
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Case Report - (2022) Volume 7, Issue 4
Lymphedema in Hydrocephalus: A Case Study
Received Date: Oct 12, 2022 / Accepted Date: Oct 18, 2022 / Published Date: Oct 24, 2022
Copyright: ©Khulood Alrashid PT, CLT. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Khulood Alrashid PT, CLT. (2022). Lymphedema in hydrocephalus: A Case Study. Int J Women's Health Care, 7(4), 149-153.
Abstract
Background: Lymphedema is a combination of pathologic condition characterized by excessive local accumulation of interstitial fluid which is rich in proteins [1-3]. It may be an isolated phenomenon or associated with a multitude of other disabling local sequelae or even life-threatening systemic syndromes. In its purest form, the central disturbance is a low output failure of the lymphvascular system, that is, overall lymphatic transport is reduced. Lymphedema can be either primary or secondary [4]. Hydrocephalus is a build-up of fluid in the brain. The excess fluid puts pressure on the brain, which can damage it. Congenital hydrocephalus is when a baby is born with excess fluid in their brain which will cause permanent brain damage such as: speech problems and vision problems [5]
Study Design: The case study was used to highlight the role of physical therapy interventions in the management of primary lower extremity lymphedema in patient with congenital hydrocephalus patient.
Case Description: 37 years-old Saudi female, case of congenital hydrocephalus, deaf, mute, blind with shunting. Patient with severe bilateral lower limb primary lymphedema, which altered her level of function. Referred to physical therapy department by vascular clinic. PT Management and Outcome: The patient received daily sessions of complete decongestive therapy (CDT) for two weeks included: multi-layer bandaging (compression therapy), manual lymphatic drainage, skin / nail care education and decongestive exercises. At the end of second week, the patient’s circumference measurements improved significantly, and her level of independency improved.
Discussion: The case study showed that the physical therapy interventions are safe, effective, in reducing lymphedema and overall quality of life (QOL) with hydrocephalus patients.
Introduction
Lymphedema is a Combination of pathologic condition character¬ized by excessive local accumulation of interstitial fluid which is rich in proteins. It occurs as the result of an imbalance between lymph production and the transport capability of the lymphatic system [1-3].
It may be an isolated phenomenon or associated with a multitude of other disabling local sequelae or even life-threatening system¬ic syndromes. In its purest form, the central disturbance is a low output failure of the lymphvascular system, that is, overall lym¬phatic transport is reduced. Lymphedema can be either primary or secondary. Primary arises from congenital lymphatic dysplasia. Or secondary, anatomical obliteration, such as after radical operative dissection (e g., axillary or retroperitoneal nodal sampling), irradi¬ation, or from repeated lymphangitis with lymphangiosclerosis or as a consequence of functional deficiency (e.g., lymphangiospasm, paralysis, and valvular insufficiency) [4].
Hydrocephalus is a build-up of fluid in the brain. The excess fluid puts pressure on the brain, which can damage it. There are 3 main types of hydrocephalus: 1- Congenital hydrocephalus: hydroceph¬alus that’s present at birth, 2- Acquired hydrocephalus: hydroceph¬alus that develops after birth, 3- Normal pressure hydrocephalus
usually only develops in older people.
Congenital hydrocephalus is when a baby is born with excess fluid in their brain. It can be caused by a condition such as spina bifi-da, or an infection the mother develops during pregnancy, such as mumps or rubella (German measles). Many babies born with hydrocephalus (congenital hydrocephalus) have permanent brain damage. This can cause several long-term complications, such as: learning disabilities, speech problems, memory problems, short attention span, problems with organiza-tional skills, vision problems, such as a squint and vision loss [5]
Study Design
The case study was used to highlight the role of physical thera¬py interventions in the management of primary lower extremity lymphedema in patient with congenital hydrocephalus patient.
Case Presentation
Patient History
37 years-old Saudi female known case of congenital hydrocepha¬lus, deaf, mute, blind with shunting. Referred to physical therapy department by vascular clinic, with severe bilateral lower limb pri¬mary lymphedema, which altered her level of function including ADL’s, reduce mobility, and the fibroses tissue that limits normal range of motion (ROM) and disrupts normal lymphatic drainage.
During the first session a full assessment of the patient was car-ried including setting long and short-term goals. Long term goals: were that the sitter to be independent with manual lymphatic drain¬age techniques, lymphedema prevention and risk factor reduction strategies, maintain reduction of limb girth achieved in phase 1 of treatment, maximize ROM and strength of lower extremities, to reach normal gait pattern, independence with postural correc¬tion in various positions, maximize independency with functional activities and to reduce her bilateral knee pain during movement and walking and tenderness over her skin in bilateral lower ex¬tremities. Long term goals to be met with first follow up visit in 6 months. As for the short-term goals: they were to reduce limb girth by 25-50%, to be independent with home exercise program, and independent with compression bandaging and skin care education
Examination
Observation
• Skin: tight, fibroses, hard and presence of edema in bilateral lower extremities.
• Scars: None.
• Wounds: None.
Palpation/Skin and scar assessment
• Assessment of skin tissue texture: dry skin, presence of deep folds with poor hygiene, brownish and fibrotic tissue over both lower legs.
• Assess scar tissue: None.
Limb Girth
• Classifications of lymphedema using the American system: Severe > 5.0 cm
• Grades or stages of lymphedema according to the Internation¬al Society of Lymphology:
• Grade II: non-pitting edema, brownish skin, not reversible with elevation.
Pain
Bilateral knee pain during movement and walking – the patient screams and cries from this pain and pointing at her knees. Tender to touch, patient tried to express pain with facial expres¬sion.
Sensation
• Assessment of light touch, pain, and proprioception: all intact.
ROM
• Bilateral hips, knees, and ankles: limited.
• End feel: Soft due to presence of edema.
Functional Status
Activities of daily living (ADL): patient’s ADL’s were severely affected due to her special needs and impairment such as dress¬ing: family were struggling with cloths that fits her. Toileting she needed 1-person assistance. Grooming and shower: poor hygiene due to folds and edema, needed 2-person assistant. Transfer and walking: Patient needs 2-person assistance with her activities as she has low endurance and heaviness.
Gait
Patient with antalgic/limping gait as a result of her lymphedema. Patient needs 2-person assistant in walking.
Findings
Patient presents with increased lower limbs size, girth and weight, which had caused loss of lower extremity ROM, and impaired sev¬eral functions such as strength of lower extremities, skin integrity and endurance.
The patient had antalgic/limping gait. In addition, the above im¬pairments contributed to functional independency.
The patient and family unaware about lymphedema treatment and prevention strategies.
Intervention
Daily at the lymphedema clinic for two weeks, treatment included the following at table 1
Table 1: Patient treatment protocol
|
Patient treatment protocol |
frequency |
|
Manual lymphatic drainage |
daily |
|
Skin / nail care and hydrate |
daily |
|
Compression bandage |
daily |
|
Home program: Walking and Decongestive exercises |
20 – 30 minutes daily with compression bandage on. |
Outcomes
After two weeks of treatment the circumference measurements de-creased as shown at table 2, Toileting assistant improved to modify independent and normal gait pattern achieved, with decreased lev¬el of assistant in transfer and walking from 2 persons to 1-person assistant.
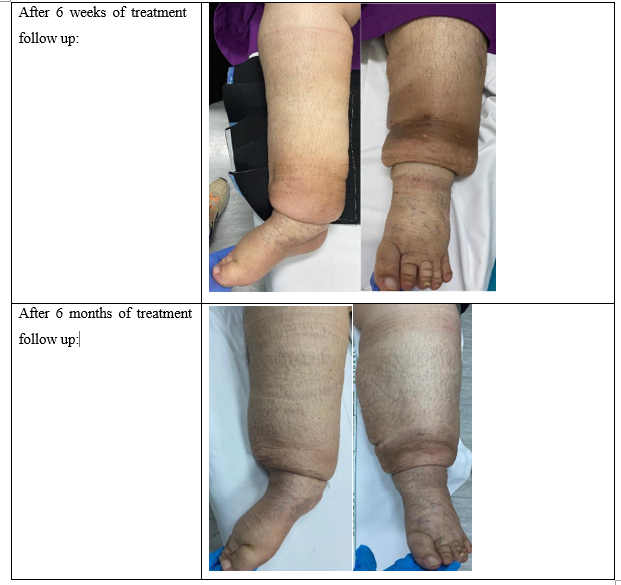
Skin tenderness and sensitivity of touch, bilateral knee pain during movement and walking improved significantly as the patient does not complain of pain after treatment and at 6 months of follow up tender to touch, patient tried to express pain with facial expression.
Skin fibroses, deep folds and skin changes (brownish) improved with compression therapy as shown in the pictures in the table 3. (Consent form was signed by the patient’s family)
Table 2: Circumference measurements before and after the intervention
|
|
Right Leg |
Left Leg |
||
|
Before |
After |
Before |
After |
|
|
Foot zero point (8) |
24 c.m. |
22.5 c.m. |
24.5 c.m. |
22.5 c.m. |
|
Ankle zero point (8) |
49 c.m. |
36 c.m. |
34.5 c.m. |
26.5 c.m. |
|
Mid leg zero point (22) |
45 c.m. |
41 c.m. |
66 c.m. |
40 c.m. |
|
Calf zero point (32) |
51 c.m. |
47 c.m. |
65 c.m. |
47 c.m. |
|
Knee zero point (45) |
50 c.m. |
50 c.m. |
54 c.m. |
49 c.m. |
|
Before treatment: |
|
|
After 2 weeks of treatment: |
|


New Plan of Care
Follow up every six months to review the decongestive exercises, MLD and issuing new compression solution.
New Goals for the Maintenance Phase
Continue with long term goals. To fit the patient with compression garment as her skin in better condition and tenderness improved.
Discussion
Lymphedema is an underdiagnosed, debilitating condition that can directly or indirectly impact patient care. The uncertainty as to when to make the diagnosis of lymphedema, what treatment ap¬proaches are most effective, and the disconnect around recogniz¬ing this condition’s potential influences on progressive disability continues to propagate the idea that it is a “rare, mysterious condi-tion” with few treatment options beyond uncomfortable compres¬sion garments [6].
Based on the result, we strongly supported the physical therapy modalities in the treatment of patient with congenital hydroceph¬alus suffering from primary lower extremities Lymphedema such as: Manual lymphatic drainage, decongestive exercises, compres¬sion bandage, and walking program.
That goes with John B Hamner (2007) who proved that complete decongestive therapy (CDT) can effectively reduce the volume of lymphedema, improve patient’s mobility and increase quality of life [7].
Additionally, CDT has been accepted to be of the most effective treatment protocols for lymphedema. A recent study by Noh et al. which investigated the changing patterns of edema and QoL after CDT included 35 patients with upper limb lymphedema who were applied CDT for two weeks before self-administered home thera-py program [8]. After evaluating the patients with Short Form-36 (SF-36; Korean version), they reported significant improvement in both QoL and lymphedema volumes. A systematic review in-cluding 26 studies about CDT between 2004 and 2011 suggest¬ed results supporting the view that CDT decreases limb volumes and improves QoL [9]. Reduction of limb volume in lymphedema patients induces better physical functionality, decreases fear of movement, and subsequently improves QoL [10].
This case study provides a strong learning opportunity for the ju-nior and newly certified lymphedema therapists to be able to de-sign a complete plan of treatment for lymphedema patients. Fur-thermore, this study provides a basis of care for other patients with similar conditions in the future.
Conclusions
The physical therapy intervention, complex decongestive therapy (CDT) is an effective treatment for primary lymphedema patients with congenital hydrocephalus as it reduces lymphedema, improve patient gait pattern, minimize assistant level and improved QOL.
References
- Foldi, E., & Foldi, M. (2006). Lipedema. Foldi’s Textbook of Lymphology (M Foldi, E Foldi Edn) Munich, germany: Elsevier GmbH, 417-427.
- Kasseroller, R. G. (1998). The Vodder school: the Vodder method. Cancer: Interdisciplinary International Journal of the American Cancer Society, 83(S12B), 2840-2842.
- Kurz, I. (1997). Textbook of Dr. Vodder’s manual lymph drainage. Thieme.
- Document, C., 2016. The diagnosis and treatment of peripheral lymphedema: 2020 Consensus document of the international society of lymphology. Lymphology, 170(1).
- Nhs.uk. 2022. Hydrocephalus. [online] Available at: <https:// www.nhs.uk/conditions/hydrocephalus/> [Accessed 8 October 2022].
- Rodrick, J., & CLT-LANA, W. C. C. The Mystery is Solved: A Case Study of Delayed Diagnosis and Treatment.
- Hamner, J. B., & Fleming, M. D. (2007). Lymphedema therapy reduces the volume of edema and pain in patients with breast cancer. Annals of Surgical Oncology, 14(6), 1904-1908.
- Noh, S., Hwang, J. H., Yoon, T. H., Chang, H. J., Chu, I. H., & Kim, J. H. (2015). Limb differences in the therapeutic effects of complex decongestive therapy on edema, quality of life, and satisfaction in lymphedema patients. Annals of rehabilitation medicine, 39(3), 347-359.
- Lasinski, B. B., Thrift, K. M., Squire, D., Austin, M. K.,Smith, K. M., Wanchai, A., ... & Armer, J. M. (2012). A systematic review of the evidence for complete decongestive therapy in the treatment of lymphedema from 2004 to 2011. PM&R, 4(8), 580-601.
- Yesil, H., Eyigör, S., Caramat, Ä°., & IÅ?ık, R. (2017). Effects of complex decongestive therapy on quality of life, depression, neuropathic pain, and fatigue in women with breast cancer-re-lated lymphedema. Turkish Journal of Physical Medicine and Rehabilitation, 63(4), 329.