




Case Report - (2024) Volume 3, Issue 1
Mitral Valve Replacement for Failed Mitra Clip: A Case Report
2Department of Cardiology, Dabbous cardiac center, Adan Hospital, Kuwait
3Department of Cardiology, Kuwait hospital, Sabah Al Salem area, Kuwait
Received Date: Feb 23, 2024 / Accepted Date: Mar 20, 2024 / Published Date: Mar 26, 2024
Copyright: ©Â©2024 Nael Al-Sarraf, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Al-Sarraf, N., Saad, J., Alhumaidan, A., Yousef, A. (2024). Mitral Valve Replacement for Failed Mitra Clip: A Case Report. J Surg Care, 3(1), 01-03.
Abstract
Mitra Clip is an interventional procedure used in mitral regurgitation patients who are surgically inoperable or are at high surgical risk. However, there is a failure rate associated with this procedure and in some instances no surgical intervention can be offered due to the inoperability risk. We report a case of failed Mitra Clip in a patient that was originally considered to be high surgical risk due to frailty that later required a double valve surgery for failed Mitra Clip within 1 year of the procedure. Although her surgical risk was even higher at the time of surgery, the patient tolerated the surgical procedure well with no complication. This case highlights the importance of properly defining patients at high surgical risk at the first instance as subsequent surgery can be performed with excellent outcome.
Keywords
Mitra Clip, Heart Failure, Mitral Valve Regurgitation.
Introduction
The use of Mitra Clip as an interventional procedure in patients with inoperable surgical risk or high surgical risk has been employed in cases with severe symptomatic mitral regurgitation (MR) who are anatomically suitable. However, the definition of high surgical risk is loosely defined based on the presence of other medical conditions or presence of frailty in such patients. Here we report a case that was initially considered to be high surgical risk at the time of Mitra Clip insertion but after failing the procedure became even higher risk (than at the time of her index procedure) and required double valve surgery instead of one with a decrease in the ejection fraction. The patient tolerated the surgical procedure well with no complication.
Case Report
66 years old lady known case of hypothyroidism, hyperlipidemia, previous cerebrovascular accident that recovered, recurrent syncope attacks secondary to partial seizures and recent paroxysmal atrial fibrillation was referred for surgical evaluation. She was frail with history of cervical spondylosis. She had positive family history of ischemic heart disease affecting her brother and mother and she was non-smoker. Patient previously underwent Mitra Clip at another institute 1 year previously for severe degenerative mitral regurgitation (MR). The procedure at the time was uneventful with reduction of her mitral regurgitation to mild MR (Garde I). However, 6 months following the procedure she had increasing shortness of breath on exertion and later at rest with New York Heart Association class III/IV symptoms (NYHA class III/IV). She subsequently required two hospitalizations for heart failure over the next 4 months. Repeat transthoracic echocardiography showed severe recurrent MR with an anteriorly directed jet with prolapse of part of P2 and P3 segments (Figure 1 A).
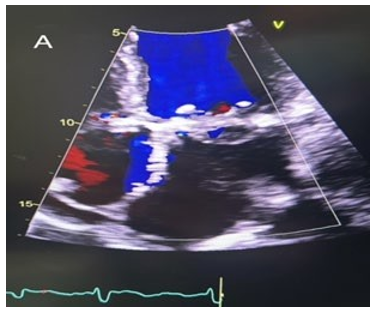
Figure 1A: Pre-operative four-chamber view of transthoracic echocardiography showing severe mitral regurgitation.
This was associated with moderate to severe functional tricuspid regurgitation (TR) and pulmonary artery systolic pressure of 65 mm HG with severely dilated left atrium. There was a decrease in the ejection fraction from 60% to 45%. This was confirmed by trans-esophageal echocardiography (TEE). Coronary angiography showed normal coronaries and dominant right system. Carotid duplex was normal with normal thyroid function tests and normal renal and liver profile. Patient underwent mitral valve replacement (Size 27 Magna Ease Bioprosthesis) and tricuspid valve repair (Size 34 MC III annuloplasty) and removal of Mitra Clip device. The procedure was performed through median sternotomy with ascending aorta cannulation and bi-cava cannulation with cardioplegic cardiac arrest using antegrade and retrograde blood cardioplegia. The mitral valve was approached through superior trans-septal approach. Intra-operatively, there was fusion of P2 and A2 leaflets from Mitra Clip which was excised en-bloc with A2 and P2 (Figure 1B and 1C).

Figure 1B: Intra-operative surgical view of mitral valve showing the Mitra Clip in place with fusion of A2 and P2 and tethering pf P3 leaflet.
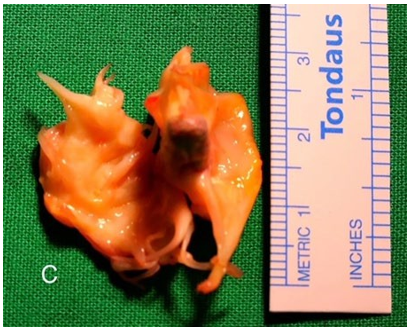
Figure 1C: En-bloc resection of mitral valve with Mitra Clip in place. P3 was prolapsed.
Tricuspid valve repair was done using MC-III ring downsize annuloplasty for functional TR. There was no intra-operative complications and aortic cross clamp time was 99 minutes and cardiopulmonary bypass time was 136 minutes. TEE post procedure showed well-functioning mitral valve prosthesis with no para valvular leak and mild tricuspid regurgitation. Post-operatively, patient was extubated 18 hours post-operatively and required small doses of inotropic support until day 2. She was transferred to the ward on day 3 and had uneventful post-operative course. She was discharged home with therapeutic level of warfarin at day 11 post-operatively. Pre-discharge echocardiography showed well –functioning mitral valve prosthesis with mean gradient of 2 mmHg (Figure 1 D). Tricuspid valve repair was satisfactory with mild tricuspid regurgitation. Patient was seen 6 months post-operatively and remained well with no shortness of breath.
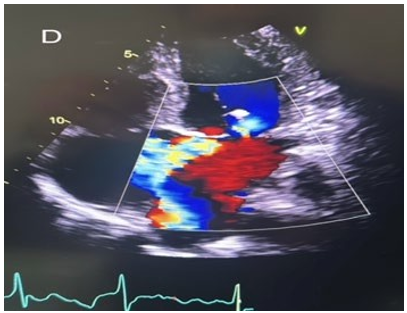
Figure 1D: Post-operative four chamber view of transthoracic echocardiography showing well-functioning bioprosthetic mitral valve.
Discussion
Since the clinical introduction of Mitra Clip device (Abbott Laboratories, Abbott Park, IL) into clinical practice, there has been increasing number of patients with MR that underwent this procedure. The procedure involves the trans-catheter placement of 1 or 2 Mitra Clip device under echocardiographic and fluoroscopic guidance with the purpose of restoring leaflet coaptation in degenerative mitral valve (whether functional or structural). The most recent American heart association guidelines recommend that Mitra Clip can be used in severely symptomatic patients (NYHA class III or IV) with primary severe MR and high (or prohibitive) surgical risk. This was recommended as class IIa recommendation [1]. However, the definition of inoperability or higher surgical risk depends on multiple factors and there is a failure rate of the device. In our case, the patient was considered initially to be higher surgical risk prior to Mitra Clip insertion due to frailty. However, the requirement of surgery within 1 year of the device failure necessitated double valve operation that the patient tolerated well with no complication despite the increased calculated surgical risk now compared to the time of Mitra Clip insertion. The results of mitral valve surgery following failed trans catheter Mitra Clip is limited to small case series in centers that have widely adapted the Mitra Clip procedure [2-6]. Their results are summarized in the table 1.
|
Study/year |
Number of patients |
Duration between Mitra Clip to surgery |
In-hospital mortality |
Morbidity |
|
Giedel 2/2014 |
19 |
12 days (median) |
10.5% |
CVA in 1 case. Pneumonia in 15.8% |
|
Monsefi 3/2014 |
6 |
106 days (mean) |
33.3% |
CVA in 1 case Bowel ischemia in 1 case |
|
Mkalaluh 4/2019 |
9 |
45 days (median) |
33.3% |
Pacemaker 33.3% Prolonged ventilation 22% |
|
Gerfer 5 /2022 |
17 |
23 days (mean) |
18% |
Pneumonia 12% Dialysis 12% |
|
Melillo 6/2021 |
172 (meta-analysis) |
330 Days (median) |
15% |
CVA 6% |
CVA: cerebrovascular accident.
Table 1: summary table of some previous reports of mitral valve surgery outcomes in failed Mitra Clip.
Mitral valve repair is challenging after failed Mitra Clip due to fusion of the leaflets with the device and /or leaflet peroration. As such, mitral valve replacement is commonly employed in such cases [2-6]. The rates of operative mortality and morbidity in these failed Mitra Clip cases partially results from the acute deterioration (i.e. cardiogenic shock) and partially results from the advanced age and comorbidities these patients originally have. Mortality rates reported ranged from 10% to 33% and is considerably high mortality following failed Mitra Clip. As shown in table 1, the morbidity associated with performing mitral valve surgery on these patients are also considerably high. Careful planning and timing of the surgical procedure in these patients is important to achieve good results. Acute deterioration of mitral valve following failed Mitra Clip results in poor outcome, especially in the immediate period following implantation. The definition of high surgical risk cases prior to Mitra Clip procedure should be reviewed in depth with heart team approach to select the best treatment modality that might benefit the patient.
Conclusion
We report a case of failed Mitra Clip 1 year following the procedure that was successfully treated with Mitral valve replacement in a patient that was considered initially as high surgical risk. Optimum timing of surgery and appropriate approach to such patients can potentially lead to improved outcome.
Acknowledgement
none.
Funding
None
Conflict of interest
None.
References
- Otto, C. M., Nishimura, R. A., Bonow, R. O., Carabello,B. A., Erwin III, J. P., Gentile, F., ... & Toly, C. (2021).2020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Journal of the American College of Cardiology, 77(4), 450-500.
- Geidel, S., & Schmoeckel, M. (2014). Impact of failed mitral clipping on subsequent mitral valve operations. The Annals of Thoracic Surgery, 97(1), 56-63.
- Monsefi, N., Zierer, A., Khalil, M., Ay, M., Beiras-Fernandez, A., Moritz, A., & Stock, U. A. (2014). Mitral valve surgery in 6 patients after failed MitraClip therapy. Texas Heart Institute Journal, 41(6), 609-612.
- Mkalaluh, S., Szczechowicz, M., Karck, M., & Weymann,A. (2019). Failed MitraClip therapy: surgical revision in high-risk patients. Journal of Cardiothoracic Surgery, 14, 1-4.
- Gerfer, S., Ivanov, B., Großmann, C., Djordjevic, I., Gaisendrees, C., Eghbalzadeh, K., ... & Wahlers, T. (2022). Mitral valve surgery after failed MitraClip—Operation for the inoperable?. Journal of Cardiac Surgery, 37(12), 4219-4224.
- Melillo, F., Baldetti, L., Beneduce, A., Agricola, E., Margonato, A., & Godino, C. (2021). Mitral valve surgery after a failed MitraClip procedure. Interactive CardioVascular and Thoracic Surgery, 32(3), 380-385.