
Archives of Clinical and Medical Microbiology(ACMMJ)
ISSN: 2835-9968 | DOI: 10.33140/ACMMJ
Impact Factor: 1.0

Research Article - (2025) Volume 4, Issue 1
Molecular and Microscopy Evaluation of Lymphatic Filariasis in Ilorin Metropolis, Kwara State Nigeria
Received Date: Jan 17, 2025 / Accepted Date: Feb 14, 2025 / Published Date: Feb 20, 2025
Copyright: ©©2025 Prosper Omah, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Omah, P., Nmorsi, O. P. G., Egwunyenga, A. O. (2025). Molecular and Microscopy Evaluation of Lymphatic filariasis in Ilorin Metropolis, Kwara State Nigeria. Archives Clin Med Microbiol, 4(1), 01-09.
Abstract
Background: Lymphatic filariasis is widespread and a major public health problem in many developing countries with warm and humid climate and it is one of the most prevalent neglected tropical diseases. This study, evaluated the diagnostics performance of molecular and conventional microscopy method of Lymphatic filariasis in Ilorin Metropolis, Kwara State Nigeria.
Methods: Genomic DNA was collected from 45 human blood samples obtained from Ilorin, Kwara State. They were then amplified by PCR and detected through gel electrophoresis. The PCR products were purified with QIAquick PCR purification kit (Qiagen, Valencia, CA) and then DNA quantified for Sanger sequencing, Bio Edit Software were used for sequence alignment and editing. 37 sequences were selected for analysis by MEGA X software to access the evolutionary connection of W. bancrofti isolates.
Results: 37 (82.2%) PCR products were positive for W. bancrofti and 16 (35.6%) were Positive for Microscopy. Hence, the sensitivity of PCR (82.2%) while the specificity was (64.4%).With the microscopy, the chances of a negative samples turning out positive by PCR, also known as the positive predictive value (PPV) was (69.8%) while the chances of being picked as truly negative predictive value was (78.4%). In assessing the level of agreement show that microscopy has a weak agreement, Kappa index statistics (0.46) with molecular techniques 95% CI,0.2-0.4).
Conclusion: Since Polymerase Chain Reaction showed higher sensitivity (82.2%) as positive predictive value, it is therefore recommended to include PCR as complementary routine diagnosis for lymphatic filariasis especially subclinical cases due to W. bancrofti despite its relatively higher cost.
Keywords
Lymphatic Filariasis, Microfilaria, Blood Smear, Microscopy, Polymerase Chain Reaction
Abbreviations
PCR-Polymerase Chain Reaction. DNA-Deoxyiribonucleic Acid. LF-Lymphatic Filariasis. USA-United States American. ELISA- Enzyme Linked Immuno Absorbant Assay. MDA-Mass Drug Administration. DALY-Disability Adjusted Life Years. MOH- Ministry of Health. WHO-World Health Organization PPV- Positive Predictive Value. NPV Negative Predictive Value.
Introduction
Lymphatic filariasis (LF) is widespread and a major public health problem in many developing countries with warm and humid climate and it is one of the most prevalent neglected tropical diseases. Wuchereria bancrofti is the most prevalent cause of lymphatic filariasis cases in the world . The World Health Organization (WHO) considers lymphatic filariasis (LF) as the second leading cause of physical disability worldwide. An estimated 120 million people in 73 countries are currently infected, while 40 million people have chronic signs like hydrocele and elephantiasis [1]. Lymphatic filariasis is widespread in sub-Saharan Africa and particularly high endemicity is seen along the coast of the Indian Ocean and in areas adjacent to the great lakes [2].Current estimates suggest that more than one billion people live in endemic areas and are at risk of infection, and more than one third of these are in Sub Saharan Africa [3].
Lymphatic filariasis, resulting from infection with the mosquito- borne filarial nematode Wuchereria bancrofti, is a disfiguring disabling disease [4]. The parasites are transmitted from one host to another through the bites of infected mosquitoes which could be of different genera; Culex, Aedes, Mansonia and Anopheles [5-7]. The disorderly growth of the metropolis, the significant increase in the number of substandard housing and the parlous sewage disposal conditions favors proliferation of the vector mosquitoes and consequently transmission of the endemic diseases in the Africa region [8]. Therefore an intervention model for the control of lymphatic filariasis should consider the social organization of urban space by identifying micro areas of risk and priority population groups at risk of acquiring the parasites [8-9]. Lymphatic filariasisis has thus been ranked the second most common cause of long term disability after mental illness [WHO,2017]. Lymphatic filariasisis results in loss of work, productivity, direct and indirect economic loss and functional impairment,In Africa ,the disease is endemic in 34 countries [Nosrat ,2021] [10-12].
Nigeria has the greatest number of people infected or at risk with lymphatic filariasis (80-121 million), among all the African nations [Ugboimoko et al,2010] [4]. Lymphatic Filariasis affect many communities in Ilorin metropolis, neighboring villages especially local farmers causing illness and disfiguring that prevent people from attendance at school and farming [6]. Most of the current diagnosis is based on the parasitological microscopy gold standard. Subclinical cases may be misdiagnosed using this techniques. This study is aimed to evaluate and compare the diagnostic performance of parasitological techniques and molecular technique using Real Time Polymerase Chain Reaction, (RT-PCR) for Lymphatic filariasis in our study area.
Materials and Methods
Study Area and Design
The study was conducted in Ilorin , Kwara State. Ilorin is located approximately on latitude 8º30’ and 8º50’ North of the equator and longitude 4º20’ and 4º35’East of the Greenwich meridian. Ilorin is the gateway city between the southern and northern Nigeria with an approximate land area of 100kilometres .Ilorin has wet and dry season. The climate of the city is humid tropical under the influence of the two trade winds prevailing over the country, characterized with high temperature throughout the year [13]. The daily average temperatures range change between September 22.5º to January 25 ºC. The mean annual rainfall is 1,200mm. The mean annual total rainfall is 1200m’The temperature in Ilorin is uniformly high throughout the year. Ilorin metropolis is currently about 974,000 ranking 6th largest city in Nigeria. The climate of Ilorin is characterized by both wet and dry seasons. The rainy season begins towards the end of April and last till October while the dry season begins in November and end in April. The pattern of drainage system of Ilorin is dendritic. Asa River occupies a fairly valley and goes a long way to divide Ilorin into two parts: namely the Eastern and Western part. The wet season is between May and October with two peak periods in June and September while the dry season spans between November and April.


Figure 1: Map of Kwara State, Showing the Study Area
Ethical Consideration
The ethical approved was obtained from Kwara State Ministry of Health Ethical Committee (MOH/KS//EU//777/354) before the commencement of the study The sample collection meeting was held with traditional leaders, teachers and communities members.
Inform written consent was obtained from the volunteers, each adult subject and parents / guardian of each child during the study following the objectives of the study .Inventory of the volunteers were recorded for the study Right to refuse and withdraw were explained to the participant. The major inclusion criteria were presence of rashes, lymphedema and fever.
Study Subject and Population
The subject were 45 blood samples for molecular and microscopy comparisons The study was carried out between July, 2022 and August 2023 which spanned throughout the dry and rainy season.
Sampling Procedure and Examination
Laboratory Analyses
Microscopy Examination
Whole blood samples were obtained by vein puncture at mid night and were submitted for microscopy in which laboratory DNA extraction, RT-PCR and sequences analysis laboratory blood filtration and microscopic evaluation of lymphatic filariasis due to W.bancrofti were performed by using 1ml of coagulated blood as described previously [Martindala et al,2024] using thick blood film why Meyer’s haematoxylin was examined microscopically and the level of microfilaeria documented [Nosrat,2021].
DNA Extraction from human blood samples
DNA from human blood samples was extracted using the alcohol precipitation 200μl of blood was added in to labeled 1.5ml eppendorf tubes and 400μl of sodium hydroxide with 1% triton was added. The mixture was heated at 65oCfor 30 minutes in a Thermomixer (Thermo Fisher) with continues shaking and quickly cooled on ice. Using a PH meter, the pH was adjusted to 8 for optimal performance of the Taq Polymerase during amplification. The DNA was centrifuged at 1400rpm, 4oC for 5 minutes and the supernatant transferred to a new eppendorf tube. Eight hundred (800) µl of absolute ethanol (98%) was added, vortexed and incubated overnight at - 80oC. The DNA was then washed thrice with 70% alcohol, dried and 50µl Tris-EDTA (TE) buffer added and stored at -20oc until amplification was performed.
Detection of W. Bancrofti Using PCR
PCR assays for detection of W. bancrofti were performed based on the sequence of the SspI repeat a pair of primers (NV-1and- NV2) were designed or PCR amplification of the SspI repeat The target primers to amplify the DNA repeat was as follows for for- ward and reverse primers:NVi:5CGTGATGGCATCAAAGTAG- CG3'; NV2:5CCCTCACTTACCATAAGACAAC3 [Martindala et al.2014] [14]. The PCR products after amplification and detec- tion by gel electrophoresis of W. bancrofti product size was 188bp against 100bp Molecular Ladder for the SspI repeat sequence.
DNA Purification And Sequencing
After identifying positive PCR product samples ( samples with the band of interest) from gel electrophoresis, the PCR products were purified with QIAquick PCR purification kit (Qiagen, Valencia, CA). After purification, gel electrophoresis was performed to check if the PCR products were present after purification. Sequencing PCR was performed in a Thermo Cycler using the purified amplicons, a single sequencing primer and a sequencing master mix The BigDye® Terminator v3.1 Cycle Sequencing Kits (Applied Bio systems, Foster City, CA). The sequencing protocol included one cycle of one minute at 95 °C followed with 50 cycles of 10 seconds of denaturation at 96 ° C, 5 seconds of annealing at 50 °C and 4 minutes of elongation at 60 °C and then a holding cycle at 4 °C. Then the Sequencing products were purified using Centri-SepTM spin columns (Princeton Separations, Inc New Jersey, USA). Followed by separation on a capillary ABI Prism 3 500 Genetic Analyzer (Applied Biosystems, Foster city, CA). The machine generates nucleotide sequence chromatograms that were obtained as ABI files format which were assembled and edited using sequence Scanner V1.0 (Applied Biosystems, Foster city, CA). Generated nucleotide sequences were edited by BioEdit® software and used in construction of a phylogenetic tree with the aid of MEGA 6.0® using the neighbor-joining method employing the Kimura-2 parameter [15-16]. Phylogenetic analysis of obtained W. bancrofti Ssp 1 repeat sequences was 1 using the Kimura-2 parameter as implemented in MEGA 6.0. Phylogeny was inferred following 1000 bootstrap replication and reverse sequences were generated using the Bio Edit computer software.
Phylogenetic Analysis Of Ssp 1
MEGA X software was employed to access the evolutionary phylogenicity of W. bancrofti isolates from Ilorin metropolis . BLAST analysis on NCBI with the accession numbers LM12035 ,sequences of Ssp 1 gene in W. bancroftil using the technique developed by The evolutionary history and distances between pairs of sequences were deduced using the neighbor joining methods algorithms [16]. The branch of phylogenetic tree was statistically evaluated using a bootstrap of 1000 replication. BLAST was used to searched Genbank nucleotides data base homogeneous gene sequences to compare with the NCBI.
Statistical Analysis
Except sequencing all other data were analyzed using statistical package for social science (SPSS) version 21.0 (SPSS Inc. Chicago). The performance of each diagnostic test was calculated by means of specificity and sensitivity using positive predictive value and negative predictive value. To validate its measured by sensitivity and specificity they are best illustrated using a conventional two by two (2x2) table. MEGA X software was employed to access the evolutionary connection of W. bancrofti isolates Kappa's statistics index was used to test the level of agreement between microscopic and PCR. P< 0.05 was considered statistical significant.
Results
Prevalence of Diagonistic Performance of Pcr In Relation To Microscopy
Out of 45 blood sample examined for lymphatic filariasis due to W. bancrofti from the metropolis for molecular (PCR) and microscopy 37 (82.2%) were positive for PCR and 16 (35.6%) were Positive for Microscopy as shown in table1
|
Diagnostic test |
No Examine |
Positive No(%) |
Negative No(%) |
|
PCR |
45 |
37 (82.2) |
8 (17.8) |
|
Microscopy |
45 |
16 (35.6) |
29 (64.4) |
|
total |
90 |
53(58.9) |
37 (41.1) |
Table 1: Comparison And Agreement Between Result Detected By Pcr And Microscopy
PCR Sensitivity And Specificity
W .bancrofti isolates were subjected to MEGA X software to access their evolutionary phylogenicity relationship. The sensitivity of PCR was (82.2%) while the specificity was (64.4%).With the microscopy, the chances of a negative samples turning out positive by PCR, also known as the positive predictive value (PPV) was (69.8%) while the chances of being picked as truly negative predictive value was (78.4%). In assessing the level of agreement using microscopy as gold standard show that microscopy has a weak agreement, Kappa index statistics (0.46) with molecular techniques (PCR) (0.46, 95% CI,02-0.4).
|
PCR |
|||||||
|
Diagnostic Test |
Positive |
Negative |
Sensitivity(%) |
Specificity (%) |
PPV% |
NPV%Kappa’s |
Index |
|
Microscopy |
|
|
|
|
|
|
|
|
Positive |
37 |
8 |
82.2 |
64.4 |
69.8 |
78.4 |
0.46 |
|
Negative |
16 |
29 |
|
|
|
|
|
|
PPV = Positive Predictive value, NPV = Negative predictive value |
|||||||
Table 2: Evaluation of Diagnostic Performance of PCR Verses Microscopy
DNA Amplification Sequence Analysis
DNA was extracted from 45 human blood samples obtained from Ilorin metropolis They were then amplified by PCR and detected through gel electrophoresis. 37 PCR products positive for W. bancrofti were purified The PCR products after amplification and detection by gel electrophoresis are shown in figure Fig 2,3 and 4. The W. bancrofti product size was 188bp against 100bp Molecular Ladder for the SspI repeat sequence. Column A showed DNA marker ladder 100 bp, column B showed the sample 1 to 13, In Figure 2, B to N (sample Number 1-13) gave a positive result for DNA W.bancrofti at 188bp .In PCR Result of the sample 14 to 23 Column A showed DNA marker ladder 100 bp, column B to K showed the sample 1 to 11,column N was blank (No sample). In Figure 3, column B,C,D,E,F,,G,H,I,J K,L,and M (sample number 1-12) also gave positive results in 188bp while N was negative. In figure 4, Column A showed DNA marker ladder 100 bp, column B showed the sample 1 to 13, B to N (sample Number 1-13) gave a positive result for DNA W.bancrofti at 188bp. The PCR examination PPV was 69.8% and sensitivity was 82.2% while the NPV was 78.4% and specificity was 64.4%. A positive control (PC) known to be infected with W. bancrofti was used. After PCR, an expected 188 bp PCR fragment was produced in the PC and NC is negative control.

Figure 2: Detection of W. Bancrofti Dna in Gel Electrophoresis Using Real Time PCR

Figure 3: Detection of W. Bancrofti DNA in Gel Electrophoresis Using Real Time PCR
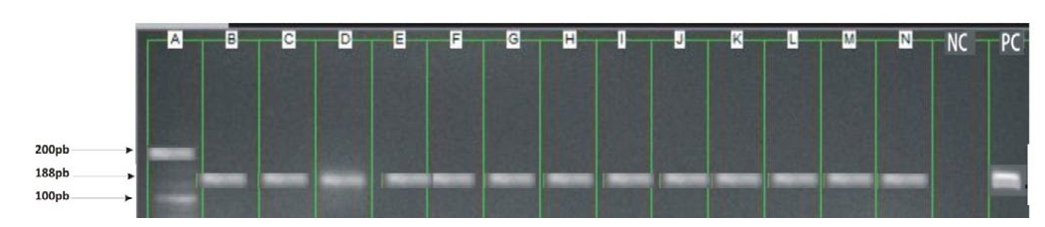
Figure 4: Detection of W. Bancrofti DNA in Gel Electrophoresis Using Real Time PCR
Phylogenetic Results
The phylogenetic analysis of SspI genes shows that the parasites were from three sites, the trees were drawn by neighbours joining method and supported with 1000 replicates bootstrap values which infer the phylogenetic trees. The division triangle, star and circle refers to the three types of parasitic variations within the species in Ilorin metropolis. Bootstrap value greater than or equal to 85% strongly support that the sequence data and branching order are accurate Fig 5. The evolutionary trees of the Ssp 1 genes in W. bancrofti was designed for the given sequences and the respective clades features were analyzed. The sequence Analysis of the amplicons of the samples investigated show a great number of similarities with W. bancrofti in Genbank according to BLAST analysis in NBCI .The genes were classified into three distinct clades based on the results of phylogenetic analysis and were indicated with symbols (circle ,star and triangle) .Circle denotes samples from Ilorin West, star denotes Ilorin East and triangle denotes Ilorin South. Each clades was presented as a monophonic member of a given ancestor. Clades (star) 19 has the largest number of members followed by clades (circle) 10 which show a level of similarities in divergence from their respective ancestors while triangle 8 has the least number of members . In addition the W. bancrofti sequences in Ilorin West were not 100% identical but were closely related. W. bancrofti strain in some communities were not closely related. For instance Ilorin South but those in Ilorin East were 100% closely related .


Figure 5: Evolutional Relationship of 37bp Of Ssp1 Gene of W. Bancrofti Using Neighbouring-Joining Phylogenetic Tree
Discussion
The positive rate detected using PCR was 37(82.2%) is a strong evidence that detection of parasite specific DNA in blood is more sensitive and specific than processing blood by standard methods, microscopy [[Nosrat,2021] [17-18]. These assays proved valuable tools for the diagnosis of lymphatic filariasis despite its relatively high cost as a diagnostic techniques. Our data corroborate with the finding of,who showed that PCR detected 22 positive cases among negative sample for blood filtration technique from individuals living in hypoendemic areas. Similar results were found using PCR and visualization on gel electrophoresis [3,7]. explained that the positive cases that were not detected using PCR could occur during the DNA amplification reaction as a result of various factors. [2,19]. Sustained reduction in prevalence of lymphatic filariasis infection in spite of missed rounds of mass drug administration in an area under mosquito nets for malaria control.
The sensitivity and specificity of the SspI PCR system has demonstrated its potential use as a diagnostic tool. The result presented in this study demonstrated that the SspI PCR assay can be used to detect low numbers of parasite. However, sometimes microscopy examination gives a negative result on microfilaria especially when the presence were only in a small amount. A PCR can overcome this weakness and PCR examination using the parasite DNA have been reproduced into thousands of copies and give a positive outcome when the microscopic examination cannot detect small number of worms [17]. Study by [Nosrat,2021] demonstrated that PCR-ELISA assay analysis of blood sample from 206 individuals from an endemic area compared with samples slide from a single sample revealed a sensitivity of 9.74% and specificity of 85.1%. Which are lower than the values in our study could be as a result of a recent population expansion [3]. This difference may be explained by factors that are inherent in the experimental procedures, which may generate errors related to the detection of parasites DNA, its degradation during the biological sample collection or absence in the sample analysed. The need for a specific and accurate diagnostic test for LF are important, the current incidence of LF does not show any signs of decline [17]. Without a sensitive and effective diagnostic test for the asymptomatic infections the accurate estimation of LF disease prevalence is not possible [18].
Without highly sensitive, specific tests, it will be difficult to ensure the objective control of LF. A recent publication from Thailand showed that filarial DNA could be detected by PCR analysis [4]. However, the authors did not report results of specificity testing or results obtained with field samples. In agreement with results reported by our preliminary studies showed that PCR work with NV1 and NV2 primers and SspI target sequence [17]. The result suggests that DNA detected by PCR is more sensitive for detecting W. bancrofti DNA in field samples in endemic country laboratories [Ugbomoiko et al, 2010] PCR can be applied to comparison between diagnostic methods and it is very useful to confirm suspicious cases that were not detected using conventional microscopy and evaluate cure control after chemotherapeutic treatment. This technique is important for long term success of parasite control by Mass Drug Administration (MDA) intervention because of the need to detect low intensity infections that persist even after treatment has occurred [Eward,2020]. This PCR technique is widely used for the diagnosis of several human diseases but its application in neglected diseases especially in Lymphatic filariasis was implored only recently. Some authors obtained high sensitivity and specificity compared to routine microscopy [10].
The nucleotide amplification sequencing and phylogenetic construction of the SspI DNA repeat reveal that there are different strains of W. bancrofti circulating in the human blood samples in Ilorin Metropolis (Ilorin East, West and South). The findings show that W. bancrofti strains in some communities were not closely related, For instance W. bancrofti strain in Ilorin South and Ilorin West. W. bancrofti in the study area clustered which differ from the previously reported W. bancrofti in China using SspI repeat region.The current study revealed a considerable diversity between the parasite strain of the three places, the phylogenetic analysis exhibited three distinct clusters of W. bancrofti among Ilorin East, South and West populations. The existence of different strains of W. bancrofti was documented in the past The parasite population of three locations of Ilorin metropolis exhibited very high genetic diversity formed at least three distinct clusters in the phylogenetic tree [20]. Though few studies have pointed to genetic and morphological variation in W. bancrofti populations, our findings agree with a previous study by,who reported the presence of two different genetic variants of the parasite with high genetic divergence and gene flow in different geo climate regions in India [12]. The existence of considerable genetic variability of W. bancrofti using RAPD markers was obtained in southern parts of India [12]. Such variability has been reported for other human parasitic nematode such as Ascaris and Trichuris trichiura [12,13]. Hence, influx of inflected population will result in a mixing up of genetically different population and thereby a great genetic diversity. It may be noted that a patient filaria infection results from multiple infective bite to human population [21]. Long term accumulation of infection brings genetic variants of the parasite in an infective individual. Thus increase in the genetic diversity and the genetic make-up of the parasite population in individuals may influence phylogenetic expressions in terms of drugs response, pathogenicity, clinical outcome and survival. The present study revealed the existence of genetically variant of parasite population of W. bancrofti. The study by showed that there is considerable genetic variability within W. bancrofti population in Ghana [7]. The genes were classified into the district clades base on the results of the phylogenetic analysis. The presence of multiple identical members depicts their common ancestors origin and can be due to a recent gene duplication event [9].
The data in this study shows that Ilorin South and Ilorin West samples are more distant. This study despite the small number of samples analyzed reveal some level of genetic variability in W. bancrofti in Ilorin metropolis thus, adding to the very few studies that aimed at understanding the genetic heterogeneity of W. bancrofti [3]. The genetic differences observed could be attributed to the environmental selection pressures. This may explain the epidemiological and field observations of lymphatic filariasis in Ilorin Metropolis. From the genetic tree the slightly closeness of samples from Ilorin East, South and Ilorin West could be as a result of migration of microfilaria individuals or vice versa. Migration is an important activity in Ilorin South and Ilorin West that occurs during specific times of the year, purposely for religious and economical activities could result in the transfer of parasites [11,14].
These findings in the genetic heterogeneity of the population at different places within microfilariae carriers called for appropriate chemotherapy strategies for the elimination of lymphatic filariasiA Furthermore, there have been reports of persistent residual Lf infections in some communities in Ghana and Burkina Faso, despite 5-8 rounds of treatments,Culex quinquefasciatus strains from Liberia had a low susceptibility to W. Bancrofti from Liberia, while the same strain had a high susceptibility to W. Bancrofti from Sri Lanka [16,19,20]. Consequently, the study concluded that the Liberian and Sri Lankan strains of W. Bancrofti differed in their ability to infect specific mosquito strains and therefore confirms our suggestion that the geographic strain of W. bancrofti can improve vector competence. The same reasons may explain the different epidemioogies of LF in East and West Africa, as to why Culex quinquefasciatusis not a vector of LF in West Africa, but is a very efficient in urban areas in East Africa [2]. However, this needs to be further investigated.In order to further explore the results produced in this study, we recommended that further studies with a much larger sample size and more detailed, population analyses be conducted on the diversity of W. bancrofti populations. This will enable the determination of profound conclusions on W. Bancrofti diversity. The availability of the complete mitochondrial genome sequence of W. Bancrofti will enhance a further understanding of phylogenetic and geographic relationships between isolates, and assessing population diversity within endemic regions [15,19].
Conclusion
Molecular assay seems to be promising substitute for direct mi- croscopy, Furthermore, another important aspect of molecular method is their applicability to epidemiological, such studies in- volved genetic diversity of populations and geographical distribu- tion of parasitic diseases The analysis of genetic profiles of Wuch- ereria bancrofti from the three sites in Ilorin Metropolis indicated the existence of considerable genetic variability among parasites population in the study area. The study showed that W. bancrofti in Ilorin metropolis were highly variable [22-24].
Acknowledgement
The authors gratefully acknowledge the technical assistance of the National Institute of Medical Research Yaba Lagos , West Africa research Ibadan .
References
- World Health Organization. (2016). Strengthening the assess- ment of lymphatic filariasis transmission and documenting the achievement of elimination. World Health Organization.
- Kwarteng, A., Arthur, Y. D., Yamba, J. K., Sylverken, A. A., Kini, P., Ahuno, S. T., & Owusu-Dabo, E. (2019). Influence of seasonal variation on reported filarial attacks among people living with lymphedema in Ghana. BMC infectious diseases, 19, 447.
- Christopher, G. M. (2020). The health and economic burdens of lymphatic filariasis prior to mass drug administration programs. Clin Infect Dis. 70(12), 2561–2567.
- Kariuki, T., Phillips, R., Njenga, S., Olesen, O. F., Klatser, P. R., Porro, R., ... & Hanne, D. (2011). Research and capacity building for control of neglected tropical diseases: the need for a different approach. PLoS neglected tropical diseases, 5(5), e1020.
- Hemalatha, K. V. R. P., & Prabhakar, R. V. (2016). Impact of lymphatic filariasis on quality of life of affected individuals: a community based cross sectional survey. Int J Health Sci Res, 6(6), 13-8.
- Krol, M., Brouwer, W., & Rutten, F. (2013). Productivity costsin economic evaluations: past, present, future. Pharmacoeco- nomics, 31, 537-549.
- Biritwum, N. K. (2016). Persistent ‘hotspots’ of lymphatic filariasis microfilaraemia despite 14 years of mass drug administration in Ghana. Transactions of The Royal Society of Tropical Medicine and Hygiene, 110(12), 690-695.
- Lau, C. L., Sheel, M., Gass, K., Fuimaono, S., David, M. C., Won, K. Y., ... & Graves, P. M. (2020). Potential strategies for strengthening surveillance of lymphatic filariasis in American Samoa after mass drug administration: Reducing ‘number needed to test’by targeting older age groups, hotspots, and household members of infected persons. PLoS neglected tropical diseases, 14(12), e0008916.
- Rainima-Qaniuci, M., Lepaitai, H. B., Bhagirov, R., Padmasiri, E., Naseri, T., Thomsen, R., ... & Yajima, A. (2022). The importance of partnership in the rollout of triple-drug therapy to eliminate lymphatic filariasis in the Pacific. The American Journal of Tropical Medicine and Hygiene, 87(1)79-87.
- Okorie, P. N., Ademowo, G. O., Saka, Y., Davies, E.,Okoronkwo, C., Bockarie, M. J., ... & Kelly-Hope, L. A. (2013). Lymphatic filariasis in Nigeria; micro-stratification overlap mapping (MOM) as a prerequisite for cost-effective resource utilization in control and surveillance. PLoS neglected tropical diseases, 7(9), e2416.
- Kumar, D., & Sharma, V. (2016). Evaluation of Acacia species as honeybee forage potential. International Journal of Science and Research, 5(1), 1726-1727.
- Stanton, M. C. (2017). Measuring the physical and economic impact of filarial lymphoedema in
- Tamura, K., Stecher, G., Peterson, D., Filipski, A., & Kumar,S. (2013). MEGA6: molecular evolutionary genetics analysis version 6.0. Molecular biology and evolution, 30(12), 2725-2729.
- Martindale, S., Mkwanda, S. Z., Smith, E., Molyneux, D., Stanton, M. C., & Kelly-Hope, L. A. (2014). Quantifying the physical and socio-economic burden of filarial lymphoedema in Chikwawa District, Malawi. Transactions of the Royal Society of Tropical Medicine and Hygiene, 108(12), 759-767.
- Kinyatta, N. M., Wangui Ng'ang'a, Z., Kamau, L., & Kagai,J. M. (2018). Comparison of indoor mosquito collection methods in the assessment of lymphatic filariasis transmission dynamics in mosquito vectors in Tana River County, Kenya. The East African Health Research Journal, 2(1), 58.
- MOH-Kenya (2019). Kenya National Breaking Transmission Strategy for Soil-Transmitted Helminthiasis, Schistosomiasis, Lymphatic Filariasis and Trachoma Parasite. Vec (2019– 2023)
- Ramesh, A., Small, S. T., Kloos, Z. A., Kazura, J. W., Nutman,T. B., Serre, D., & Zimmerman, P. A. (2012). The complete mitochondrial genome sequence of the filarial nematode Wuchereria bancrofti from three geographic isolates provides evidence of complex demographic history. Molecular and biochemical parasitology, 183(1), 32-41.
- Njenga, S. M., Mwandawiro, C. S., Wamae, C. N., Mukoko,D. A., Omar, A. A., Shimada, M., ... & Molyneux, D. H.(2011). Sustained reduction in prevalence of lymphaticfilariasis infection in spite of missed rounds of mass drug administration in an area under mosquito nets for malaria control. Parasites & vectors, 4, 1-9.
- De Souza, D. K., Koudou, B., Kelly-Hope, L., Wilson, M. D., Bockarie, M. J., Boakye, D. A. (2012). Lymphatc filariasis vectors and the implicatons for accelerated elimnation of Anopheles-transmitted filariasis in West Africa. Parast Vect. 5, 259
- Dai, M., Sato,A., Maeba, H., Iuchi, T., Matsumoto, M., Okuwa, M., ... & Sugama, J. (2016). Dermal structure in lymphedema patients with history of acute dermatolymphangioadenitis evaluated by histogram analysis of ultrasonography findings: a case-control study. Lymphatic Research and Biology, 14(1), 2-7.
- Njenga, S. M., Kanyi, H. M., Mwatele, C. M., Mukoko, D.A., Bockarie, M. J., & Kelly-Hope, L. A. (2022). Integrated survey of helminthic neglected tropical diseases and comparison of two mosquito sampling methods for lymphatic filariasis molecular xenomonitoring in the River Galana area, Kilifi County, coastal Kenya. Plos one, 17(12), e0278655.
- Chikwawa district, Malawi: A case–control study. Infec Dis. 6(1), 1–9.
- Federal Ministry of Health . Neglected tropical diseases:Nigeria multi -year master plan, 2015 2020. Abuja, Nigeria
- Lodh, N., Mwansa, J. C., Mutengo, M. M., & Shiff, C. J. (2013). Diagnosis of Schistosoma mansoni without the stool: comparison of three diagnostic tests to detect Schiostosoma mansoni infection from filtered urine in Zambia. The American journal of tropical medicine and hygiene, 89(1), 46.