
Journal of Neuro and Spine(JNS)
ISSN: 2836-5968 | DOI: 10.33140/JNS

Case Report - (2024) Volume 2, Issue 2
Management of Spinal Cord Cavernous Malformation: A Case Report
2Department of Neurosurgery, Hopital des Specialites, Faculty of Medicine and Pharmacy, Mohammed V University, Rabat, Morocco
Received Date: Jun 24, 2024 / Accepted Date: Jul 22, 2024 / Published Date: Jul 23, 2024
Copyright: ©©2024 Yao Christian Hugues Dokponou, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Mohcine, S., El Kacemi, I., Dokponou, Y. C. H., Obame, F. O., El Asri, C., et al. (2024). Management of Spinal Cord Cavernous Malformation: A Case Report. J Neuro Spine, 2(2), 01-04.
Abstract
Cavernomas of the spinal cord are a group of abnormal capillaries without an interlayer of nerve tissue. This vascular malformation is rare and rarely localized in the spinal cord. Their heterogeneous symptoms range from asymptomatic forms to acute or progressive forms with fatal consequences. The radiological diagnosis is based on a spinal MRI. Surgery represents the basis for its management. We report the case of an intramedullary cavernoma in a 43-year-old patient admitted for cervical pain associated with left cervico-brachial neuralgia. MRI revealed intramedullary cav- ernomas at C5–C6. In this case report, we report the surgical management and discuss the clinical and radiological features of this unusual intramedullary malformation. We anticipate that this case report adds to the existing literature on this topic.
Keywords
Cavernous, Spinal Cord, Vascular Malformation, MRI, SurgeryIntroduction
Cavernomas are a group of abnormal capillaries with no intervening nerve tissue. This vascular malformation occurs frequently in the brain; its prevalence is 0.5% [1,3]. Familial forms account for 10%, while spinal cord cavernomas (SCCMs) are rare, accounting for only 5% of all cavernomas [1,2]. These malformations have a slow flow and a lower risk of rupture compared to the other vascular malformations. Their symptoms are heterogeneous and range from asymptomatic forms to acute or progressive forms. The radiological diagnosis is based on a spinal MRI. We report this case of a 43-year-old patient successfully treated by surgical resection.
Case Presentation
A 43-year-old patient with no significant medical history was admitted with cervical pain of 8 months duration, recently complicated by left cervical neuralgia in the C6 dermatome with paresthesia and numbness in the same area, but without sphincter disorders nor weight loss or fever. Physical examination revealed no neurological deficit and shoulder examination revealed no abnormalities. Spinal MR imaging showed an intramedullary lesion widening the cervical spinal cord at C5-C6, with a popcorn sign and heterogeneous signal on T1- and T2-weighted images, surrounded by a hypointense ring in all sequences (Figure 1), especially in gradient echo, which represents hemosiderin. Susceptibility-weighted imaging shows hypointense lesions, without adjacent intramedullary hemorrhage and contrast enhancement. The diagnosis of cervical medullary cavernoma was confirmed and the patient underwent surgery via a posterior approach to the cervical spine with complete removal of the cavernoma (Figure 2). Postoperative follow-up was easy, except for transient quadriparesis, which disappeared within a few days with physical rehabilitation. The follow-up MRI was satisfactory (Figure 3)


Figure 1: Pre-operative Cervical Spinal MRI showing the C5-C6 Cavernoma
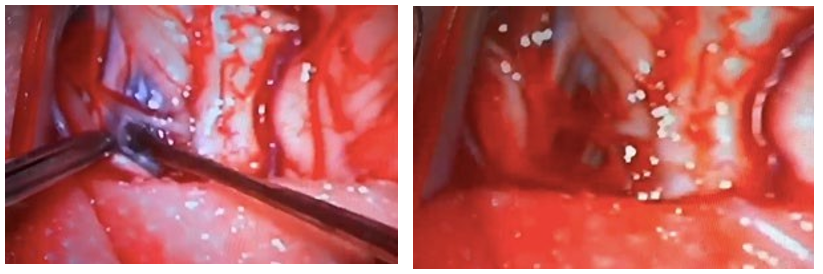
Figure 2: Operative view of the Cervical Spine Cavernoma Resection
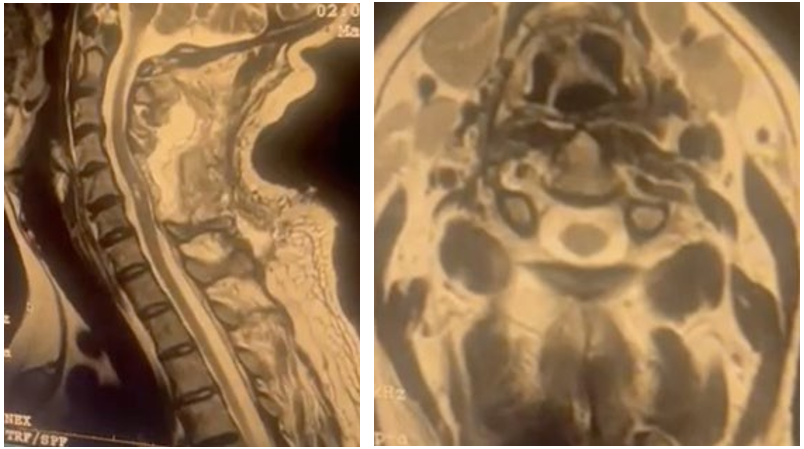
Figure 3: Post-operative Cervical Spinal MRI showing the Total Resection of the Cavernoma
Discussion
Cavernomas are groups of abnormal capillaries without intervening nervous tissue that occur in the brain and/or spinal cord [1]. They form large “caves” of slow-flowing blood. Cavernomas resemble a raspberry in appearance and can increase in size from a few millimeters to several centimeters over time. It can occur anywhere in the brain and spinal cord. The blood vessel walls in cavernomas are weak and thin and can cause bleeding [3]. The hemorrhage or cavernoma volume can damage the surrounding spinal cord tissue and cause ongoing neurological problems. Spinal cavernomas are histologically identical to those in the brain, most commonly intramedullary and rarely epidural [4]. These lesions consist of dilated venous canals without intervening normal nerve tissue.
Medullary cavernomas are rare, with an estimated frequency of 5% of all cavernomas in adults and 1% in pediatric series. The average age at onset of symptoms is 40 years, with a predominance of women and a sex ratio of 2:1. The frequency of familial forms is estimated at 10% and, in contrast to sporadic forms, is characterized by the presence of multiple lesions. Therefore, the presence of multiple lesions, even in the absence of a family history, should prompt the doctor to investigate a familial form.
Furthermore, we identify heterozygous loss-of-function mutations in the CCM1/KRIT1, CCM2/MGC4607, and CCM3/ PDCD10 genes in approximately 90% of familial cases of CCMs and two-thirds of sporadic cases with multiple lesions [1,5]. The annual risk of bleeding is approximately 2 to 3%; in the case of bleeding cavernomas, the risk of rebleeding is 9 to 10% [6]. The most common symptoms are motor and sensory deficits (58 to 61%), pain (34%), urinary and/or bowel dysfunction (24%), and respiratory insufficiency (0.5%) with involvement of the upper cervical spinal cord [7]. Spinal MRI is the key examination for diagnosing cavernoma; It is not pathognomonic but highly suggestive, showing a central heterogeneous area, a mixture of predominant hyperintensity (corresponding to methemoglobin, indicating recent hemorrhage) and hypointensity (fibrosis -calcifications) with a peripheral hypointense ring (corresponding to hemosiderin, the final degradation product of hemoglobin) [8].
The differential diagnosis may include thrombosed arteriovenous malformation (AVM), telangiectasia, or hemangioblastoma. On the other hand, angiography is rarely used because cavernomas are angiographically hidden, but gadolinium injection helps to distinguish between hemorrhagic intramedullary tumors and cavernomas [8]. For symptomatic cavernomas, especially in the early stages, treatment is surgical and includes laminectomy focusing on the pathological level, opening of the dura mater, evacuation of the hematoma, and removal of the entire lesion under the operating microscope [9]. Gross et al. in their study recommend removal of exophytic lesions regardless of clinical presentation, monitoring of asymptomatic deep lesions, and surgical intervention for symptomatic deep lesions only if symptoms are severe or progressive [10]. Furthermore, a retrospective study suggests that earlier (usually within 3 months of symptom duration) surgical resection may generally lead to a better prognosis [11-13].
Conclusion
Cavernomas of the spinal cord are rare vascular malformations with heterogeneous symptoms. Diagnosis is based on MRI and treatment is surgical, especially in symptomatic patients. Cohort analyses are desirable to understand the various management of these malformations and improve their outcomes.
Disclosures
The authors have nothing to disclose.
Funding
No funding was received for this research.
Conflict(s) of Interest
The authors report no conflicts of interest.
Acknowledgments
None
Authors' Contributions
Yao Christian Hugues Dokponou: Conceptualization, writing draft, reviewing and editing, visualization, supervision, validation, methodology.
Salami Mohcine: Writing, review & editing.
Fresnel Ontsi Obame: Writing, review & editing.
Inas El Kacemi: Writing & editing.
Abad Cherif El Asri: Writing & editing.
Miloud Gazzaz: Supervision, Validation, & review.
References
- Izi, Z., El Haddad, S., Allali, N., & Chat, L. (2023). Spinal Cord Cavernous Malformation: A Case Report. Global Pediatric Health, 10, 2333794X231184317.
- Zafar, A., Quadri, S. A., Farooqui, M., Ikram, A., Robinson, M., Hart, B. L., ... & Morrison, L. (2019). Familial cerebral cavernous malformations. Stroke, 50(5), 1294-1301.
- Cantore, G., Delfini, R., Cervoni, L., Innocenzi, G., & Orlando, E. R. (1995). Intramedullary cavernous angiomas of the spinal cord: report of six cases. Surgical neurology, 43(5), 448-452.
- Merello, E., Pavanello, M., Consales, A., Mascelli, S., Raso, A., Accogli, A., ... & De Marco, P. (2016). Genetic screening of pediatric cavernous malformations. Journal of Molecular Neuroscience, 60, 232-238.
- Ren, J., Hong, T., He, C., Sun, L., Li, X., Ma, Y., ... &Zhang, H. (2019). Coexistence of intracranial and spinal cord cavernous malformations predict aggressive clinical presentation. Frontiers in Neurology, 10, 618.
- Lonjon M, Gavotto A. revue de la neurochirurgie, mai 2020. [Google Scholar]
- Clark, A. J., Wang, D. D., & Lawton, M. T. (2017). Spinal cavernous malformations. Handbook of clinical neurology, 143, 303-308.
- Fiani, B., Reardon, T., Jenkins, R., Covarrubias, C., Sekhon, M., Soula, M., & Kortz, M. (2020). Intramedullary spinal cord cavernous malformations in the pediatric population.Surgical Neurology International, 11.
- Canavero, S. (1993). Intramedullary cavernous angiomas of the spinal cord: clinical presentation, pathological features, and surgical management. Neurosurgery, 32(4), 693-694.
- Gross, B. A., Du, R., Popp, A. J., & Day, A. L. (2010).Intramedullary spinal cord cavernous malformations.Neurosurgical focus, 29(3), E14.
- Liao, D., Wang, R., Shan, B., & Chen, H. (2023). Surgical outcomes of spinal cavernous malformations: A retrospective study of 98 patients. Frontiers in Surgery, 9,1075276.
- Asimakidou, E., Meszaros, L. T., Anestis, D. M., & Tsitsopoulos, P. P. (2022). A systematic review on the outcome of intramedullary spinal cord cavernous malformations. European Spine Journal, 31(11), 3119-3129.
- Rauschenbach, L., Santos, A. N., Engel, A., Olbrich, A., Benet, A., Li, Y., ... & Dammann, P. (2023). Functional neurological outcome of spinal cavernous malformation surgery. European Spine Journal, 32(5), 1714-1720.