



Research Article - (2021) Volume 6, Issue 2
Mental Stress and Multiple Risk Factors of Cardiovascular Diseases with Regional Variations in Women of Urban and Rural Areas of Sindh, Pakistan
2Demonstrator, Department of Pathology, Bilawal Medical College, LUMHS, Jamshoro, Pakistan
Received Date: May 01, 2021 / Accepted Date: May 08, 2021 / Published Date: May 24, 2021
Copyright: ©Khalida Soomro, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Khalida Soomro, Muhammad Ali Soomro (2021) Mental Stress and Multiple Risk Factors of Cardiovascular Diseases with regional variations in women of Urban and Rural areas of Sindh, Pakistan. Cardio Open, 6(2): 134-140.
Abstract
Introduction: The high prevalence of risk factors in women in developing countries of South Asia appears to have been translated into early and severe CHD in contrast to their counterpart in the first world nations, which has been related to obesity and insulin resistance and genetically determined increased lipoprotein Lp(a) levels. Mental stress due to urbanization, sedentary life style and physical inactivity may be the most important factor initiating obesity and the clustering of all other risk factors hypertension, dyslipidaemia and (WHR). These risk factors vary in different regions of South Asia.
Aims and Objectives: Our aim of the study was to describe and analyse differences between the frequency of risk factors such as psychological stress due to, socio-economical aspects, life style especially physical activity, and health behaviours which may contribute in the course of CAD in women of both rural and urban areas of Pakistan because no such significant data is available in women with CAD.
Study Design: This descriptive cross-sectional comparative study was conducted in Cardiology Department of Dow University of Health and Sciences Karachi, Pakistan, from March 2014 to March 2016 by filling a questionnaire and laboratory data. The study group comprised female subjects around 577 (Urban 347 {60.1%} and Rural 230 {39.9%}) women ranged from 25-65 years of age who underwent coronary angiography and had definite coronary atherosclerotic diseases. Our study was conducted by examining the psychological stress in women of both areas and its strength of association with frequency of other risk factors in female patients of urban and rural areas with definite CHD taking account the difference in age and education level into account.
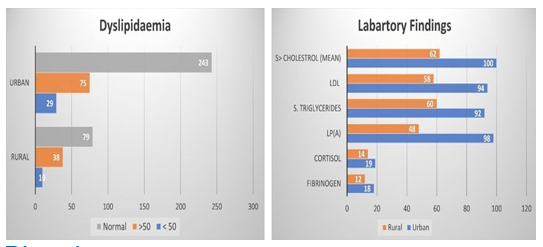
Result: Analysis of this study conducted at department of Cardiology in Dow University Karachi from March 2014 to March 2017 revealed that the women of rural area were comparatively more physically active then women of urban area. Prevalence of mental stress, hypertension, diabetes, obesity, higher BMI, hyperlipidaemia (especially TC) waist and hip circumference of both areas were found to be different after adjustment made for age. A considerable association was found between psychological stress and other factors in ischemic heart disease patients showing the p-value (p=0.043). Psychological stress was found 82% in both groups and (13%) women had no stress rated as normal more in rural (26%) vs (04%) in urban population. Physical inactivity in women with CHD was found in 92% urban in contrast to 45% in rural population, (p=0.009). Hypertension prevalence was more in urban 253 in comparison to 151 women in rural area. Diabetes Mellitus was also found more in urban than rural population, especially in age below 50, 79 (23%) urban vs 60 (26%) in rural population. Women beyond 50 years of age, 85 (24%) urban vs 64 (27%) rural area had prevalence of obesity comparatively higher in urban residents 71 (20%) than 44(%) in rural dwellers and 32 (9%) urban vs 16 (7%) in rural women in age range below 50 years. Higher waist circumstance was observed more in urban residents (4.8 cm) whereas BMI was more (1.8 unit) in women of rural area than urban women. Prevalence of smoking and nicotine chewing was relatively higher in urban population in below 50 years of age with 30 (09%) urban vs 13 (05%) in rural women and in age beyond 50, 11 (03%) urban vs 10 (04%) in rural women was witnessed. Average total cholesterol, serum triglycerides and LDL were found to be higher in urban compared to rural area residents and HDL was comparatively lower in urban area group. Mean cholesterol level was seen at average of 353 mg% in urban vs 223 mg% in rural population. Serum cortisol level showed significant variation in urban group 19.1 vs 14.2 in rural group (sample, as well as serum fibrinogen was raised more raised in urban population).
Conclusion: Our study shows increased prevalence of mental stress and physical inactivity in female residents of urban area leading to Higher blood pressure, DM, dyslipidaemia and central obesity specially in Waist circumference than rural area. The mental stress induced by excessive demands of work at home and at working place with too little control is not unique to women of urban areas.
Keywords
CHD: Coronary Heart Disease, LP: Lipoprotein, WHR: Waist-to-hip ratio, DM: Diabetes Mellitus, BMI: Body mass index, SPSS: Statistical Package for the Social Sciences, SD: Standard Deviation, GHQ: General Health Questionnaire, HSD: Hyper- mobility spectrum disorder
Introduction
CVD is the number one cause of death and disability in wom- en globally. Is the leading cause of death in developed countries where the substantial difference in morbidity and mortality also exists in women with a disproportionate share of suffering born by different life style conditions of urban and rural areas due to unexplained regional variations [1,2]. The role of the risk factors like high blood pressure, dyslipidaemia, diabetes, nicotine/tobacco consumption and obesity for CVD are established but underlying differences of lifestyle between women of different regions and places are still imperfectly understood [2]. In developing countries especially of South Asia, cardio-vascular risk factors are uniform- ly higher in both young and old women than European countries. The data collected from India, where lifestyles of urban commu- nities are similar to Pakistan supports the observation of early on- set of CHD in Asian women of urban areas. The relationship of life style induced stress in women of urban area is due to work at home and their professional responsibilities at work place are more associated with hypertension, hyperlipidaemia and coronary atherosclerosis then rural area women [2-6]. Due to sparse data, it is unknown whether these risk factors have had an impact on CVD levels and treatment in women of both areas of Pakistan. However, the widening array of preventive and therapeutic tools of safe and effective modern therapies along with selective adoption of health- ier habits due to increase awareness and literacy rate in urban areas are major links to expected cause of decline in CVD mortality.
Background
In the USA and England cardiovascular disease (CVD) mortality is higher in rural regions than in women of urban regions. Official statistics from the study conducted at Sweden show that regions dominated by rural communities have a higher incidence of myo- cardial infarction (MI) and stroke in both women and men. Studies by MONICA from 1986 to 1999 also supported that the burden of risk factors was higher in rural communities having low education level. Higher prevalence of dyslipidaemia, blood pressure, BMI and Diabetes were found in them [7-9]. Pakistan has passed through great socioeconomic transitions during the last 30 years with a large migration of population from rural to urban areas including women, having more mental stress in urban area, as they make it harder to practice heart-healthy habits, such as exercise in the form of physical work, in order to have healthy diet, and adequate sleep-in comparison to women of rural area. It is possible that those who stayed in the rural areas may have a less stress and have healthy lifestyle, therefore have less risk factors for CVD. Lower education and awareness about the modifiable risk factors of CVD in rural areas may have role to enhance or mediate the risk but mental stress due to multiple socioeconomical prob- lems of urban areas are leading to increase in the risk of CVD as there is evidence of well-defined connections between the mental stress and greater risk of CVD due to increasing atherosclerosis resulting in increased chances of the myocardial ischemic event. A recent study published in “The Lancet” had reported that the amygdala, an almond shaped portion of the brain located in tem- poral lobe which is involved in mental stress is associated with the depression and anxiety. Its activity has amplified when it receives stress signals, which leads to a larger risk of developing cardiovas- cular diseases [10]. The role of mental stress depends on an inter- action of at least three factors: the nature of stressor, its perception by individual, and the individual’s physiological susceptibility. These might lead to an increase in the secretion of the glucocorti- coids, catechol amines, and the inflammatory cytokines by initiat- ing the stimulation of sympathetic nervous system, Hypothalamus and Pituitary adrenal axis, thus on heart rate, blood pressure and cardiovascular disease. The stress may aggravate inflammation in coronary arteries, leading to blood clots that can trigger a heart attack. Unfortunately, the body does a poor job of discriminating between grave, imminent dangers and less momentous ongoing sources of stress, such as financial difficulties, job strain, home re- lated stress and even worries about potential problems that haven’t yet arisen and the body suffers [11].
Our aim of study was to describe and analyse the differences be- tween the frequency of risk factors due to psychological stress from life style and socioeconomical aspects, which may contribute in the course of CAD in women of both areas.
Study design
This descriptive cross-sectional comparative study was conducted at Cardiology Department of Dow University of Health and Sci- ences, Karachi, Sindh, Pakistan from March 2014 to March 2016 to examine the strength of association between mental stress and frequency of other risk factors in female patients of rural and urban areas with definite CAD after taking differences into account of age and education level. The study group comprised female sub- jects 577 (Urban 347 {60.1%} and Rural 230 {39.9%}) ranged from 25-65 years of age who underwent coronary angiography and found to be having definite coronary atherosclerotic diseases selected through non probability consecutive sampling. The pos- sible adverse effects of prolonged stress due to socioeconomical and cultural differences on risk factors of the CHD in both regions have been the subject of intensive study. Thus, we designed the study protocol to assess and compare the incidence of stress, obe- sity, hypertension, diabetes, dyslipidaemia and physical inactivity in both groups.
Patient’s psychological stress level was determined by Self-Ad- ministered General Health Questionnaire assessing the psycho- logical stress level and other risk factors. Data was collected for risk factors in women who underwent coronary angiography and found to be having confirmed coronary atherosclerotic heart dis- ease. Biochemical profile for CVD risk factor inclusive of Lipid Profile, after 12 hours especially Lp (a), Cortisol levels and fibro- gen at morning hours was done. All collected data was analysed by using Statistical Package of Social Sciences (SPSS) version 21. Descriptive data on numerical variables was analysed through mean and standard deviation (SD) while categorical results were analysed in the form of frequencies and percentages were assessed by chi square test.
Result
Study was conducted at single centre in Cardiology Department of Dow University of Health and Sciences Karachi, Sindh, Pakistan, from March 2014 to March 2016. The study group comprised 577 (Urban 347 {60.1%} and Rural 230 {39.9%}) women patients of known IHD of age ranged from 25-65 years with Primary educa- tion 166 (48%) in urban vs 18 (8%) in rural area women. Table 1
Table 1: Age, regional variation and primary educational level of the patients of study
|
Area of living; |
Number of Patients |
Educational Level |
|
Urban |
347 (60.1) |
166 (48%) |
|
Rural |
230 (39.9) |
18 (8%) |
|
Age; mean ± SD |
54.84 ± 9.56 |
184 (32%) |
Table 2: Psychological stress and other factors in women with ischemic heart disease of Urban and Rural Population
|
Stress Level |
Total 577 |
Urban 347 |
Rural 230 |
|
No Stress |
75 (13%) |
15 (04%) |
60 (26%) |
|
Minimal Stress |
58 (10%) |
40 (11%) |
18 (08%) |
|
Moderate Stress |
242 (42%) |
140 (40%) |
52 (22%) |
|
Severe Stress |
201 (35%) |
168 (48%) |
33 (14%) |
|
Physical Inactivity |
Total 577 |
Urban 347 |
Rural 230 |
|
Normal category |
154 (26%) |
28 (8%) |
127 (55%) |
|
Moderate inactivity |
326 (56%) |
246 (71%) |
80 (35%) |
|
Severe inactivity |
96 (16%) |
73 (21%) |
23 (10%) |
|
Hypertension 404 |
Total 577 |
Urban 347 |
Rural 230 |
|
< 50 |
179 (31%) |
109 (31%) |
70 (30%) |
|
Above > 50 |
225 (39%) |
144 (33%) |
81 (35%) |
|
Normal |
173 (30%) |
94 (27%) |
79 (34%) |
|
Diabetes 288 |
Total 577 |
Urban 347 |
Rural 230 |
|
< 50 |
139 (24%) |
79 (23%) |
60 (26%) |
|
Above > 50 |
149 (25%) |
85 (24) |
64 (27%) |
|
Normal |
289 (50%) |
183 (53%) |
106 (46%) |
|
Dyslipidaemia 152 |
Total 577 |
Urban 347 |
Rural 230 |
|
< 50 |
39 (07%) |
29 (08%) |
10 (04%) |
|
Above > 50 |
113 (19%) |
75 (21%) |
38 (16%) |
|
Normal |
425 (73%) |
243 (70%) |
182 (79%) |
|
Obesity – Over weight 153 |
Total 577 |
Urban 347 |
Rural 230 |
|
< 50 |
25 (04%) |
16 (04%) |
9 (04%) |
|
Above > 50 |
10 (02%) |
2 (0.5%) |
8 (3.4%) |
|
Over weight |
Total |
Urban |
Rural |
|
< 50 |
80 (14%) |
55 (16%) |
35 (15%) |
|
Above > 50 |
38 (06%) |
24 (07%) |
14 (6%) |
|
Normal Weight |
424 (73%) |
244 (70%) |
170 (74%) |
|
Smoking – Tobacco Chewing 64 |
Total 577 |
Urban 347 |
Rural 230 |
|
< 50 |
43 (07%) |
30 (09%) |
13 (05%) |
|
Above > 50 |
21 (03%) |
11 (03%) |
10 (04%) |
|
Normal |
513 (89%) |
306 (88%) |
207 (90%) |
The total frequency of psychological stress in women with Isch- emic Heart Disease was found as 82% in both groups. According to standard cut of GHQ-12 results, no stress was found in 75 (13%) patients and rated as normal with 15 (04%) in urban vs 60 (26%) in rural population. While 58 (10%) had minimal stress more in contrast to urban 40 (11%) vs rural 18 (08%) 242 (42%) patients had moderate level of mental stress more in urban 140 (40%) then 52 (22%) in rural population, while total 201 (35%) showed se- vere psychological stress, 168 (48%) in urban vs 33 (14%) in rural population.
Table 3: A considerable association has been found between psychological stress and other factors in ischemic heart disease patients showing the p-value (p=0.043).
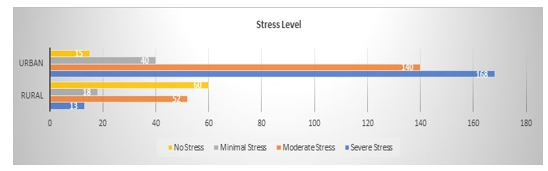
Physical inactivity in women with CHD was found in 92% urban women vs 45% in rural women of this study group, a significant association between the physical inactivity and psychological stress (p=0.009) was found. On the basis of standard cut offs of WHO DAS 2.0 questionnaire, 246 (71%) in urban vs 80 (35%) patients in rural were found to have moderate physical inactivity and 73 (21%) in urban vs 23 (10%) in rural were rated in severe category, while only 28 (8%) in urban vs 126 (55%) in rural were rated in normal category. Table 4
Table 4:
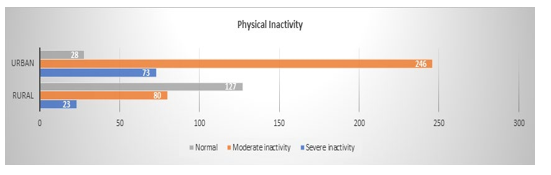
Table 5: Total women 577 of Study group had more than 1 CVD risk factors varying in women of both rural and urban communities [12].
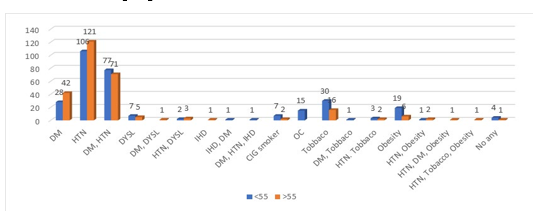
Overall prevalence of hypertension was more in urban 253 vs 151 in rural area. Women in both age group, in age<50 age were 109 (31%) urban vs 70 (30%) rural and in age>50 age 144 (33%) urban vs 81 (35%) rural population. Table 6(A) Average age adjusted, values of systolic and diastolic BP were highest in urban group 162/105 mmHg, and lowest in rural area with 155/100 mmHg.
Table 6:
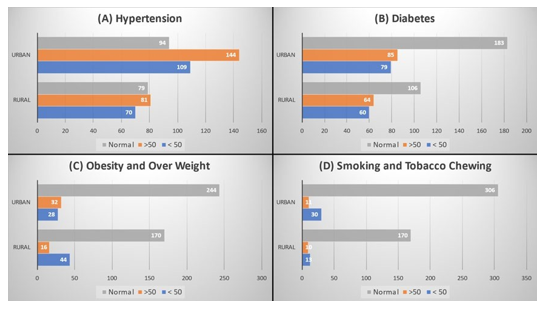
Diabetes Mellitus was found in 288 women of study group more in urban then rural population, in age < 50, 79 (23%) urban vs 60 (26%) in rural population. Amongst women aged >50, 85 (24%) urban vs 64 (27%) rural women were found to be diabetic Table 6(B). Over all over weight and obesity prevalence was 153 pa- tients in study group, comparatively high incidence was seen in 71 (20%) urban vs 44(19%) in rural area women in age<50 years and 28(8.0%) urban vs 22 (9.5%) in rural women of age group>50 years Table 6(C). Increase waist circumstance was seen more in urban residents (4.8 cm) and increased BMI in rural area residents (1.8 units) then in urban women. Smoking and Tobacco consump- tion in patients were high again in urban population both age group in age <50 30 (09%) urban vs 13 (05%) in rural women and in age >50, 11 (03%) urban vs 10 (04%) in rural women had this habit Table 6(D).
Biochemical Analysis: Total lipids were assessed. Dyslipidae- mia was found in 152 patients in age <50, 29 (08%) in urban vs 10 (04%) rural women. While in age >50, 75 (21%) urban vs 38 (79%) in rural women was observed Table 7(A). High incidence in urban population with average LP(a), total cholesterol, serum triglycerides and LDL and LPA were seen in urban compared to rural area women and HDL was lower in urban area group. Mean cholesterol Level was seen at average of 353 mg% in urban vs 223mg% in rural population. Increased triglycerides (mean 361 mg%) and higher LDL/HDL ratio>5 was seen in Urban than Ru- ral group. Serum cortisol level showed significant in urban group 19.1 vs 14.2 in rural group (sample taken at 8-10 a.m.), as well as serum fibrinogen was raised more in urban then in rural population Table 7(B).
Table 7:
Discussion
Many studies including NCD-RisC shows the presence of major geographic variations in risk factor for CVD in women and gen- erally small regional differences within same geographic regions [13]. In our study significant risk factors difference were observed in rural and urban areas due to general lack of awareness about modifiable risk factors because of difference in education level, in physical activity and psychological stress arising from dual re- sponsibilities at home and working place in major urban cities. Women in Pakistani culture specially of rural areas are under ed- ucated and often married at an early age leading to economical and psycho social dependence on male and lack of awareness which restrict their health care. Although they are more likely to be physically active then men and women of urban areas and meet all the life style targets in comparison to urban women, where- as women of the urban area may develop CVD because they are more stressed and exhibit greater cardiovascular reactivity [14,15]. Analysis of our study revealed by comparison with GHQ-12 and DAS 2.0 strong association between psychological stress and physical inactivity (p=0.009).The rural area women were older and more physically active then urban area women having more leisure time and physical inactivity, here the term physical activ- ity is not merely about sport or physical exercise but can be daily activity i.e. Walking to the market, working in fields, house hold work e.g. sweeping, washing clothes, and moping the large houses then in towns as physical movements can burn the body fat store. The excess calories will be stored as fat deposits therefore an in- crease in physical activity had an apparent relationship with waist circumference in rural area. The danger is when fats are stored in the blood vessel wall, causing atherosclerosis, hypertension, type 2 diabetes and obesity which are the known risk factors for heart disease and stroke. When calories consumed is more than calories used in daily activities, regular more physical activity can reduce it in urban women. [16,17].
Obesity is also result of imbalance between dietary intake and physical activity, i.e. someone who takes greasy foods, high fat and salty foods especially then their amount of calories consump- tion. It occurs twice more likely in urban women than women of rural area (OR =2, 06, 95%CI= 1, 13-3, 76) whereas intake of veg- etables and fruits is more common in rural area, as fibres inside fruit and vegetable would dissolve and bind bile acids in which fat is dissolved that will pass along with faeces, meaning that the more vegetable is eaten, the more fat and cholesterol are thrown away, and ultimately reducing fat deposits in the body. Also reduce the consumption of fat and sugar because fibre gives a sensation of fullness. Raised fruit and vegetable consumption ultimately reduce body weight and total cholesterol. In our study risk factors like obesity and waist circumference were less prevalent in rural area women explaining the favourable dietary habits and more physical activity as compared to urban women in whom rapid change in nu- trition pattern and physical inactivity occurs leading to these two risk factors as seen globally in urbanization [18-21]. A study by Mustelin et al. found a relationship between physical activity and waist circumference [17]. Waist and hip circumference with high- est value in rural areas in our study are same as other post-hoc stud- ies e.g. post-hoc Tukey HSD test which showed more obesity and increased BMI in women of rural than in urban areas (p < 0.001) but Waist circumference was higher in urban women, which cor- roborates a previous Swedish study. Combination of waist and hip circumferences better predicts CVD mortality than waist circum- ference alone, and an increased hip circumference might be bene- ficial both by potentially reflecting an increased muscle mass and by a protective physiology of the gluteo-femoral adipose tissue. In our study the increased hip circumference seen in the rural popu- lation underestimates the risk in rural women and might therefore represent a metabolically beneficial sign, to some extent balancing the increased risk and waist circumference in urban communities puts women at a higher risk of comorbidities associated with over- weight and obesity [13,21].
Over all, systolic and diastolic blood pressure was highest in urban area and lowest in rural area. The prevalence of systolic BP was higher in young women <50 age and diastolic BP in women of >50 age in both groups in our study, In a post-hoc analysis of studies women in rural areas differed from those in the cities. In the previ- ous MONICA report from 1986-1999, the systolic blood pressure was higher in rural communities then urban areas, which was no longer evident in 2009. Possibly better awareness and treatment in rural areas has led to a decreased difference in both popula- tion women [22,23]. The prevalence of dyslipidaemia was high in urban women with average increase in total cholesterol, serum triglycerides, Lp(a), LDL and HDL were found to be lower in ur- ban area group in comparison to rural women in our study. Mean cholesterol Level was seen as 353 mg% in urban vs 223 mg% on average in rural population. Similar result with study conducted in Indonesia revealed 36.2% in women living in rural area vs 56.7% women in urban area. The data showed that the prevalence of hy- percholesterolemia was higher among urban population compared to rural population. In our study, in three cohorts of women, higher Lp(a) was associated with CVD only among those with high TC, and improvement in prediction was minimal [24]. Tobacco use in the form of smoking and chewing was more common in urban young women but elderly women of rural areas have the similar prevalence of smoking in comparison to tobacco chewing which is more common in urban population. Overall Tobacco use in the form of Smoking and chewing was more in urban women in both age group in<50, 30 (09%) urban vs 13 (05%) in rural women and in age>50, 11 (03%) urban vs 10 (04%) in rural women. Increased prevalence of diabetes was seen in women living in urban areas compared to women in rural area. Out of 288 diabetic women of study group more were found in urban areas then in age<50, 79 (23%) urban vs 60 (26%) in rural population. In age>50, 85 (24%) urban vs 64 (27%) rural women. DM risk factor detection is very important while paying attention to the territory in order to map the cause and risk factor clearly [9,25].
Due to low socioeconomical status regular physical activity, hav- ing low leisure time. As well as more vegetable and fruit con- sumption then meat, better mental health and less stress is more common in sparsely populated regions (rural areas) then in large cities of Sindh province. These findings corroborate our results and extend them to the whole of Pakistan population having simi- lar living and life style conditions under the poverty level in back ground leading to more risk factors and lower life expectancy in the urban area women. This is different from study conducted in Sweden which revealed that rural communities have a higher bur- den of cardiovascular risk factors than urban communities, socio- economic transition and urbanization have led to decreased popu- lations in rural areas and changing characteristics of the remaining inhabitants in 2009, the rural population in northern Sweden was older, with less education, more abdominal obesity and higher cholesterol levels compared with the urban population. There was clustering of important CVD risk factors in Swedish rural areas due to more sedentary and under active physical style of life. Lack of jobs and opportunities to get an education influence and a more diverse cultural life of mixed population [7-9,18].
In Pakistan women of rural area are more physically active than men. Cultural aspects of rural living along with the socioeconomic and low educational level may affect the rural population to adapt primary preventive measures, increasing awareness due to social media network now days has overcome the difference hence wom- en of urban area of Pakistan have adverse impact of unhealthy life- style and mental stress due to dual responsibilities at home and work place. Findings from the Women’s Health Study (WHS) a landmark inquiry into disease prevention involving more than 17,000 female health professionals show that women whose work is highly stressful have a 40% increased risk of heart disease com- pared with their less-stressed colleagues [26]. The results, which were presented at an American Heart Association meeting in 2010, also showed that women who worry about losing their jobs are more likely to have high blood pressure and unhealthy cholesterol levels and to be obese. These findings are especially distressing in the current economic climate in Pakistan as well.
A study conducted to evaluate the prevalence of depression, anxi- ety and their associated risk factors, among the students of a med- ical college of Dow University in Karachi and Liaquat University of Health Sciences in Jamshoro, Pakistan used a self-administered General Health questionnaire (GHQ-12) [27]. Its Primary outcome was anxiety and depression which was revealed as a cut off val- ue of 19. The mean (SD) age of the students was 21.3 ± (1.88) years. A very high prevalence of anxiety and depression (70%) was found in women students after coming from rural areas and residing in hostels due to changes of life style. According to this study the role of physical inactivity in students is strongly and in- dependently cause of the obesity, and is also risk factor for CAD with odd ratio 3.9%, 95% of confidence interval (CI) 1.4-10.9 at adult age. Cultural aspects of rural living along with the socioeco- nomic and educational level were supposed to affect the rural pop- ulation to adapt primary preventive measures. In Pakistan primary education in women of rural area is comparatively less, leading to lack of awareness and higher levels of cardiovascular risk factors as a result but a causal link has not been proven in prospective studies [14,15]. Expansion of social media network now days has overcome the difference of awareness about the risk factors and hence women of urban area of Pakistan have adverse impact of unhealthy lifestyle more with less favourable eating, drinking, ex- ercising habits, variable psychological and emotional states due to dual responsibilities at home and work place, multiple concurrent jobs e.g, caring for children, aging parents, or other relatives while running a household and working outside the home job insecuri- ties. All can lead to increased prevalence of risk factor for CHD in urban women [12,28,29]. Giving rise to atherosclerosis due to direct effect of nor-epinephrine’s on fat cells alteration of the blood flow through adipose tissue. There is also evidence of link of cor- ticosteroid with CAD based on ↑ serum lipids leading to different coronary atherosclerotic status and variable risk factors in women of rural and urban area.
Strengths and weaknesses
In this study our women of rural areas who are having no facilities and economical resources due to sociocultural reasons were unable to reach in major centres for their CHD treatment in comparison to urban area residents e.g. for screening purpose, like most modern population studies on average younger age group are more likely to smoke and chew tobacco or have diabetes could not be included in study due to similar reason. This may limit the external validity of the study and introduce some bias, and caution is warranted in extrapolating the findings to the whole population. The definition of urban and rural in our study was subjective. Small communities lying very close to a town or city might reflect a different way of living compared with small communities in very remote areas, which are common in Pakistan.
Conclusion
Our comparison study shows increased prevalence of mental stress, physical inactivity and unhealthy diet in women of urban area lead- ing to increase in weight/obesity, waist circumference, and higher chance of diabetes, hypertension and dyslipidaemia more than in rural area with simultaneous increase in triglycerides, LDL and Lp(a). Cortisol and fibrinogen level were more in urban than rural area women giving rise to Coronary Atherosclerosis observed in most of the women of urban area with mental stress because of history of dual work load, and stressful job responsibilities which could be likely cause to increase the risk factors of CVD in them. Situations like this may be unavoidable. The presence of stress makes the urban area group more vulnerable for manifestation of multiple risk factors. Occupational hazards should be considered in the management of the Cardiovascular Disease in women.
References
- Barnett E, Halverson J (2000) Disparities in premature coro- nary heart disease mortality by region and urbanicity among black and white adults ages 35-64, 1985-1995. Public Health Rep 115: 52-64.
- Gupta R, Guptha S, Sharma KK, Gupta A, Deedwania PC (2012) Regional variations in cardiovascular risk factors in India: India heart watch. World J Cardiol 4: 112-120.
- Pandey RM, Gupta R, Misra A, Misra P, Singh V, et al. (2013) Determinants of urban-rural differences in cardiovascular risk factors in middle-aged women in India: A cross-sectional study. Int J Cardiol 163: 157-162.
- Gupta R, Deedwania PC, Sharma KK, Gupta A, Guptha S, et al. (2012) Association of educational, occupational and so- cioeconomic status with cardiovascular risk factors in Asian Indians: A cross-sectional study. PLoS One 7: e44098.
- Gupta R, Prakash H, Majumdar S, Sharma S, Gupta VP (1995) Prevalence of coronary heart disease and coronary risk factors in an urban population of Rajasthan. Indian Heart J 47: 331-338.
- Bhopal R, Unwin N, White M, Yallop J, Walker L, et al. (1999) Heterogeneity of coronary heart disease risk factors in Indian, Pakistani, Bangladeshi and European origin popula- tions: cross sectional study. BMJ 319: 215-220.
- Asplund K, Eliasson M, Janlert U, Stegmayr B (2006) What the MONICA project has taught us about cardiovascular dis- eases-society, public health and health care. Läkartidningen 103: 3006-3011.
- Eriksson M, Holmgren L, Janlert U, Jansson JH, Lundblad D, et al. (2011) Large improvements in major cardiovascular risk factors in the population of northern Sweden: the MONICA Study 1986-2009. J Intern Med 269: 219-231.
- Eliasson M, Janlert U, Jansson JH, Stegmayr B (2006) Time trends in population cholesterol levels 1986-2004: influence of lipid-lowering drugs, obesity, smoking and educational lev- el. The northern Sweden MONICA study. J Intern Med 260: 551-559.
- Stevo Julius (1969) Mental stress in labile hypertension. Lan- cet 293: P1215.
- Henry JP (1983) Coronary Heart Disease and arousal of Ad- renal Cortical axis in Dembroski TM, Schmidt T, eds Biobe- havioral Bases of Coronary Heart Disease based Karger 1-29.
- Khalida Soomro, Zaman Baloch (2020) Post PCI with Stent- ing Follow-Up in Women for 7 Years in Public Sector Tertiary Care Cardiac Unit. Retrospective Study. Cardio Open 5: 65- 71.
- NCD Risk Factor Collaboration (NCD-RisC) (2016) Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement stud- ies with 19•2 million participants. Lancet 387: 1377-1396.
- Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, et al. (2004) Effect of potentially modifiable risk factors associat- ed with myocardial infarction in 52 countries (the INTER- HEART study): case control study. Lancet 364: 937-952.
- Anand SS, Islam S, Rosengren A, Franzosi MG, Steyn K, et al. (2008) Risk factors for myocardial infarction in women: insights from the INTERHEART study. Eur Heart J 29: 932- 940.
- Louis J Ignarro, Maria Luisa Balestrieri, Claudio Napoli (2007) Nutrition, physical activity, and cardiovascular dis- ease: an update. Cardiovasc Res 73: 326-340.
- Mustelin L, Silventoinen K, Pietiläinen K, Rissanen A, Kap- rio J (2009) Physical activity reduces the influence of genet- ic effects on BMI and waist circumference: a study in young adult twins. International Journal of Obesity 33: 29-36.
- Sjöholm A (2007) Strong connection between abdominal obe- sity and socioeconomic factors Swedish IDEA study shows relation to cardiovascular diseases. Lakartidningen 104: 3862-3866.
- McKeigue PM, Marmot MG, Adelstein AM, Hunt SP, Ship- ley MJ, et al. (1985) Diet and risk factors for coronary heart disease in Asians in northwest London. Lancet 2: 1086-1090.
- Satija A, Hu FB, Bowen L, Bharathi AV, Vaz M, et al. (2015) Dietary patterns in India and their association with obesity and central obesity. Public Health Nutr 18: 303103041.
- McKeigue PM, Shah B, Marmot MG (1991) Relation of cen- tral obesity and insulin resistance with high diabetes preva- lence and cardiovascular risk in South Asians. Lancet 337: 382-386.
- Bord J, Fencl V, Hejl Z, Jirka J (1959) Circulatory changes underlying Blood Pressure Elevation during Acute Emotional Stress (Mental Arithmetic) in normotensive and Hypertensive subject. Clin Sci 18: 269-279.
- Von Kanel R, Mills PJ, Fainman C, Dimsdale JE (2001) Ef- fects of psychological stress and psychiatric disorders on blood coagulation and fibrinolysis: A biobehavioral pathway to coronary artery disease? Psychosom Med 63: 531-544.
- Nancy R Cook, Samia Mora, Paul M Ridker (2018) Lipopro- tein(a) and Cardiovascular Risk Prediction among Women. J Am Coll Cardiol 72: 287-296.
- Misra A, Pandey RM, Devi JR, Sharma R, Vikram NK, et al. (2001) High prevalence of diabetes, obesity and dyslipidemia in urban slum population in northern India. Int J Obes Relat Metab Disord 25: 1722-1729.
- Rexrode KM, Lee I-M, Cook NR, Hennekens CH, Bur- ing JE (2004) Baseline Characteristics of Participants in the Women’s Health Study. Journal of Women’s Health & Gen- der-Based Medicine.
- Muhammad Ali Soomro, K Soomro, Sadia Qasim, Shamshad Anwer (2016) Cardiac Risks in Youngsters: A Comparative Study In between Medical Students of DUHS & LUMHS. Med Channel 22: 70-76.
- Theorell T, Tsutsumi A, Hallquist J, Reuterwall C, Hogstedt C, et al. (1998) Decision latitude, job strain, and myocardial infarction: a study of working men in Stockholm. The SHEEP Study Group. Stockholm Heart Epidemiology Program. Am J Public Health 88: 382-388.
- Thomas KS, Nelesen RA, Ziegler MG, Bardwell WA, Dims- dale JE (2004) Job strain, ethnicity, and sympathetic nervous system activity. Hypertension 44: 891-896.