
Archives of Case Reports: Open Access(ACROA)
ISSN: 3065-7598 | DOI: 10.33140/ACROA


Case Report - (2024) Volume 1, Issue 2
Metronidazole-Induced Encephalopathy: A Case Report
2Department of Clinical Pharmacy, Wenzhou Medical University, Wenzhou, Zhejiang, PR,, China
Received Date: Nov 01, 2024 / Accepted Date: Nov 20, 2024 / Published Date: Dec 10, 2024
Copyright: ©©2024 Khaled Saleh, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Saleh, K., Mutahhar, A. W., Al-Zaazaai, A. A. (2024). Metronidazole-Induced Encephalopathy: A Case Report. Arch of case Rep: Open, 1(2), 01-03.
Abstract
Metronidazole is very commonly used worldwide. Minor adverse reactions to metronidazole include nausea, mouth dryness, vomiting, and diarrhea. Neurotoxicity is rare and seen predominantly as peripheral neuropathy, dizziness, vertigo, and headache. Cerebellar toxicity is quite rare and a serious side effect of metronidazole toxicity. We are reporting a rare case of metronidazole toxicity that presented with cerebellar ataxia.
Keywords
Metronidazole Toxicity, Encephalopathy, Cerebellum, Ataxia, Dentate Nucleus
Introduction
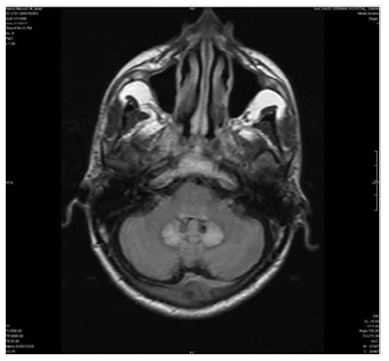
Metronidazole is a widely used drug in day-to-day gastro-enterology practice. It is prescribed for conditions like Crohn’s disease, intra-abdominal abscess, infection with Helicobacter pylori, hepatic encephalopathy, and Recurrent Pyogenic Cholangitis (RPC) [1]. Metronidazole is fairly safe and well tolerated but can induce toxicity of the central nervous system, which is also referred to as metronidazole-induced encephalopathy [2]. Three types of symptoms have been reported: seizures, cerebellar dysfunction, and acute changes in mental status. These symptoms can develop alone or in combination [2]. Brain MRI on T2-weighted FLAIR images reveals abnormalities, most commonly within the cerebellar dentate nuclei and corpus callosum. The third cerebral ventricle was sandwiched by bilateral cerebellar dentate nuclei, taking the form of a “chestnut.” The abnormality within the cerebellar dentate nuclei has thus been termed the “Chestnut Sign” in Japan, where several cases of metronidazole-induced encephalopathy have been reported [3].
Case Report
A 50-year-old male patient presented with progressively worsening difficulty in talking, imbalance during walking, mental confusion, headache, and weakness over the past 3 days the patient had a known case of decompensated alcohol-related cirrhosis of the liver with ascites, portal hypertension, and a history of recurrent hepatic encephalopathy.
At the presentation, his medical history showed that he had been using metronidazole (500 mg three times daily) for more than a year. On examination, he was inicteric and afebrile. The patient was drowsy with mild mental confusion but was easily arousable and oriented in time, place, and person. Neurologic examination revealed dysarthria, bilateral horizontal gaze nystagmus, positive Romberg's sign, positive bilateral finger nose test, wide base stance and gait, and impaired tandem walking suggestive of cerebellar-type ataxia. Asterixis was absent. Laboratory parameters on admission were normal.


Discussion
Neurotoxicity is one of the most important adverse effects of metronidazole therapy. The exact mechanism of metronidazole toxicity has not yet been elucidated [1]. Rao and Mason report that catecholamine neurotransmitters reduce the efficacy of 5-nitroimidazole drugs such as metronidazole and generate both semiquinone and nitroanion radicals [4]. These radicals are proposed to cause nervous tissue damage. Because of the reversibility of the MR imaging changes, the cause of the changes is most likely due to “axonal swelling with increased water content”, not axonal demyelination [5]. Metronidazole can cause irreversible neurotoxicity to the supratentorial white matter, and the mechanism of encephalopathy may differ from that of cerebellopathy. In addition, it can be inferred that MRI including DWI may have a role in diagnosis and the prediction of the prognosis of metronidazole-induced encephalopathy [6]. MR imaging findings exhibit typical abnormalities. High signal intensities in the globus pallidus on T1-weighted images have been established as a characteristic finding on MR images in chronic hepatic encephalopathy, and recent data have shown that white matter abnormalities can also be detected [7]. However, cerebellar lesions have rarely been observed in MRI studies, and there are a few reports describing abnormal T2 high signal intensities in superficial and deep cerebellar white matter including the brachium pontis in patients with acquired hepa- to cerebral degeneration [8]. In Mulcahy's study, the cerebellar lesions were the only demonstrated lesion on MR imaging [9]. A case report presented a patient with metronidazole-induced encephalopathy with contrast-enhanced lesions followed by permanent damage in the form of cystic changes [10].
References
- Sonthalia, N., Pawar, S. V., Mohite, A. R., Jain, S. S., & Surude,R. G., et al. (2016). Metronidazole-induced encephalopathy in alcoholic liver disease: a diagnostic and therapeutic challenge. The Journal of Emergency Medicine, 51(4), e79-e83.
- Kuriyama, A., Jackson, J. L., Doi, A., & Kamiya, T. (2011). Metronidazole-induced central nervous system toxicity: a systematic review. Clinical neuropharmacology, 34(6), 241-247.
- Kuriyama, A. (2017). Chestnut sign: metronidazole-induced encephalopathy. Journal of Emergency Medicine, 52(1), 101-102.
- Rao, D. N., & Mason, R. P. (1987). Generation of nitro radical anions of some 5-nitrofurans, 2-and 5-nitroimidazoles by norepinephrine, dopamine, and serotonin. A possible mechanism for neurotoxicity caused by nitroheterocyclic drugs. Journal of Biological Chemistry, 262(24), 11731-11736.
- Ahmed, A., Loes, D. J., & Bressler, E. L. (1995). Reversible magnetic resonance imaging findings in metronidazole-induced encephalopathy. Neurology, 45(3), 588-589.
- Kim, D. W., Park, J. M., Yoon, B. W., Baek, M. J., & Kim,J. E., et al. (2004). Metronidazole-induced encephalopathy.Journal of the neurological sciences, 224(1-2), 107-111.
- Brunberg, J. A., Kanal, E., Hirsch, W., & Van Thiel, D. H. (1991). Chronic acquired hepatic failure: MR imaging of the brain at 1.5 T. American journal of neuroradiology, 12(5), 909-914.
- Lee, J., Lacomis, D., Comu, S., Jacobsohn, J., & Kanal, E. (1998). Acquired hepatocerebral degeneration: MR and pathologic findings. American journal of neuroradiology, 19(3), 485-487.
- Mulcahy, H., & Chaddha, S. K. (2008). MRI of metronidazole-induced encephalopathy. Radiology Case Reports, 3(4), 239.
- Furukawa, S., Yamamoto, T., Sugiyama, A., Ohira, K., & Aotsuka, Y., et al. (2015). Metronidazole-induced encephalopathy with contrast enhancing lesions on MRI. Journal of the Neurological Sciences, 352(1-2), 129-131.