



Case Report - (2016) Volume 1, Issue 1
Management of Resistant Pericarditis in an End Stage Renal Disease Patient: Case Presentation
2St George’s, University of London, London, UK
3Leviev Heart Center, The Chaim Sheba Medical Center at Tel HaShomer, Israel
4Management, The Chaim Sheba Medical Center at Tel HaShome, Israel
5Sackler School of Medicine, Tel-Aviv University, Israel
Received Date: Oct 15, 2016 / Accepted Date: Oct 27, 2016 / Published Date: Nov 01, 2016
Copyright: ©Lotan D, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
A 75 year old female receiving dialysis 3 times weekly due to end-stage renal disease (ESRD), secondary to polycystic kidney disease, presented to the emergency room. She complained of right upper quadrant pain together with pleuritic chest pain. The chest pain worsened on deep inspiration and on lying down flat, but improved on sitting up and bending forwards. An abdominal ultrasound, performed due to a known liver cyst, revealed a solid dense lesion, which was not indicative of a cyst. There was the suspicion that the lesion may have been infectious or hemorrhagic in nature. As a result the patient was admitted to the surgical department for further evaluation. Due to her failure to respond to antibiotic treatment a PET-CT with F-18-FDG was ordered. The studies revealed increased mediastinal absorption between her large vessels and pericardium as well as a small pericardial effusion. Her serum CRP peak was 236.83 mg/l, the troponin was negative and her blood urea was 42 mg/dl (15-45 mg/dl). The ECG did not show any typical changes of pericarditis.
Case Presentation
A 75 year old female receiving dialysis 3 times weekly due to end-stage renal disease (ESRD), secondary to polycystic kidney disease, presented to the emergency room. She complained of right upper quadrant pain together with pleuritic chest pain. The chest pain worsened on deep inspiration and on lying down flat, but improved on sitting up and bending forwards. An abdominal ultrasound, performed due to a known liver cyst, revealed a solid dense lesion, which was not indicative of a cyst. There was the suspicion that the lesion may have been infectious or hemorrhagic in nature. As a result the patient was admitted to the surgical department for further evaluation. Due to her failure to respond to antibiotic treatment a PET-CT with F-18-FDG was ordered. The studies revealed increased mediastinal absorption between her large vessels and pericardium as well as a small pericardial effusion. Her serum CRP peak was 236.83 mg/l, the troponin was negative and her blood urea was 42 mg/dl (15-45 mg/dl). The ECG did not show any typical changes of pericarditis.
However, treatment for pericarditis was initiated. Due to her ESRD she was started on prednisone, which had an immediate symptomatic and laboratory response. Her CRP declined to 5.1 and a tapering protocol of prednisone was initiated.
A week after the protocol was completed she complained of chest pain resembling pericarditis, her blood urea was 45.83 mg/dl (pre- dialysis) and CRP was over >400 mg/l. Her echocardiography showed normal ejection fraction with preserved valves and heart walls. The pericardium showed consistent signs of an ongoing inflammatory process leading to the diagnosis of: flare of acute pericarditis. As a result, prednisone and colchicine were initiated, and again, there was an immediate response and resolution of symptoms. This time a slower corticosteroid tapering protocol was used, however, 2 months into the treatment, while on 8 mg of prednisone, she suffered from a second flare of pericarditis. This was resolved by increasing the prednisone to 20 mg SID.
Due to the resistant nature of the pericarditis and failure of the prednisone treatment, a third line therapy was initiated. The patient was put on azathioprine 25 mg BID and colchicine 0.5 mg SID and the slow corticosteroid tapering protocol was re-started.
Three weeks into this last treatment plan the patient was admitted to the internal medicine department with central line-associated bloodstream Infection. It was managed with the removal of the central line and a broad-spectrum antibiotic regimen. Following this incident the patient suffered from 2 more episodes of central line-associated bloodstream infection with Klebsiella pneumonia and extended spectrum beta-lactamase (ESBL) positive bacteria. These high rates of infection were most probably due to the immunosuppression caused by the azathioprine and corticosteroid regimens as well as her regular dialysis treatment.
Towards the end of the treatment regimen, just around the time the azathioprine had been stopped, the patient presented once more to the ER. Her symptoms of increased weakness, confusion and vomiting were suspected to be those of colchicine overdose. The colchicine was therefore stopped and the patient was only kept on the prednisone tapering protocol.
Discussion
The treatment of patients with ESRD and pericarditis is not straightforward. The typical first line treatment for pericarditis involves the use of NSAIDs and colchicine, which should both be used with caution in patients with reduced kidney function [1]. To compound the problem further there is only a limited amount of studies on the subject, which could have offered some guidance on how to manage the patient.
This patient was diagnosed as having idiopathic recurrent pericarditis due to her recurrent flares. An extensive workup of the patient was undertaken, however, the aetiology behind her diagnosis is still unknown.
Given her ESRD, it was crucial to consider uremic pericarditis as a possible cause [2]. However, uremic pericarditis is diagnosed when the serum BUN level rises above 60 mg/dl . This diagnosis was ruled out because her serum BUN levels never surpassed this threshold and clinical presentation was associated with non-uremic pericarditis [3]. Moreover, her regular dialysis treatment further reduced the likelihood of her developing uremic pericarditis [4,5]. Other causes of pericarditis were also considered, including: malignancy, infection and tuberculosis, which were all excluded. In addition, systemic immune-mediated causes were ruled out by running a full rheumatological profile on the patient, which was also normal.
There is insufficient data to determine whether colchicine should be used as standard therapy in ESRD patients due to different pharmacokinetics in these patients [6]. However, colchicine 0.5 mg BID together with prednisone was introduced as second line therapy, in this patient, after her first flare of pericarditis. There was a good initial response to the treatment, but the patient then showed signs of colchicine overdose, most likely due to her poor kidney function. As a result of the side effects this medication was stopped. This situation highlighted the complexity of treating patients with ESRD and the need for further studies to determine if colchicine is suitable for patients with concurrent pericarditis and ESRD.
Another important aspect in treating this patient became apparent when she started developing recurrent episodes of severe sepsis. These episodes were due to her immunosuppressed state caused firstly by her frequent dialysis treatment but exacerbated by the immunosuppressive therapy (azathioprine and the long-standing corticosteroid regimens). Physicians need to consider the fine balance between treating a flare of pericarditis and not over- immunosuppressing the patient. With this in mind,It is important to be aware of alternative treatments and acceptable third-line agents such as IVIG and Anakinra [1,7]. A working hypothesis, amongst experts, is that perhaps physicians should prescribe IVIG or Anakinra earlier in ESRD patients due to the fact that these patients are more prone to infection. This treatment regimen may decrease the possibility of sever septic events which patients can suffer from whilst on azathioprine and most importantly long- standing corticosteroid regimens.
For the past 6 months the patient has remained asymptomatic and pericarditis-free while on prednisone 5mg once daily. Unfortunately, a recent Cardiac MRI showed late circular enhancement of the pericardium, which correlates with chronic or subacute pericarditis (Figure 1).
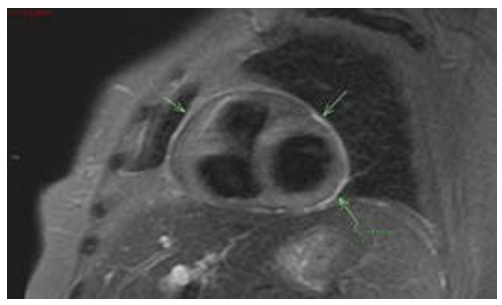
Figure 1: Cardiac MRI showed late circular enhancement of the pericardium.
In the next flare of her recurrent idiopathic pericarditis, she will be prescribed with Anakinra (IL-1 inhibitor) to see if this will have a more positive outcome.
References
- Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, et al. (2015) 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 36: 2921-64.
- Gunukula SR, Spodick DH (2001) Pericardial disease in renalpatients. Semin Nephrol 21: 52-56.
- Lange RA, Hillis LD (2004) Clinical practice. Acutepericarditis. N Engl J Med 351: 2195-2202.
- Sadjadi SA, Mashahdian A (2015) Uremic pericarditis: a report of 30 cases and review of the literature. Am J Case Rep 16: 169-173.
- Silverberg S, Oreopoulos DG, Wise DJ, Uden DE, Meidok H, et al. (1977) Pericarditis in patients undergoing long-term hemodialysis and peritoneal dialysis. Incidence, complications and management. Am J Med 63: 874-879.
- Wason S, Mount D, Faulkner R (2014) Single-dose, open-label study of the differences in pharmacokinetics of colchicine in subjects with renal impairment, including end-stage renal disease. Clin Drug Investig 34: 845-855.
- Lotan D, Wasserstrum Y, Fardman A, Kogan M, Adler Y (2016) Usefulness of Novel Immunotherapeutic Strategies for Idiopathic Recurrent Pericarditis. Am J Cardiol 117: 861-866.