
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2018) Volume 3, Issue 2
Management of Antenatal Pelvic Girdle Pain Study (MAPS): A Double Blinded, Randomised Trial Evaluating the Effectiveness of Two Pelvic Orthoses
2Royal Cornwall Hospitals NHS Trust, Cornwall, United Kingdom
Received Date: Jul 07, 2018 / Accepted Date: Jul 13, 2018 / Published Date: Jul 20, 2018
Copyright: ©Lee Cameron, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Pelvic girdle pain (PGP) occurs in 70% of pregnant women; of whom 25% have severe pain and 8% severe disability requiring the use of crutches, wheelchair or confinement to bed [1]. Patients with pregnancy related PGP have been shown to have increased pelvic joint motion compared with healthy pregnant controls, probably due to a combination of hormonal and biomechanical factors, leading to an increase in pelvic joint laxity, changes in lumbopelvic posture and increase in shearing forces through pelvic joints, thus leading to pain [2,3].
Introduction
Pelvic girdle pain (PGP) occurs in 70% of pregnant women; of whom 25% have severe pain and 8% severe disability requiring the use of crutches, wheelchair or confinement to bed [1]. Patients with pregnancy related PGP have been shown to have increased pelvic joint motion compared with healthy pregnant controls, probably due to a combination of hormonal and biomechanical factors, leading to an increase in pelvic joint laxity, changes in lumbopelvic posture and increase in shearing forces through pelvic joints, thus leading to pain [2,3]. PGP is difficult to manage; activities such as turning in bed, prolonged walking, or carrying items may cause pain; impacting negatively on quality of life [4]. In economic terms societal costs are significant, mainly as a consequence of work absenteeism; with 20% of people requiring an average of 7-11 weeks sick leave [5-8]. There are high direct health costs as well as increased health risks as women with PGP have a higher request for induction of labour and elective caesarean section to achieve symptomatic relief [3,5,7].
Orthoses such as pelvic belts are commonly used in clinical practice to manage pregnancy related PGP [9,10]. They are used to apply external compression to the pelvis to improve pelvic stability, increase neuromuscular control and reduce shearing forces through the pelvis, by way of a substitute for reduced ‘force closure’ associated with pelvic pain [9]. Studies, for example, suggest that the orthoses may be effective in reducing sacro-iliac joint (SIJ) laxity and provide more effective load transfer through the pelvis [11,12]. Recently, dynamic elastomeric fabric orthoses (DEFO’s) have been developed for PGP management. Evidence of their effectiveness in reducing pain and improving function is, however, limited to athletes and two case reports in pregnant women, providing preliminary evidence of benefits in terms of pain, function and comfort [13]. The purpose of this study was to investigate the relative effectiveness of this newly developed orthosis compared to other commercially available pelvic belts in managing pregnancy related PGP.
Our primary aim was to determine the relative effectiveness of a rigid pelvic orthosis (plus standardised advice) compared to a customised DEFO (plus standardised advice) in reducing pain in pregnant women with PGP. Secondary aims were to compare these two interventions in terms of activity levels and health-related quality of life.
Materials and Methods
Ethical approval was gained from the National Research Ethics Service, South West 3 Regional Ethics Committee (REC reference number: 12/SW/0014), and the Faculty of Health Ethics Committee at Plymouth University. National Health Service (NHS) Research and Development approval was gained from the participating NHS centre.
Trial Design
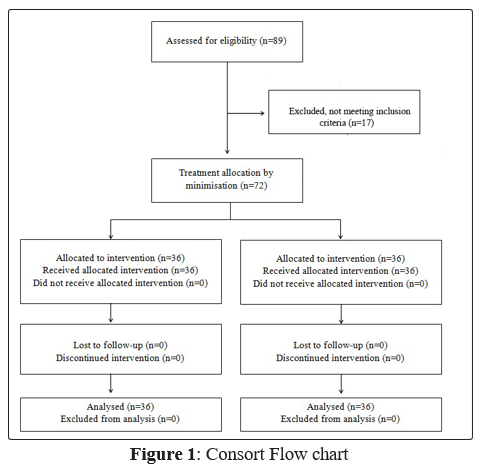
This was a single centred, double blinded, randomised comparative trial (RCT). CONSORT guidelines were adhered to maintain a quality and transparent approach [14]. Fig 1 shows the CONSORT flow chart detailing participant flow through the trial.
Setting and Participants
The trial was carried out within the maternity department of a regional hospital in the South West of England, United Kingdom. Recruitment commenced in January 2013 and ceased in December 2014 due to reaching recruitment target.
Participants were recruited from the maternity department of the regional hospital. The Consultant Obstetricians and Midwives were the main recruiters as they typically had first contact with women with pregnancy related musculoskeletal problems. With the potential participant’s consent, the lead researcher was informed, via a generic email account/ contact telephone number, of the individual’s contact details. This enabled them to contact the participant, typically within 24 hours, to investigate whether it was appropriate to book a screening appointment with the individual to determine their eligibility for inclusion within the trial.
To be eligible for entry to the trial participants were required to have intermittent PGP (commenced during or aggravated by pregnancy), which caused walking and/or stairs to be bothersome and were between 20 and 36 weeks pregnant. The decision was taken to not enrol any participants before 20 weeks due to the potential for increased complication rate within the 1st Trimester and no later than 36 weeks due to the practicality of providing a custom made orthosis so close to their delivery date. The participant also had to test positive on at least three out of seven pain provocation tests (one out of two symphysis pain tests and two of the five SIJ pain tests as detailed under the classification of pelvic girdle pain (see Fig 2).
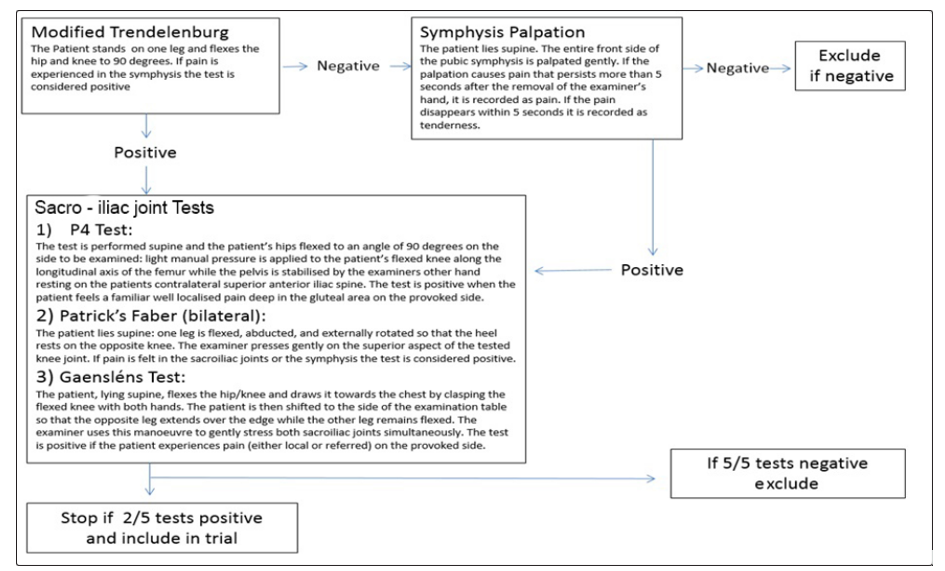
Figure 2: The pain provocation pathway required for inclusion or exclusion of the study
Exclusion criteria were a reported history or signs and symptoms indicative of a serious cause of pain that might be inflammatory, infective, traumatic, neo plastic, degenerative or metabolic. This included a history of trauma, unexplained weight loss, history of cancer, steroid use, drug abuse, HIV infection, immune suppressed state, neurological symptoms such as bowel or bladder, sensory, motor, reflex involvement (cauda equina, lumbar disc lesion, spinal stenosis), fever, systemically unwell, obstetric complications, pain that does not improve with rest/severe disabling pain. Also excluded were those women with a history of chronic back or pelvic pain requiring surgery, focal inflammatory signs/tenderness of the spine (spondylolisthesis), those who had a known allergy to Lycra, or were<20 or > 36 weeks pregnant.
Screening
Having confirmed the participant wished to take part in the study their written informed consent was obtained for the screening appointment, which was held at the regional hospital. This was undertaken by the lead physiotherapy researcher (LC), in the presence of a female chaperone. Screening involved:
• Gathering demographic and diagnostic information to confirm eligibility criteria, described above
• Identifying pain sites using a Pain Referral Map3
• Undertaking a pain provocation test battery for diagnosis of pelvic girdle pain. The tests used were those recommended by the European Guidelines for the diagnosis and management of pelvic girdle pain [3](Fig 2)
Symphysis Pain: Palpation of the symphysis or Modified Trendelenburg test
Sacroiliac Joint (SIJ) Pain: Posterior pelvic pain provocation test (P4/thigh thrust), Patrick’s Faber Test and Gaenslen’s test. All tests were undertaken in a standardised order to enable confirmation of eligibility, whilst minimising aggravation of pain irritability. The order of tests was as follows (Fig 2): The Modified Trendelenburg test was undertaken first to identify pain in the SP. If this test was positive, SIJ tests were then carried out. If it was negative direct palpation of symphysis was undertaken, if this test was negative then the female was excluded from the trial, if it was positive then SIJ tests were undertaken. For SIJ pain tests, the P4 test was applied first (bilaterally), followed by the Patrick’s Faber test (bilaterally), and Gaenslan’s test. If two of the SIJ tests were positive then the female was recruited into the study. If not testing continued to the final SIJ provocation test, Gaensléns test, The tests were ranked in this hierarchy based on their provocation levels and the positions the participants would have to get into for testing.
Randomisation and Blinding
To optimise blinding, all participants who met the inclusion criteria were measured for a customised DEFO at the conclusion of the screening process, regardless as to whether or not they were randomly allocated to receive this intervention. The measurement process, which involved undertaking 12-13 pre-specified measurements, was undertaken by the physiotherapy researcher (LC) with the assistance of a female chaperone, and took approximately six minutes to complete. This ensured that all participants were given the same amount of time and attention, regardless of potential group allocation.
Following screening and confirmation of eligibility, participants were asked to leave the room whilst they were randomly allocated, by the method of minimisation. This has been referred to as the platinum standard for randomised trials [15]. Participants were allocated to receive either the off-the-shelf rigid pelvic belt plus standardised advice or the customised DEFO plus standardised advice. In line with recommendations by Scott (2002), the first 10 participants were randomised through the use of a randomised number generator (http http://www.random.org/) to limit bias [16]. Thereafter, computer software ‘minim’ (https://www-users.york.ac.uk/~mb55/guide/ minim.htm) was used by the lead researcher (LC) to allocate participants to either group according to: age, gestation, parity and body mass index, since these variables have demonstrated to be prognostic indicators for PGP [16]. The software accommodated these variables and balanced the group selection accordingly, ensuring a more even distribution of potential factors which could alter any intervention effect.
Following randomisation, all participants were given an appointment seven days later in order to undertake the baseline assessments and receive the allocated intervention. This seven-day time frame allowed for the production of the customised DEFO and ensured that the timeline and experience of both groups were matched.
Interventions
In line with TIDieR Guidelines, full details of each intervention are described below [17].
Standardised Advice
In addition to the orthoses, participants in both Groups were given the same standardised advice sheet ‘Guidance for mothers to be and new mothers: Pregnancy-related pelvic girdle pain’ accessible via the Association of Chartered Physiotherapists in Women’s Health website (http://www.csp.org.uk/sites/files/csp/secure/acpwh-pgppat_0.pdf). The participant could use this as a resource throughout their pregnancy. All the participants were also given a standard advice sheet regarding the washing of their orthosis.
Off-the-shelf rigid pelvic belt This pelvic belt
(supplied by Serola Biomechanics Inc. www. appliedbiomechanics.co.uk/) consisted of an open cell urethane inner layer (3” in width), wrapping the circumference of the pelvic girdle and fastening with Velcro tape (see Fig 3). It has an added extra-strong, double-pull elastic straps which can be applied, also with Velcro tape, for further tension and support. The Serola Belt required a single waist measurement.

Figure 3: Shows both interventions: the Serola belt (Top) and the customised dynamic elastomeric orthoses (DEFO) (Bottom).
Customised Dynamic Elastomeric Fabric Orthosis (DEFO)
A customised Dynamic Elastomeric Fabric Orthosis (DEFO) (supplied by DM Orthotics’ Ltd, www.dmorthotics.com/) was supplied and fitted by the lead physiotherapy researcher (LC)(see Fig 3). This orthosis was individually tailored to the participant on the basis of 12 measurements for the 2nd trimester participants (13-27 weeks pregnant) and 13 measurements for 3rd trimester participants (28-40 weeks pregnant). Designed in the form of a pair of shorts opposed to the standard belt, the customised DEFO is made of a flexible compression fabric (Lycra) to aid pelvic stability, providing comfort and movement. It has reinforced panelling for strength and stability with an option for open crotch available (a closed crotch was used during this study).
Data Collection Procedures
At the day seven appointment, participants completed their first battery of self-report questionnaires (described below) in the waiting room before contact with the lead researcher (to maintain lead researcher blinding). The completed questionnaires were placed into a sealed, opaque, freepost envelope and posted to an independent researcher at the University. At the same time they were also supplied with folders containing questionnaires and freepost envelopes grouped together in two week batches. They were requested to return the completed questionnaires to the independent external blinded researcher every two weeks. Each envelope was given a unique code so that the independent external blinded researcher could systematically check that the forms had been returned and fully completed. A notification system was in place to follow up any non-returns or missing data by telephone. At this telephone conversation the question (pertaining to the missing data) was read out and the participant was requested to provide a response. This telephone conversation was scripted to ensure standardisation. Once checked the questionnaire was locked in a cabinet which only the independent external blinded researcher could access. Blinding of the lead researcher, and other members of the research team, was thereby ensured for the duration of the study.
Outcome Measures
Standardised, validated self-report postal questionnaires were compiled in a questionnaire booklet. Participants were requested to complete the booklet in the pre-designed order; this typically took approximately 10 minutes. Some answers required extra information if answered ‘yes’ or ‘no’ so that, at a minimum, participants were asked to answer 79 items, and at a maximum 88 items.
The primary outcome measure was the Numerical Pain Rating Scale (NPRS), which is the gold standard for reporting pain intensity within healthcare, with established validity and reliability [18-20]. This 11-point scale, consists of integers from 0 (no pain) to 10 (unbearable pain). In this study pain intensity was measured by asking two questions: (1) “Over the last week, how would you rate your average level of pelvic pain during the day?” and (2) “Over the last week, how would you rate your average level of pelvic pain during the night (after going to bed)?” Pain classifications were divided between mild pain (0-4), moderate pain (5-7) and severe pain (8-10) [18-21].
The secondary outcome measures were the:
• Pelvic Girdle Questionnaire (PGQ); this condition-specific, 25-item self-report questionnaire evaluates activity/participation (20 items) and body functions/symptoms (5 items) (5) using a 4-point Likert scale. High validity and reliability have been reported by the developer, however more research is required to further support this claim [22,23].
• European Quality of Life 5 Dimension, 5 level Questionnaire (EQ5D-L): this widely used, generic, 5-item self-report questionnaire with established psychometric properties provides an evaluation of health related quality of life (HRQoL) and a standardised health index to enable cost utility or cost effectiveness analysis [24-26].
• Short Form-36 Version 2 (SF-36v2): this 36 item self-report questionnaire is widely viewed as the gold standard generic health related quality of life measure with evidence to support its use in pregnant women. This version asks participants to rate their quality of life over the past week [27-29].
Sample Size
The recruitment target of 72 was based on data from Depledge RCT which assessed effectiveness of pelvic belts and exercise on PGP in pregnant women [30]. Average pain (measured by VAS) was assessed before and after a one week intervention. A combination of a non-rigid belt and exercise decreased pain from 42.5% (±11 mean ±SD) to 38.5% (±11) whilst a rigid belt and exercise decreased pain from 52 % (±11) to 38.5% (± 11).The resultant effect size was 0.86 [(42.5-38.5)-(52-38.5) / 11]. For a two tailed unpaired t-test at 85% power and a significance level of 0.05 an estimated 25 people were required in each group. Depledge et al’s attrition rate was 6.6% for two outcome measures spaced one week a part; attrition rates of up to 20% have been reported in other studies [30]. With an estimated 10% attrition rate for each measurement session (n=4) we aimed to recruit 36 participants in each group.
Data Analysis
Due to a variable baseline length, as a result of participants entering the trial at different time points relative to their delivery date, the analyses of outcome measures were calculated using the final three time points pre partum (antenatal -6 /-4 /-2 weeks) and the first three time points post-partum (postnatal +2/+4/+6 weeks).
Separate analyses were performed for each of the outcome measures using SPSS Software (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY) and Quality Metric Outcomes TM Scoring Software 4.5 to score the SF-36v2. Separate 2x3 (Group x Time) repeated measure analysis of variance (RM-ANOVA), were used to analyse the NPRS and the EQ5D-L dimensions and EQ5DL- VAS pre and postpartum. A Mann- Whitney U test was used for analysis of the SF36 to compare group differences and Freidman’s test to compare differences between time intervals. A Mann-Whitney U test was used for analysis of the PGQ and the EQ5D-5L subscales.For all tests, the alpha level was set at .05 and Bonferroni corrections were used when post hoc pair wise comparisons were calculated.
The primary outcome measure, NPRS, was assessed for clinical significance using a Minimal Clinically Important Difference (MCID) of one point [31]. The mean difference from the final pre-pregnancy data point (-2 weeks) was compared against baseline in both the groups to identify any reduction in pain score.
Results
Table 1 details the sample characteristics. There was complete data for all participants for all time points. Table 2 details mean and standard deviations for both primary and secondary outcome measures for both the SEROLA and DEFO group.
Table 1. Sample characteristics
|
Participant Characteristics |
||
|
(n=72) |
SEROLA (n=36) |
DEFO (n=36) |
|
Age |
29 (18-39) |
30 (20-40) |
|
Gestation |
29 (20-35) |
28 (20-35) |
|
Parity |
1.3 (0-3) |
1.4 (0-3) |
SEROLA = off-the-shelf rigid orthosis; DEFO = customised Dynamic Elastomeric Fabric Orthosis
Table 2: Descriptive statistics for all outcome measures across time and allocated to groups (SEROLA and DEFO)
|
|
SEROLA (Antenatal) |
SEROLA (Postnatal) |
DEFO (Antenatal) |
DEFO (Postnatal) |
||||||||||||
|
Time in weeks relative to birth Antenatal = -6/-4/-2 & Postnatal = +2/+4/+6 |
||||||||||||||||
|
Outcome Measures |
Baseline |
-6 |
-4 |
-2 |
This line signifies birth of child |
+2 |
+4 |
+6 |
Baseline |
-6 |
-4 |
-2 |
This line signifies birth of child |
+2 |
+4 |
+6 |
|
(Mean(+/- SD)) |
scores |
|
|
|
|
|
|
scores |
|
|
|
|
|
|
||
|
NPRS DAY * |
6.00 |
5.56 |
5.72 |
5.92 |
1.36 |
1.06 |
0.83 |
5.92 |
4.89 |
5.03 |
4.92 |
1.06 |
1.06 |
1.00 |
||
|
Available range 0-10 |
(1.20) |
(1.59) |
(1.65) |
(1.65) |
(1.07) |
(0.92) |
(0.91) |
(1.42) |
(1.83) |
(1.76) |
(1.86) |
(1.51) |
(1.96) |
(2.00) |
||
|
NPRS NIGHT * |
6.61 |
6.22 |
5.92 |
5.97 |
1.39 |
1.19 |
0.94 |
5.78 |
5.06 |
5.22 |
4.83 |
1.11 |
1.14 |
1.06 |
||
|
Available range 0-10 |
(1.75) |
(1.94) |
(1.79) |
(2.04) |
(1.27) |
(1.06) |
(1.07) |
(2.17) |
(2.33) |
(2.19) |
(2.30) |
(1.19) |
(2.02) |
(2.10) |
||
|
PGQ † |
64.78 |
61.9 |
62.3 |
64.8 |
16.9 |
12.2 |
10.1 |
64.19 |
62.2 |
61.4 |
62.0 |
14.1 |
14.8 |
12.1 |
||
|
Available range |
(12.64) |
(16.61) |
(17.42) |
(19.12) |
(13.41) |
(10.95) |
(10.31) |
(11.91) |
(18.80) |
(20.28) |
(20.98) |
(13.08) |
(19.62) |
(19.60) |
||
|
0-100 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
EQ5D‡ |
0.52 |
0.51 |
0.51 |
0.47 |
0.74 |
0.78 |
0.81 |
0.49 |
0.48 |
0.52 |
0.47 |
0.77 |
0.78 |
0.81 |
||
|
Available range 0-10 |
(0.17) |
(0.22) |
(0.17) |
(0.17) |
(0.11) |
(0.12) |
(0.12) |
(0.20) |
(0.19 |
(0.17) |
(0.20) |
(0.13) |
(0.23) |
(0.23) |
||
|
EQ5D VAS§ |
55.69 |
54.89 |
52.22 |
50.56 |
74.36 |
74.39 |
77.50 |
60.89 |
58.33 |
57.61 |
55.64 |
70.50 |
74.86 |
77.44 |
||
|
Available range |
(17.33) |
(16.68) |
(17.09) |
(16.36) |
(13.13) |
(13.83) |
(14.16) |
(17.17) |
(20.24) |
(18.39) |
(18.47) |
(18.57) |
(20.18) |
(19.37) |
||
|
0-100 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
SF36 (PC)|| |
35.51 |
34.91 |
34.91 |
33.12 |
45.37 |
48.27 |
50.60 |
35.62 |
34.26 |
34.78 |
35.09 |
46.16 |
47.82 |
51.86 |
||
|
Available range |
(7.30) |
(7.46) |
(7.64) |
(7.98) |
(7.94) |
(7.78) |
(7.90) |
(5.95) |
(5.72) |
(6.37) |
(6.61) |
(7.00) |
(9.24) |
(9.06) |
||
|
0-100 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
SF36 (MC)¶ |
43.61 |
43.75 |
42.84 |
41.98 |
49.34 |
51.27 |
50.86 |
46.77 |
47.85 |
48.16 |
48.52 |
55.08 |
56.65 |
56.03 |
||
|
Available range |
(9.46) |
(11.02) |
(11.45) |
(10.41) |
(9.07) |
(8.97) |
(9.13) |
(9.90) |
(11.29) |
(10.62) |
(10.54) |
(9.77) |
(10.64) |
(9.44) |
||
|
0-100 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
* Numerical Patient Reported Score (NPRS) primary outcome measure - higher scores = worse pain; negative change score = improvement † Pelvic Girdle Questionnaire (PGQ) Secondary outcome measure – higher scores = more pain during tasks; positive change score = improvement ‡EuroQol 5 dimension (EQ5D) secondary outcome measure higher scores = worse quality life; positive change score = improvement §EuroQol 5 dimension Visual Analogue Scale (EQ5D – VAS) secondary outcome measure lower scores = worse quality of life; negative change score = improvement || Short Form 36 item questionnaire – physical component (SF36 (PC)) secondary outcome measure Low scores = worse quality of life; positive change score = improvement ¶ Short Form 36 item questionnaire – mental health component (SF36 (MC)) secondary outcome measure. Low scores = worse quality of life; change score = improvement |
||||||||||||||||
Primary Outcome Measure
Numerical Pain Rating Scale – DAY (NPRS-DAY):
The antenatal data analyses revealed no significant main effect of Time F(2, 14) = .901, p =.409, but a significant difference between the groups F(1, 70) = 4.601, p<.05. There was no interaction between time and groups F(2, 140) = 2.079, p = .129. Pair wise comparisons revealed a significant difference between the two groups at the final (-2 week) antenatal time point (p <.05), while the second (-4 week) time point approached significance (p = .089) with the SEROLA group ranking consistently higher day pain ratings (i.e. worse pain) than the DEFO group (see Fig 4 and 5).
Analysis of the postnatal data revealed no significant main effect of Time F(2, 140) = 3.085, p =.063, or significant differences between Groups, F(1, 70) = .021, p = .885, indicating similar postnatal scores for the two groups across time. Pair wise comparisons revealed a significant decrease in pain ratings for the SEROLA group from the first and last (+2 to +6) postnatal time points (p< .05), but no significant change across Time for the DEFO group (p>.05), and no significant differences between Groups at all time points (p<.05) (Fig 4 and 5).
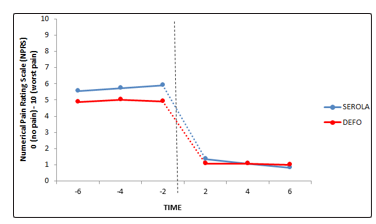
Figure 4: Mean day NPRS for SEROLA and DEFO groups at pre-birth time points (-6, -4, -2 weeks) and post-birth time points (+2, +4, +6 weeks). Vertical dotted line symbolises birth of child
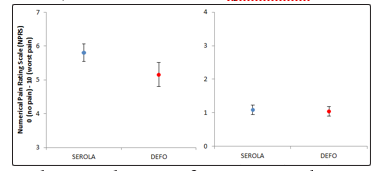
Figure 5: Grand average day NPRS for SEROLA and DEFO groups over the pre and post birth periods, along with 95% confidence intervals
The analysis of minimally clinical important difference (MCID) was significant in the DEFO group with a one point reduction in the NPRS (Baseline = 5.917; Final pre-pregnancy data point = 4.917 (-2)). There was no MCID found for the Serola group.
Numerical Pain Rating Scale – Night (NPRS-NIGHT)
The antenatal data analyses revealed a similar pattern of results to the day NPRS with no significant effect of Time F(2, 140) = 1.233, p =.297, but a significant difference between Groups, F(1, 70) = 4.657, p<.05, and no significant interaction between time and groups. Pair wise comparisons revealed a significant difference between the groups at both the first (-6) and final (-2) prenatal time points (p’s <.05), indicating significantly higher night pain ratings (worse pain) for the SEROLA group compared to the DEFO group. Furthermore, a decrease in pain ratings for the DEFO group from time points -4 to -2 approached significance (p =.053), while pain ratings for the SEROLA group increased, but not significantly (p = .779) (see Fig 6 and 7).
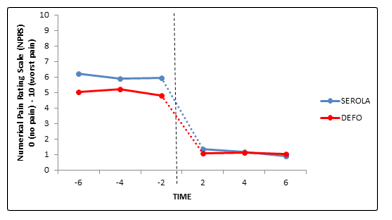
Figure 6: Mean night NPRS data for both SEROLA and DEFO, at pre-birth time points (-6, -4, -2) and post-birth time points (+2,+4, +6), dotted line symbolises birth of child.
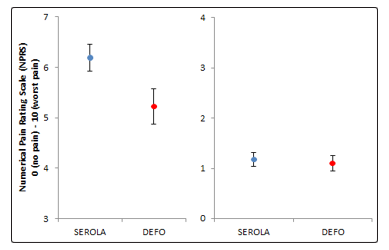
Figure 7: Total mean data for both SEROLA and DEFO, at pre and post birth, along with upper and lower 95% confidence intervals Analysis of the postnatal data revealed no significant main effect of Time F(2, 140) = 2.104, p =.142, or significant differences between Groups, F(1, 70) = .051, p =.821. Pair wise comparisons revealed no significant differences between the groups at all time points (all p’s>.05), and a significant decrease in pain ratings for the SEROLA groups from +4 to +6 time points (p<.05), but no significant change for the DEFO group (p =.410)(Fig 6 and 7).
There was no MCID found for either the Serola or DEFO, although both groups reported a reduction in pain. However, the mean difference between baseline and final antenatal (-2 weeks) NPRS score for the DEFO approached clinical significance (0.94), but not for the Serola group (0.64).
Secondary outcome Measures
EuroQOL 5 Dimension, 5 Level: (EQ5D-5L)
There were no significant differences between the groups at all time intervals either in the ante-natal or post-partum periods for the EQ5D-L health state scores (p> 0.05).
EuroQOL 5 Dimension, 5 Level – Visual Analogue Scale (EQ5D-5L-VAS)
There was a significant effect of Time F(2, 140) = 5.999, p <.001,for the antenatal data with health scores increasing over time, but there was no significant differences between Groups, F(1, 70) = 1.667, p = .264, indicating similar perceived health ratings for both the DEFO and SEROLA groups. Pair wise comparisons revealed no significant differences between the groups at any time point (all p’s >.05). However, there was a significant increase in reported health score for the SEROLA group from the first (-6) to final (-2) antenatal time points (p <.01); the increase for the DEFO group was close to significance (p = .051).
Postnatal results revealed a significant main effect of Time F(2, 140) = 9.506, p =.001, but no significant differences between Groups F(1,70) = 0.092, p = .763. Pair wise comparisons revealed no significant differences between the groups at any time point (all p’s >.05), but a significant increase in health score for both the DEFO (p <.01) and SEROLA (p =.001) groups from the first (+2) to final (+6) postnatal score.
Pelvic Girdle Questionnaire (PGQ):
There were no significant differences between the Groups at any time intervals either in the antenatal or postpartum periods (p>.05), indicating that both groups reported similar levels of activity levels and pain across time.
Short Form-36, Version 2 (SF-36v2):
Analysis of the SF-36 Physical Component revealed no significant difference between the SEROLA and DEFO at all time intervals (p >.05). However, the Mental Component revealed significant differences between the SEROLA and DEFO at all postnatal time intervals (p<.008), and at the final antenatal time interval (p = .008), with higher median values for the DEFO than the SEROLA across all cases. However, no significant differences were found at either the first (p = .110) or second (p = .062) antenatal time intervals.
Follow up analyses using the Friedman’s Test was performed on the SF-36 Physical Component to compare differences across all time intervals. Results for the SEROLA revealed an overall significant difference between time intervals χ2(6) = 142.401, p < 0.001. This was also found for the DEFO χ2(6) = 117.221, p < 0.001. Each time interval was further analysed using a post hoc Wilcoxon’s signed ranks test to determine whether there was any significant difference between each linear time interval. Results, which were corrected using the Bonferroni adjustment, revealed no significant differences for the SEROLA from baseline to the first antenatal time interval (-6) (p = .140) or between the first (-6) and second (-4) antenatal time interval (p = .647). However, there was a significant decline from the second (- 4) and final antenatal time interval (-2) (p = .001), but as expected, there was a significant improvement from the final antenatal (-2) to first postnatal (+2) and all other time intervals (p <.001). Post hoc analysis for the DEFO revealed a significant decline from baseline to the first antenatal time interval (-6), but this appeared to stabilize during antenatal time period as no significant differences were found between the first (-6) and second antenatal (-4) time (p = .694), or second (-4) and last (-2) antenatal time interval (p = .728). As expected, there was a significant improvement from the last antenatal (-2) to first postnatal (+2) time interval and the second postnatal (+4) to last postnatal (+6) time interval (p<.001). Finally, the first (+2) to second (+4) postnatal time intervals approached significance, following Bonferroni correction (p = 0.01).
Analysis of the SF-36 Mental Component revealed similar results, with a significant difference found for both the SEROLA χ2(6) = 60.440, p < 0.001 and DEFO χ2(6) = 69.416, p < 0.001 across time. Post hoc analysis revealed no significant difference between baseline, or any antenatal time intervals (p>.008). However, as expected, a significant improvement was found from the last antenatal (-2) to first postnatal (+2) time (p<.001), and the first (+2) and second (+4) postnatal time (p<.001). No significant difference was also found for the second (+4) and final postnatal (+6) time, once corrected (p = .025). Post hoc analysis of the DEFO revealed no significant differences between the antenatal or postnatal time points (p>.008), but as expected a significant difference was found from the last antenatal (-2) to first postnatal (+2) time (p<.001). Finally, the improvement from baseline to the first antenatal (-6) time interval was marginally significant (p = .009).
Discussion
This is the first double blinded, randomised comparative trial evaluating the effectiveness of two pelvic orthoses during pregnancy. Further it includes the evaluation of a novel intervention, the customised DEFO. It shows that, in comparison to the ‘off the shelf’ rigid pelvic belt (Serola Belt) group, pain levels for those wearing the customised DEFO were significantly less during both the day and night. These changes in day time pain were clinically significant, as determined by a one point reduction in the NPRS, which equates to a ‘slightly better’ improvement in pain. Whilst no significant difference was detected between the two groups with regard to the secondary outcomes of activity levels and quality of life, it is highlighted that the study was not powered to detect changes in these outcomes. Further studies could address this issue.
Lee & Vleeming (1998) report the need for force-form closure, neuromuscular control and emotion/awareness for optimum joint function and a balance between movement and control for optimal stability [32]. During pregnancy multiple factors have been shown to affect these aspects and potentially contribute to PGP.
The hormone serum relax in is believed to directly impact ligament laxity, thus reducing stability and stiffness in the pelvic girdle [33]. This reduction in stability can lead to increased shear forces through the Symphysis Pubis (SP) and SIJ potentially causing pain [2]. The European Guidelines for Management and Diagnosis of PGP, along with a systematic review completed by Aldabe 2012, reported that there was a low association between relaxin levels and pregnancy related PGP, therefore no conclusion could be drawn [3,33].
Biomechanical changes occur in the lumbar spine and pelvis during pregnancy due to the need to adapt centre of gravity as a result of the increasing weight of the womb [34]. The increase in maternal weight is believed to play a role in the requirement for changing lumbar biomechanics, with increased lordotic adjustment in the lumbar spine required to maintain the centre of gravity [35,36]. Other changes such as reduced muscular activity and compensatory muscle patterns can also be a potential cause of pain through reduction of joint proprioception and neuromuscular control [12].
Pelvic belts are hypothesised to enhance ‘force closure’, thereby aiding stability of the pelvic ring and reducing shearing forces through the SP and SIJ [11,37-39]. Applying external pelvic compression can: be a substitute for normal isometric abdominal activity; increase hip adduction strength; and reduce SIJ laxity [11,37-38]. This can also lead to a decrease in compensatory mechanisms through the pelvis and lumbar spine and facilitate load transfer more appropriately [12]. A pelvic belt has been observed to influence proprioception and neuro-motor control, which can also contribute with the reduction of compensatory patterns, and further improving force closure [11,39-43]. With changing pelvic biomechanics, it has been observed that a pelvic orthosis can release strain on sacroiliac ligaments which can reduce potential tensile stress thus reducing the pain [34,42,43]. Passive force-closure using a pelvic belt reduces abdominal muscle activation and there are concerns this could lead to muscle weakness [9]. The European Guideline advocates that pelvic belts should be considered alongside other treatment modalities [3]; our study supplemented its use with standardised advice.
Strength and limitations of the study
Our study is the first to compare the relative effectiveness of two orthoses (plus standardised advice) on pain, activity levels and quality of life, providing clinicians and patients with evidence on which to guide treatment selection. Self-report questionnaires were used in this study, primarily to reduce participant burden and missing data in a sample who may find it difficult to attend follow-up assessments due to work and family commitments and in whom travelling can irritate their pain. This approach, alongside our data checking and management systems, are strengths of this study since there was no missing data. This is important since missing data can compromise inferences made from clinical trials [44]. A particular challenge in this trial was that a pre-defined threshold of pain needed to be reached before participants were eligible for entry, resulting in participants entering the study at different time points during their pregnancy (relative to delivery date). The minimisation procedure utilised to reduce the likelihood of disparity between the groups, with no significant difference between the two groups in their baseline level of pain and the time they entered the study. The analyses thereby focused on the final three data points in the antenatal phase and the first three data points in the post-partum phase – a total of 12 weeks. Future studies could explore whether a DEFO could be used at an earlier stage in those individuals at high risk of developing PGP since with many musculoskeletal conditions prevention/early intervention is favoured.
Conclusion
The novel, customised dynamic elastomeric fabric orthoses was more effective than an off-the-shelf rigid pelvic belt at reducing day and night time pain in pregnant women with pelvic girdle pain.
References
- Wu WH, Meijer OG, Uegaki K, Mans JMA, van Dien JH et al, (2004) Pregnancy-related pelvic girdle pain (PPP), I: Terminology, clinical presentation, and prevalence. Eur Spine J 13: 575-589.
- Mens J, Pool-Gouzwaard A, Stam H (2009) Mobility of the pelvic joints in pregnancy related lumbopelvic pain: A systematic review. Obstet Gynecol Surv 64: 200-208.
- Vleeming A, Albert HB, Ostgaard HC, Sturesson B, Stuge B (2008) European guidelines for the diagnosis and treatment ofpelvic girdle pain. Eur Spine J 17: 794-819.
- Wang SM, Dezinno P, Maranets I, Berman MR, Caldewell-Andrews AA, et al. (2004) Low back pain during pregnancy: prevelance, risk factors, and outcomes. American College of ObstetGyenocol 104: 65-70.
- Vermani E, Mittal R, Weeks A (2010) Pelvic girdle pain and low back pain in pregnancy: a review. Pain Pract 10: 60-71.
- Dørheim SK, Bjorvatn B, Eberhard-Gran M (2013) Sick leave during pregnancy: a longitudinal study of rates and risk factors in a Norwegian population. British Journal of Obstetrics and Gynaecology 120: 521- 530.
- Norén L, Ostgaard S, Nielsen TF, Ostgaard HC (1997) Reduction of sick leave for lumbar back and posterior pelvic pain in pregnancy. Spine 22: 2157-2160.
- Malmqvist S, Kjaermann I, Andersen K, Økland I, Larsen JP, et al. (2015) The association between pelvic girdle pain and sick leave during pregnancy ; a retrospective study of a Norwegian population. BMC Pregnancy Childbirth 1–8.
- Hu H, Meijer O, Van Dien J, Hodges P, Bruijn S, et al. (2010) Muscle activity during the active straight leg raise (ASLR), and the effects of a pelvic belt on the ASLR and on treadmill walking. Journal of Biomechanics 43: 532-539.
- Damen L, Spoor CW, Snijders CJ, Stam HJ (2002) Does a pelvic belt influence sacroiliac joint laxity? Clin Biomech 17: 495-498.
- Arumugam A, Milosavljevic S, Woodley S, Sole G (2012) Effects of external pelvic compression on form closure , force closure , and neuromotor control of the lumbopelvic spine: A systematic review. Man Ther 17: 275-284.
- Oh J (2014) Effects of pelvic belt on hip extensor muscle EMG activity during prone hip extension in females with chronic low back pain. J Phys Ther 26: 1023-1024.
- Sawle L, Freeman J, Marsden J, Matthews MJ (2013) Exploring the effect of pelvic belt configurations upon athletic lumbopelvic pain. ProsthetOrthotInt [Internet] 37: 124-131.
- Schulz KF, Altman DG, Moher D (2011) CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. Int J Surg 9: 672-677.
- Treasure T, MacRae K (1998) Minimisation: the platinum standard for trials? BMJ 317: 362-363.
- Scott NW, McPherson GC, Ramsay CR, Campbell MK (2002) The method of minimization for allocation to clinical trials. a review. Control clin Trials 23: 662-674.
- Hoffman T, Glasziou P, Boutron I, Milne R, Perera R, et al. (2014) Better reporting of interventions: template for intervention description and replication (TIDieR) checklist. BMJ 348: 1687.
- Williamson A, Hoggart B (2005) Pain: a review of three commonly used pain rating scales. J Clin Nurs 14: 798-804.
- Jensen MP, Turner JA, Romano JM, Fisher LD (1999) Comparative reliability and validity of chronic pain intensity measures. Pain 83: 157-162.
- Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP (2011) Validity of four pain intensity rating scales. Pain 152: 2399-2404.
- Robinson HS, Mengshoel AM, Veierød MB, Vøllestad N (2010) Pelvic girdle pain: potential risk factors in pregnancy in relation to disability and pain intensity three months postpartum. Man Ther 15: 522-528.
- Stuge B, Garratt A, Krogstad Jenssen H, Grotle M (2011) The pelvic girdle questionnaire: a condition-specific instrumentfor assessing activity limitations and symptoms in people withpelvic girdle pain. Phys Ther 91: 1096–1108.
- Sklempe Kokic I, Ivanisevic M, Uremovic M, Kokic T, Pisot R, et al. (2017) Effect of therapeutic exercises on pregnancy-related low back pain and pelvic girdle pain: secondary analysis of a randomized controlled trial. J Rehabil Med 49: 251-257.
- Kind P, Brooks R, Rabin R (2005) EQ-5D concepts and methods: a developmental history. Springer 201-220.
- Rabin R, De Charro F (2001) EQ-5D: A measure of health status from the EuroQol group. Annals of Medicine 33: 337-340.
- Badia X, Roset M, Herdman M, Kind P (2001) A comparison of United Kingdom and Spanish general population time trade-off values for EQ-5D health states. Med Decis Making 21: 7-16.
- Ware JE, Sherbourne CD (1992) The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 30: 473-483.
- Ware JE, Gandek B (1998) Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project. J Clin Epidemiol 51: 903-912.
- Bastiaenen CHG, Bie RA De, Wolters PMJC, Vlaeyen JWS, Leffers P, et al. (2006) Effectiveness of a tailor-made intervention for pregnancy-related pelvic girdle and / or low back pain after delivery : Short-term results of a randomized clinical trial. BMC Musculoskeletal Disorders 7:19.
- Depledge J, Mcnair PJ, Keal-smith C, Williams M (2005) Management of symphysis pubis dysfunction during pregnancy using exercise and pelvic support belts. Phys Ther 85: 1290-1300.
- Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W (2004) Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur J Pain 8: 283-291.
- Lee DG, Vleeming A (1998) Impaired load transfer through the pelvic girdle – a new model of altered neutral zone function. In: Proceedings of the 3rd Interdisiplinary World Congress on Low Back and Pelvic Pain, Vienna, 1998. European Conference Organizers, Rotterdam.
- Aldabe D, Milosavljevic S, Bussey MD (2012) Is pregnancy related pelvic girdle pain associated with altered kinematic , kinetic and motor control of the pelvis ? A systematic review. Eur Spine J 21: 1777-1787.
- Liddle SD , Pennick V (2015) Interventions for preventing and treating low-back and pelvic pain during pregnancy. Cochrane Database of Systematic Reviews 30: 9.
- Branco M, Santos-rocha R, Vieira F (2014) Biomechanics of Gait during Pregnancy. The Scientific World Journal 5.
- Foti T, David JR, Bagley A (2000) A biomechanical analysis of gait during pregnancy. J Bone Joint Surg AM 82: 625-632.
- Mens JM (2017) Does a pelvic belt reduce hip adduction weakness in pregnancy-related posterior pelvic girdle pain?: a case-control study. Eur J Phys Rehabil Med 53: 575-581.
- Mens JMA, Snijders CJ, Stam HJ (2006) The mechanical effect of a pelvic belt in patients with pregnancy-related pelvic pain Clin Biomech 21: 122-127.
- Bertuit J, Eloise C, Rooze M, Feipel V (2018) Pregnancy and pelvic girdle pain: Analysis of pelvic belt on pain. J ClinNurs 27: 129-137.
- Shaffer SW, Harrison AL (2007) Aging of the somatosensory system : A translational perspective. Phys Ther 87: 193-207.
- Soisson O, Lube J, Germano A, Hammer K (2015) Pelvic belt effects on pelvic morphometry , muscle activity and body balance in patients with sacroiliac Joint Dysfunction. PLoS ONE 1-26.
- Takasaki H, Lizawa T, Hall T, Nakamura T, Kaneko S (2009) The influence of sacroiliac joint force closure on the hip and lumbar spine extensor muscle firing pattern. Man Ther 5: 484-489.
- Sichting F, Rossol J, Soisson O, Klima S, Milani T, et al. (2014) Pelvic belt effects on sacroiliac joint ligaments: A computational approach to understand therapeutic effects of pelvic belts. Pain Physician 17: 43-51.
- Little RJ, D’Agostino R, Cohen ML, Dickersin K, Emerson SS, et al. (2012) Stern H. The prevention and treatment of missing data in clinical trials. New England Journal of Medicine 367: 1355-1360.