
Biomedical Science and Clinical Research(BSCR)
ISSN: 2835-7914 | DOI: 10.33140/BSCR
Impact Factor: 1.7


Short Article - (2025) Volume 4, Issue 2
Medical Equipment Technological Assessment at Fatebenefratelli-Sacco Hospital: an ad hoc Replacement Priority Index
2Humanitas Mirasole SpA, Milan, Italy
3Azienda Socio-Sanitaria Territoriale Fatebenefratelli Sacco, Via G.B.Grassi 74, Milan, Italy
4Polygon SpA c/o Azienza Socio-Sanitaria Territoriale Fatebenefratelli Sacco, Milan, Italy
Received Date: Mar 10, 2025 / Accepted Date: Apr 04, 2025 / Published Date: Apr 14, 2025
Copyright: ©Â©2025 Alessandro Grasso, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Grasso, A., Milani, E., Olivieri, P., Fornari, R., Orsi, G., et al. (2025). Medical Equipment Technological Assessment at Fatebenefratelli-Sacco Hospital: an ad hoc Replacement Priority Index. Biomed Sci Clin Res, 4(2), 01-10.
Abstract
The latest report of the Osservatorio Parco Installato (OPI) highlights the widespread state of obsolescence of electromedical equipment in Italy; in this context, Sacco hospital has implemented an internal strategy of management and evaluation of such equipment, in order to improve the planning of purchases, for greater profitability and efficiency of the service. The hospital has devised its own evaluation strategy for the installed park, developing an ad hoc model for multi- presidio public structures in which there is an outsourced management of the maintenance of electromedical equipment.
The model, based on the synergy between a technical Replacement Priority Index (RPI) and a clinical RPI, aims to be quickly upgradable and able to grasp the urgency of replacing an equipment based on the state of the others of the same type.
The strategy, given the heterogeneity of the group involved and the parameters analyzed, is based on the Multi-Criteria Decision Analysis (MCDA); the specific weights of the parameters have been assigned thanks to an internal survey in which the various industry experts have drawn up their ranking of importance of the parameters considered. The goal is therefore the search for total harmony between health and decision-making bodies, providing for the involvement of nurses, active engine of hospitals, and doctors, to outline a shared strategy of technological modernization and better use of the resources offered by the Piano Nazionale di Resistenza e Resilienza (PNRR) and D. lgs. 34/2020, next step of the project in progress.
Keywords
Clinical Engineering, Health Technology Assessment (HTA), Technology Management, Replacement Priority Index (RPI)
Highlights
- Evaluation of the technology functionality in the hospital, thanks to the development of a Replacement Priority Index
- Inclusion of all the professionals working in the hospital, taking into account nurses’ experience
- Data analysis and implementation of a structured strategy in terms of new technologies acquisition.
Introduction
Management and implementation of the maintenance of the electromedical equipment present in a healthcare facility are central activities of the Clinical Engineering Service, which can be contained in the expression "Technology Management" [1,2].
Moreover, in the post-pandemic period of Sars-Cov-2, the need for tools, increasingly oriented towards the world of information technology, to support and monitor the performance of the electromedical equipment for better hospital management has become more acute [3].
As confirmed by the latest report by Confindustria Dispositivi Medici in its Osservatorio Parco Installato (OPI), the medical instrumentation provided to healthcare companies in Italy is in a state of widespread antiquity and poor technological updating [4,5].
The main factors behind this phenomenon can be identified in the few funds reserved for health in recent years. Moreover, the system of "Reimbursement to Performance", based on the "Diagnosis Related Groups" (DRG), does not favor the modernization of the equipment and therefore this is reflected in an absence of innovation in the within of the public policies of purchase [6].
Then, management of electromedical equipment plays a more and more increasing role in ensuring the efficiency and safety requirements of a health care facility. It is necessary to provide for a timely monitoring of the state of the equipment in the hospital, in order to have the most in-depth view of technological adequacy [7].
Hospital decision-makers must therefore be supported by robust tools to understand what the plans for replacing equipment in facilities should be. These tools must be based on real data, structured, and validated by experience [8].
Several strategies have been spread on a global scale to develop Replacement Priority Index (RPI) to determine what should be the choices in terms of investment in technology. The first recognized work about an objective management strategy of electromedical equipment replacements is due to Fennigkoh [9].
In 1992, the author developed a RPI model that still represents the basis for the implementation of innovative algorithms. The index is based on seven evaluation parameters for each device, each with its respective weight.
Since then, there has been an increasing tendency for health agencies to use such tools; therefore, 41 related articles from PubMed or Scopus have been investigated.
The large majority of the RPIs only implements technical parameters but in a study in addition to the change of some parameters, scores and weights, an evaluation of the equipment is introduced with an RPI not unique, but divided into two indices, one technical and one subjective of clinical opinion [10].
It has been shown that the use of multidimensional criteria produces more efficient and relevant evaluation mechanisms for electromedical equipment [11,12].
The most widespread method to assess the need for replacement of electromedical equipment is the Analytical Hierarchy Process (AHP), a methodology to address multi-critical issues, able to operate with both quantitative and qualitative data [13].
Starting from this background, a study was developed at the hospital Fatebenefratelli-Sacco in Milan, aiming to implement a tool capable of capturing the urgency of replacement for electromedical equipment, in order to be able to monitor their functional status in real time. It provides a strategy based on data from Fatebenefratelli-Sacco Hospital and it has the goal to build a strong technology management instrument based on its specific needs, but it is easily adaptable to other public facilities in the Lombardy region. The ultimate purpose of this research is to implement thoughtful choices in terms of investment and purchasing, to optimize the use of resources; therefore, once identified the major issues, a purchase plan has been elaborated for the resolution of the main issues present in the hospital.
Materials and Methods
This project is based on the implementation of a priority replacement index (RPI) that, although it is based on a careful analysis of the literature available on the subject, departs from it in relation to the needs of the Hospital. The model of inspiration is the RPI developed by Eng. Elena Milani at Humanitas Mirasole SpA, which is shown in table 1. [14].
The index consists of 10 indicators and is characterized by both objective and subjective parameters, such as technical adequacy and clinical fitness [15].
Therefore, although there is no real conception of an RPI based on the opinion of users, the author entering these subjective parameters opens the way to strategies that integrate objective assessments with those of health professionals. It is arranged in a "fuzzy logic", a recent methodology which is part of the Multi Criteria Decision Analysis techniques and allows to expand the "yes/no" duality of the Fennigkoh model, allowing the use of intermediate scores [16].
From this theory, the subdivision of the values that the various parameters can assume has been resumed; in fact, each of it is worth 0, 0.5 or 1. The use of three ranges to evaluate the parameters makes mathematical processing easier and allows a robust analysis of the different levels of criticality that a device can show in a specific evaluation criterion [17].
|
METRIC |
PARAMETER DESCRIPTION |
ASSUMED VALUE |
NOTES |
|
X1 |
AGE |
0; 0,5; 1 |
ASSIGNED WRT AN AVERAGE THRESHOLD VALUE OF THE CLASS |
|
X2 |
FUNCTIONAL STATUS |
0; 0,5; 1 |
|
|
X3 |
SPARE PARTS AVAILABILITY |
0; 1 |
|
|
X4 |
DEGREE OF USE |
0; 0,5; 1 |
|
|
X5 |
CRITICALITY |
0; 0,5; 1 |
|
|
X6 |
RELIABILITY |
0; 0,5; 1 |
ASSIGNED WRT AN AVERAGE THRESHOLD VALUE OF THE CLASS |
|
X7 |
AVAILABILITY |
0; 0,5; 1 |
ASSIGNED WRT AN AVERAGE THRESHOLD VALUE OF THE CLASS |
|
X8 |
CLINICAL FITNESS |
0; 0,5; 1 |
|
|
X9 |
TECHNICAL ADEQUACY |
0; 0,5; 1 |
|
|
X10 |
MAINTENANCE COST |
0; 0,5; 1 |
ASSIGNED WRT AN AVERAGE THRESHOLD VALUE OF THE CLASS |
Table 1: RPI by Milani [14]
Thresholds have been attributed since the historical of the maintenance interventions and the strategic choices undertaken within the structure to create an ad hoc model.
Milani’s research already assigns different importance to each criterion in the calculation of the RPI, depending on the strategic choices of the management, making it possible to shift the focus to the indicators deemed most relevant.
The proposed index at Fatebenefratelli-Sacco consists of two distinct parts: first, an index has been created called internally "Technical" RPI, resulting from the weighted sum of technical parameters. This first construct serves as a filter for the identification of the equipment on which it is necessary to place an additional focus for the evaluation of the substitution. To implement an effective replacement plan and thus make proper use of the resources to purchase the necessary equipment, the second step of the work is focused on the direct involvement of users, namely medical and nursing professionals, to calculate the “Clinical” RPI. In this regard, a questionnaire was created to be submitted to employees to prioritize the urgency of renewal of equipment based on actual work activity and the perception of users constantly in contact with technology. The starting point for the analysis is the CosWin portal. It represents the Computerized Maintenance Management System (CMMS) at the Hospital, from which the necessary information about the equipment has been extracted. It has been provided by the Global Service, the external company that provides the service of management and maintenance of electromedical equipment and collects data about the medical devices in dowry to the hospital. In addition, another feature of CosWin is the ability to store inside the historical maintenance carried out on the fleet. All the data of interest, related to the equipment registry and maintenance carried out in the last year, have been extrapolated and unified on an Excel spreadsheet. This calculation tool allowed to determine at first the Technical IPS, which was then implemented on the company CMMS, as the call for the award of the service for the management and maintenance of medical equipment places the obligation on the part of the Global Service to make available to the institution such a tool.
Table 2 shows the parameters included in the calculation of the Technical IPS and the respective weights. The age of the equipment and the possible unavailability of spare parts or technical assistance by the manufacturer in case of failure (EoS) were evaluated. Then, the number of annual corrective maintenance interventions and the resulting derived downtime were counted. As noted above, the acceptability threshold was defined on the average values of these criteria on the homogeneous cohort installed at the Hospital. A critical parameter has been inserted referring to what was defined in the call for the management and maintenance of electromedical equipment organized by ARIA S.p.A., which establishes a specific first intervention time per type of equipment according to the criticality threshold assigned during the award of the tender. A first step is implemented by calculating an IPS for each equipment considering these indicators. At this point, the algorithm inserts a sixth parameter. It evaluates the number of devices of the same type working in a department. In fact, the number of equipment needed for each department of the hospital has been defined through comparison with the departments and the creation of "standard equipment" for the type of service offered. Therefore, the amount of equipment with IPS below the threshold defined as the necessary replacement alert is considered and, based on the comparison with the number set as standard, the technical IPS is recalculated [18].
|
TECHNICAL IPS CRITERIA |
WEIGHT 1° STEP |
WEIGHT 2° STEP |
|
AGE |
0.17 |
0.13 |
|
END OF SUPPORT (EoS) |
0.19 |
0.15 |
|
CRITICALITY |
0.23 |
0.20 |
|
AFFIDABILITY |
0.20 |
0.16 |
|
UPTIME |
0.21 |
0.17 |
|
PRESENCE OF OTHER EQUIPMENT OPERATING IN THE SAME DEPARTMENT |
/ |
0.19 |
Table 2: Technical RPI
Once the technical IPS has been calculated, the focus is only on equipment with an above-threshold value. For these, the Clinical IPS is calculated, consisting of the parameters in Table 3;parameters chosen on the basis of the result of the administration of an ad hoc questionnaire to healthcare professionals [19].
|
CLINICAL IPS CRITERIA |
WEIGHT |
|
DEGREE OF RISK DERIVED ON THE PATIENT/OPERATOR |
0.19 |
|
FREQUENCY OF USE |
0.10 |
|
FUNCTIONAL STATUS |
0.08 |
|
CLINICAL ADEQUACY |
0.23 |
|
FAILURE CAUSED BY THE ABSENCE OF THE DEVICE |
0.10 |
|
LEVEL OF TRAINING BY OPERATORS |
0.06 |
|
DEGREE OF TECHNOLOGICAL INNOVATION |
0.11 |
|
AVAILABILITY OF OTHER ALTERNATIVE EQUIPMENT |
0.13 |
Table 3: Clinical RPI
The weights are assigned to obtain criteria of relative importance that fully reflect the structure.
Definition of these weights was implemented following the operating mode adopted by the Lombardy Region for the Regional Health Technology Assessment model, collecting expert opinion on the relative importance of the various criteria [20].
The definition of acceptability thresholds for RPI was also fundamental, inspired by Armisi’s model [16]. This is the adopted RPI scale:
0.5: the equipment does not need intervention.
0.5 0.7: the equipment must be monitored in the short.
0.7: the equipment needs urgent replacement. It was decided to outline the final ranking as the weighted sum of the two indices, assigning a slightly greater coefficient to the Technical IPS. In this way, it is possible to reduce any biases due to the willingness of clinicians to replace equipment even if not strictly necessary [21].

Results
Once the calculation algorithm was implemented, it was used to define the technical IPS value of all equipment installed at the ASST.
In Figure 1, the number of equipment showing a certain value of Technical RPI is shown. To sum up, as can be observed from Figure 2, out of a total of 18.614 equipment, 925 should be further investigated. Of these, 91 are in urgent need of replacement.
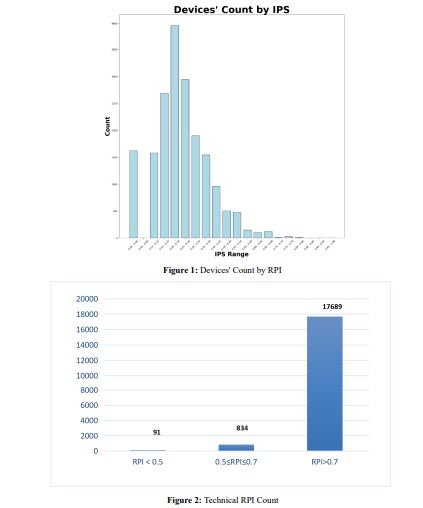
An analysis of the various departments was carried out in order to take a picture of the most critical conditions. Figure 3 shows theresults of this analysis, with the percentage of equipment that have a technical RPI to be discussed.
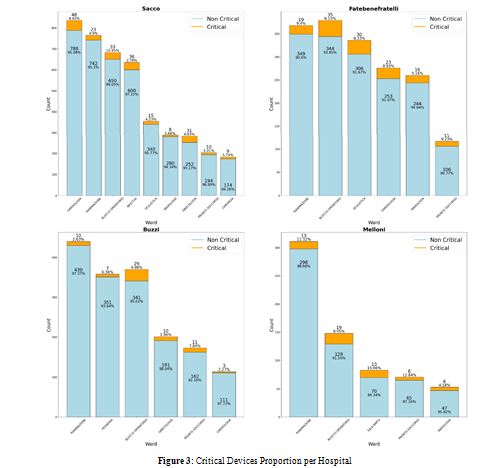
Each column represents the number of devices present in the hospital ward; those that have an RPI above threshold have been highlighted. In Figure 4, the number of equipment belonging to each criticality class has been counted for each criterion to understand what are the factors that cause the most urgent replacement.
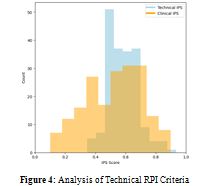
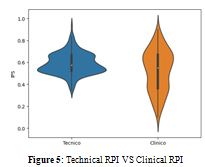
Once the technical RPI had been calculated for all equipment, interviews were organized to validate the model, with the aim of gaining a complete view of the installed fleet and thus being able to draw up the renewal strategy. Thirty-eight departments were questioned for a total of 211 questionnaires collected for 258 devicesIn Figure 5, the comparison between Clinical RPI and Technical RPI is represented, in which it can be noticed a prevalent leptokurtosis of the Technical RPI, against the evident platikurtosis of the Clinical one, which is therefore reflected in a greater variance in the distribution.
One of the most visible results, which demonstrates the achievement of the goal set, is found in the fact that the Clinical RPI effectively acts as an additional filter to be able to make the best use of economic resources and not invest in equipment notstrictly necessary. To this end, a violin plot is reported in Figure 6, for 258 devices subjected to Clinical RPI, demonstrating the filter role of the latter instrument.
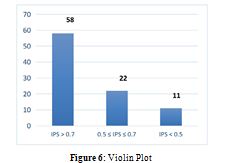
For the 91 devices whose Technical RPI value required urgent replacement, it was calculated for all Clinical IPS. For 58 of them, the Clinical RPI confirmed the urgency of substitution, for 22 reported a value of attention and for the remaining 11 it emergedthat substitution is not actually necessary.
In Table 4, you see the ranking obtained after the weighted sum of the two RPI.
|
EQUIPMENT NUMBER |
DESCRIPTION |
HOSPITAL CODE |
WARD |
TOT RPI |
|
0001954 |
LAVAPADELLE |
SACCO |
GENERAL SURGERY |
0.94 |
|
0002373 |
MICROSCOPIO OTTICO |
FBF |
MICROBIOLOGY |
0.88 |
|
0001245 |
ECOTOMOGRAFO |
SACCO |
CARDIOLOGY |
0.86 |
|
0003628 |
LETTO DA PARTO |
MELLONI |
DELIVERY ROOM |
0.84 |
|
0003803 |
LETTO DA PARTO |
SACCO |
DELIVERY ROOM |
0.83 |
|
0001018 |
DEFIBRILLATORE |
MELLONI |
GYNAECOLOGY |
0.81 |
|
0002410 |
DEFIBRILLATORE |
FBF |
NEPHROLOGY |
0.78 |
|
0017825 |
ARTROSCOPIO |
FBF |
SURGERY ROOM |
0.78 |
|
0004016 |
TRAVE TESTALETTO |
BUZZI |
EMERGENCY |
0.78 |
|
0015407 |
CENTRALE MONITORAGGIO |
SACCO |
PAEDIATRICS |
0.77 |
|
0001110 |
DEFIBRILLATORE |
MELLONI |
GYNAECOLOGY |
0.75 |
|
0004007 |
TRAVE TESTALETTO |
SACCO |
EMERGENCY |
0.74 |
|
0004008 |
TRAVE TESTALETTO |
SACCO |
EMERGENCY |
0.74 |
|
0004009 |
TRAVE TESTALETTO |
SACCO |
EMERGENCY |
0.74 |
|
0003656 |
AUTOCLAVE |
BUZZI |
DELIVERY ROOM |
0.74 |
|
0014200 |
SPETTROFOTOMETRO |
FBF |
PATHOLOGICAL ANATOMY |
0.74 |
|
0003801 |
LETTO DA PARTO |
SACCO |
DELIVERY ROOM |
0.72 |
Table 4: Total RPI
Discussion
The purpose of this paper is to illustrate the strategies undertaken regarding the objective planning of investments and purchases of medical equipment, in order to ensure an increasingly profitable efficiency and safety of the service. The goal is therefore the search for total harmony between health and decision-making bodies, providing for the involvement of nurses and clinicians to outline a shared strategy of technological modernization and better use of the resources offered by the Piano Nazionale di Resistenza e Resilienza (PNRR) [22].
In the total conviction that only the communion of intentions can lead to the achievement of valuable goals, the common guideline of the Management is the search of ad hoc models for the hospital, that therefore they are not simply a valid contribution to the scientific research but useful to the Company and shared by all the actors involved in the operating processes.
In order to do this, the described RPI was developed, and it was possible to build improvement strategies for the installed park, to act in a structured way and therefore make the best use of the available resources and ensure greater safety of the service [23].
The results show how the instrument can capture the urgency of replacing an electromedical device, through a multicriterial tool and using a multidisciplinary approach.
As proof of the study conducted by Confindustria Medical Devices, it can be noted that also in the Fatebenefratelli Sacco hospital the problem of the age of the instrumentation is evident. In fact, as demonstrated before, it is evident the large number of devices with an advanced age [4].
As shown in Figure 7, from the interviews with the departments, it has emerged as the Technical RPI is able to define what are the equipment to be replaced.
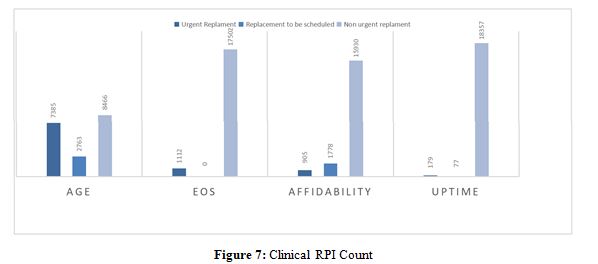
From the results, most of the critical equipment for Technical IPS has also been evaluated by clinicians as a necessary replacement. However, as the present work wanted to demonstrate, some of the equipment was instead excluded from the urgent replacement plan since, although no longer suitable for clinical practice, it is not used in the department or net of outdated and out-of-support communication, it continues to work in compliance with safety requirements and therefore, it is not a priority for staff to have an immediate alternative.
The implemented index has also found practical application in one of the major projects in place at the hospital, namely the construction of the New Buzzi Children’s Hospital, next to the homonymous structure in Milan.
The role of Clinical Engineering was to define the equipment to be in the departments, in order to estimate the necessary resources and provide the request for funding to the Lombardy Region. In this sense, a model has been applied according to which, at first defined a set of basic equipment for each department, then integrated by those specific to each department and a group of generic devices with low technological complexity.
The study in being introduces some criticalities, dictated in the first place from the difficulty in finding all the necessary data to the implementation of the index. In fact, due to the alternation of 3 different Global Services in a few years and the consequent change of CMMS used, the master shows some holes. The lack of data or the incomplete availability of all the necessary information can sometimes result in an erroneous assessment of the urgency of replacement; also, for this reason, the idea of integrating technical IPS with an evaluation by clinicians has matured.
The introduction of a subjective questionnaire, although of functional value, may lead to inaccuracies; operators may answer questions negatively and thus raise the value of the RPI more than the true value. For this reason, it was deemed appropriate to give a somewhat less specific weight to the clinical RPI to alleviate the bias between subjectivity and objectivity [24].
By making a comparison with the literature, the attention to the clinical opinion, gives the RPI a strong identity character compared to the structure where it is implemented [25,26].
More generally, the technical parameters are in line with the references, in order to ensure consistency to the model using criteria already widely validated. However, a novelty factor is the emergence of a criticality when the number of tools in a department is reduced compared to the use and evaluation of threshold based on the maintenance statistics of the specific structure.
Conclusion
The implemented model has allowed the company to have a tool to support to the Clinical Engineering for the definition of the substitution plan of the installed park, guaranteeing a greater objectivity and allowing to monitor the equipment in real time.
As demonstrated, the developed model has led to the definition of a massive strategy of technological renewal, providing for the replacement of most of the equipment with a high degree of functional criticality, laying the foundation for future actions [27].
Moreover, it was felt necessary to give the end-users a voice, believing firmly in their professionalism and their ability to weigh subjective evaluation for the greater good of the patient.
References
1. Lumbers, M. (2018). Approaches to leadership and managing change in the NHS. British Journal of Nursing, 27(10), 554- 558.
2. Grasso, A., Cimolin, V., Orsi, G., Olivieri, P., Milani, E., Scazzina, B., & Fornari, R. (2024). Medical Equipment Technological Assessment at Fatebenefratelli-Sacco Hospital: an ad hoc Replacement Priority Index.
3. Arabi, Y. M., Azoulay, E., Al-Dorzi, H. M., Phua, J., Salluh, J., Binnie, A., ... & Citerio, G. (2021). How the COVID-19 pandemic will change the future of critical care. Intensive care medicine, 47, 282-291.
4. Confindustria Dispositivi Medici (2023) Osservatorio parco installato.
5. Ministero Della Salute (2017) Rilevazione per il monitoraggio delle apparecchiature sanitarie: Linee guida per il monitoraggio del sistema apparecchiature sanitarie.
6. Coppola, V. (1999). Criteri per pianificare il rinnovamento delle apparecchiature. Radiol Med, 1-9.
7. Zamzam, A. H., Al-Ani, A. K. I., Wahab, A. K. A., Lai, K. W., Satapathy, S. C., Khalil, A., ... & Hasikin, K. (2021). Prioritisation assessment and robust predictive system for medical equipment: a comprehensive strategic maintenance management. Frontiers in Public Health, 9, 782203.
8. Faisal, M., & Sharawi, A. (2015). Prioritize medical equipment replacement using analytical hierarchy process. IOSR Journal of Electrical and Electronics Engineering, 10(3), 55-63.
9. Fennigkoh, L. A. R. R. Y. (1992). A medical equipment replacement model. journal Of Clinical engineering, 17(1), 43-47.
10. Maggi, N., Adornetto, A., Scillieri, S., Urbina, E. N. B., Ruggiero, C., & Giacomini, M. (2019). Medical equipment replacement prioritisation: A comparison between linear and fuzzy system models. In MEDINFO 2019: Health and Wellbeing e-Networks for All (pp. 1538-1539). IOS Press.
11. Mora-García, T., Piña-Quintero, F., & Ortiz-Posadas, M. (2018). Medical equipment replacement prioritization indicator using multi-criteria decision analysis. In Progress in Artificial Intelligence and Pattern Recognition: 6th International Workshop, IWAIPR 2018, Havana, Cuba, September 24–26, 2018, Proceedings 6 (pp. 271-279). Springer International Publishing.
12. Dondelinger, R. M. (2004). A complex method of equipment replacement planning: an advanced plan for the replacement of medical equipment. Biomedical instrumentation & technology, 38(1), 26-31.
13. Capuano, M. (2010). Prioritizing Equipment for Replacement: A plan based on data not perception. Biomedical instrumentation & technology, 44(2), 100-109.
14. Milani, E., Oliva, P., Mirabella, C., & Griziotti, M. (2018). IPS e KPI: Best practice integrate nel technology management. Healt Technol Chall AIIC.
15. David, Y., & Jahnke, E. G. (2004). Planning hospital medical technology management. IEEE Engineering in medicine and biology magazine, 23(3), 73-79.
16. Armisi, L., Trombetta, C., Gatti, D., & Rosato, N. (2013). Elaborazione di un indice di priorità di sostituzione per apparecchiature elettromedicali. Tec Osp Tecnol Obiett Efic,
42-46.
17. Saleh, N., Rosati, S., Sharawi, A., Wahed, M. A., & Balestra, G. (2014, December). Application of quality function deployment and genetic algorithm for replacement of medical equipment. In 2014 Cairo International Biomedical Engineering Conference (CIBEC) (pp. 91-94). IEEE.
18. Chiara, C., Andrea, B., Buizza, A., & Giuseppe, G. (2001). A new model for the replacement priority value of medical equipment. In IFMBE Proceedings-Medicon 2001 (Vol. 1, pp. 183-186). IFMBE, FER, CROMBES.
19. Ewertsson, M., Gustafsson, M., Blomberg, K., Holmström, I. K., & Allvin, R. (2015). Use of technical skills and medical devices among new registered nurses: a questionnaire study. Nurse education today, 35(12), 1169-1174.
20. Radaelli, G., Lettieri, E., Masella, C., Merlino, L., Strada, A., & Tringali, M. (2014). Implementation of EUnetHTA core Model® in Lombardia: the VTS framework. International Journal of Technology Assessment in Health Care, 30(1), 105- 112.
21. Nobre, F. F., Trotta, L. T. F., & Gomes, L. F. A. M. (1999). Multiâ?criteria decision making–an approach to setting priorities in health care. Statistics in medicine, 18(23), 3345- 3354.
22. Salute MD (2024) Ammodernamento del parco tecnologico e digitale ospedaliero.
23. Leoni M, Paparella M, Solvi S, Franzoni C (2020) Sanità stremata dal covid, ecco le azioni digitali che non possiamo più rinviare. Agenda Digitale.
24. Taylor, K., & Jackson, S. (2005). A medical equipment replacement score system. Journal of Clinical Engineering, 30(1), 37-41.
25. Osman, A. M., Al-Atabany, W. I., Saleh, N. S., & El-Deib, A. M. (2018, December). Decision support system for medical equipment failure analysis. In 2018 9th Cairo International Biomedical Engineering Conference (CIBEC) (pp. 94-97). IEEE.
26. Alvarado, M. A., & Rocha, S. L. (2018, May). Development of methodology of evaluation for medical equipment replacement for developing countries. In World Congress on Medical Physics and Biomedical Engineering 2018: June 3-8, 2018, Prague, Czech Republic (Vol. 3) (pp. 383-386). Singapore: Springer Singapore.
27. Bologna, F., Perilongo, G., Mennini, F. S., Scarpa, M., & Silvano, G. (Eds.). (2024). Malattie rare: Una sfida tra passato e futuro. Gius. Laterza & Figli Spa.