
International Journal of Preventive Medicine and Care(IJPMC)
ISSN: 2994-032X | DOI: 10.33140/IJPMC

Research Article - (2025) Volume 3, Issue 2
Mortality Results Based on Antimicrobial Resistance and HIV Status in a Low-Income Developing Country. A Monocentric Ambispective Study
Received Date: Dec 11, 2024 / Accepted Date: Jan 17, 2025 / Published Date: Sep 09, 2025
Copyright: ©©2025 Kick Kayembe Kakese, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Kakese, K. K., Ka, D., Cisse, M. V., Wembulua, B., Botalema, F. (2025). Mortality Results Based on Antimicrobial Resistance and HIV Status in a Low-Income Developing Country. A Monocentric Ambispective Study. Int J Prev Med Care, 3(2), 01-05.
Abstract
Multi-resistant bacteria represent a major public health problem throughout the world in general, and in sub-Saharan Africa in particular (1). Many patients admitted with infectious diseases are carriers of bacteria, some of which are multi- drug resistant, but only a few studies have been carried out to determine the factors that could influence the outcome of patients in hospital (2).
Besides, Previous studies have estimated the number of deaths associated with drug- resistant infections and sepsis and found that infections remain a leading cause of death globally (3).
The study assesses the impact of immune status on mortality associated with multi- drug resistant bacterial infections. This ambispective observational study was conducted from the 1st of January 2021 to the 31st of December 2022. The patients included during this period were adults admitted to hospital regardless of their HIV status, with a multi-drug resistant bacterial infection confirmed after culture and antibiotic susceptibility testing. The criteria for assessment were the occurrence of death and, consequently, the identification of factors associated with this mortality.
During the study period, 200 patients were included: 81 with positive HIV serology and 119 with negative serology. Considering the 2 groups according to their serological status, overall mortality was 20.17% in the HIV-negative group and 23.46% in the HIV-positive group, with no significant difference between the 2 groups (p-value: 0.6). On the other hand, co- infections and/or opportunistic infections accounted for a 2.82-fold increase in the risk of death in the HIV-positive group compared with the reference group (OR=2.82 [1.14-7.52] and p-value: 0.029).
HIV infection itself does not appear to have a direct impact on mortality associated with resistant bacterial infections, but factors associated with infection may contribute to an increased risk of mortality.
Keywords
Multi-Resistant Bacteria, HIV, Risk Factors, Mortality
Introduction
The problem of multi-resistant bacteria is global, and the cause of hundreds of thousands of deaths every year [4]. Globally, antibiotic-resistant bacterial infections are on the rise and were responsible for the deaths of more than 1.2 million people in 2019 [5].
In addition, research estimates that around 5 million deaths in 2019 were associated with bacterial antimicrobial resistance [6]. On a financial level, modelling studies predict human losses estimated at 10 million per year worldwide, with an impact on resources representing more than 100 billion dollars by 2050 if no appropriate measures are taken regarding bacterial resistance to antibiotics [7].
Immunosuppressive factors such as HIV infection represent a risk of bacteraemia, which is generally associated with an increased mortality rate [8]. Mortality linked to HIV infection is higher in sub-Saharan Africa, and in the absence of treatment, the following causes are mainly found: tuberculosis, serious bacterial infections, cryptococcosis, mainly neuromeningeal, and cancers such as Kaposi's sarcoma and lymphoma [9].
Inappropriate antibiotic prescription is also a major factor in the emergence of resistance. It has been hypothesised that people living with HIV are at greater risk of receiving inappropriate antibiotics for acute respiratory infections, because they are at high risk of mortality [10].
It should also be noted that environmental animal reservoirs of resistance are having a growing impact in resource-limited countries [11].
In addition, there are limited data between HIV infection and bacterial Antimicrobial Resistance, and to our knowledge this had never been reviewed systematically until 2021 in African Low/Middle income countries [12]. We analyzed data from patients hospitalized with a resistant bacterial infection, with known HIV-related immune status, to identify the impact of the serological status related to the infection on the overall mortality recorded during the study period; but also, to describe the epidemiological characteristics of the hospitalized patients and to evaluate the bacterial isolates found as well as the phenotypes of resistance.
Materials and Methods
Framework and Conception of the Study
We conducted a monocentric, ambispective observational study in the infectious and tropical diseases department (SMIT) of the Fann National University Hospital in Dakar, Senegal, over the period from the 1st of January 2021 to the 31st of December 2022. Patients were included successively according to their date of admission. This included men and women aged 18 or above, with positive and negative HIV serology, hospitalized for at least 48 hours with q-SOFA greater than or equal to 2 or with at least one of the following danger signs: Fever ≥ 38°C or hypothermia < 36°C, respiratory rate > 22 cycles, oxygen saturation < 90%, heart rate > 120/minutes, systolic BP < 100 mmHg, inability to walk unassisted or Glasgow Scale < 15 or any other pathological neurological manifestation. In addition, all the patients included in the study had a cytobacteriological pathological examination carried out in the CHNU Fann laboratory or in a partner laboratory. Patients with cytobacteriological results of colonization were not included in the study. Patients with tuberculosis, including multi-resistant tuberculosis, were also not included in the study. It should be noted that the data were obtained following informed consent signed by each patient or their legal representative.
Study Sample Size
Patients meeting the inclusion criteria were included comprehensively during the study period.
Data Collection
The data was collected from records of requests for analyses in the hospital bacteriology laboratory and also from patient records during the retrospective period of the study. From the 1st of August to the 31st of December, the data was collected from the collection forms filled in at the request of the laboratory analyses and subsequently completed once the results had been obtained. They were then recorded in a password-protected Excel spreadsheet containing various parameters required for the statistical analysis of the data collected (socio-demographic parameters including age and sex, clinico-biological parameters including HIV status, CD4 count or presence of opportunistic infections or co-infections for HIV-positive patients, as well as bacteriological parameters including bacterial isolates or resistance phenotype).
Statistical Analysis
The analysis was carried out using R software version 4.2.2. Categorical variables were described in terms of relative and absolute frequencies, while quantitative variables were presented in terms of mean ± standard deviation or median depending on the type of distribution.
The factors associated with the lethality of bacterial resistant infections were first evaluated in a bivariate analysis, using Fisher's exact test, and the variables with p<20 were then introduced into a multivariate model using logistic regression.
Results
We collected 200 cases of bacterial infections in patients hospitalised during this period, 48.5% of whom were women. The median age was 46, and the most frequent age group was between 30 and 50 (35.48%).

There were 81 seropositive samples (40.50%) and 119 seronegative samples (59,50 %).
|
Characteristics |
Non-deceased = 157 |
Deceased = 43 |
|
HIV status |
|
|
|
Negative |
97 [79,83%] |
24[20,17%] |
|
Positive |
62[76,54%] |
19[23,46%] |
Table 1: Distribution of death cases according to HIV serology, SMIT CHNU de Fann, from 1 January 2021 to 31 December 2022 (n=200)
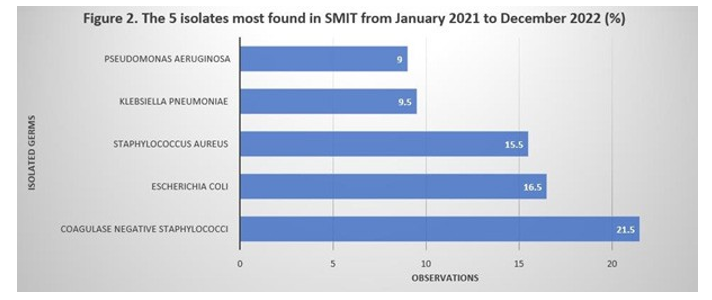
The 5 most frequent germs were: coagulase-negative staphylococci (21.50%), Escherichia coli (16.50%), Staphylococcus aureus (15.5%), Klebsiella pneumoniae (9.50%) and Pseudomonas aeruginosa (9,00%).
In terms of sensitivity to antibiotics, the rates of resistance to methicillin for coagulase- negative staphylococci and staphylococci aureus were 80.43% (37/46) and 58.00% (18/31) respectively. ESBL-producing bacteria were mainly Enterobacteriaceae and were represented by Klebsiella pneumoniae 62.50% (15/24), Escherichia coli 57.57% (19/33), Enterobacter spp 70.00% (7/10) and Proteus mirabilis 100% (3/3). The carbapenemase-producing strains were Escherichia coli 50.00% (3/6), Klebsiella Pneumoniae 33.33% (2/6) and Xanthomonas spp 16.66% (1/6). We found no association between HIV status and the number of deaths recorded (p> 0,05).
|
Characteristics |
Non-deceased = 157 |
Deceased = 43 |
P-value |
|
HIV status |
|
|
0.6 |
|
Negative |
97 [79,83%] |
24[20,17%] |
|
|
Positive |
62[76,54%] |
19[23,46%] |
|
Table 2: Distribution of Death Cases According to HIV Serology, SMIT CHNU de Fann, from 1 January 2021 to 21 December 2022 (n=200
After the multiple variable analysis, only co-infections and/or opportunistic infections were associated with the risk of death (OR= 2,82 [1,14-7,52]).
|
Characteristics |
OR |
95% IC |
P-Value |
|
Coinfection-opportunistic infection |
|
|
|
|
No |
- |
- |
|
|
Yes |
2.82 |
1.14-7.52 |
0.029 |
Table 3: Distribution of Cases of Death According to Coinfections and/or Opportunistic Infections, Smit Chnu De Fann, From 1 January 2021 To 31 December 2022 (N=200)
The final results of this study show the need for ongoing monitoring of antibacterial resistance, but also the need to consider the diseases associated with bacterial infections, particularly in people living with HIV, and finally the importance of appropriate antibacterial therapy based on monitoring.
Discussion
Overall lethality linked to resistant bacterial infections was one of the main criteria assessed in our study (43 out of 157, i.e. 27, 39%-->results). The various variables analyzed, i.e. socio- demographic parameters, HIV serological status, germ species and bacterial resistance phenotypes, failed to demonstrate an increase in the risk of mortality linked to resistant bacterial infections. However, there was a significant increase in mortality in HIV-positive patients who were hospitalized with at least one opportunistic infection or co-infection, after multivariate analysis of the different variables (p-value: 0,029).
Few comparative studies have been carried out on the impact of resistant bacterial infections in relation to HIV serological status. However, Sabrina Sabino et al, in a cohort study evaluating mortality within the first 30 days of hospitalization for sepsis due to bacterial infections linked to Carbapenem-resistant Enterobacteriaceae, demonstrated a significant association with HIV-positive status, but also with other factors such as advanced age, cirrhosis and septic shock [13].
Furthermore, in a study designed to assess the usefulness of the qSOFA (quick Sepsis- related Organ Failure Assessment) score in predicting the risk of mortality in hospitalized and emergency care patients in sub-Saharan Africa, Adam R. Aluisio et al were unable to identify a statistically significant difference in mortality in PLHIV compared with the general population, despite an increase in mortality in patients with high qSOFA [14].
These results contrast with the lack of evidence of an association between HIV-positive serological status and increased mortality from resistant bacterial infections demonstrated by M.A Vandenhende P.Blanc et al, who found a similarity in the percentage of resistance between people living with HIV and the general population, in a study of antibiotic resistance profiles and changes over time, particularly in infections with Staphylococcus aureus, pneumococci and enterobacteria [15].
These findings suggest that the same recommendations should be applied to people living with HIV as to the general population, particularly in terms of monitoring, but also in terms of specific care, including the proper use of antibiotics, regardless of HIV status. The study collected data over 2 years, retrospectively and then prospectively, including all eligible hospitalized patients, with the possibility of monitoring their progress during the prospective phase and readjusting the treatment if necessary.
The main limitations of our study were, on the one hand, the very low number of CD4 counts available, which prevented us from looking for an association between increased mortality and HIV-positive serological status, according to the level of immunodeficiency.
On the other hand, as most of the data was collected retrospectively, insufficient information in patient files or registers meant that a certain number of patients could not be included in the study. Furthermore, as the presence of an opportunistic infection or co- infection was considered to be a dichotomous variable, it was not possible to carry out a detailed analysis of the impact of different co-infections and/or opportunistic infections.
Conclusion
This prospective study enabled us to assess the role of HIV serostatus on the impact of multidrug-resistant bacterial infections, mainly in terms of mortality. The percentage of deaths and the analysis of the data for an association between serostatus and mortality show a similarity between people living with HIV and the general population. However, the presence of opportunistic infections or co-infections in HIV-positive patients is a risk factor for higher mortality. Consequently, it is important to emphasise the need for special monitoring of patients with resistant bacterial infections, and particularly those with a positive serological status presenting with an opportunistic infection and/or co- infection. In addition to this, a more in-depth study of immunodeficiency factors, in particular CD4 counts, should be carried out to investigate the link with a possible increase in mortality in patients with resistant bacterial infections.
References
- Aruhomukama, D., & Nakabuye, H. (2023). Investigating the evolution and predicting the future outlook of antimicrobial resistance in sub-saharan Africa using phenotypic data for Klebsiella pneumoniae: a 12-year analysis. BMC microbiology, 23(1), 214.
- Fongang, H., Mbaveng, A. T., & Kuete, V. (2023). Global burden of bacterial infections and drug resistance. In Advances in Botanical Research (Vol. 106, pp. 1-20). Academic Press.
- Ikuta, K. S., Swetschinski, L. R., Aguilar, G. R., Sharara, F., Mestrovic, T., Gray, A. P., ... & Dhingra, S. (2022). Global mortality associated with 33 bacterial pathogens in 2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet, 400(10369), 2221-2248.
- Laxminarayan, R. (2022). The overlooked pandemic of antimicrobial resistance. The Lancet, 399(10325), 606-607.
- Zhang, C., Fu, X., Liu, Y., Zhao, H., & Wang, G. (2024). Burden of infectious diseases and bacterial antimicrobial resistance in China: a systematic analysis for the global burden of disease study 2019. The Lancet Regional Health– Western Pacific, 43.
- Dadgostar, P. (2019). Antimicrobial resistance: implications and costs. Infection and drug resistance, 3903-3910.
- Chokshi, A., Sifri, Z., Cennimo, D., & Horng, H. (2019). Global contributors to antibiotic resistance. Journal of global infectious diseases, 11(1), 36-42.
- Jenson, A., Rao, A., Mda, P., Cawe, B., Iruedo, J., Dubula, T., ... & Hansoti, B. (2021). One in four die from acute infectious illness in an emergency department in Eastern Cape Province, South Africa. South African Medical Journal, 111(2), 129-136.
- World Health Organisation (2023). HIV and AIDS. WHO, July 13 [Google scholar]
- Keintz, M. R., Abbas, A., Lyden, E., Ma, J., Bares, S. H., Van Schooneveld, T. C., & Marcelin, J. R. (2022, July). Antibiotic prescribing for acute respiratory illnesses in persons with HIV compared with persons without HIV. In Open Forum Infectious Diseases (Vol. 9, No. 7, p. ofac218). Oxford University Press.
- Nadimpalli, M., Delarocque-Astagneau, E., Love, D. C., Price, L. B., Huynh, B. T., Collard, J. M., ... & Guillemot, D. (2018). Combating global antibiotic resistance: emerging one health concerns in lower-and middle-income countries. Clinical infectious diseases, 66(6), 963-969.
- Olaru, I. D., Tacconelli, E., Yeung, S., Ferrand, R. A., Stabler, R. A., Hopkins, H., ... & Kranzer, K. (2021). The association between antimicrobial resistance and HIV infection: a systematic review and meta-analysis. Clinical Microbiology and Infection, 27(6), 846-853.
- Sabino, S., Soares, S., Ramos, F., Moretti, M., Zavascki, A. P., & Rigatto, M. H. (2019). A cohort study of the impact of carbapenem-resistant Enterobacteriaceae infections on mortality of patients presenting with sepsis. MSphere, 4(2), 10-1128.
- Aluisio, A. R., Garbern, S., Wiskel, T., Mutabazi, Z. A., Umuhire, O., Ch'ng, C. C., ... & Levine, A. C. (2018). Mortality outcomes based on ED qSOFA score and HIV status in a developing low-income country. The American journal of emergency medicine, 36(11), 2010-2019.
- Vandenhende, M. A., Blanc, P., Bessede, E., Meriglier, E., Leleux, O., Cazanave, C., ... & Bonnet, F. (2021). Infections bactériennes chez les patients infectés par le VIH: Profil de résistance aux antibiotiques et évolution au cours du temps. La Revue de Médecine Interne, 42, A34.