
Archives of Infectious Diseases & Therapy(AIDT)
ISSN: 2577-8455 | DOI: 10.33140/AIDT
Impact Factor: 1.385


Research Article - (2025) Volume 9, Issue 3
Mineral Oxychloride: A Continuous Disinfection Method for Legionella Control in Healthcare Water Systems
Received Date: Sep 16, 2025 / Accepted Date: Oct 28, 2025 / Published Date: Nov 28, 2025
Copyright: ©2025 Tony Tanner. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Tanner, T. (2025). Mineral Oxychloride: A Continuous Disinfection Method for Legionella Control in Healthcare Water Systems. Archives of Infect Diseases & Therapy, 9(3), 01-06.
Abstract
Legionella colonization in healthcare and long-term care facility water systems continues to pose a significant public health risk. Traditional disinfection approaches, including thermal eradication and chemical oxidation, often fail to achieve stable, measurable microbial control. This study evaluates a mineral oxychloride-based method for continuous microbial reduction and biofilm suppression within hospital and extended care facility water systems. Data were collected by Legionella Specialties from over 105 facilities across the United States.
In accordance with the U.S. Environmental Protection Agency’s description of environmental testing, which includes analyzing the internal plumbing systems of buildings for the presence of Legionella pneumophila (the bacteria causing Legionnaires’ disease) and related water quality parameters such as pH (a measure of water acidity), temperature, and disinfectant residual (the remaining amount of disinfectant in the water) to assess treatment effectiveness and overall water quality (U.S. Environmental Protection Agency [EPA], 2016, p. 22), baseline analyses in this study included measuring water conductivity (which reflects the amount of dissolved salts), pH, oxidation-reduction potential (ORP, an indicator of a solution’s ability to break down contaminants using oxygen), free and total chlorine (levels of chlorine available for disinfection), adenosine triphosphate (ATP, a molecule found in all living cells used here as a marker for the presence of microorganisms), and temperature. Among 1,213 initial baseline sample points, approximately 40% exhibited ATP readings greater than 5 relative light units (RLUs, a scale indicating how much ATP—and therefore microbial activity—is present), with some exceeding 1,578 RLUs, indicating high microbial activity. Following application of the mineral oxychloride method and standard flushing protocols over a six-month period, fewer than 1% of post-treatment samples exceeded an ATP reading of 5 RLUs.
These results demonstrate that mineral oxychloride treatment effectively stabilizes key water quality parameters, creating a measurable, sustained oxidative environment. The approach aligns with EPA guidance, emphasizing ongoing monitoring of disinfectant residual levels, temperature, and water chemistry as indicators of treatment performance, thereby supporting proactive Legionella risk management and compliance with current healthcare water safety standards.
Keywords
Nuclear Tests, Radioactive Contamination, Groundwater, Algeria, Strontium-90, Cesium-137, Aquifer, Public Health, Health Impacts, Environmental Responsibility, Legionella Control, Legionella Prevention in Healthcare, Legionella Treatment for Hospitals, Mineral Oxychloride Disinfection, Continuous Disinfection System, Healthcare Water Safety, Infection Prevention Water Safety, U.S. Hospital Water Management, Waterborne Pathogen Control, CDC Legionella Guidance, Joint Commission Water Management Requirements, Ashrae 188 Compliance, St108 Water Program
Introduction
Legionnaires’ disease was first identified in 1976 following an outbreak at an American Legion convention in Philadelphia, where over 200 attendees became ill and 34 died. The causative agent, Legionella pneumophila, was later isolated and recognized as a waterborne bacterium that thrives in warm, stagnant environments such as those found in building plumbing systems, cooling towers, and decorative water features. Infection occurs primarily through the inhalation of aerosolized water droplets containing Legionella, allowing the bacteria to reach the lower respiratory tract, where they can cause severe pneumonia. The risk of disease is greatest in hospitals and long-term care facilities, where complex hot-water systems provide ideal growth conditions and patient populations often include the elderly, immunocompromised, and those with chronic respiratory conditions. These factors make healthcare water systems both a critical reservoir for Legionella and a focal point for prevention efforts to protect vulnerable occupants.
Today, Legionella bacteria remain one of the leading causes of waterborne disease outbreaks in healthcare and long-term care settings. Reported cases of Legionnaires’ disease have risen sharply over the past two decades, increasing nearly ninefold since 2000. According to the Centers for Disease Control and Prevention (CDC, 2017) and Ambrose, Roselle, Kralovic, & Gamage (2021), approximately 76 percent of all reported Legionnaires’disease cases are associated with healthcare facilities. Mortality rates among affected patients are estimated at roughly 25 percent, reflecting the vulnerability of populations typically served in these environments. (Patients in health care facilities at risk for Legionnaires’ disease, 2017) (Control & Prevention, 2017) Hospitals and extended care facilities present a unique convergence of risk factors: complex, temperature-variable plumbing systems that promote microbial growth and patient populations with compromised immune defenses. These combined elements underscore the critical need for active, verifiable control measures to prevent Legionella colonization and transmission within healthcare water systems.
A 2023 Meta-analysis of 48 studies (covering 23,640 water samples from hospital systems worldwide) found Legionella pneumophila in 41.6% of hospital water systems overall, with hot water systems at 47.6%-the most common contamination source. (A meta-analysis of Legionella pneumophila contamination in hospital water systems, 2023, pp. 1-8) (A meta-analysis of Legionella pneumophila contamination in hospital water systems, 2023) According to the Centers for Disease Control and Prevention (CDC), reported cases of Legionnaires’ disease have increased nearly ninefold since 2000, with the majority of outbreaks linked to complex building water systems such as those found in hospitals and extended care facilities [3]. (Legionellosis—United States, 2000-2009, 2011) (Hicks et al., 2011) Additionally, the number of cases of Legionnaires' disease has increased by 5.5 times since 2020 [4]. (Why Legionnaires' Disease is Surging in America, 2023) These environments provide ideal conditions for Legionella proliferation, including warm temperatures, stagnation, and biofilm accumulation within plumbing systems.
National standards such as ASHRAE 188 and Joint Commission Standard EC02.95.02 (outlined in the R3 report and ST108 Mandate) now require healthcare facilities to document and measure control measures as part of water management programs. Compliance now includes demonstrating continuing microbial control and data-backed system performance. (ANSI/ASHRAE Standard 188-2021, Legionellosis: Risk Management for Building Water Systems, 2021) (New Standard for Water Management Program, 2021).
Traditional mitigation strategies, including superheat-and-flush, chlorine dioxide, and monochloramine, face well-documented constraints in premise plumbing. Heat treatments can select for heat-tolerant strains and are often followed by rapid recolonization in complex hot-water circuits, particularly where recirculation losses reduce sustained thermal control [5]. Chemical oxidants frequently exhibit limited penetration into biofilms and undergo accelerated residual decay under stagnation, low-flow, and elevated-temperature conditions common in healthcare buildings [6]. The U.S. Environmental Protection Agency notes that while technologies such as emergency superheat-and-flush, hyperchlorination, and point-of-use filtration can temporarily reduce Legionella concentrations, no approach has consistently achieved long-term eradication of the organism from premise plumbing systems [6]. Monochloramine programs may be complicated by nitrification, temperature-dependent demand, and residual instability within distribution networks [7]. Chlorine dioxide requires careful control of chlorite and chlorate by- products and can raise concerns about material compatibility and corrosion, adding operational complexity [8]. Collectively, these factors contribute to inconsistent oxidant residuals and enable recolonization in low-flow or poorly mixed distribution zones (CDC). According to Liang, Cameron, and Faucher in “Development of heat-shock resistance in Legionella pneumophila modeled by experimental evolution,” adaptive heat tolerance further complicates thermal control strategies [9]. (Technologies for Legionella Control in Premise Plumbing Systems: Scientific Literature Review, 2016).
To address these limitations, Legionella Specialties implemented a mineral oxychloride-based approach to deliver a stable, continuously active oxidant residual (a persistent amount of disinfectant that remains in the water over time) throughout the water system. This method targets both planktonic (free-floating) and biofilm-associated (attached to surfaces in a slimy layer) Legionella by sustainably enhancing oxidation-reduction potential (ORP, a measure of the water’s ability to break down contaminants through oxidation) while maintaining stable water chemistry. ORP represents the oxidizing (disinfecting) power of an environment; the higher the value, the greater the disinfecting ability. Unlike conventional oxidants that degrade rapidly or require frequent dosing, mineral oxychloride gradually releases active oxidant species (molecules that can destroy bacteria) from a mineral matrix, providing predictable control with minimal corrosive impact. The present study evaluates the efficacy of this method across more than 105 hospitals and long-term care facilities, assessing baseline microbial activity through ATP (adenosine triphosphate, an indicator of living microorganisms) measurement and post-treatment outcomes following six months of mineral oxychloride application.
Materials and Methods
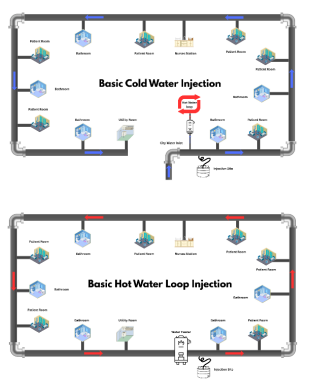
The mineral oxychloride disinfection approach implemented by Legionella Specialties employs precise metered injection of a mineral oxychloride solution into the facility’s water system. The cold-water injection points were strategically placed near the main water inlets to promote uniform distribution throughout the system and to facilitate comprehensive monitoring of hydraulic flow and disinfectant dispersion. In hot-water circuits, injection sites were selected in locations where temperatures consistently remained below 140 °F to prevent accelerated breakdown of the disinfectant, thereby preserving oxidant stability and ensuring sustained biocidal efficacy. Critically, the selection of adenosine triphosphate (ATP) as a primary monitoring parameter was informed by its utility as a sensitive, quantitative indicator of total microbial activity, encompassing both culturable and non- culturable microorganisms. Elevated ATP readings, which signal increased microbial load, or the presence of positive Legionella cultures during baseline assessments, prompted the initiation of mineral oxychloride treatment in both hot and cold-water loops to maximize system-wide microbial control. In contrast, systems exhibiting low baseline microbial activity began with cold-water injections only, reflecting a risk-based, data-driven deployment strategy.
This approach aligns with the U.S. Environmental Protection Agency’s observation that many facilities choose to implement supplemental disinfection systems following the detection of Legionella in tap-water samples or as a preventive measure to reduce risk and liability [6]. By installing a verifiable, continuously active oxidant residual within premise plumbing, Legionella Specialties’ mineral oxychloride program provides a consistent and measurable control method that complements the EPA’s recommendation for proactive treatment in facilities seeking long- term microbial stability.


The data collected from the participating facilities provide evidence that the application of continuous mineral oxychloride- based oxidation is causally associated with enhanced and sustained microbial control when compared to intermittent or reactive disinfection strategies documented in the EPA’s report. Specifically, after six months of mineral oxychloride treatment, more than 90% of sampling sites consistently exhibited ATP readings of 0 or 1 RLU, coupled with a stabilized mean oxidation- reduction potential of approximately 705 mV. This strong correlation between the initiation of mineral oxychloride treatment and the marked reduction in ATP —an established proxy for total microbial activity —suggests that maintaining an elevated oxidative environment directly impedes both general microbial regrowth and the proliferation of Legionella species. Moreover, the observed parameters remained within safe, regulatory-compliant residual limits throughout the study period. These results substantiate the hypothesis that a rigorously implemented, continuous disinfection regimen can fulfill the EPA’s anticipated standards for effective microbial risk management, thereby converting theoretical preventive recommendations into demonstrable operational outcomes.
Residual oxidant levels were maintained between 0.5 and 2.0 mg/L free chlorine equivalent, with 1.0 mg/L ±20% considered optimal. ORP was used as the primary indicator of oxidative activity, with values above 600 mV considered effective and above 700 mV ideal. Legionella are highly sensitive to oxidative environments, and high ORP values (e.g., above 550 mV) are generally correlated with no risk of proliferation. But this is not a hard rule. After six months of treatment, approximately 78% of test locations maintained ORP values above 700 mV, compared to fewer than 21% during baseline testing. Tanks containing the mineral oxychloride solution were refilled and inspected quarterly to maintain consistent dosing and system stability.
Sampling and analysis were performed by Legionella Specialties field technicians. Samples were collected from both predetermined sentinel points and randomly selected sites throughout each facility. Parameters measured included conductivity, pH, ORP, free chlorine, total chlorine, ATP, and temperature. ATP measurements were obtained using the Hygiena SystemSURE Plus v.2 luminometer with AquaSnap test devices. Based on more than 8 years of ATP monitoring in running-water systems, Legionella Specialties defines a pass threshold of ≤ 5 RLU for rapid ATP bioluminescence measurements. This threshold is more stringent than many surface-cleaning benchmarks (e.g., 10 RLU pass limit recommended for food-processing surfaces by Hygiena) and aligns conceptually with drinking-water studies that suggest action levels around 5 pg ATP/mL for distribution systems. When indicated, samples were submitted to a CDC-Elite-certified third- party laboratory for Legionella culture testing, conducted in accordance with Standard Methods for the Examination of Water and Wastewater (APHA).
Data were collected from over 105 hospitals and extended care facilities, comprising approximately 1,213 baseline samples and equivalent post-treatment follow-ups. Each facility’s post-treatment samples were collected from the same locations as the baseline to ensure comparability. ATP served as the primary indicator of microbial load. Baseline results indicated that approximately 40% of samples exceeded an ATP reading of 5 RLU, with some reaching 1,578 RLU. After six months of treatment and standard flushing protocols, fewer than 1% of samples exceeded an ATP reading of 5 RLU. (Exum et al., 2025) (Exum et al., 2025)
Results and observations
Following the introduction of mineral oxychloride treatment, microbial activity across all participating facilities decreased markedly and sustained. After six months of treatment, 90% of test results measured 0 or 1 RLUs, and fewer than 1% exceeded 5 RLU. The average post-treatment ORP was 705 mV, confirming a stable oxidative environment. Facilities with higher bacterial activity that received dual injections into the hot and cold loops saw microbial reduction 70% faster than with a single injection into the cold water loop. While the hot-water loop demonstrated faster results due to recirculation, the cold-water loop treatment remained the most practical solution for long-term operation and compliance.
Most facilities required initial dosage adjustments, beginning with higher concentrations to disrupt biofilm, followed by stabilization at lower doses within six months. In the majority of cases, Mineral oxychloride achieved effective microbial reduction at approximately one-tenth the concentration required for standard chlorine-based disinfection. Over time, facilities also observed gradual descaling of calcium carbonate deposits as biofilm and scale loosened from pipe walls. Post-treatment Legionella cultures were nearly all negative, with no persistent positives reported after six months of continuous treatment. (Elimination of Legionella colonization in a hospital water system: evidence from 23 years of chlorine dioxide use, 2025) (Exum et al., 2025).
Discussion
This multi-facility field study demonstrates that continuous application of mineral oxychloride can achieve sustained microbial control across complex healthcare plumbing systems while maintaining chemical stability and safety. Chemically, mineral oxychloride functions through energized oxygen molecules supported by a mineral electrolyte matrix, with energized chlorine molecules serving as a background component. This produces a dual-action oxidative potential; reactive oxygen species provide broad-spectrum microbial inactivation, while the stable mineral matrix maintains residual activity without significant corrosion or byproduct formation. The result is a consistently high ORP that directly correlates with low microbial activity and long-term system cleanliness.
From a regulatory standpoint, this approach aligns with ASHRAE 188 and Joint Commission Standard EC.02.05.02 as outlined in the R3 Report (Issue 32). The R3 Report calls for facilities to maintain a living water management program that identifies system components, defines monitoring parameters, and tracks corrective actions. By using measurable indicators such as ATP and ORP, facilities can demonstrate ongoing microbial control, fulfill documentation requirements, and maintain compliance with ST108 expectations for measurable outcomes. All Legionella samples were collected under full chain of custody and analyzed by accredited CDC laboratories in accordance with APHA and CDC guidelines, ensuring data accuracy and regulatory integrity.
Compared with traditional chlorine or monochloramine systems, mineral oxychloride offers a more stable, lower-dose, and less corrosive method for continuous disinfection. Peer-reviewed studies of mineral oxychloride compounds in other disinfection contexts have shown strong antimicrobial efficacy, supporting the performance observed in this field application. (Ghimire et al., 2025) (Ghimire et al., 2025) Sustained ORP levels above 700 mV and ATP readings below 5 RLU indicate reliable suppression of microbial activity, satisfying both infection prevention and compliance objectives.
Limitations and future work
Despite the consistent outcomes observed across the 105 facilities, several important limitations constrain the generalizability and interpretive strength of these findings. Most notably, the study relied on data collected in heterogeneous operational environments, where considerable variability in plumbing design, water-source composition, and systemic flow conditions could confound direct attribution of efficacy solely to the mineral oxychloride intervention. Reliance solely on ATP bioluminescence as a measure of microbial activity introduces additional limitations, as this method lacks specificity across microbial taxa and cannot distinguish between pathogenic and non-pathogenic organisms. To address these gaps, future research should incorporate a broader array of microbial assays, such as heterotrophic plate counts (HPC) and quantitative polymerase chain reaction (qPCR), to provide more taxonomically resolved and pathogen-focused assessments of disinfection performance. Furthermore, the absence of a controlled, comparative arm in this field evaluation precludes direct assessment of relative efficacy, dose-response dynamics, and operational resilience of mineral oxychloride versus established disinfectants such as sodium hypochlorite, chlorine dioxide, and monochloramine. Rigorous, side-by-side laboratory experiments are necessary to elucidate these relationships and validate field observations under standardized conditions. Additionally, the current six-month observation period may be insufficient to capture the impacts of seasonal temperature fluctuations, variations in water usage, and long-term shifts in biofilm structure or disinfectant decay kinetics. Extending surveillance to 12–18 months would facilitate a more comprehensive understanding of oxidant stability and treatment durability. Finally, integrating automated, real-time monitoring of key parameters such as ORP and ATP could strengthen process control, support more granular compliance documentation under Joint Commission ST108 and R3 Report requirements, and provide faster detection of performance deviations. These enhancements would not only address methodological limitations but also support the development of best practices for continuous disinfection in dynamic healthcare water systems.
Conclusion
The results of this multi-facility evaluation demonstrate that mineral oxychloride provides a reliable, measurable, and regulatory- compliant method for microbial control in healthcare and long- term care facility water systems. Across more than 105 facilities and 1,213 baseline samples, the application of mineral oxychloride consistently reduced ATP readings to near-zero and sustained ORP levels above 700 mV. Its energized oxygen chemistry, supported by a mineral electrolyte matrix, delivers stable oxidation across varying conditions while minimizing corrosion and byproduct formation. This approach meets the documentation and monitoring expectations of ASHRAE 188, Joint Commission EC.02.05.02, and the R3 Report, enabling facilities to demonstrate measurable outcomes and continuous improvement under the evolving ST108 framework. Mineral oxychloride represents a scalable, science- based strategy for long-term Legionella risk reduction and improved water safety in healthcare environments [10-15].
References
- Centers for Disease Control and Prevention. (2017). Developing a water management program to reduce Legionella growth and spread in buildings: A practical guide to implementing industry standards. U.S. Department of Health and Human Services.
- Ambrose, M., Roselle, G. A., Kralovic, S. M., & Gamage, S.D. (2021). Healthcare-associated Legionella disease: A multi- year assessment of exposure settings in a national healthcare system in the United States. Microorganisms, 9(2), 264.
- Centers for Disease Control and Prevention. (2017). Vitalsigns: Health care–associated Legionnaires’ disease.
- Fang, Z., Zhou, X., Liao, H., & Xu, H. (2023). A meta- analysis of Legionella pneumophila contamination in hospital water systems. American Journal of Infection Control, 51(11), 1250–1262.
- Lanrewaju, A. A., Oguntoyinbo, F., Ojumu, T. V., & Babalola, O. O. (2022). A review on disinfection methods for inactivation of building-water-system linked pathogens: Conventional approaches to emerging technologies. Frontiers in Microbiology, 13, 991856.
- U.S. Environmental Protection Agency. (2016). Technologies for Legionella control in premise plumbing systems: Scientific literature review (EPA 821-R-16-001).
- Zhang, Y., Qiu, J., Xu, X., & Zhou, L. (2021). Disinfection kinetics of free chlorine, monochloramines, and chlorine dioxide on ammonia-oxidizing bacterium inactivation in drinking water. Water, 13(21), Article 3026.
- World Health Organization. (2008). Chlorine dioxide, chlorate and chlorite in drinking-water: Background document for development of WHO guidelines for drinking-water quality (WHO/HSE/WSH/08.07/52).
- Liang, J., et al. (2023). Development of heat-shock resistance in Legionella pneumophila modeled by experimental evolution. Applied and Environmental Microbiology, 89(9), e00666-23.
- Agency for Toxic Substances and Disease Registry. (2004). Toxicological profile for chlorine dioxide and chlorite. U.S.Department of Health and Human Services.
- American Society of Heating, Refrigerating and Air- Conditioning Engineers. (2018). ASHRAE Standard 188- 2018: Legionellosis: Risk management for building water systems. ASHRAE.
- The Joint Commission. (2024). R3 Report Issue 38: New and revised water management requirements (EC.02.05.02).
- The Joint Commission. (2024). Standard ST108: Watermanagement programs in health care facilities.
- Zhao, Y., Xie, X., Liu, Y., Zhang, S., & Wang, H. (2023). Evolution and control of Legionella pneumophila in water distribution systems: A review. Frontiers in Microbiology, 14, 10537758.
- Zhou, Q., Zhang, S., & Sun, L. (2021). Effect of temperature and disinfectant residual on Legionella pneumophila growth and control in premise plumbing. Applied Sciences, 11(10), 4474.