
World Journal of Radiology and Imaging(WJRI)
ISSN: 2835-2440 | DOI: 10.33140/WJRI


Research Article - (2022) Volume 1, Issue 1
Magnitude and Predictors of Anaemia among Pregnant women attending Antenatal Clinics in Dar es salaam, Tanzania
2Cavendish university, Uganda
3PIM foundation & Medics, Tanzania
Received Date: Oct 20, 2022 / Accepted Date: Oct 30, 2022 / Published Date: Nov 08, 2022
Copyright: ©Copyright: ©2022 Samson Peter Mvandal. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Mvandal, S, P., Kumbunja, P, L., Lupoly, G., Nhandi, J, S. (2022). Magnitude and Predictors of Anaemia among Pregnant women attending Antenatal Clinics in Dar es salaam, Tanzania. World J Radiolo Img 1(1), 42-48.
Abstract
Background: Anaemia in pregnancy have been a cause of serious concern and burden as it contributes significantly to high maternal mortality worldwide. This study aims to explore how big the burden of anaemia in pregnant women is, how it can be reduced during antenatal clinic in order to minimize risks and complications of anaemia among pregnant women.
Method: An analytical cross-sectional study design used, involved 560 pregnant women attending antenatal clinic at three regional referral hospitals in Dar es Salaam region, Tanzania, from January to June 2022. Those willing to participate and met inclusion criteria were included in the study. Data was collected by interview through a structured questionnaire. Analysis of data was done using SPSS v25.0, (p<0.001) considered statistically significant.
Results: A total of 560 pregnant women were interviewed. The prevalence of anaemia in pregnancy is high about 70.9% whereby 61.2% participants had mild anaemia, 33.2% participants had moderate anaemia and 25.6% participants had severe anaemia. Significant associations were found between age, education level, marital status, Less ANC attendance (<3 visit), lack of health insurance and lack of employment among pregnant women.
Conclusion: Prevalence of anaemia in pregnancy women is still high and its predictors highly affect its control. Hence the ministry of health in collaboration with other stakeholders should develop policies, educating community on the importance of antenatal visit for early detection and treatment of anaemia and impacting knowledge to medical personnel in management of anaemia in pregnancy and associated complications in order to decrease maternal mortality rate.
Keywords
Anaemia, Antenatal, Dar Es Salaam, Hospital, Pregnant, Prevalence.
Introduction
Anaemia in pregnancy remains serious concern and burden in pregnant women and the number of women affected is still high. It contributes significantly to high maternal mortality and poor birth outcome worldwide [1, 2]. The level of haemoglobin var- ies by age, sex, altitude, smoking, and pregnancy status. Anae- mia is the commonest haematological disorder that may occur in pregnancy, the others being Rhesus iso-immunization and blood coagulation disorders[3–5]. Anaemia in pregnancy is an import- ant public health problem worldwide, WHO estimates that more than half of pregnant women in the world have a haemoglo- bin level indicative of anaemia (<11.0g/dl), the prevalence may however be as high as 56 or 61% in developing countries [3]. Anaemia in pregnancy is a common problem in most developing countries and major cause of morbidity and mortality especially in malaria endemic areas. It is frequently severe and contributes significantly to maternal mortality and reproductive health mor- bidity [4, 6].
Anaemia in pregnancy it deserves more attention than it is cur- rently receiving [7]. Published rates of prevalence of anaemia for developing countries range from 35% to 56% for Africa, 37% to 75% for Asia and 37% to 52% for Latin America, this is in sharp contrast to industrialized countries where anaemia in pregnancy occurs in less than 20% of women [8]. Exact popula- tion prevalence figures are usually not available for developing countries. Nevertheless it is clear to those in clinical practice and research that anaemia in pregnancy is a public health prob- lem and under-reported. Each year worldwide more than 500 000 women die from pregnancy related causes, the vast majority 99% in developing countries [9].
The incidence of anaemia in pregnancy ranges widely from 40% to 80% in tropics compared to 10% to 20% in the devel- oped countries and is responsible for 20% of maternal deaths in the third world countries [10]. Women often become anae- mic during pregnancy because the demand for iron and other vitamins is increased due to physiological burden of pregnancy [11]. The inability to meet the required level for these substances either as a result of dietary deficiencies or infection gives rise to anaemia [12, 13].
Globally, the most common cause of anaemia is iron deficiency, which is responsible for about half of anaemia cases in preg- nancy, and it is estimated that in developed countries 38% of pregnant women have iron depletion [14].
Antenatal care is a key strategy to improve maternal and infant health[7]. However, survey data from sub-Saharan Africa indi- cate that women often only initiate ANC after the first trimes- ter particularly adolescent pregnant women, therefore they do not fully benefit from its preventive and curative services [15]. In Tanzania, 97% of pregnant women attend antenatal care and 70% do so at least four times and do not achieve the recommend- ed number of ANC visits [16].
Anaemia ranges from mild, moderate to severe and the WHO pegs the haemoglobin level for each of these types of anaemia in pregnancy at 10.0-10.9g/dl (mild anaemia), 7-9g/dl (moderate anaemia) and <7g/dl (severe anaemia). But the pregnant wom- an in second trimester is said to be anaemic when haemoglobin level is less than 10.5g/dl [17]. Prevalence of anaemia can be as high as 42% in developing countries with a high incidence and severity occurring among primigravidae living in malaria endemic areas [18].
In Tanzania the most causes of anaemia in pregnant women are nutritional deficiencies, malaria, parasitic infestation, too short child spacing, poor diet (malnutrition), and chronic infec- tion[12,19].
Women often become anaemic during pregnancy because the demand for iron and other vitamins such as folic acid and vitamin B12 is increased due to physiological burden of pregnancy [2, 19]. Anaemia due to malaria in pregnancy is one of the major causes of maternal morbidity worldwide, and leads to poor birth out- comes [21]. Maternal mortality in Tanzania from Demograph- ic and health survey is estimated to be 556 deaths/100,000 live births [22, 23].
In pregnancy, anaemia has a significant impact on the health of the foetus as well as that of the mother whereas 20% of maternal deaths in Africa have been attributed to anaemia[23]. Fetes is at risk of preterm deliveries, low birth weights, morbidity and perinatal mortality due to the impairment of oxygen delivery to placenta and foetus [24]. The disparity between high antenatal care attendance, high prevalence of anaemia in pregnancy, high maternal mortality raise questions about the quality of care pro- vided and particularly the management of anaemia in pregnancy at antenatal clinics[21]. The management and control of anaemia in pregnancy is enhanced by the availability of local prevalence statistics, which is however not adequately provided in Tanza- nia. Therefore, this study aims to determine the prevalence and predictors of anaemia in pregnant woman attending antenatal clinics that can be used to reduce health problem pertaining to anaemia and changing the way used in treating and preventing anaemia.
Materials and Methods Study setting
The study was conducted at Antenatal clinics found in three re- gional referral hospitals namely Amana, Mwananyamala and Temeke regional referral hospital in Dar es Salaam city, Tan- zania. Dar es salaam found at eastern part of Tanzania is the most populous city in Tanzania, important economic centre and largest city in East Africa and the fifth most populous in Africa and the fastest growing cities in the world with population over 6.4 million people by 2020 [25]. Dar es Salaam has five districts: Kinondoni in the north, Ilala in the centre; Ubungo and temeke in the south; and kigamboni in the eastern. Amana RRH which is found in Ilala, Mwanyamala RRH which is found in Kinondoni and Temeke RRH found in Temeke.
Study population
All pregnant women who did not have sickle cell disease attend- ing ANC’s located in three regional referral hospitals (Amana, Mwananyamala and Temeke) in Dar es Salaam region from Jan- uary to June 2022 and willingly to take part in the study after consent.
Study design
An analytical cross-sectional study with quantitative approach was carried out in three regional referral hospitals (Amana, Mwananyamala and Temeke) in Dar es Salaam region, Tanza- nia. With aim of determining predictors and magnitude of anae- mia in pregnancy in Dar es salaam, Tanzania
Sample size and sampling procedure
The estimated sample size was calculated by using single pop- ulation proportion formula with the assumption of 50% propor- tion, 95% confidence interval and 5% margin of error. Given that the source population was less than 10,000 correction formu- la was used and 5% non-response was added, making the final sample size 560. Simple random sampling technique was used and all participants with inclusive criteria have a chance to be selected. Numbers of respondents from antenatal clinics located in Dar es Salaam regional level hospitals were selected basing on their clinic identity card/RCH card on their scheduled clinic visits.
Recruitment of participants
In this study were including all pregnant women attending at ANC clinic, mentally and physically fit and willing to participate after consent and all pregnant women who were not attending ANC clinic, physically unwell women during data collection and those who refuse to participate after consent were excluded from the Study. (See Figure 1).
Data collection tool and procedure
A standardized structured questionnaire was used to collect data. The questionnaire comprises of both open and closed ended questions and was translated in Swahili. The respondents filled the questionnaires and confidentiality was preserved.
Data processing and analysis
The data collected, analysed, coded and entered into statisti- cal package for social sciences (SPSS) version 25. The SPSS package was employed to determine frequency and percentage of the respondents, Chi square (X2) test was used to show the association between variables, a significance level (p< 0.001) were used to compare and conclude for statistical significance of the association and finally guide researcher to draw graphs and tabulation.
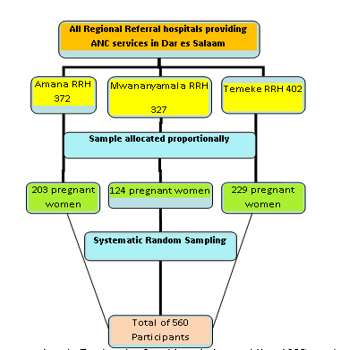
Figure 1: Sampling procedure in Regional referral hospitals providing ANC service in Dar es Salaam.
Results
Socio-demographic characteristics of study population. A total of five hundred and sixty (560) women attending an- tenatal clinic at Amana, Mwananyamala and Temeke RCH clinics in Dar es Salaam were enrolled in the study. Majority about 219(39.1%) respondents were in the age group of 21 to 30 years. Majority of respondent had formal education 85.7% and primary level of education was higher about 222(39.6%) com pared to others. Majority of respondents about 373(66.6%) were married and 372(66.4%) were unemployed. Moreover, about 288 (51.4%) pregnant women booked at first trimester (GA of 1-13weeks), about 278 (49.6%) respondents were multigravi- da having one to four children, and most of respondents 206 (36.8%) had spaced their child by 2 years. The information on socio-demographic data summarized in Table 1.
Table 1: Socio-demographic characteristics of study population (N=5
|
|
|
Frequency (N) |
Percent (%) |
|
Age |
|||
|
|
15-20 |
132 |
23.6 |
|
|
21-30 |
219 |
39.1 |
|
|
30-40 |
187 |
33.5 |
|
|
>41 |
22 |
3.4 |
|
Education level |
|||
|
|
Primary school |
222 |
39.6 |
|
|
Secondary school |
155 |
27.7 |
|
|
University/college |
103 |
18.4 |
|
|
None |
80 |
14.3 |
|
Marital status |
|||
|
|
Married |
373 |
66.6 |
|
|
Not married |
120 |
21.4 |
|
|
Divorced/sepa- rated |
61 |
10.9 |
|
|
Widowed |
6 |
1.1 |
|
Employment |
|||
|
|
Employed |
188 |
33.6 |
|
|
Unemployed |
372 |
66.4 |
|
First ANC Attendance |
|||
|
|
1-3 |
288 |
51.4 |
|
|
4-6 |
242 |
43.2 |
|
|
7-9 |
30 |
5.4 |
|
Parity |
|||
|
|
Primigravidae |
97 |
17.3 |
|
|
1-4 |
278 |
49.6 |
|
|
>5 |
185 |
33.1 |
|
Pregnancy interval |
|||
|
|
First pregnancy |
98 |
17.5 |
|
|
1 |
140 |
25 |
|
|
2 |
206 |
36.8 |
|
|
>2 |
116 |
20.7 |
Overall prevalence and severity of anaemia among pregnant women attending antenatal clinic
Women attending their antenatal clinic at Amana, Mwananya- mala and Temeke RCH were asked to choose the ANC booking haemoglobin level as written on their antenatal cards. Based on haemoglobin level, the overall prevalence of anaemia among the studied sample was 70.9% (397/560). See table 2
Table 2: Overall prevalence of anaemia among antenatal women of study population
|
|
Frequency |
Percent % |
|
Anaemia |
397 |
70.9 |
|
Non-anaemic |
163 |
29.1 |
|
Total |
560 |
100 |
Out of the 397 anaemic women, 243 (61.2%) had mild anaemia, 132(33.2%) had moderate anaemia and 22 (5.6%) had severe anaemia. The information related to prevalence and severity of anaemia are summarized in figure 2
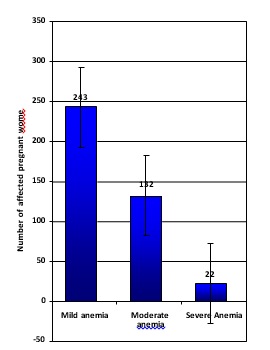
Figure 1: Showing severity of anaemia (n=560)
Anaemia in relation to socio-demographic characteristics of women attended ANC
Anaemia was found to be more prevalent in women aged be- tween 21-30years at 38.0% as compared to other age group and least prevalence among pregnant women above 40 years (p<0.001) therefore, statistical analysis of age being a factor in predicting anaemia in pregnancy.
Level of education seem to predict anaemia among pregnant women, whereby those who had attained primary education seem to have higher percentage of anaemia (42.9%) compared to others. The relationship between education level being a factor in predicting anaemia in pregnancy (p<0.001). Anaemia found to be more prevalent among women who were married (61.4%) compared to those women who were unmarried, divorced/sep- arated or widowed (p=0.022). There is no statistical association between marital status and anaemia in pregnancy
Furthermore, anaemia found to be more prevalent to unem- ployed pregnant women about 77.2% compared to those who were employed (p<0.001) and having health insurance, about 65.6% who don’t have health insurance (p<0.001) found to be statistical significant. Thus, there is statistical significant be- tween level of employment and anaemia in pregnancy (Table 3).
Table 3: Prevalence of anaemia in relation to socio-demographic characteristics of women (N=560)
|
Age |
|||
|
15-20 |
170 |
30.4 |
< 0.001 |
|
21-30 |
213 |
38.0 |
|
|
30-40 |
153 |
27.3 |
|
|
>41 |
24 |
4.3 |
|
|
Education level |
|||
|
Primary school |
240 |
42.9 |
< 0.001 |
|
Secondary school |
155 |
27.7 |
|
|
University/college |
67 |
11.9 |
|
|
None |
98 |
17.5 |
|
|
Marital status |
|||
|
Married |
344 |
61.4 |
0.022 |
|
Not married |
144 |
25.7 |
|
|
Divorced/separated |
67 |
12.0 |
|
|
Widowed |
5 |
0.9 |
|
|
ANC Attendance |
|||
|
1-3 |
288 |
51.4 |
<0.001 |
|
4-6 |
242 |
43.2 |
|
|
7-9 |
30 |
5.4 |
|
|
Health insurance |
|||
|
Yes |
194 |
34.6 |
|
|
No |
366 |
65.5 |
<0.001 |
|
Employment |
|||
|
Employed |
127 |
22.7 |
|
|
Unemployed |
433 |
77.3 |
< 0.001 |
Discussion
The study findings reported a high overall prevalence of 70.9% with anaemia among pregnant women attending antenatal clin- ics, out of the anaemic women, 61.2% had mild anaemia, 33.2% had moderate anaemia and 5.6% had severe anaemia this is al- most similarity with the study done in Nigeria in which preva- lence was 76.5% of the pregnancy women where by 57.8% had moderate anaemia, 40.3% had mild anaemia and 1.9% were se- verely anaemic[26].
Findings of this study are almost similar to those of various stud- ies done previously in sub-Saharan Africa which reported prev- alence rates of anaemia among pregnant mothers ranging from 33% to 75%[2,27].
Furthermore, the results from this study were slightly similar to that conducted at Unguja islands in which the overall preva- lence of anaemia among pregnant women was 80.8% whereby 68.64% of respondents had mild anaemia, 11.24% had moderate anaemia and 0.89% had severe anaemia[28].
Other regions in Tanzania shown a low prevalence of anaemia compared to this study findings, in Morogoro and Kilimanja- ro region the identified prevalence were 44.9% and 47.4% re- spectively. The differences could be the sample size of our study compared to these studies, also these variations could be due to dietary differences between these communities[29,30].
Study finding shows that anaemia is more prevalent with age in pregnant women, whereby the age group of 21-30 years seem to have high risk of anaemia which is comparable to the study done at 2013 in Ethiopia that showed close significance [31].
The level of education among pregnant women and anaemia, in these study findings shows the significant relationship. Edu- cation level seems to be a factor in predicting anaemia in preg- nancy. Mothers who had attained primary education had higher percentage of anaemia compared to those who had secondary school. Also those with primary education seem to have less visit to ANC and this similar to the study done 2015 in Dhaka city[32].
Anaemia in pregnancy in this study finding was not affected by marital status, despite the prevalence was high among married women compared to those women who were unmarried, di- vorced/separated or widowed. This is different comparable to this study done 2012 in Nigeria whereby anaemia in pregnancy was affected by marital status [33].
Furthermore, having health insurance and level of employment found to be predicting factor of anaemia in pregnancy, whereas those who were unemployed they failed in term of achieving dietary needs and have more risk compared to those who were employed, as compared to the study done in Ethiopia[32]. Anaemia in pregnancy in this study finding was not affected by marital status, despite the prevalence was high among married women compared to those women who were unmarried, di- vorced/separated or widowed. This is different comparable to this study done 2012 in Nigeria whereby anaemia in pregnancy was affected by marital status [33].
Furthermore, having health insurance and level of employment found to be predicting factor of anaemia in pregnancy, whereas those who were unemployed they failed in term of achieving dietary needs and have more risk compared to those who were employed, as compared to the study done in Ethiopia[32].
Conclusion
There is high prevalence of anaemia among pregnant women attending antenatal clinic at Amana, Mwananyamala and Teme- ke regional referral hospitals despite of having speciality. Anae- mia in pregnancy is predominantly associated with younger age, married, unemployment and lower level of education.
Recommendations
Based on the results of this research the ministry of health in collaboration with other relevant health partners should develop policies on health education to the community on the importance of ANC visit as it will help in early detection of anaemia. The need for CME to medical personnel to raise awareness and in- crease skills in management of anaemia in pregnancy and other associated complications in order to decrease maternal mortality rate. Community should be educated on importance of delivery in a health facility which is potentially protective against anae- mia. Further the research suggests that all health facility centres where pregnancy mother visit for ANC must provide free check of haemoglobin levels for early identification of problem. Final- ly, more researches should be done in determining prevalence, severity and factors associated with anaemia in pregnancy so as to prevent further maternal and foetal complications as well as reducing mortality rate.
Abbreviations
ANC: antenatal care; CDC: Center of Disease Control and Pre- vention; CME:Continuous medical education; Hgb: haemoglo- bin; MOI: medical officer incharge; RCH: Reproductive child health; RMO: Regional medical officer; RRH: Regional referral Hospital; SPSS: statistical product and service solution; SOPs: standard operating procedures; WHO: World Health Organiza- tion.
Ethics consideration and consent
Ethical approval was sought from CREC. And permission from RMO Dar es salaam region, permission from MOI of Amana RRH, Mwananyamala RRH and Temeke RRH. Written consents were collected from the study participants, confidentiality and anonymously assurance of voluntary participation and right to withdraw from the study.Acknowledgement
We are grateful to Regional medical officer (RMO) Dar es Sa- laam region, hospitals Medical officer incharge (MOI); Amana RRH, Mwananyamala RRH and Temeke RRH. Also study par- ticipants for their willingness of participation.
Authors’ contributions: SPM designed the study, data collection, analysed data and drafted manuscript; PLK, GL and JSN par- ticipated in the design of the study, data collection and revision of the manuscript; all authors read and approved the final man- uscript.
Funding: Not applicable.
Availability of data and materials: The data sets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Consent for publication: Not applicable.
Competing interests: The authors declare no competing inter- ests.
References
-
- Gogoi M, Prusty RK. Maternal anaemia, pregnancy compli- cations and birth outcome: evidences from north-east India. J North East India Stud. 2013;3(1):74-85.
- Sunguya BF, Ge Y, Mlunde L, Mpembeni R, Leyna G, Huang J. High burden of anemia among pregnant wom- en in Tanzania: a call to address its determinants. Nutr J. 2021;20(1):65. doi:10.1186/s12937-021-00726-0
- Ahmad MO, Kalsoom U, Sughra U, Hadi U, Imran M. Ef- fect of maternal anaemia on birth weight. J Ayub Med Coll Abbottabad JAMC. 2011;23(1):77-79.
- Akinbami AA, Ajibola SO, Rabiu KA, et al. Hematolog- ical profile of normal pregnant women in Lagos, Nigeria. Int J Womens Health. 2013;5:227-232. doi:https://doi.org/10.21.47/IJWH.S42110
- Akinlaja O. Hematological changes in pregnancy-The preparation for intrapartum blood loss. Obstet Gynecol IntJ. 2016;4(3):00109
- Desai M, Hill J, Fernandes S, et al. Prevention of malar- ia in pregnancy. Lancet Infect Dis. 2018;18(4):e119-e132. doi:10.1016/S1473-3099(18)30064-
- 7WHO ,World Health organization Recommendations on Antenatal Care for a Positive Pregnancy Experience. World Health Organization; 2016
- WHO, World Health Organization. World Health Statistics 2015. World Health Organization; 2015. Accessed Septem- ber 17, 2022. https://apps.who.int/iris/handle/10665/17025
- GBD 2015 Maternal Mortality Collaborators. Global, re- gional, and national levels of maternal mortality, 1990- 2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Lond Engl. 2016;388(10053):1775-1812. doi:10.1016/S0140-6736(16)31470-
- Dutta DC. Textbook of obstetrics. Hypertens Disord Preg- nancy. 2004;6:221-24
- Darnton-Hill I, Mkparu UC. Micronutrients in preg- nancy in low- and middle-income countries. Nutrients. 2015;7(3):1744-1768. doi:10.3390/nu703174
- Marchant T, Armstrong Schellenberg JRM, Edgar T, et al. Anaemia during pregnancy in southern Tanza- nia. Ann Trop Med Parasitol. 2002;96(5):477-487. doi:10.1179/000349802125001221
- Suryanarayana R, Chandrappa M, Santhuram AN, Prathi- ma S, Sheela SR. Prospective study on prevalence of ane- mia of pregnant women and its outcome: A community based study. J Fam Med Prim Care. 2017;6(4):739-743. doi:10.4103/jfmpc.jfmpc_33_17
- Oumer A, Hussein A. Knowledge, attitude and practice of pregnant mothers towards preventions of iron deficien- cy anemia in Ethiopia: Institutional based cross sectional study. Heal Care Curr Rev. 2019;7(1):1-7
- Gross K, Alba S, Glass TR, Schellenberg JA, Obrist B. Timing of antenatal care for adolescent and adult pregnant women in south-eastern Tanzania. BMC Pregnancy Child- birth. 2012;12:16. doi:10.1186/1471-2393-12-1
- Samson G. Utilization and Factors Affecting Delivery in Health Facility among Recent Delivered Women in Nkasi District. 2012
- Cappellini MD, Motta I. Anemia in Clinical Practice-Defini- tion and Classification: Does Hemoglobin Change With Ag- ing? Semin Hematol. 2015;52(4):261-269. doi:10.1053/j. seminhematol.2015.07.00
- Tunkyi K, Moodley J. Prevalence of anaemia in pregnancy in a regional health facility in South Africa. South Afr Med J Suid-Afr Tydskr Vir Geneeskd. 2015;106(1):101-104. doi:10.7196/SAMJ.2016.v106i1.9860
- Margwe JA, Lupindu AM. Knowledge and Attitude of Pregnant Women in Rural Tanzania on Prevention of Anae- mia. Afr J Reprod Health. 2018;22(3):71-79. doi:10.29063/ ajrh2018/v22i3.8
- Goldenberg RL, McClure EM, Saleem S. Improving preg- nancy outcomes in low-and middle-income countries. Re- prod Health. 2018;15(1):7-14.
- Tikmani SS, Ali SA, Saleem S, et al. Trends of antenatal care during pregnancy in low- and middle-income coun- tries: Findings from the global network maternal and new- born health registry. Semin Perinatol. 2019;43(5):297-307. doi:10.1053/j.semperi.2019.03.020
- Leyna GH, Berkman LF, Njelekela MA, et al. Profile: The Dar Es Salaam Health and Demographic Surveil- lance System (Dar es Salaam HDSS). Int J Epidemiol. 2017;46(3):801-808. doi:10.1093/ije/dyw324
- Mir MK, Yousaf S, Ilyas A, Tahir S. Maternal anemia is a risk factor for low birth weight babies at term. Pak J Med Health Sci. 2016;10:741-743.
- Menon KC, Ferguson EL, Thomson CD, et al. Effects of anemia at different stages of gestation on infant outcomes. Nutr Burbank Los Angel Cty Calif. 2016;32(1):61-65. doi:10.1016/j.nut.2015.07.009
- Brinkhoff T. Major agglomerations of the world. Published online 2020.
- Idowu OA, Mafiana CF, Dapo S. Anaemia in pregnancy: a survey of pregnant women in Abeokuta, Nigeria. Afr Health Sci. 2005;5(4):295-299. doi:10.5555/afhs.2005.5.4.295
- Lelissa D, Yilma M, Shewalem W, et al. Prevalence of Anemia Among Women Receiving Antenatal Care at Boditii Health Center, Southern Ethiopia. Clin Med Res. 2015;4(3):79. doi:10.11648/j.cmr.20150403.14
- Ali MM, Ngowi AF, Gibore NS. Prevalence and obstetric factors associated with anaemia among pregnant wom- en, attending antenatal care in Unguja island, Tanzania. Int J Community Med Public Health. 2019;6(3):950-957. doi:10.18203/2394-6040.ijcmph20190577
- Massawe SN, Urassa EN, Nyström L, Lindmark G. Anae- mia in women of reproductive age in Dar-es-Salaam, Tan- zania. East Afr Med J. 2002;79(9):461-466. doi:10.4314/ eamj.v79i9.9117
- Ngandango VP. Etiology and risk factors associated with iron deficiency anaemia among pregnant women: a case study of kilosa district, Tanzania. Sokoine Univ Agric. 2018;(2018). https://www.suaire.sua.ac.tz/handle/123456789/2951
- Alem M, Enawgaw B, Gelaw A, Kena T, Seid M, Olkeba Y. Prevalence of anemia and associated risk factors among pregnant women attending antenatal care in Azezo Health Center Gondar town, Northwest Ethiopia. J Interdiscip His- topathol. 2013;1(3):137-144.
- Chowdhury HA, Ahmed KR, Jebunessa F, Akter J, Hossain S, Shahjahan M. Factors associated with maternal anae- mia among pregnant women in Dhaka city. BMC Womens Health. 2015;15(1):77.
- Ndukwu GU, Dienye PO. Prevalence and socio-demo- graphic factors associated with anaemia in pregnancy in a primary health centre in Rivers State, Nigeria. Afr J Prim Health Care Fam Med. 2012;4(1):328. doi:10.4102/phcfm. v4i1.328