and their families. The Association of Child Life Professionals is responsible for developing and maintaining the scope of practice and ethics of certified child life specialists [2]. The ACLP notes that certified child life specialists (CCLSs) are educated and clinically trained in understanding the impact of illness and injury on developmental outcomes [2]. CCLSs typically work both in healthcare and community settings, with their main goal being to help infants, children, youth, and their families cope with the stress and uncertainty of illness, injury, trauma, disability, loss, and bereavement [2]. Clinicians work towards this goal by providing evidence based, developmentally, and psychologically appropriate interventions that include therapeutic play, preparation and coping support for procedures, and health education to reduce fear, anxiety, and pain [2]. For example, child life specialists can participate in patient care by teaching a child coping strategy for adjusting to a life-changing injury, promoting coping with examinations for alleged abuse, assisting families in talking to their children about death, facilitating nonpharmacologic pain-management techniques, preparing and educating children about their medical care in age-appropriate ways, and communicating the child’s developmental and individual needs and perspective to others. These interventions are most effective when delivered in collaboration with the entire health care team [3].
Child life has been recognized by key regulating health organizations in their support of hospitalized children and their families. In January 2021, the American Academy of Pediatrics (AAP) noted “Child life services contribute to an organization’s efforts to meet the standards set forth by The Joint Commission and other accreditation agencies, including effective communication, patient- and family-centered care, age-specific competencies, and cultural competence.” This policy statement was a significant step forward in the field of child life because as a mostly non-billable service, it demonstrated that these governing bodies saw the essentiality of child life services leading in providing quality pediatric care [3].
Noted in the policy statement were seven recommendations for child life
1. Child life collaboration with the entire interdisciplinary team is essential to meeting the overall health care needs of children and families,
2. Child life services are part of an integrated patient- and family-centered model of care and can be used as a quality measure in the delivery of health care services for children and families,
3. Child life services, provided directly by CCLSs, are recommended in pediatric inpatient units, EDs, chronic care centres, and other diagnostic and treatment areas to the extent appropriate for the population served. In hospitals with a small number of inpatient or outpatient pediatric visits, ongoing consultation with a CCLS is needed to educate health care team members and support developmentally appropriate patient- and family-centered practice,
4. Child life services staffing must be individualized to address the needs of specific inpatient and outpatient areas. The ratio of child life specialist to patient should be adjusted to account for the patient’s medical, psychosocial, and developmental complexity and vulnerability, and family needs and preferences. Child life services need to continuously evolve to meet the changing needs in pediatric health care, including the significant increases in children with disabilities and medical complexity,
5. Child life services optimize pediatric health care and, therefore, should be included in the hospital operating budget; they cannot solely rely on contingency or philanthropic funding,
6. Legislative advocacy of child life services by paediatricians and other stakeholders is recommended at the state and federal levels,
7. Additional research is needed to further identify the impact of child life services on patient care outcomes, including patient experience, cost-effectiveness, and quality and safety measures [3].
Despite the growth the field of child life has seen, child life specialists continue to educate on and advocate for their role and responsibilities as there is still limited awareness. Child life specialists are part of an interdisciplinary, patient- and family-centered model of care, collaborating with the family, physicians, advanced practice providers, nurses, social workers, and other members of the health care team to develop a comprehensive plan of care [3]. Ballard and Lookabaugh noted that while many pediatric healthcare professionals are aware of child life, they may not have a comprehensive understanding of the educational and training requirements, services provided, and the role of child life specialist within the multidisciplinary team [4]. Furthermore, despite the growth of the child life profession, only a few empirical studies have examined the perceptions of the medical team towards child life specialists. Prior research has shown that the collaboration between different healthcare professionals leads to positive outcomes of patients as one cannot be an effective team member within the healthcare field if there is not a shared understanding of one another’s roles [5].
Three studies have examined perceptions of child life professionals [6,7]. Gaynard surveyed a total of 945 health care workers including nursing, social work, physicians, and child life backgrounds throughout 21 hospitals in the north-eastern United States to better understand their perception of the role, status, and power of child life specialists. Within this study, child life specialists frequently reported that a primary role of the profession is to be a member of the healthcare team, but other members of the multidisciplinary team rarely mentioned this as a primary role of child life. Additionally, healthcare members were noted to hold the belief that amusing and entertaining children was a primary role of a child life specialist. This study suggested that the discrepancies among perceptions may be due to members of the multidisciplinary team’s lack of knowledge about the role of child life professionals and that when child life specialists are observed in therapeutic play activities, other health care professionals might misconstrue these support activities as mere entertainment.
Cole et al., completed a partial replication of the Gaynard study to assess the perceptions of child life professionals within the broader health care team by making modifications to the original questionnaire [6]. The authors hypothesized that healthcare team members’ perceptions have changed due to the growth and greater exposure to the child life profession and a greater emphasis placed on cost management. Of the 228 participants of this study, almost 50% noted preparation and orientation as a responsibility of child life. Amuse and entertain remained a commonly reported responsibility, with only a select few participants mentioning being a member of the health care team as a primary responsibility child life [6]. Another area reported minimally for responsibilities was the area of patient support with this study suggesting that other health care professionals may underestimate the importance of CCLSs establishing and maintaining supportive relationships with patients [6].
In 2021 study done by Wittenberg et al. expanded on the previous two studies to examine how healthcare professionals perceive the responsibilities and job tasks of child life specialists through the theoretical framework of interprofessional collaboration [7]. This study found that patient support and patient education were the most identified responsibilities by members of the multidisciplinary team [7]. Patient play, normalization and development, and support and collaboration with staff responsibilities were similar to Gaynards and Cole et al., preparation and orientation, amusement and entertainment, growth and development, and member of healthcare team responsibilities, respectively [6,7].
Existing literature has demonstrated the positive impact child life interventions have on patient and parent perception and satisfaction levels, which are becoming increasingly important for reimbursement, accreditation, marketing, and even public reporting of outcomes [3]. Health care professionals and organizations acknowledge the significant impact child life specialists have on the patient experience as well as the role child life plays in helping the concept of patient experience continue to evolve and grow [3]. With today’s health care practices leaning towards the benefit of empirical evidence when making decisions about everything from institutional goals and initiatives to departmental staffing or budges, it’s crucial that professionals have an intimate knowledge about the evidence that supports their interventions, but also the gaps that require further investigation. The goal of the present study is to support CCLSs to understand how healthcare professionals view the contributions of child life to patient care. This will further allow child life specialists to assess and identify the need to educate others, clarify misconceptions within their teams, and grow in the ability to be effective team members within the multidisciplinary team.
Methodology
Participants
The sample came from clinical staff who work in the emergency and radiology departments at Nemours Children’s Hospital Florida. Eligible roles included nurses, physicians, nurse practitioners, physician’s assistants, paramedics, patient care technicians, radiology technicians, and registration assistants. Participants were required to understand English and be at least 18 years of age. All shifts were included. As of September 2022, 154 staff were considered eligible to participate.
Procedure
This study was approved by the Institutional Review Board of Nemours Children’s Health #1926155 on October 10, 2022. An original electronic survey with 23 questions was developed by researchers using Qualtrics, a survey software which collected the results. The research manager, a nonclinical role, emailed all eligible participants throughout October and November of 2022. Additional paper slips with a QR code for the survey were also provided to all staff members. The survey included an informed consent before moving on to the main survey. Types of questions included demographics, agreement scenarios, ranking, and free response. Results were collected by the Qualtrics software, deidentified by the research manager, and provided to the researchers for analysis. Researchers arranged data into groups and visualized data as appropriate. Free-response answers were analysed using content analysis and themes were developed using the “Cutting and Sorting” technique [8].
Results
Out of 154 eligible staff members, 89 participated in the survey, yielding a response rate of 56%.34), radiology technologists (n=23), emergency physicians (n=10), paramedics (n=7), registration assistants (n=4), patient care technicians (n=1), nurse practioners (n=2), and physician’s assistant (n=1), within the emergency department and radiology departments. A total of 57 emergency department staff and 29 radiology staff completed the survey. There was a total of 62 female participants and 25 male participants with 83 being full time and 4 being part time. From day shift (7a-7p) there were 48 participants, 19 from mid shift (11a-11p), 12 from night shift (7p-7a), and 3 weekends only. Finally, the years employed at the hospital varied from more than 5 years (n=27), less than 1 year (n=25), 1-3 years (n=18), and 2-3 years (n=17).
Staff Perceptions on Child Life
Staff were first asked to rate their level of agreement on a 4-point scale (strongly disagree to strongly agree) with the statement “Child life specialists are an important part of the health care team.” A total of 75 of the 87 respondents selected “strongly agree” for this statement, with 7 respondents selecting “somewhat/strongly disagree.” When prompted to list one word or phrase they would use to describe the role of child life, there were 62 total responses in which content analysis revealed that the top two categories including the words “essential,” “vital,” and “important” were noted a total of 21 times, “amazing” and “awesome” were counted 11 times, while “supportive” and “helpful” were noted 10 times.
Participants were then presented with a free text question to explain or list the specific roles they felt a child life specialist typically engages in for their patients. Content analysis of the 64 total responses revealed 3 primary categories: (a) procedural preparation and distraction/support, (b) calming and easing anxiety, and (c) bridging the gap between the clinical team and families. Staff were later prompted to rank from 1-10, with 1 being the most important and 10 being the least important, the following in terms of child life responsibilities: playing with patients and/or providing toys and activities, procedural support, education (procedures and diagnosis teaching), family-centered care, nonpharmacologic pain management, bereavement support, donations and special events, supervising child life interns and volunteers, participating in department, unit and hospital-wide committees, and completing developmental and stress potential assessments. In the ED, the top 3 perceived responsibilities noted were procedural support, education and preparation, and nonpharmacological pain management. In radiology, the top 3 perceived responsibilities noted were education and preparation, procedural support, and providing toys/playing with patients

Figure 1: ED Graph
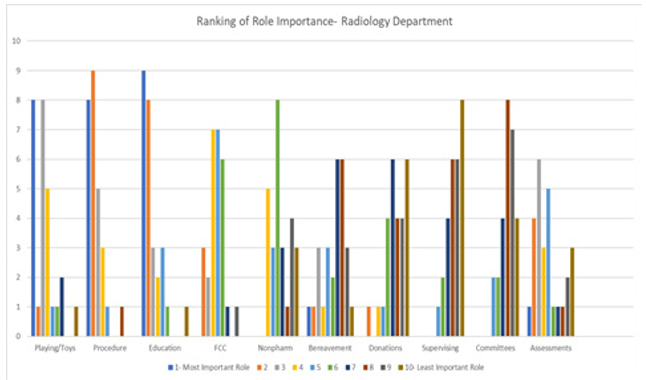
Figure 2: Rad Graph
Staff were then prompted with a 6-point rating scale (significantly negative, somewhat negative, neutral, somewhat positive, significantly positive, and not observed) to rate the level of impact child life has had on their patients and families in the following areas: overall quality of life, procedural support, procedural preparation, compliance with treatment plan, non-pharmacologic pain management, opportunities for expressing needs/concerns, opportunities for dealing with stress/anxiety, sibling support, sensory needs/difficulties, parents coping with hospitalization and stressors, developmentally appropriate play, end of life care, and special events/donations. The top three areas which saw the most positive effect were procedural support, procedural preparation, and easing stress and anxiety. The area that was rated as the least significant was end of life care. Finally, participants were able to write about the use of and/or role of child life in their units. Content analysis of these responses showed an overwhelming agreement amongst staff that more child life support/increased staffing is needed in both the emergency department and radiology.
Discussion
This study sought to understand the perspectives of the multidisciplinary team on the benefit of utilizing child life services of the researcher’s hospital. Most participants showed agreement that child life is a valued and important part of the healthcare team. When asked how it would impact the overall healthcare experience for patients and families if child life did not exist, 87% of staff indicated that it would negatively impact the healthcare experience. This could be due to the fact the child life specialists often have many roles and responsibilities when providing when providing care to the family system. The three previous studies on perceptions of child life specialists all found similar categories of patient education, play and normalization, and multidisciplinary collaboration [6,7]. Like Wittenberg and Barnhart, our study analysis also did not find the theme of advocacy as noted in the two previous studies [7].
There could be two potential reasons for this, 1) patient advocacy is inherent to all the work of a child life specialist, or 2) healthcare professionals may not view this as a core responsibility. With end-of-life care being ranked of least importance, one can infer that because it’s rarely seen in the emergency department and radiology, staff would not be as familiar with it.
Staff had slightly different perceptions when asked how the direct patient care they specifically provided if child life did not exist. Eighty-three percent of respondents noted there would be a somewhat to significant impact on their direct care provided. Within the ER and radiology units, a singular child life specialist physically cannot be present for all procedures and psychosocial needs, which is why there is always a need for more adequate staffing of child life specialists. Therefore, the multidisciplinary team often must provide quality care without the support of a child life specialist. Our findings may be influenced by the many behind-the-scenes tasks that pull us away from direct patient care like documentation, committee work, and student supervision, as they may not be seen as important or necessary responsibilities. Other important responsibilities of CCLSs, such as acquiring resources or writing assessments and documentation, may be overlooked as they are not seen as providing typical direct patient care.
An eighty-two percent level of agreement was found as staff noted that having a child life specialist present enhances the multidisciplinary team’s ability to complete procedures successfully. Procedural preparation and support ranked highest on the importance of child life responsibilities in units where child life services cannot be universally offered to patients and families.
This continues to add to the existing literature that child life’s impact on procedures should be of key focus in the research. In a 2018 study on the impact of child life on pain and distress in the emergency department, Cistal et al., noted that preparation and procedural support provided by a CCLS reduced the observed and perceived distress for children undergoing PIV placement. Research has shown that children who receive preparation and support prior to and after a procedure often experience less anxiety, increased knowledge, and enhanced coping, which results in a better experience for parents, staff, and patients [9]. With both units ranking procedural education and support in their top three responsibilities, it can be inferred that the ER and radiology staff witness this benefit to patient coping and understanding.
Staff further noted that they felt patients would definitely or probably not (56%) receive the same quality of prep and support if provided by a non-CLS. Due to the educational emphasis placed on human growth and development and psychology, child life specialists are uniquely able to address patient fears through individualized and developmentally appropriate procedural preparation and support based on developmental level, coping style, and other situational factors [3]. The American Academy of Pediatrics notes that while other members of the healthcare team share in these responsibilities for the psychosocial concerns of the child and family, this is the primary role for child life specialists [3]. However, this rating may bring light to the larger point that staff may feel confident in providing support without a CCLS due to the perceived inadequate staffing. In-services about how staff can provide support on their own may be required for units with limited presence of child life.
Limitations
While there have been only three previous studies on staff perceptions of child life specialists, there have not been any that were singularly focused on specific units within the hospital. While this study aimed to address these areas, we did experience several limitations. The study was limited to participants from only one pediatric hospital in the Central Florida area. The sample size constituted another limitation with just over half of the identified and eligible 154 staff members completing the survey. Also, not all staff are experienced in working with a child life specialist due to their schedule. As this was a survey that was sent out via email, the response rate be a result of staff having email fatigue and/or not having time to check their emails consistently due to high patient caseloads. As we are unaware of how those who did not respond might differ than those who did, caution should then be used in generalizing the results of this study.
Implications for Future Research
With the expansion of the field, it is essential to understand the perceptions of child life specialists from those who are making the financial decisions. Given the changes in healthcare as a business, particularly those focusing on cost management, it is important to understand the roles and responsibilities of child life specialists as not that of a supplemental team member. Similar surveys should be administered within hospitals of the same health system to improve equity and quality of care as these systems have similar standards of practice and organizational goals.
Conclusion
A majority of participants indicated they wanted an increase in the presence of child life in their units. While participants felt that child life was adequately meeting the needs of their unit, the free text answers and final study comments all echoed the wish to have child life coverage on nights, weekends, and having more than one providing coverage to be able to support more children and families. It’s clear that child life specialists are essential and invaluable members of the healthcare team, but the lack of knowledge of the field of child life has caused child life specialists to be viewed supplementary team members when compared with other health care professionals. As the role of child life specialists continues to evolve in parallel with the appreciation and integration of psychosocial care, it is crucial that those in the field of child life are aware of how others health care team members view them. Only then will they be able to address these perceptions and support other professionals in gaining a better understanding of the value and goals of the child life team [10].
References
- Bajoghli, M., Bajoghli, F., Tayari, N., & Rouzbahani, R. (2010). Children, CT scan and radiation. International Journal of Preventive Medicine, 1(4), 220.
- Association of Child Life Professionals. (2023). The Child Life Profession. Childlife.org.
- Romito, B., Jewell, J., Jackson, M., Ernst, K., Hill, V., Hsu, B., ... & Vinocur, C. (2021). Child life services. Pediatrics, 147(1).
- Lookabaugh, S., & Ballard, S. M. (2018). The scope and future direction of child life. Journal of Child and Family Studies, 27, 1721-1731.
- Zwarenstein, M., Goldman, J., & Reeves, S. (2009). Interprofessional collaboration: effects of practiceâ?based interventions on professional practice and healthcare outcomes. Cochrane database of systematic reviews, (3).
- Cole, W., Diener, M., Wright, C., & Gaynard, L. (2001). Health care professionals' perceptions of child life specialists. Children's Health Care, 30(1), 1-15.
- Wittenberg, B. M., & Barnhart, D. (2021). How are Certified Child Life Specialists perceived by healthcare professionals: a call for interprofessional collaboration. Journal of Interprofessional Care, 1-9.
- Sanchez Cristal, N., Staab, J., Chatham, R., Ryan, S., Mcnair, B., & Grubenhoff, J. A. (2018). Child life reduces distress and pain and improves family satisfaction in the pediatric emergency department. Clinical pediatrics, 57(13), 1567-1575.
- Kinnebrew, S. L., Dove, C. G., Midwin, C. M., Olson, T. M., & Guimaraes, C. V. (2020). The role of child life in pediatric radiology. Pediatric Radiology, 50, 1509-1513.
- National Center for Health Statistics (US. (2023). Health, United States, 2020-2021.