
Journal of Traditional Medicine & Applications(JTMA)
ISSN: 2833-1389 | DOI: 10.33140/JTMA
Impact Factor: 1.02



Research Article - (2025) Volume 4, Issue 1
Medicinal Flora of Chad: An Ethnobotanical Investigation into Traditional Healing Practices in N’djamena City
2Department of Pharmacognosy, College of Pharmacy, King Saudi University, Saudi Arabia
3Universite des Sciences et de Technologie d’Ati, Ati,T, Chad
4Centre National de Recherche, Roma, Italy
5Institut National Supérieur d’Elevage de Mossoro, Ndjamena, T, Chad
6Laboratory of Pharmacology, Pharmacokinetics and Clinical Pharmacy, Faculty of pharmacy, University of Lille, France
7Laboratoires TBC, Laboratory of Pharmacology, Pharmacoki-netics and Clinical Pharmacy, Faculty of Pharmacy, University of Lille, France
Received Date: Aug 26, 2024 / Accepted Date: Jan 23, 2025 / Published Date: Feb 06, 2025
Copyright: ©©2025 Bruno ETO, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Seid, A. B., Ngoupayo, J., Alqahtani, A. S., Bechir, A. B., Mahamat, A. B., et al. (2025). Medicinal Flora of Chad: An Ethno-botanical Investigation into Traditional Healing Practices in N
Abstract
Ethnopharmacological Relevance: Traditional medicine plays a significant role in the daily lives of Chadians, harmonizing alongside modern healthcare services provided by medical centers and hospitals. This practice is deeply rooted in the culture, both in rural areas and urban centers across the country.
Aim of the Study: This study aims to comprehensively document the medicinal plants utilized by the residents of N’Djamena, the capital city of Chad. In addition to cataloging the plants, we seek to understand the methods of preparation and administration of traditional remedies.
Materials and Methods: A thorough ethnobotanical survey was conducted in ten districts of N’Djamena between August and September 2021. This approach allowed for a deep dive into the traditional medical practices of the region.
Results: The study revealed a remarkable wealth of traditional knowledge in primary healthcare, highlighting the importance of plants in the local pharmacopoeia. At the end of this survey, we interviewed 25 traditional healers, which led to the identification of 60 plant species belonging to 37 different botanical families. Among these, the Fabaceae and Combretaceae families stood out for their frequent use. The collected recipes comprised a total of 159 preparations, with roots (23.33%), leaves (21.66%), and fruits (11.66%) being the most commonly used plant parts. The most prevalent methods of administration were oral (71.66%) and Oral use (16.66%), while decoction (46.66%) and maceration (40%) were the most popular preparation techniques. Water (84.35%) was the most frequently used solvent. These preparations were employed to treat a wide range of ailments, including malaria, typhoid fever, hemorrhoids, diarrhea, diabetes, gonorrhea, and sexual weakness.
Conclusions: This study underscores the extraordinary diversity of medicinal plants in Chad and their crucial role in primary healthcare. The 60 identified plants represent promising candidates for experimental studies aimed at developing new herbal medicines. By valuing traditional knowledge and integrating it into modern medical practices, it is possible to promote a holistic approach to healthcare that addresses the varied needs of the Chadian population.
Keywords
Ethnobotanical Inventory, Medicinal Plants, Traditional Medicine, Ndjamena Chad
Introduction
Improving human health is a pressing concern for many countries and international organizations worldwide, as it is a key aspect of sustainable development [1]. Despite the spectacular growth of the pharmaceutical industry, herbal medicine retains its significance, given that 25% of drugs produced and marketed globally are derived from plants. The African continent harbors a vast diversity of medicinal plants, with two-thirds of identified plant species residing in the tropical countries of Africa [2]. Access to these species is essentially cost-free for the population, with nearly 80% relying on them due to limited access to pharmaceutical drugs. However, the widespread adoption of traditional medicine poses several challenges, including insufficient scientific data resulting from tests evaluating the safety and efficacy of these traditional products [3]. The importance of plants for food, crafts, traditional medicine, pharmaceutical and phytopharmaceutical production, industry, economy, culture, and plant conservation in Africa, especially in Chad, remains in its infancy, despite being an essential resource for the planet. Additionally, very few inventories of medicinal plants have been conducted, despite the majority of the population relying on them for medical care. Given the variety and richness of Chad’s flora, coupled with the limited number of local plants subjected to clinical investigations, it is crucial to conduct an ethnobotanical survey of plants used in traditional Chadian medicine, specifically in the city of N’Djamena.
N’Djamena lies within a dry tropical climate that has transitioned from the Sudanian-Sahelian type between 1951-1967 to a Sahelian type. Its climate is characterized by distinct seasons, including a long dry season lasting 7 to 8 months (from November to May) and a short rainy season spanning 3 to 5 months (from May to October). Precipitation levels range between 400 and 700 mm per year, occurring mainly as intermittent downpours, with recent years witnessing a concentration of rainfall over a three-month period (July to September). Temperature variations are considerable, ranging from 20°C to 45°C during the dry season and from 18°C to 30°C during the rainy season [4]. The soils in N’Djamena are predominantly clay-sandy to clayey, often containing limestone nodules. Soil composition varies depending on the location, and despite the presence of clayey horizons, soil permeability is not negligible. Evaporation is the primary mechanism for dissipating surface water stagnation, despite the presence of clay. The characteristic vegetation formation in the area is shrub savanna dominated by Acacias, with additional steppic vegetation and varying densities of Balanite eagyptiaca and some species from the Combretaceae family. There is also a noticeable increase in urban tree planting initiatives as part of the government’s environmental policy.
This survey aims to not only document the diversity of medicinal plants but also to contribute to the scientific understanding of their therapeutic potential and cultural significance in addressing health needs in Chad. By bridging traditional knowledge with modern scientific methods, we can unlock the full potential of Chad’s rich botanical heritage for the benefit of its people and the wider global community.
Materials and Methods
Study Area Description
Our investigations were conducted in the city of N’Djamena, the capital and largest city of Chad, located in the central-western part of the country, on the right bank of the Chari River, at the confluence of the Chari and Logone rivers, approximately 100 km from Lake Chad. N’Djamena is situated at coordinates 12° 08’ North latitude, 15° 02’ East longitude, and an altitude of 295 meters [4]. N’Djamena serves as a vital hub for commerce, culture, and administration in Chad, making it an ideal location for studying traditional medicinal practices. Its geographical position at the convergence of major waterways and its proximity to Lake Chad contribute to its rich biodiversity and cultural heritage, including the utilization of medicinal plants in traditional healing methods. The city’s diverse population, comprising various ethnic groups and communities, further enriches its traditional knowledge of medicinal plants. Our study aimed to explore and document this rich botanical heritage within the urban landscape of N’Djamena, shedding light on the use of medicinal plants in local healthcare practices.

Figure 1: Geographical Map of N’Djamena
Material
All the medicinal plants listed in the province of N’Djaména.
Ethnobotanical Survey
The ethnobotanical survey was conducted across the ten different districts of N’Djamena, with two traditional practitioners selected from each district based on a sampling plan considering their ethnicities, religions, and various characteristics (including gender). With a total of 64 neighborhoods in N’Djamena distributed among the ten districts, our survey plan involved selecting two traditional practitioners from each district’s different neighborhoods, except for the 5th district where we interviewed seven traditional practitioners. We interviewed a total of 25 traditional practitioners representing the main ethnic groups in the region, including Hausa, Arab, Baguirmi, Boulala, Mandra, Kotoko, Moundang, Sara, Yoruba, Borno, and Mousgoum. To ensure a comprehensive understanding of the subject matter, our survey utilized a pre-established questionnaire containing specific questions tailored for traditional practitioners and herbalists. These questions covered ethnobotanical characteristics (such as the form of usage and the plant parts used) and ethno-pharmacological aspects (including preparation methods, administration modes, and essential effects). This approach aimed to provide a more representative insight into the local therapeutic and traditional applications within the population of N’Djamena. Fieldwork was conducted primarily during daylight hours, either after sunrise or before sunset, to facilitate effective data collection and plant specimen gathering.
Selection of Plant Species
Three criteria guided the selection of medicinal plant species used:
1. Plants most commonly used by multiple traditional practitioners to treat a single ailment without the association of another plant.
2. Plants notable for their quality of treatment in Chadian traditional medicine, especially those used to treat specific ailments.
3. Plants that are diverse and accessible for collection.
Data Processing
The data recorded on the survey forms were processed and entered into GraphPad software. Data analysis utilized simple descriptive statistical methods. Quantitative variables were described using the usual descriptive statistics, including measures of central tendency (mean, median) and measures of dispersion (standard deviation, range). Qualitative variables were summarized using frequencies and percentages. Additionally, graphical representations such as histograms and pie charts were used to illustrate the distribution and characteristics of the collected data.
Statistical Analysis
The quantitative data collected underwent analysis of variance using GraphPad, version 5.0 software. The Tukey test was employed to discern differences between means. The analysis aimed to identify any significant variations or disparities among the collected data sets. Using ANOVA, we assessed the impact of different factors on the observed outcomes. Subsequently, the Tukey test was employed to conduct pairwise comparisons between multiple groups, enabling us to determine which means were significantly different from each other.
Results and Discussion
Floristic Aspect
Medicinal Plants Listed in the Province of N'Djamena
|
Scientific name |
Family name |
Local name |
Herbarium identification |
|
Acacia albida; Faidherbia albida |
Fabaceae |
Haraz |
Num 3301 /Chad |
|
Acacia nilotica |
Fabaceae |
Garade |
Num 3499 /Chad |
|
Acacia senegal |
Fabaceae |
Kitir |
Num 1286 /Chad |
|
Acassia sieberiana |
Fabaceae |
Kouk |
Num 1747 /Chad |
|
Alium sativum |
Amaryllidaceae |
Thoum |
44810 SRf/Cam |
|
Allium cepa |
Amaryllidaceae |
Bassal |
42791 SRF/Cam |
|
Allium sp |
Amaryllidaceae |
Birrede |
Not yet classified |
|
Anogeisus leiocarpus |
Combretaceae |
Sahba |
Num 2419 /Chad |
|
Arachis hipogaea |
Fabaceae |
Foul |
Num 1924 /Chad |
|
Artemisia herba-alba |
Asteraceae |
Chih |
RAB76713 |
|
Azadiracta indica |
Meliaceae |
Guindjé |
Num 143 /Chad |
|
Balanites egyptiaca |
Zygophyllaceae |
Hydjilidje |
Num 1847 /Chad |
|
Bauhina ruffessens |
Fabaceae |
Koulkoul |
Num 1469 /Chad |
|
Blepharis maderaspatensis |
Acantaceae |
Albikhela |
Num 2375 /Chad |
|
Boscia senegalensis |
Capparaceae |
Mikhète |
Num 831 /Chad |
|
Brassica oleracea |
Brassicaceae |
Salat ta |
Num 25686 SRF/Cam |
|
Calotrpis procera |
Apocynacaea |
Achorro/Ouchar |
Num 2281 /Chad |
|
Camellia sinensis |
Theaceae |
Chahi |
Num 43103 SRF/Cam |
|
Capparis decidua |
Capparaceae |
Toumtoum |
Num 1201 /Chad |
|
Carica papaya |
Caricaceae |
Papai |
Num 658 /Chad |
|
Cassia italica; Senna italica |
Fabaceae |
Tor Azarag/Sana sana |
Num 728 /Chad |
|
Cassia seamea |
Fabaceae |
Dankani |
Num 2308 /Chad |
|
Citrus aurantium |
Rutaceae |
Yossoufi |
Num 34678 SRF/Cam |
|
Citrus limon |
Rutaceae |
Laymoune |
Num 25861 SRF/Cam |
|
Cleome gynandra L |
Cleomaceae |
Timlegue |
Num C1506 BF |
|
Coffea sp |
Rubiaceae |
Amkalawa |
Num 58228 SRF/Cam |
|
Combretum glutinosum |
Combretaceae |
Habil |
Num 2474 /Chad |
|
Combretum nigricans |
Combretaceae |
Chikhete |
Num 1991 /Chad |
|
Cratera adensonia |
Capparaceae |
Dabcar |
Num 1372 /Chad |
|
Cymbopogon schoenanthus |
Capparidaceae |
Mahareb |
Num 1876 /Chad |
|
Delbergia melanoxylon |
Fabaceae |
Babanousse |
Num 1305 /Chad |
|
Desmodium velutinum. Willd. |
Fabaceae |
Lebdo (Ngambay) |
Num 26682 |
|
Diospyros mespiliformis |
Ebenaceae |
Djokhane |
Num 1487/Chad) |
|
Eucaluptus globulus |
Fabaceae |
Safarmotte |
Num 4077 SRF/Cam |
|
Ficus sp |
Moraceae |
Djimese |
Num 1701 /Chad |
|
Gossipium sp |
Malvaceae |
Goutoune |
Num 1307 /Chad |
|
Greuia bicolor |
Malvaceae |
Daraba cadade |
Num 1301 /Chad |
|
Guiera sengalensis |
Combretaceae |
Khibeche |
Num 1474 /Chad |
|
Hypheane thebaica |
Arecaceae |
Dom |
Num 1336 /Chad |
|
Khaya sengalensis |
Meliaceae |
Mouraie |
Num 2336 /Chad |
|
Kygelia africana |
Fabaceae |
Machtour |
Num 1414 /Chad |
|
Leptadania hastata |
Asclepiadaceae |
Chalobe |
Num 2922 /Chad |
|
Manguifera indica |
Anacardiaceae |
Manga |
Num 1747 SRF/Cam |
|
Manihot esculenta |
Euphorbiaceae |
Angali |
Num 1792 /Chad |
|
Musa parasidiaca |
Musaceae |
Maouz |
UIH001/1186 |
|
Nigelle sativa |
Ranunculaceae |
Kamoun |
Num 3901 /Chad |
|
Olimum basilicum |
Lamiaceae |
Amrihané |
Num 6899 SRF/Cam |
|
Philiostigma reticulatum |
Fabaceae |
Kharoum |
Num 1205 /Chad |
|
Prosopis africana |
Fabaceae |
Amkachaw |
Num 1426 /Chad |
|
Psidium guayava |
Rosaceae |
Khirwe |
Num 1945 /Chad |
|
Sarcocephalus latifolius |
Myrtaceae |
Djawafa |
Num 49336 SRF/Cam |
|
Scleroaerya biarrea |
Anacardiaceae |
Himede |
Num 59469 SRF/Cam |
|
Senna italica |
Fabaceae |
Sanasa |
Num 13549 SRF/Cam |
|
Sesamum indicum |
Pedaliaceae |
Simsim |
Num 1277 /Chad |
|
Syzygium sp |
Myrtaceae |
Grunful |
Not yet classified |
|
Tamarundus indica |
Fabaceae |
Ardeb |
Num 2442 /Chad |
|
Trigonella foenum graecum |
Fabaceae |
Hilba |
FENU60001 |
|
Triulis terrestris |
Zygophylaceae |
Andirressa |
Num 1990 /Chad |
|
Vernonica clorata |
Asteraceae |
Tazou |
Num 44933 SRF/Cam |
|
Walteria indica |
Malvaceae |
Irgannar |
Num 3299 /Chad |
|
Zingiber officinalis |
Zingiberaceae |
Khurundjal |
Num 14757 SRF/Cam |
|
Ziziphus mauritiana |
Ramnaceae |
Nabag |
Num 1213 /Chad |
Most Represented Botanical Families in the City of N'Djamena
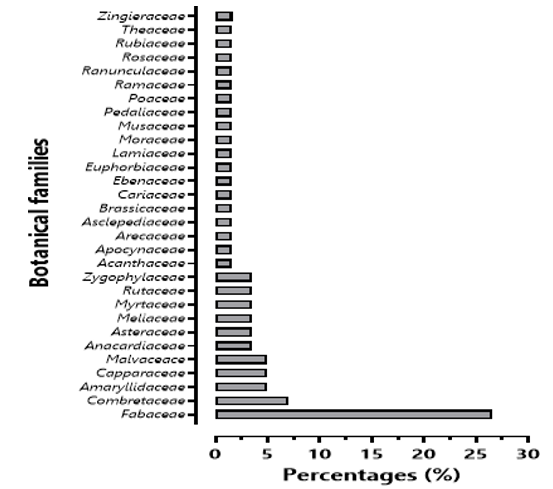
Figure 2: Percentage of Most Commonly Used Families in the Study Area
During our survey, we documented, collected, and identified 60 species of medicinal plants (Table 1). These 60 species, classified into 47 genera, belong to 37 plant families. Among these families, Fabaceae and Combretaceae were the most represented, accounting for 26.67% and 6.67% of the total species, respectively. Fabaceae emerged as the predominant family. This observation highlights the significance of Fabaceae and Combretaceae in the traditional medicinal practices of N;Djamena. These families likely contain species with potent therapeutic properties, contributing to their frequent utilization by traditional healers in the region.
Frequency of the Most Utilized Medicinal Plants
Analysis of the collected botanical data reveals that seven medicinal plants are the most commonly used in the survey area (see Figure 1). The species Khaya senegalensis, Guiera senegalensis, Allium sp, and Balanites egyptiaca are the most represented, accounting for 44%, 40%, 40%, and 36% respectively, followed by Diospyros mespiliformis, Prosopis africana, and Cassia italica with respective frequencies of 28%, 28%, and 24%.

Figure 3: Frequency of Most Commonly Used Plants in the Study Area
Ethnobotanical and Pharmacological Aspect
Classes of Traditional Practitioners
The ethnobotanical survey was conducted among 25 traditional practitioners, with a distribution of 96% men and 4% women. This gender distribution is also reported in the work of Mamadou Aissa et al. in 2017 [5]. According to traditional medical experience, 64% of traditional practitioners acquired their knowledge verbally from their parents or through involvement of the entire family in this field.
Preparation of Remedies
Medicinal species are used either alone or in combination with other plants for the treatment of various ailments, including malaria, typhoid fever, hemorrhoids (internal, external), diarrhea, constipation, diabetes, gonorrhea, jaundice, colic (intestinal, renal), parasitic diseases, and sexual weakness. The survey allowed us to record the recipes presented in the following tables:
|
Scientific name |
Family name |
Local name |
Parts used |
Method of preparation |
Routes of administration |
Diseases |
|
Acacia albida; Faidherbia albida |
Fabaceae |
Haraz |
bark |
Decoction |
Oral use |
Joint pain |
|
Acacia nilotica |
Fabaceae |
Garade |
Stem and bark; fruit; leaves and fruit |
Decoction or powder of fruits and dried leaves mixed |
Oral use; Oral use, nasal route |
Menorrhagia; Icterus; Gastritis; Angina; Dermatosis; Burn ulcer and breast cancer |
|
Acacia senegal |
Fabaceae |
Kitir |
Root |
Maceration |
Oral use |
Headache |
|
Acassia sieberiana |
Fabaceae |
Kouk |
Root |
Decoction |
Oral use |
Intestinal and renal colic, Diarrhoea |
|
Alium sativum |
Amaryllidace ae |
Thoum |
Garlic cloves |
Direct intake |
Oral use, nasal route |
Fever, diabetes, malaria, sinusitis, cough, cold |
|
Allium cepa |
Amaryllidace ae |
Bassal |
Bulbs |
Maceration |
Foot bath, nasal route; Oral use, Oral use |
Diabetes; sinusitis, coughs, colds; measles |
|
Allium sp |
Amaryllidace ae |
Birrede |
Bulbs, leaves |
Decoction |
Oral use |
Sexual impotence, lack of spermatozoa, burn ulcers, breast cancer; joint pains; myoma, paralysis, female sterility |
|
Anogeisus leiocarpus |
Combretacea e |
Sahba |
Leaves; roots |
Maceration or Decoction |
Oral use |
Diarrhoea; jaundice, joint pains |
|
Arachis hipogaea |
Fabaceae |
Foul |
Epicarp |
Maceration of epicarp powder |
Oral use |
jaundice |
|
Artemisia herba-alba |
Asteraceae |
Chih |
Whole plant |
Decoction or Maceration |
Oral use; Topical use; gargle |
Asthmatic attack, colic, dysentery; skin allergy; angina |
|
Azadiracta indica |
Meliaceae |
Guindjé |
Fruit, leaves, roots |
Maceration of leaves and fruit, Decoction of roots |
Oral use |
Diabetes; malaria, fever |
|
Balanites egyptiaca |
Zygophyllac eae |
Hydjilidje |
Fruit, seeds, buds; stem, root |
Maceration or Decoction |
Oral use |
Cough, bronchitis, cold, intestinal, and nephritic colic; jaundice; gastric ulcer; eye infection, joint pain |
|
Bauhina ruffessens |
Fabaceae |
Koulkoul |
Leaves and buds |
Decoction |
Oral use |
Typhoid, diabetes, malaria, chickenpox |
|
Blepharis maderaspatensis |
Acantaceae |
Albikhela |
Whole plant |
Maceration after transformation into powder |
Oral use |
Female sterility |
|
Boscia senegalensis |
Capparaceae |
Mikhète |
Fruits |
The fruit is eaten fresh after fermenting for 48 hours. |
Oral use |
Diabetes |
|
Brassica oleracea |
Brassicaceae |
Salat ta |
Leaves |
Maceration |
Oral use |
Diabetes |
|
Calotrpis procera |
Apocynacaea |
Achorro/O uchar |
Leaves; flowers |
Topical dressing |
Oral use; Oral use |
Filaria; gastric ulcer; abdominal pain; |
|
Camellia sinensis |
Theaceae |
Chahi |
Leaves; roots |
Decoction |
Oral use; local application on the scar |
Fever, malaria, haemorrhage |
|
Capparis decidua |
Capparaceae |
Toumtoum |
Bark; stems and buds |
Maceration or grilling of chickens with fresh stems; |
Oral use |
Fever; jaundice |
|
Carica papaya |
Caricaceae |
Papay |
Roots, leaves |
Decoction |
Oral use |
Gonorrhoea, intestinal worms, joint pains; jaundice. |
|
Cassia italica ; Senna italica |
Fabaceae |
Tor Azarag/San a sana |
Roots, leaves, whole plant |
Powdered paw |
Oral use |
Tooth decay, cough, bronchitis, colds; jaundice, malaria, intestinal worms. |
|
Cassia seamea |
Fabaceae |
Dankani |
Roots |
Decoction |
Oral use |
Typhoid, malaria |
|
Citrus aurantium |
Rutaceae |
Youssuffi |
Fruits |
Maceration |
Oral use |
Joint pain |
|
Citrus limon |
Rutaceae |
Laymoune |
Fruits |
Maceration |
Oral use |
Gastric ulcer, malaria |
|
Cleome gynandra L. |
Cleomaceae |
Timlegue |
Whole plant |
Decoction |
Oral use |
Fever, buccal infection |
|
Coffea sp |
Rubiaceae |
Amkalawa |
seeds |
Decoction |
Oral use |
Urinary retention |
|
Combretum glutinosum |
Combretacea e |
Habil |
Bark, roots, whole plant, seeds |
Maceration or Decoction |
Oral use |
Cancer; Burning ulcers; Malaria; Diarrhoea |
|
Combretum nigricans |
Combretacea e |
Chikhete |
Roots |
Decoction |
Oral use |
Jaundice |
|
Cratera adensonia |
Capparaceae |
Dabcar |
Bark, leaves |
Poudre or Decoction or Maceration |
Oral use |
Dermatitis, joint pain ; Diabetes, malaria |
|
Cymbopogon schoenanthus |
Capparidace ae |
Mahareb |
Whole plant |
Decoction or Herbal tea |
Oral use |
Menorrhagia |
|
Delbergia melanoxylon |
Fabaceae |
Babanouss e |
Seeds |
Maceration |
Oral use |
Sexual impotence |
|
Diospyros mexpiliformis |
Ebenaceae |
Djokhane |
Bark, roots |
Decoction |
Oral use |
Cough, bronchitis, cold, pneumonia, intestinal and nephritic colic; headache |
|
Eucaluptus globulus |
Fabaceae |
Safarmotte |
Leaves and roots |
Maceration |
Oral use |
Fever; intestinal worms |
|
Ficus sp |
Moraceae |
Djimese |
Roots |
Decoction |
Oral use |
Fever |
|
Gossipium sp |
Malvaceae |
Goutoune |
Leaves |
Decoction |
Oral use |
Diabetes, anaemia |
|
Greuia bicolor |
Malvaceae |
Daraba cadade |
Roots |
Maceration |
Oral use |
Skin infection |
|
Guiera sengalensis |
Combretacea e |
Khibeche |
Roots; Whole plant; Leaves |
Maceration or Decoction |
Oral use; Oral use |
Breast cancer and burn ulcer; Cough, bronchitis, cold, diarrhoea, Gonococcal disease, malaria, diabetes; Diabetes |
|
Hypheane thebaica |
Arecaceae |
Dom |
Leaves, roots; Fruit; Trunk of young plant |
Maceration or Powder |
Oral use, Eye drop |
Diarrhoea; hypertension, eye infection and haemorrhoids |
|
Khaya sengalensis |
Meliaceae |
Mouraie |
Fruits; bark, leaves, roots |
Decoction or Maceration |
Topical and oral use, Ear drop, |
Burning ulcer, Tooth decay; Burning ulcer, Breast cancer, Ear infection; Fever, jaundice, Gastric ulcer, Headache, Intestinal worms |
|
Kygelia africana |
Fabaceae |
Machtour |
Fruits, leaves |
Decoction or Powder |
Oral use; Topical use |
Typhoid; breast cancer; burn ulcer |
|
Leptadania hastata |
Asclepiadace ae |
Chalobe |
Whole plant |
Decoction or Maceration |
Oral use; Massage |
Fever, diabetes, bone or joint lesions (fractures, |
|
|
|
|
|
|
|
dislocations) |
|
Manguifera indica |
Anacardiacea e |
Manga |
Bark and leaves |
Decoction |
Oral use |
Insomnia, intestinal worms, diabetes |
|
Manihot esculenta |
Euphorbiace ae |
Angali |
Les tubercules |
Maceration |
Oral use |
Sperm insufficiency |
|
Musa parasidiaca |
Musaceae |
Moz |
Bark and leaves |
Decoction or Maceration |
Oral use |
Icterus, diabetes |
|
Nigelle sativa |
Ranunculace ae |
Kamoun |
Seeds |
Maceration |
Oral use; Oral use |
Fever, dermatitis |
|
Olimum basilicum |
Lamiaceae |
Amrihané |
Whole plant |
Powder |
Oral use |
Coughs, bronchitis, colds |
|
Philiostigma reticulatum |
Fabaceae |
Kharoum |
Leaves; roots |
Maceration or Powder |
Oral use; Topical use |
Diarrhoea; Gonococcal disease |
|
Prosopis africana |
Fabaceae |
Amkachaw |
Les racines ; les écorce de racine ; |
Powder or Decoction |
Topical use; Oral use |
Tooth decay, intestinal worms, diabetes, joint pain, malaria; Intestinal and renal colic. |
|
Psidium guayava |
Rosaceae |
Khirwe |
Les feuilles |
Decoction |
Oral use |
Fever |
|
Sarcocephalus latifolius |
Myrtaceae |
Djawafa |
Les racines |
Decoction |
Oral use |
Icterus, joint pain, complications following childbirth |
|
Scleroaerya biarrea |
Anacardiacea e |
Himede |
Bark and leaves |
Maceration or Decoction |
Oral use |
Diabetes; joint pain |
|
Senna italica |
Fabaceae |
Sanasa |
Leaves; roots |
Maceration or Powder |
Oral use, Topical use |
Constipation; gonorrhoea |
|
Sesamum indicum |
Pedaliaceae |
Simsim |
Seeds |
Maceration |
Oral use |
Fever, sperm insufficiency |
|
Syzygium aromaticum |
Myrtaceae |
Grunful |
Seeds |
Maceration or Essential oil |
Oral use; Topical use |
Asthma attack; tooth decay |
|
Tamarundus indica |
Fabaceae |
Ardeb |
Buds; leaves; fruit; bark |
Maceration or Decoction |
Oral use |
Fever; diabetes; headache; myoma |
|
Trigonella foenum graecum |
Fabaceae |
Hilba |
Whole plant |
Maceration or Decoction or Powder |
Oral use; Nasal route |
Dysentery, intestinal colic, diarrhoea, sinusitis |
|
Triulis terrestris |
Zygophylace ae |
Andirressa |
seeds |
Maceration |
Oral use |
Sexual impotence |
|
Vernonica clorata |
Asteraceae |
Tazou |
leaves |
Decoction |
Oral use |
Malaria |
|
Walteria indica |
Malvaceae |
Irgannar |
Whole plant |
Decoction |
Oral use |
Joint pain, Dermatitis, Skin infection |
|
Zingiber officinalis |
Zingiberacea e |
Khurundjal |
bulb |
Decoction |
Oral use |
Sexual impotence |
|
Ziziphus mauritiana |
Ramnaceae |
Nabag |
Bark roots |
Maceration |
Oral use |
Gonorrhoea, Prolonged lochia |
Table 1: List of Plant Species Found by Traditional Practitioners and Areas of Therapeutic Indication
Parts of Plants Used
According to the data collected during the survey, 11 different parts of plants are utilized for treating illnesses based on their therapeutic properties. Among the 159 recorded recipes, we present the utilization of these different parts in order of prevalence: roots (23.33%), leaves (21.67%), fruits (11.67%), bark, whole plant, and seeds (10% each), bulbs (5%), tubers (3.33%), stems (2.62%), pods, and epicarp (1.67% each). Overall, traditional practitioners primarily utilize roots, accounting for 23.33% of plant parts used, compared to other parts (Figure 4).

Figure 4: Graphical Representation of the Number of Plant Parts Used
Mode of Administration
The findings of this survey reveal that oral administration (71.67%) is the most preferred method among traditional healers, as well as their patients, followed by Oral use (16.67%). Other modes of administration did not exceed a rate of more than 7% (Figure 5).

Figure 5: Graphical Representation of the Different Types of Administration Identified
Mode of Preparation
Many traditional healers always seek the simplest method to prepare herbal medicines. Consequently, it is recognized that decoction, with its percentage of 46.67% (Figure 6), represents the most suitable method for preparation.

Figure 6: Graphs of the Different Preparation Methods Used
Discussion
The ethnobotanical survey conducted among 25 traditional healers has allowed for the inventory of potentially used medicinal plants in the city of N’Djamena. The utilization of these plants is closely linked to the profile of the respondents. Both elderly individuals and the younger generation share medicinal knowledge, albeit with slight differences in usage percentages. Women are nearly absent in the traditional medical field. Despite the challenges of life in the city, traditional healers often show great understanding regarding the pricing of herbal medicines, as prices are usually tailored to the financial capacity of their patients.
The investigations have gathered information concerning therapeutic practices in this city. The analysis of the results obtained by this survey identifies an inventory of 90 plants distributed among 37 families. It also shows that among the 37 families, Fabaceae is the most recorded (35%). From an ethnobotanical and pharmacological perspective, roots constitute the most utilized part (23.4%), decoction is the most practiced pharmaceutical form (52%), and traditional remedies are more commonly consumed orally (68%). Similarly, among all treated diseases, digestive disorders and infectious diseases represent the most frequently mentioned ailments.
The most represented Botanical Families used by traditional healer in the City of N’Djamena was Fabaceae. This result is similar to that observed in the capital of a neighbouring country of Chad in Bangui by Lakouéténé and colleagues in 2009 [6]. The Fabaceae, or Leguminosae, are a family of dicotyledonous plants in the order Fabales. It is one of the largest families of flowering plants, third only to the Orchidaceae and Asteraceae in terms of the number of species and is most easily found in the towns and cities of Central Africa. In contrast the most commonly used medicinal plants in the survey area were Khaya senegalensis and Guiera senegalensis and has been previously documented in the literature by Haidara et al. in 2020 [7]. Similarly, the multiple uses of Balanites egyptiaca by local populations in the Ouaddai province of Chad have been reported by Abdoulaye Brahim et al. in 2017 [8].
These findings underscore the importance of these medicinal plants in the traditional healing practices of the region. The high frequency of utilization those plants suggests that these species possess potent therapeutic properties and are valued by traditional healers for their efficacy in treating various ailments. Further research into the pharmacological properties and mechanisms of action of these plants could provide valuable insights for their potential integration into modern healthcare systems. This study reveals that in the study area, there are more men working as traditional healers. The ethnobotanical survey was conducted among 25 traditional practitioners, with a distribution of 96% men and 4% women. This gender distribution is also reported in the work of Mamadou Aïssa et al. in 2017 [7]. Indeed, age emerged as a predominant factor in qualifying a traditional healer. The majority of traditional healers were elderly individuals, as these older individuals are often considered to provide more reliable information. Traditional medicine (TM) is deeply rooted in ancestral knowledge and oral tradition, with younger generations often lacking interest in traditional practices. This finding aligns with ethnobotanical surveys conducted in Benin by Koudokpon et al. in 2017 and by Bentabet et al. in 2022 in Algeria [9,10].
In traditional medicine, the parts of the plant used to make the traditional potion are also important. Overall, traditional practitioners primarily utilize roots, accounting for 23.3% of plant parts used, compared to other parts. This finding differs from those found in Niger, where bark is the most utilized due to its high yield in active ingredients, efficacy, and conditions of use [11]. Roots are readily available throughout the year, even for non-annual plants. Despite the delicacy of their harvest, they remain the most resilient to heat, humidity, and transportation. Although the dry season is preferable for harvesting among traditional practitioners, it was noted that certain plant parts require collection during or at the end of the rainy season, such as leaves and fruits. This exploration revealed that plant parts are often used in combination to enhance efficacy, especially for treating infectious diseases [12-14]. However, the association is not limited to plants alone; sometimes, plants need to be mixed with an acidified solution (such as natural yogurt, tamarind fruit juice, etc.), or a vehicle to enhance their effects.
The mode of drug administration is also important. The findings of this survey reveal that oral administration (71.67%) is the most preferred method among traditional healers, as well as their patients, followed by Oral use (16.67%). Other modes of administration did not exceed a rate of more than 7%. For both traditional healers and patients, the oral route is the royal road for administering medicines. Oral administration appears to be the quickest in terms of absorption and distribution, enabling the treatment of diseases related to unknown or incurable causes, including witchcraft. Therefore, administering orally is deemed necessary, followed by body cleansing treatments. All diseases with internal triggers (such as hemorrhoids, intestinal worms, etc.) typically require this mode of administration. This investigation aligns with similar findings reported by Dibong and colleagues in 2011 in Cameroon [15]. This preference for oral administration underscores the perceived efficacy and convenience associated with this mode of delivery. It allows for rapid absorption and systemic distribution of the medicinal components, facilitating their therapeutic effects on internal ailments. Additionally, the cultural and traditional beliefs surrounding the perceived potency of orally administered remedies may contribute to its widespread adoption among traditional healers and patients alike.
Many traditional healers always seek the simplest method to prepare herbal medicines. Consequently, it is recognized that decoction, with its percentage of 46.67% (Figure 6), represents the most suitable method for preparation. Decoction allows for the extraction of a maximum of active principles and helps to mitigate or eliminate the toxicity of certain recipes. It also facilitates the homogeneous combination of multiple plants. Additionally, maceration and infusion also play a significant role in maximizing the extraction of active principles and therapeutic effects. Numerous studies have echoed similar approaches, including the ethnobotanical study conducted by Mehdioui and Kahoudji in 2007 among the riparian population of the Amsittène forest [16].
This emphasis on decoction aligns with the traditional practices of many cultures, where boiling plant materials in water is a common method for preparing herbal remedies. Decoction is valued for its ability to release active compounds from plant tissues, making them more readily available for absorption and exerting therapeutic effects. Moreover, the simplicity and accessibility of this method make it particularly suitable for traditional healers who may lack sophisticated equipment or resources for more complex extraction techniques.
Highlights
• Traditional medicine is widely used by Chadians, with more than 80% of the population relying on it, even in the capital city of Ndjamena.
• The study revealed a remarkable wealth of traditional knowledge in primary healthcare, highlighting the importance of plants in the local pharmacopoeia.
• The results obtained will be used by the Ministry of Health to create a positive list of plants to be recommended to the population for primary care.
Conclusion
In conclusion, this study is a source of information on not only the medicinal flora found around Chad’s capital, but also on the diseases treated by traditional healers and the population concerned. This study will serve as a basis for the development of improved traditional medicines for our populations.
Authors Contribution Statement
Abakar Bechir Seid: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Resources, Visualization, Writing – original draft.
Joseph Ngoupayo and Giulia Cappelli: Methodology, Validation. Bernard Gressier: Conceptualization, Writing.
Bruno ETO: Conceptualization, Data curation, Formal analysis, Methodology, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
A B Bechir, A B Mahamat, Ngameni Barthelemy: Investigation.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data Availability
Data will be made available on request.
Acknowledgements
The authors would like to thank the direction of Pharmacopeia and Traditional Medicine, Ministry of Health and Prevention, B.P. 440, N’djamena, Chad and TBC Laboratory (Faculty of Pharmacy, University of Lille) for assistance and helpful discussion.
References
- Regional Committee for Africa, 56. 2006. “Health research: program of action for the WHO African Region: report by the Regional Director”.
- Sofowara, A. (1993). Medicinal plants and traditional medicine in Africa Spectrum books LTD. Ibadan, Nigeria, 289.
- World Health Organization. (2013). WHO traditional medicine strategy: 2014-2023. World Health Organization.
- Bazin, F., Bechir, A. B., & Khamis, D. D. (2013). Etude prospective: systèmes d’élevage et changements climatiques au Tchad. Institut de recherches et d’applications des méthodes de développement, Rapport final.
- Jazy, M. A., Karim, S., Morou, B., Sanogo, R., & Mahamane,S. (2017). Enquête ethnobotanique auprès des tradipraticiens de Santé des régions de Niamey et Tillabéri au Niger: Données 2012–2017. Eur. Sci. J, 13, 276-304.
- Lakouéténé, D. P. B., Ndolngar, G., Berké, B., Moyen, J. M., KoshKomba, E., Zinga, I., ... & Chèze, C. (2009). Enquête ethnobotanique des plantes utilisées dans le traitement du paludisme à Bangui. Bull Soc Pharm Bord, 148, 123-38.
- Mahamane, H., Ardine, A. C., Ben Adam, M. A., Mamadou, G., Mahamadou, T., & Rokia, S. (2020). Enquête Ethnobotanique Des Plantes Utilisées Pour La Protection Cutanée Des Personnes Atteintes D’albinisme Dans Le District De Bamako (Mali) Et Analyse Qualitative De Bixa Orellana L.(Bixaceae). Bixaceae). Eur Sci J ESJ [Internet], 30.
- Abdoulaye, B., Bechir, A. B., & Mapongmetsem, P. M. (2017). Utilités socioéconomiques et culturelles du Balanites aegyptiaca (L.) Del.(Famille Zygophyllaceae) chez les populations locales de la Région du Ouaddaï au Tchad. Journal of Applied Biosciences, 111, 10854-10866.
- Koudokpon, H., Dougnon, V. T., Bankolé, H. S., Fah, L., Hounmanou, Y. M. G., Baba-Moussa, L., & Loko, F. (2017). Enquête ethnobotanique sur les plantes utilisées dans le traitement des infections au Sud-Bénin. Health Sciences and Disease, 18(2).
- Bentabet, N., Rajaa, R., & Sakina, N. (2022). Enquête ethnobotanique et inventaire des plantes médicinales utilisées dans le traitement des maladies dermatologiques dans la ville d’Ain Temouchent. Journal of applied Biosciences, 170(1), 17704-17719.
- Baggnian, I., Abdou, L., Yameogo, J. T., Moussa, I., & Adam,T. (2018). Étude ethnobotanique des plantes médicinales vendues sur les marchés du centre ouest du Niger. Journal of Applied Biosciences, 132, 13392-13403.
- Bruno, E. T. O. (2013). Research in clinical phytopharmacology to develop health care in developing countries: State of the art and perspectives. Phytopharmacol, 4(2), 149-205.
- Boutahiri, S., Bouhrim, M., Abidi, C., Mechchate, H., Alqahtani, A. S., Noman, O. M., ... & Eto, B. (2021). Antihyperglycemic effect of lavandula pedunculata: in vivo, in vitro and ex vivo approaches. Pharmaceutics, 13(12), 2019.
- Zakraoui, M., Outman, A., Kinambamba, M. S., Bouhrim, M., Ndjib, R. C., Alshawwa, S. Z., ... & Eto, B. (2024). Ifanosine: Olea europaea L. and Hyphaene thebaica L. combination, from traditional utilization to rational formulation: Preclinical and clinical efficacy on hypertensives patients. Journal of Ethnopharmacology, 325, 117834
- Dibong, S. D., Mpondo, E. M., Ngoye, A., Kwin, M. F., & Betti, J. L. (2011). Ethnobotany and phytomedicine of medicinal plants sold in Douala markets.
- Mehdioui, R., & Kahouadji, A. (2007). Etude ethnobotanique auprès de la population riveraine de la forêt d’Amsittène: cas de la Commune d’Imi n’Tlit (Province d’Essaouira). Bulletin de l’Institut scientifique, Rabat, section Sciences de la vie, 29, 11-20.