
International Journal of Clinical and Medical Education Research(IJCMER)
ISSN: 2832-7705 | DOI: 10.33140/IJCMER
Impact Factor: 0.93


Research Article - (2025) Volume 4, Issue 4
Lymphatic Filariasis and Schistosomiasis Co-Infection in Ilorin Metropolis, Kwara State Nigeria
Received Date: Jul 01, 2025 / Accepted Date: Aug 18, 2025 / Published Date: Aug 29, 2025
Copyright: ©Â©2025 Prosper Omah, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Omah, P., Nmorsi, O. P. G., Egwunyenga, A. O. (2025). Lymphatic Filariasis and Schistosomiasis Co-Infection in Ilorin Metropolis, Kwara State Nigeria. Int J Clin Med Edu Res, 4(4), 01-20.
Abstract
Objectives: The study aimed at the prevalence and possible interaction of schistosomiasis and LF co-infection in Ilorin metropolis.
Methods: Schistosomiasis and LF were investigated using standard methods. The study was carried out in Ilorin Metropolis which consists of three Local Government Areas – Ilorin West, East and South in Kwara State. A sample populations of five thousand eight hundred and fifty (5850) Urine, stools and blood samples were collected from the participants from Ilorin metropolis and investigated in order to determine the prevalence of Schistosomiasis and Lymphatic filariasis and their co-infections A questionnaire consisting of different sections relevant to Schistosomiasis and LF were issued to each participant to obtain information on demographic data. Data were double-entered and cross-checked using Microsoft excel 2016 and computer-based software programme SPSS version 20 (statisti- cal package for social science). Data were analysed using Chi square to test the infected and uninfected.
Result: A total of five thousand eight hundred and fifty (5850) urine, stool and blood samples were collected in the study area from all the selected locations and examined. A total of nine hundred 900(46.2%) urine sample were infected from the inhabitants and were found positive with ova of S haematobium. Six hundred 600(30.8%) stool samples were infected and were found positive for S. mansoni ova while 450(23.1%) blood samples were infected with Wuchereria bancrofti and were found positive. Multiple infection occurred among the subject was common 53(13.4) of subjects were positive for SM also had SH in age >10 as the highest prevalence while co-infection of LF and SH recorded 4(0.21) prevalence, LF and SM recorded 1(0.05) prevalence while 4(0.21) of the subject had the three parasites. The age- specific patterns in the prevalence of infection indicated that the infection cut across all the age bracket with the age group 11-20 recorded the highest prevalence rate of 377(58.0%) for S haematobium out of 650 individual examined,294(45.2%) for S.mansoni out of 650 individual examined with slight difference compared with other age ranges studied The male subject have an overall high- est prevalence rate in the study areas 508 (51.8%) than their female counterparts 392(40.0%) in S.haematobium out of 980 samples examined , 334(34.1%) males and 266(20.7%) female for S mansoni out of 970 samples examined ,253(25.8%) males and 197(20.3%) females for LF due to W.bancrofti .out of 980 and 970 samples examined respectively. The prevalence of schistosomiasis and LF in five (5) occupational groups, shows that Children whose parent occupation was farming recorded the highest rate of prevalence with 345(88.5%) for SH,150(38.5%) for SM,63(41.8%) while least prevalence rate were among children whose father occupation was civil servant with 80(20.5),73(18.7%),53(13.6%). for SH,SM, and LF respectively. Out of Twelve (12) locations used in the study area, Eight (8)) were infected with schistosomiasis infection and LF. The highest individual infected with schistosoma species were those living in Zango with 146(89.5) for SH and 100(61.3) while those living in Oloje recorded the highest rate of prevalence 112(69.1) for LF.. This was closely followed by those living in Alalubosa with 125(77.2),89(54.9 ) for SH and SM respectively while 106(65.0) for LF. Followed by Balogun Fulani with 118(72.4), 78(47.9) for SH and SM respectively and Okoka 88(54.0) for LF. Oloje records the least number of prevalence with 90(55.5),42(25.9) for SH and SM respectively while Alalubosa recorded the least rate of prevalence 66(40.7) for LF.
Conclusion: This finding suggest that co-infections are common in Ilorin metropolis of Kwara State, Nigeria. Children who were infect- ed with schistosomiasis have equal chances of being infected as with LF as they increase in age.
Keywords
Schistosomiasis, Lymphatic Filariasis, Metropolis, Freshwater, Kwara State
Introduction
Schistosomiasis and Lymphatic filariasis (LF) are among the Neglected Tropical Diseases (NTDs) that are prevalent in many of the tropical and sub-tropical developing countries where poverty, ignorant and some cultural beliefs are rampant [1]. These are communicable diseases linked with poverty and are prevalent in areas with poor sanitation, inadequate safe water supply and substandard housing conditions in low income and middle-income countries in Africa, Asia and Latin America with about 534,000 deaths [2,3]. Globally, Schistosomiasis and LF and their impact are gaining increase on the health and the economy of neglected communities which call for global effort to eliminate or eradicate them by 2030 [4,5]. These diseases are common in 149 countries, affecting more than 1.4 billion people (including more than 500 million children) and costing developing economies billions of dollars every year [5]. It is estimated that over a third of the world’s population, mainly those individuals living in the tropics and sub-tropic, are infected by parasitic intestinal helminths [6]. Schistosomiasis and LF are a group of infections that mainly affect people living in remote rural area, urban slums or conflict zones, [7]. Thus, more than 70% of countries and territories affected by Schistosomiasis and LF are low income and lower middle-income countries, and 100% of low-income countries are affected by Schistosomiasis and LF [8]. Over the years attention has been paid to health implications of bacterial, viral, fungal and malaria diseases, neglecting diseases causing potential of so many parasitic diseases [9]. In the United States, there are up to 1.46 million families including 2.8 million children living on less than two dollars a day [10]. In countries such as these, the burdens of neglected tropical diseases are often overshadowed by other public health issues [11].
Schistosomiasis and LF are the most important public-health problems affecting children and adults in sub-Saharan Africa [12]. According to a World Bank study, 51% of the population of sub- Saharan Africa, a major focus for NTDs, lives on less than US$1.25 per day, and 73% of the population lives on less than US$2 per day [13]. In sub-Saharan Africa, the effect of these diseases as a group is comparable to malaria and tuberculosis [14]. Schistosomiasis and LF co-infection can also make HIV/AIDs and tuberculosis more deadly [15]. These diseases are contrasted with the big three diseases (HIV/AIDS, tuberculosis and Malaria), which generally receives greater treatment and research funding [16]. In Nigeria, Schistosomiasis and LF parasitic infections are reportedly and pose a significant health problem among children [17,18]. They are particularly more prevalent in rural communities and are closely associated with poverty [19]. The population of Nigeria account for about 20% of the population of sub-Saharan Africa and globally rank among the top three countries for Schistosomiasis and Lymphatic filariasis [20]. Schistosomiasis and LF are mores common in Nigeria than any other African country, and no country anywhere has more cases of schistosomiasis. LF also endemic in Nigeria and the country has the highest burden of these diseases in Africa. [21].
Nigeria has the greatest number of people infected or at risk with schistosomiasis (29 million), lymphatic filariasis (80-121 million), among all the African nations [22]. In Nigeria, 27million people need protection against Schistosomiasis and Lymphatic filariasis more than any other country in the world [23]. Nigeria identified as a country with the greatest number of cases in sub-Saharan Africa analysis of the so-called high prevalence, such as Schistosomiasis and LF [24]. These diseases are common in 149 Countries, affecting over 1.5 billion around the world, (more than 500 million children), representing 40% of African burden ,3 of every 5 are at risk with 122 million Nigerian are estimated to be at risk while about 1.5 million Kwarans are at risk out of 2.591,555 million population [1,19]. Schistosomiasis and Lymphatic affect many communities in Ilorin metropolis, neighbouring villages especially local farmers causing illness and disfiguring that prevent people from attendance at school and farmings. 16 local government areas in Kwara State were epidemics to schistosomiasis and lymphatic filariasis, Ilorin West was endemic to LF followed by Baruten and Irepolodun Local Government of the State [25]. Schistosomiasis and LF affect many communities in Ilorin metropolis, neighbouring villages especially local farmers causing illness and disfiguring that prevent people from attendance to schools, farming and performing other activities that gives rise to malignant which are very fatal. Ecological modifications have been recognized as major threats to the emergence and re-emergence of Schistosomiasis and LF in Kwara state because they facilitate the breeding of vectors and transmission of parasites [26]. Schistosomiasis and LF transmission is usually seasonal primarily due to the variation in temperature and irrigation cycle.
Materials & Methods
Study Area
The study was carried out in Ilorin Metropolis which consists of three Local Government Areas – Ilorin West, East and South in Kwara State. The following community were sampled: Ilorin West (Adewole, Baboko, Ojo-Oba, Oloje), Ilorin East (Gambari, Oke-Oyi, Alalobosa, Zango), Ilorin South (Fufu, Balogun- Fulani, Akambi, Okaka). Ilorin the state capital of Kwara state is approcimately located on latitude 40 30 and 40 50N and longitude 40 201 and 40 35’ E of the equator. Ilorin City occupies an area of about 468sqkm and it situated at the transitional Lagos and 500km away from Abuja the Federal Capital of Nigeria. As at the 2006 census, it had a population of 777,667 making it the 7th largest City by population in Nigeria [27]. In 2016 it was estimated to be 1,055,500 ranking 6th largest City in Nigeria. The pattern of the drainage system of Ilorin is dendritic. Asa River occupies a fairly wide valley and goes a long way to divide Ilorin into two parts; namely the eastern and the western part. The eastern part covers those areas where the GRA is located while the core indigenous area of Ilorin falls under the western part. Other rivers in Ilorin that drains into Asa river are river Agba, river Alalubosa, river Okun, river Osere, river Aluko, river Yalu, river Odota, river Loma and Lower Niger River Basin dam (LNRB).
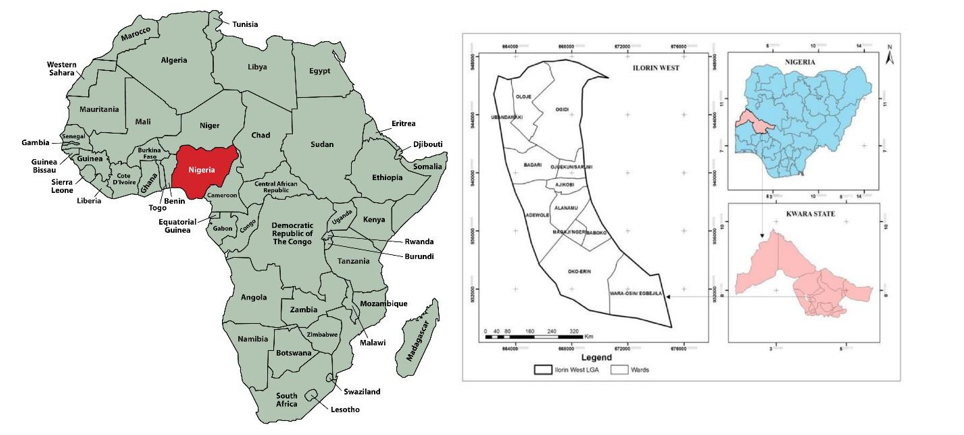
Figure 1: Map of Kwara State, Showing the Study Area
Study Design
This cross sectional study was carried out from October 2019 to August 2023 which spanned through dry and wet seasons to assess the prevalence of Schistosomiasis and LF in Ilorin metropolis, Kwara State. 90% of the samples were hospital-based data from patients attending University of Ilorin teaching hospital (UITH), Kwara State Cottage medical hospital laboratory as well as health centres while the remaining 10% of the samples were drawn from volunteers of the local communities in the study area. This was carried out in Kwara State Cottage medical hospital laboratory, Kwara State for the parasitological examination.
Study Population
A sample population of five thousand eight hundred and fifty (5850) volunteers comprising of (1950 males and females) were recruited for this investigation for urine samples collection ,(1950 males and females) were used for stool samples collection while (1950 males and females ) were used for blood samples collection. This was proportionately allocated based on the population of the Ilorin metropolis. Data such as age, sex, volunteers, parent occupation, types of toilet facilities, source of drinking water and levels of education were obtained from each participant using a well-structured questionnaire.
Participant
The participants comprise the inhabitants of the three local government area in Ilorin metropolis (Ilorin East, West and South) which include male and female, residents in each local government area, age which was categorize as follows: >10, 11-20, 21-30, for Schistosomiasis and 31-40, 41-50, 15 and above for Lymphatic filariasis.
Rapid Assessment Procedure (RAP)
The manifestation of Lymphatic filariasis and Schistosomiasis was assessed by observation of the exposed body parts.
• Lymphatic Filariasis: Manifestation such as shaking, chill, sweating, headache, nausea, elephantoid or filarial fever with temperature reaching 40°C inflammation of various parts of the lymphatic system which becomes swollen and painful, chyluria (presence of lymph in urine) making the urine milky, lymphoedema (especially in lower limbs, scrotum, vulva, breast and arms which becomes swollen and hard).
• Schistosomiasis: Manifestations are abdominal pain, diarrhoea with bloody mucus and pus, hepatosplenomegaly, S. haematobium are appearance of eggs in urine, dysuria, increased frequency of micturition and haematuria (presence of blood in urine) pain in urination. Clinical features include intermittent fever, allergic reactions such as itching and rashes, sweating, swelling in the vulva and vagina, bloody vaginal discharge, cervix lesion with irregular bleeding, backache, ectopic pregnancy.
Administration of Questionnaire
A questionnaire consisting of different sections relevant to Schistosomiasis and LF were issued to each participant to obtain information on demographic data such as age, sex, parent occupation, types of toilet facilities, source of drinking water and levels of education were obtained from each participant. All data were rechecked one after the other to ensure accuracy and to avoid omission and error. (Appendix 1).
Microscopic Examination
• Examination of Stool for the Detection and Quantification of S. Mansoni: Ideal sterile specimen bottles containers made up of waxed cardboard materials with wide mouth, tightly fitting lid or plastic cup with a leak proof were distributed for stool sample collection and instructions were given for proper collection. Kato-Katz was used to quantify the intensity of infection which was proved to be more efficient means of diagnosis of intestinal helminths (Schistosoma mansoni).
• Examination of Urine for the Detection and Quantification of S. Haematobium: Urine samples were processed and analyzed, using filtration method. Sterile and dry ideal universal bottles were distributed for urine collection between the hour of 10.00 am to 2.00 pm. The participants were instructed to collect only terminal drops of urine at least 10ml after a brick walking going up and down the stair case a few times. This was because the last few drops of urine is more productive for S. haematobium eggs or ova and must be collected [25].
• Examination of Blood for Lymphatic Filariasis due to W. Bancrofti: Blood filtration and microscopic evaluation of LF due to W.Bancrofti was prepared using 1ml of coagulated blood using thick blood film. This a prepared by placing a small drop of blood at the middle of dry clean slide. With the edge of another slide an approximately 1cm in diameter made and leave film to dry thoroughly in a flat, level position, protected from flies, dust and extreme heat. This slide was dipped into water and lysed the red blood cells and dried in air fixed in methyl alcohol 2-5 minutes. The slides were placed on a staining rack and flooded with stains (Meyer’s acid haemalum). This slide was warmed by heating for 5-10 minutes. The slides were briskly washed in a jar of water ,dried and examined by focusing film with the x10 objective lens and search for microfilaria .Prevalence and intensity of infection was measured using a direct counting of parasites.
Statistical Analysis
Data were double-entered and cross-checked using Microsoft excel 2016 and computer-based software programme SPSS version 20 (statistical package for social science).
Ethical Consideration /Informed Consent
The ethical consideration was approved and obtained for the ethical committee to the Faculty of Science, Delta State university Abraka, Kwara State Ministry of Health Ethical Committee (MOH/KS//EU//777/354) before the commencement of the study. The sample collection meeting was held with traditional leaders, teachers and communities members for informed consent. Inform written consent was obtained from each adult subject and parents/ guardian of each child during the study detailing the objectives of the study , which includes physical examination, study procedure, collection of small stool and urine in sterile plastic bottles for parasitological analysis; study benefit and potential risk and discomfort , inconvenience as well as precaution such as collection of urine and stool samples were fully explained to adult and children before commencement of the study. Right to refuse, withdraw and also to give consent to participate in the study were requested from the participants.
Results
Summary of Prevalence and Infection of Schistosoma Haematobium, Schistosoma Mansoni and Lymphatic Filariasis
A total of five thousand eight hundred and fifty (5850) urine, stool and blood samples were collected in the study area from all the selected locations and examined. A total of nine hundred 900(46.2%) urine sample were infected from the inhabitants and were found positive with ova of S haematobium. Six hundred 600(30.8%) stool samples were infected and were found positive for S. mansoni ova while 450(23.1%) blood samples were infected with Wuchereria bancrofti and were found positive (Table 1).

Table 1: Prevalence of Schistosoma Haenatobium, Schistosoma Mansoni, and Lymphatic Filariasis
Multiple Infection of Prevalence of Schistomasis and LF Co- Infection in Relation to Age
Table 2 further revealed that multiple infection occurred among the subject was common 53(13.4) of subjects were positive for SM also had SH in age >10 as the highest prevalence while co- infection of LF and SH recorded 4(0.21) prevalence, LF and SM recorded 1(0.05) prevalence while 4(0.21) of the subject had the three parasites.

Table 2: Multiple Infection Prevalence of Schistosomiasis and LF Co-Infection in Relation to Age in Ilorin Metropolis, Kwara State Nigeria
Multiple Infection of Prevalence of Schistosomiasis and LF Co-Infection in Relation to Sex in Ilorin
Co-infections occur among the subject in sex group. Male 126(11.5) subject recorded more multiple infection compare to the female 65(7.6) subject .Sex related multiple infection show significant difference (P<0.05).Table 3.

Table 3: Multiple Infection Prevalence of Schistomasis and LF Co-Infection in Retailoring to Sex in Ilorin Metropolis
Prevalence of Schistosomiasis and LF with Respect to Demographic Factors in Ilorin, Kwara State
The age- specific patterns in the prevalence of infection indicated that the infection cut across all the age bracket with the age group 11-20 recorded the highest prevalence rate of 377(58.0%) for S haematobium out of 650 individual examined,294(45.2%) for S.mansoni out of 650 individual examined with slight difference compared with other age ranges studied. This was closely followed by the age range 21-30 with total prevalence of 275( 42.3% ) out of 650 individual examined in urine and 190(29.2%) in stool in this group for schistosoma ova out 650 individual examined while the least prevalence rate 248(38.2%) ,116(17.8%) were observed in age group >10 for S.haematobium and S.mansoni respectively Table 10. Out of 450 blood samples evaluated for lymphatic filariasis due to W bancrofti from the volunteers, 450 (23.1%) were found positive. The age specific patterns in the prevalence of infection indicated age group 51 and above with the prevalence of 210 (32.3%) Out of 650 samples examined as the highest prevalence among the age groups studied. This was closely followed by age group 41-50 with the prevalence of 160 (24.6%) out of 650 samples examined. In subject with age groups 31-40 the prevalence significantly declines gradually with prevalence of 80 (12.3). Out of 650 samples examined. (Table 4).
The male subject have an overall highest prevalence rate in the study areas 508 (51.8%) than their female counterparts 392(40.0%) in S.haematobium out of 980 samples examined, 334(34.1%) males and 266(20.7%) female for S mansoni out of 970 samples examined ,253(25.8%) males and 197(20.3%) females for LF due to W.bancrofti. out of 980 and 970 samples examined respectively. The overall analysis of the result showed that the infection in males and females did not differ significantly (P< 0.05) Table 4 therefore the null. Hypothesis is rejected that the prevalence is significant within the age and sex range. The result of this study show that the three local government area have a fair knowledge of prevention of schistosomiasis and LF infection, a very high number of the subject population of Ilorin East has the highest rate of prevalence on the three different parasites examined, 404(62.2%) out of 650 individual examined for S.haematobium, 255 (39.2%) out of 650 individual examined for S mansoni and 215(33.1%) out of 650 individual examined LF. The overall analysis of the result showed that the infection in Iloin did not differ significantly
(P< 0.05) .The respondent in the location show that the highest individual infected with schistosoma species were those living in Zango with 146(89.5) for SH and 100(61.3) while those living in Oloje recorded the highest rate of prevalence 112(69.1) for LF. This was closely followed by those living in Alalubosa with 125(77.2),89(54.9 ) for SH and SM respectively while 106(65.0) for LF. Followed by Balogun Fulani with 118(72.4) , 78(47.9) for SH and SM respectively and Okoka 88(54.0) for LF. Oloje records the least number of prevalence with 90(55.5),42(25.9) for SH and SM respectively while Alalubosa recorded the least rate of prevalence 66(40.7) for LF Table 4.


Table 4: Prevalence of Schistosomiasis and LF with Respect to Demographic Factors in Ilorin, Kwara State
Prevalence of Schistosomiasis and LF with Respect to Socio-Economics Factors in Ilorin, Kwara State
Children whose parent occupation was farming 345(88.5%) for SH,150(38.5%) for SM,63(41.8%) had the highest prevalence rate of infection while lower prevalence rate were among children whose father occupation was civil servant with 80(20.5),73(18.7%),53(13.6%). In relation to level of education, it was observed that children whose parent had no education had the highest rate of prevalenece with 280(57.4) for SH, 200(41.1) for SM, 136(27.9) for LF. While those whose parent had the highest level of education recorded the least rate of prevalence 180(37.0), 50(10.2), 77(15.8) for SH,SM and LF respectively. Respondent who uses river/stream/dam as source of toilet facilities recorded the highest rate of infection with 215(55.1) for SH, 169(41.3) for SM, while those that uses bush recorded the highest rate of prevalence for LF. The respondent in the source of water supply, the respondent that uses pond as source of water supply recorded the highest rate of prevalence 242(62.1) for SH while those who uses river/stream/dam recorded the highest rate of prevalence 265(67.9) , 201(51.5) for SM and LF respectively. Table 5.
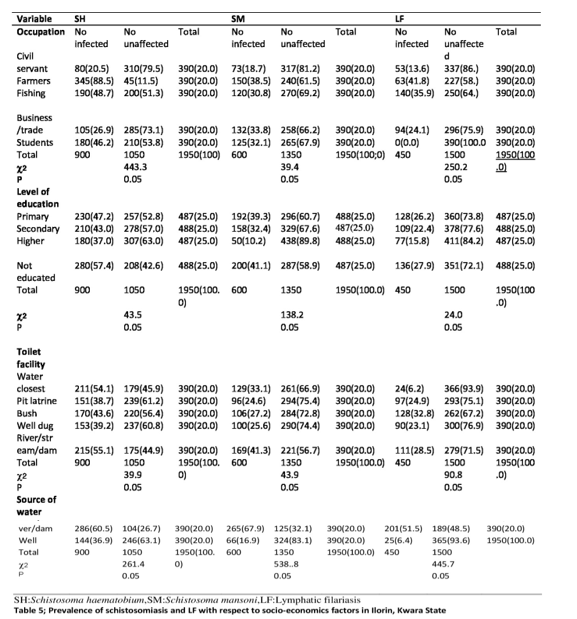
Table 5: Prevalence of Schistosomiasis and LF with Respect to Socio-Economics Factors in Ilorin, Kwara State
Prevalence, Knowledge, and Perception of Schistosomiasis and LF in Ilorin, Kwara State
The respondent that were not aware of the diseases recorded the highest rate of prevalence 678(69.5), 487(49.9), 325(33.3) for SH,SM and LF respectively while those that were aware of the diseases recorded the least rate of prevalence 222(22.8), 113(11.5), 125(12.8) for SH,SM, and LF respectively. In agent of dissemination, those that have not heard of the diseases recorded the highest rate of prevalence 286(73.3) ,270(69.2) 275(70.5) for SH,SM and LF respectively while those that heard through social media recorded the least prevalent rate 57(14.6), 17(4.4), 4(1.0), for SH,SM and LF respectively. Respondent that have no idea of source of infection recorded the highest rate of prevalence 420(86.1), 392(80.3), 276(56.6) for SH,SM and LF respectively. Those whose family income below #50,000 recorded the highest rate of prevalence 462(71.1), 382(58.8), 242(37.2) for SH,SM and LF respectively while those whose family income is above #100,000 recorded the least prevalent rate 156(24.0), 99(15.2), 88(13.5) for SH,SM and LF respectively. Table 6.
Prevalence of Schistosomiasis and LF with Respect to Pack Cell Volume (PCV) in Ilorin, Kwara State
The proportion of participant with low pack cell volume (PCV) with respect to SH,SM, and LF participant infected with SH,SM and LF had significantly higher proportion. Those with PCV less than 30 has the highest rate of prevalence 310(79.5%) for SH,260(66.7%) for SM,220 (56.4%) for LF. The result is in line with those who have no knowledge of PCV with 428(65.8%),288(44.3),196(30.2%) forSH, SM, and LF respectively. Table. The candidates with SM+SH with age group >10 had significantly higher proportion 53(13.2%) of low PCV when compare to candidates without infection. Table 7.

Table 7: Prevalence of Schistosomiasis and LF with Respect to Pack Cell Volume (PCV) in Ilorin, Kwara State
Prevalence, Knowledge and Perception of Lymphatic Filariasis and its Vector in Ilorin, Kwara State
Those that are unaware of the knowledge of the breeding site of mosquito had more prevalent rate with 360(36.9%) while those that are aware of the breeding site had least prevalent rate with 90(9.2%) out of 450 number infected. Most of the participant that had discarded object around them had highest prevalence rare with 215(33.15), followed by those that their answers were don’t know with the prevalent rate of 165(25.4) while those that do not discard object around them had least prevalent with 70(10.8%). The participant that responded ‘don’t know‘ that there is ongoing development activities around them recorded the highest rate of prevalence with 232(35.7), followed by those that responded “Yes” that there is ongoing development activities around them with prevalent rate of 196(30.2) while those that responded “No” that there is no ongoing development activities around them had the least prevalent rate 22(3.4).Those that had plant growing capable of retaining water had the highest rate of prevalence 296(45.5) while those that do not have plant growing capable of retaining water had least prevalent rate 62(9.5). For The participant who do not use house screen net recorded the highest rate of prevalence 218(33.5) while the least rate of prevalence was recorded with those that do not know with prevalence rate of 43(6.6).Table 8.
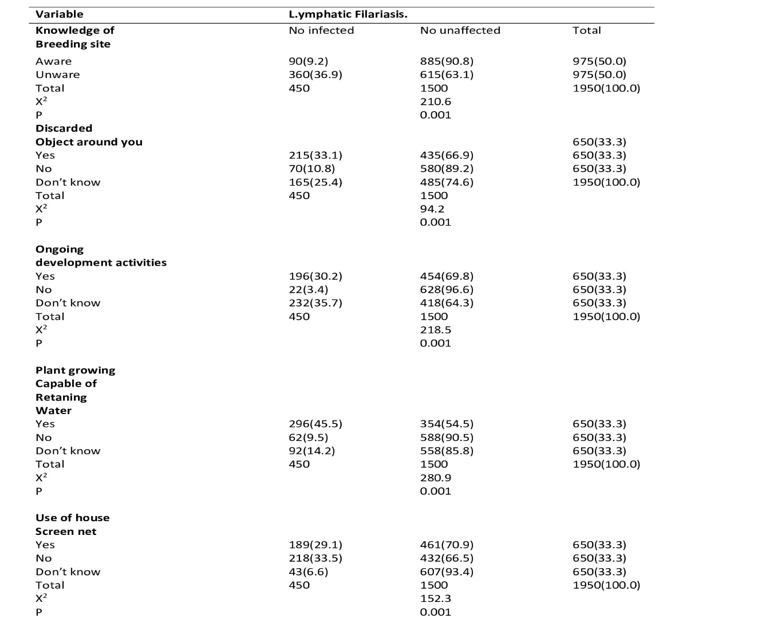
Table 8: Prevalence, Knowledge and Perception of Lymphatic Filariasis and its Vector in Ilorin, Kwara State
Prevalence of Schistosomiasis and LF with Respect to Control Measured in Ilorin, Kwara State
Respondent who have contact with infected water recorded the highest prevalent rate 356(65.6) for SH, 277(71.0 for SM, while those that is having bush around them recorded the highest prevalent for LF 272(69.7).Those that have been infected 5-6 times had the highest rate of prevalence 280(71.8) for SH while those infected 3-4times recorded the highest rate of prevalence 210(53.8) for SM and those 5-6 times recorded the highest rate of prevalence 210(53.9) for LF. In time of drug taken, those that took drug in the year 2020 recorded the highest rate of prevalence 310(63.7), 211(43.3), 156(32.0) for SH,SM and LF respectively. The respondent that recorded effective had the highest rate of prevalence 199(51.0), 161(41.3) for SH and SM respectively while responded moderate recorded the highest rate prevalence 138(35.4) for LF. Table 9.

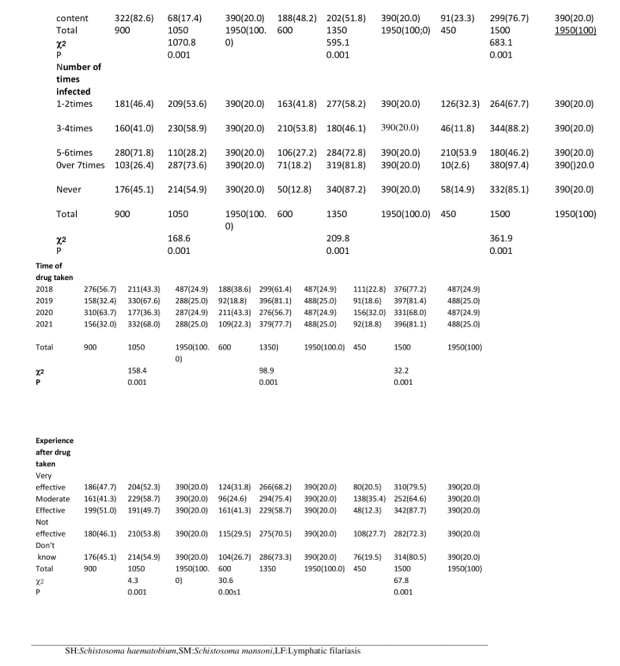
Table 9: Prevalence of Schistosomiasis and LF with Respect to Control Measured in Ilorin, Kwara State
Prevalence of Schistosomiasis with Respect to Contact Activities in Ilorin, Kwara State
The respondent that visited water body had the highest prevalent rate 646(66.3) for SH 482(49.4) for SM. In duration of stay in water body, those that spent all their life recorded the highest rate of prevalent 470(72.3) for SH and 316(48.6) for SM while those that visited few years recorded the least prevalent 118(18.2), 66(10.2) for SH and SM respectively. The respondent that visited the water very often had the highest rate of prevalence 618(95.1) for SH and 370(56.9) for SM while those that have not visited the water at all had the least prevalent 55(8.5), 10(1.5) for SH and SM respectively. The responded who have the reason of visiting the water body for swimming/bath had the highest prevalent rate 282(72.3) and 188(48.2) for SM while those whose reason of visiting the water body “collecting snail” had the least prevalent rate of 98(25.1), 30(7.7) for SH and SM respectively. The participant who had blood in their urine and feces had the highest prevalence 586(90.2), 62(9.5) respectively. Table 10.
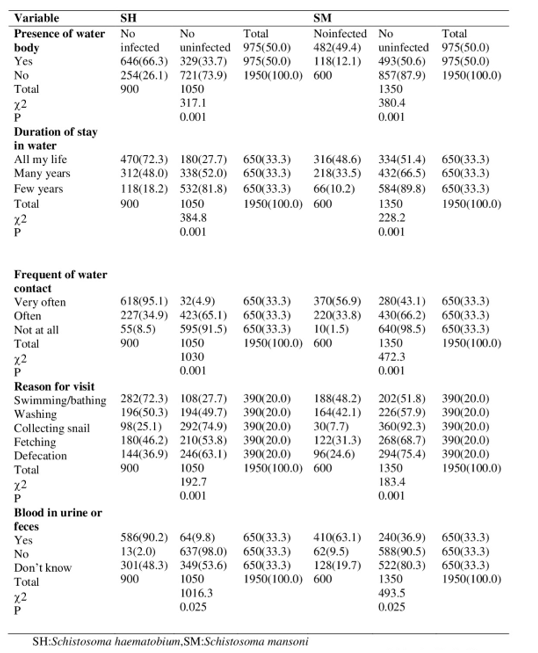
Table 10: Prevalence of Schistosomiasis with Respect to Contact Activities in Ilorin, Kwara State
Prevalence of Schistosomiasis and LF in Different Occupation
The prevalence of schistosomiasis and LF in five (5) occupational groups, (civil servant, farmers, fishing, business/ trade and students) shows that Children whose parent occupation was farming recorded the highest rate of prevalence with 345(88.5%) for SH,150(38.5%) for SM,63(41.8%) while least prevalence rate were among children whose father occupation was civil servant with 80(20.5),73(18.7%),53(13.6%). for SH,SM, and LF respectively.
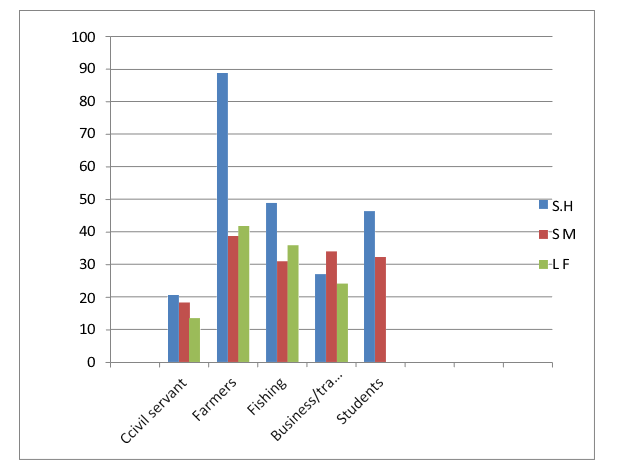
Table 11: Prevalence of Schistosomiasis and LF in Different Occupation in Ilorin Metropolis, Kwara State, Nigeria
Prevalence and Infection of Schistosomiasis and LF in Relation to Location in Ilorin Metropolis Kwara State, Nigeria
Out of Twelve (12) location used in the study area, Eight (8)) were infected with schistosomiasis infection and LF (Balogun Fulani, Akanbi, Okaka, Oke-oyi, Alalubosa, Zango, Ojo-Oba, Oloje). The highest individual infected with schistosoma species were those living in Zango with 146(89.5) for SH and 100(61.3) while those living in Oloje recorded the highest rate of prevalence 112(69.1) for LF. This was closely followed by those living in Alalubosa with 125(77.2), 89(54.9 ) for SH and SM respectively while 106(65.0) for LF. Followed by Balogun Fulani with 118(72.4) , 78(47.9) for SH and SM respectively and Okoka 88(54.0) for LF. Oloje records the least number of prevalence with 90(55.5),42(25.9) for SH and SM respectively while Alalubosa recorded the least rate of prevalence 66(40.7) for LF. The following four (4) locations (Fufu, Gambari, Baboko and Adewole) recorded zero infection. Figure 3. The prevalence of lymphatic filarisis due to W. bancrofti show that the following five locations Akambi, Fufu, Zango, Gambari, Ojo- Oba, Baboko and Adewole shows were not infected in the study area. Figure 3.
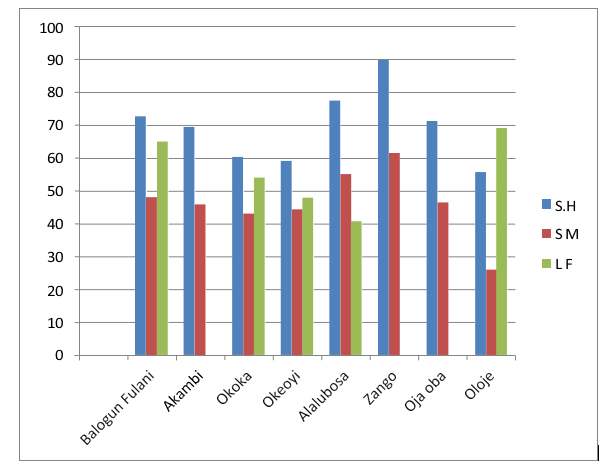
Figure 3: Prevalence and Infection of Schistosomiasis and LF in Relation to Location in Ilorin Metropolis Kwara State, Nigeria
Prevalence and Infection of Schistosomiasis and LF in Regard to Source of Water Supply in Ilorin Metropolis Kwara State, Nigeria
Figure 4 shows the prevalence of schistosomiasis and LF in the metropolis who uses various source of water supply (pond, borehole, tap water, stream/river/ dam, well). Individual who uses pond as source of water supply recorded highest prevalence with 242(62.4) for SH, while those who uses stream/river/dam recorded the highest prevalent rate of 265(67.9) for SM and 201(51.5) for LF out of 1500 each individuals examined .This was closely followed by individual who uses stream/river/dam as sources of drinking water SH, pond 199(51.0) for SM and 196 (50.3) for LF. The least infection occurred on individual who uses borehole as a source of water supply 103(26.4), 27(6.9), 8(2.1) for SH,SM and LF respectively The different in the infection rate of the groups was statistically significant P<0.05 (Figure 4).
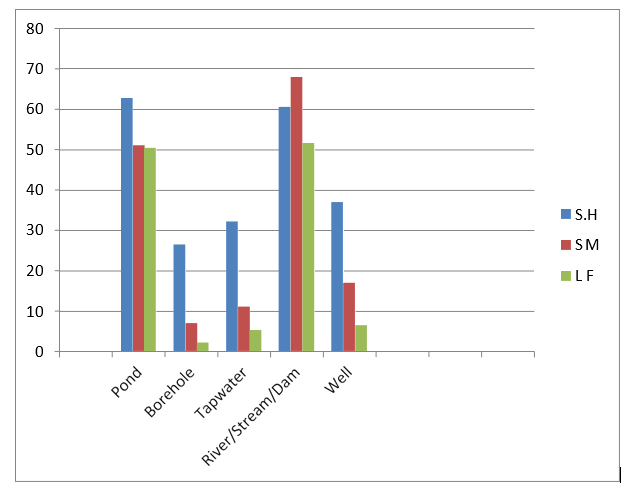
Figure 4: Prevalence of Schistosomiasis and LF in Regard to Source of Water Supply in Ilorin Metropolis Kwara State, Nigeria
Prevalence and Infection of Schistosomiasis and LF in Regard to Toilet Facility in Ilorin Metropolis Kwara State, Nigeria.
With regards to toilet facilities individual who used river/stream/ dam as source of defecation had the highest rate of infection 215(55.1) for SH,169(41.3) and those that uses bush as source of defecation recorded the highest rate of prevalence for LF out of 1950 individual each examined. Table6. This was followed closely with individual who uses water closest as source of defecation with 215(54.1) for SH,129(33.1) for SM and those who uses river/ stream/dam recorded 111(28.5) for LF. Those who uses pit latrine were least infected with slight difference prevalence of 151(38.7) for SH,96(24.6) for SM and those who uses water closet were least infected for LF with prevalence rate of 24(6.2.) Figure 5.
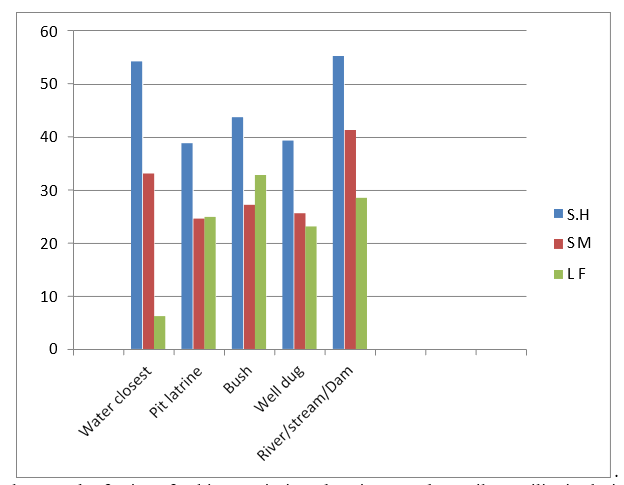
Figure 5: Prevalence and Infection of Schistosomiasis and LF in Regard to Toilet Facility in Ilorin Metropolis
Prevalence and Infection of Schistosomiasis and LF in Regard to Level of Education in Ilorin Metropolis Kwara State, Nigeria
Figure 6 shows that parent in Ilorin metropolis who had no education recorded the highest prevalence rate with 280(57.4) for SH,200(41.1) for SM and 136(27.9) for LF .While parents who obtained higher education qualification recorded the least rate of of prevalence of 180(37.0) for SH,50(10.2) for SM and 77(15.8) for LF. 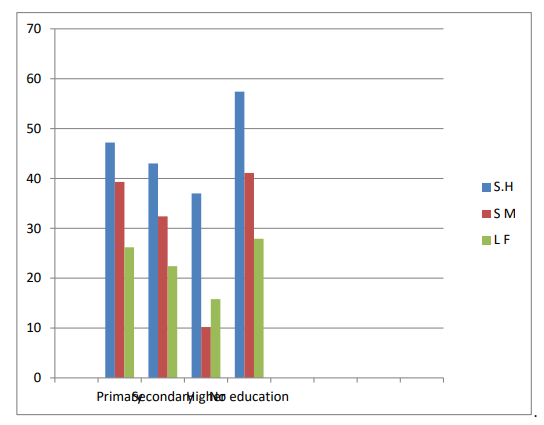
Figure 6: Prevalence of Schistosomiasis and LF Regard to Level of Education in Ilorin Metropolis Kwara State, Nigeria
Discussion
The overall prevalence rate of 33.3% recorded in this study show that Ilorin metropolis, Kwara State Nigeria fall within WHO classification of moderate infection and as endemic. The overall prevalence of 21.0 in this study area is threshold higher than the national Nigerian average of 13% [28]. The findings of S.haematobium, S.mansoni, LF due to W.bancroftico-infection observed in this study are supported by other previous studies in sub-sahara African [29]. The prevalence of co-infection of schistosomiasis and LF is an indication of polyparasitism in the metropolis. The rate of co-infection may be influence not only on chance but also on the spatial distribution of environmental conditions that favour the transmission of multiples species. The co- infection have similar geographical distribution and it is estimated that over a third of the world population, mainly those living in the tropics and sub tropics are affected The prevalence rate of this present study is similar to various reports across Nigeria where Schistosomiasis and LF had been found to be moderately endemic, 34.1% in rural community in Enugu State and 37.9% in Sankwala, Cross River State, [30-32]. These findings are comparable to several reports from many endemics regions in Nigeria and other endemic country such as Senegal, Malawi, Madagascar, Tazania, and Cameroon [33-37]. Factors that may support the prevalence in this study area includes abundance presence of snail vectors, poor sanitary disposal, open air defecation, intense water contact activities observed in this study areas.
In contrast, the result obtained in this study is lower than the reports of who recorded 65.0% in Edo State and who recorded 58.7% in AjaseIpo Community of Ifelodun Local Government, Kwara State [38,39]. who recorded 71.1% in four states (Borno, Niger, Ondo and Ogun) of Nigeria [40]. However, also obtained high prevalence of 54.6% and 51.9% in Ogun State and Niger Delta respectively, Ugbomoiko also reported high prevalence of 62.0% in two peri-urban communities of Southwestern, Nigeria [40,41]. The prevalence rate recorded in this presence study is higher than finding of who reported prevalence of 11.3% and 18.7% in Ohaji/ Egbema LGA Imo State and Niger Benue basin of Kogi State respectively [42]. The differences could be explained by differences in ecological factors that could in turn lead to differences in transmission intensity. Therefore, the recent study call for global intervention and effort to eliminate human Schistosomiasis and LF by 2025 by world health organization should include health education in Schistosomiasis and LF endemic communities of the world [43].
The prevalence of Schistosomiasis and LF were not associated with sex or age group. This may be an indication that both sex and all age groups were being equally exposed to infection through similar water contact activities as there were no cultural barriers against any sex or age group. Our findings on age sex pattern of infection is identical of what is obtainable in many endemic communities in Africa, [44]. The highest prevalence (28.5%) was recorded within the age group (15-24). These age groups have been tremendously characterized with boisterous water related activities such as fishing, washing, bathing and playing that increase the risk of infection in the communities. This probably accounts for high infection rate among the groups. The finding concerning the age disagree with that of in Ogun State with Western Nigeria in 2011, where the peak of infection was within age 8-10, that of who recorded a significant age related increase in prevalence with the age group 13-15 years recording highest prevalence [17,35,38]. In this presence study the prevalence of age group 11-20 recorded the highest prevalence rate of 377(58.0%) for S haematobium out of 650 individual examined,294(45.2%) for S.mansoni out of 650 individual examined with slight difference compared with other age ranges studied significantly decline gradually. A possible explanation to this could be that the participants within the age group may have higher level of awareness about Schistosomiasis transmission and practice more personal hygiene compare to younger age group thus are less exposed to Schistosomiasis and LF infections. This is not an unexpected finding, given that most urban areas in tropical countries including Nigeria is overcrowded and associated with poor sanitary conditions. Parasitic infections persist and flourish whenever poverty, inadequate sanitation and overcrowding are entrenched [19]. This could also be attributed that the age groups (11-20) are involved in more water contact activities and also have higher duration of exposure to infection.
Similarly, the high infections in male than the female suggest the higher exposure risk activities in males than the females. This observations indicates that the sex and other factors are important transmission foci in our study communities and it corroborates findings from many other endemic settings [35,38]. In contrast, reported insignificantly higher prevalence in female than male [42]. Other studies also found that male had higher prevalence of infections compare to their female counter parts [43]. This is agrees in parts with that females possess significantly higher levels of awareness about parasitic infections generally [44]. However, the fact that both sexes had almost the same prevalence agrees with previous report that Schistosomiasis and LF infection were not gender specific in many parts of Nigeria [30]. Many infected male children considered haematuria (blood urine) as a sign of maturity rather than a symptom of infection, belief which has serious implication on the control and treatment of infection.
The pattern of infection among occupational groups indicated that students were more infected than individual in other occupational groups followed by farmers. This observation of the prevalence of Schistosomiasis is in agreement with the reports of [19]. Occupational activities such as farming was a significant risk factor in transmission of infection among the participants as shown by the increase in the prevalence of the diseases. The reason is that parent and their children participate in farming activities and most of their farms are irrigated by water from Schistosomiasis and LF species infected rivers. The higher infection rate among students and farmers could be due to high water contact as the student frequently visit the stream/river/dam for bathing or recreational activities like playing and more importantly farmers unknowingly uses the infected water bodies for the recreational, occupational and domestic activities. These categories of people have water exposure to infection and as a result, constitute sources of infection to the water bodies through which other groups may be infected. This result can be often used for civil servant who recorded zero prevalence and those involves in Business/trade who recorded low prevalence rate.
Despite the availability of well and borehole that serve as major source of water for domestic use in the communities, stream/ river/dam and pond were on the increase and recorded the highest prevalence of infection with statistically significant difference when compared to those that had well and borehole as their domestic source of water. This present study has shown that contact with infected stream/river/dam and pond is significant in the transmission of Schistosomiasis as the participant that had visited and used stream/river/dam and pond showed higher prevalence than those who never visited. This is similar to the findings of who separately concluded that availability of safe water is necessary for reducing the incidence and prevalence of Schistosomiasis and other water related diseases [13,21]. Majority of the population had no access to borehole and tap water. This possibly influence the high frequency and duration of water contact in the community. These findings had demonstrated that Schistosomiasis and LF are endemic and constitute severe morbidity in Ilorin metropolis, Kwara State. Therefore, continuous disease evaluation and implementation of a broad-based public health and socio-economic development that includes provision of clean and safe drinking water and education are essential to prevent the transmission of infection in the endemic areas.
The prevalence of Schistosomiasis was found to be high among individual that uses stream/river/dam as source of toilet facility than those that used bush, well dug drench and pit latrine as source of defecation. This was similar to the study in Republic of China [41]. This is contrary to the reports of who reported that poor toilet facility contributes to the spread of S. haematobium among primary school children when a high prevalence of the disease was discovered among children that practice open defecation [19,37]. The types of toilet facilities available to the inhabitant of the study area had effect on the prevalence of the disease as those who uses water closet and stream/river/dam were more infected than those who uses bushes and pit latrine. This observation is contrary with the work of other researches in different parts of Kwara State and other parts of the country such as [18]. The highest prevalence rate in the individual using stream/river/dam as their source of toilet facilities can be attributed to the inhabitant in such area getting exposed to water bodies harboring the infective stage of the parasite in the vicinity of the water closet and stream/river/dam which they utilized.
Educational background of the parents and their children affected the prevalence of Schistosomiasis in the study area; parents who had not educated recorded the highest prevalence of infection. This could be due to lack of proper knowledge of the disease which leads to inability to properly educate their children about the preventive measure against the disease. One of the major risk factors associated with endemicity of Schistosomiasis in this study area was low parental literacy which lead to others factors such as farming occupational activities of the parents, increased frequency of visit and prolonged duration of stay to the infected water bodies, poor utilization of protective shoes while visiting the river are some of the practice that could place them at yet a greater risk of being infected by the causative agents .This impact of educational backwardness on the distribution of schistosomiasis in rural communities has been reported in Cross River State of Nigeria [39].
For Lymphatic filariasis due to W. bancrofti, the prevalence was higher among the older age group. It was previously observed that the majority of lymphatic filariasis infections in individual living in endemic regions are asymptomatic with the young children being the highest burden of diseases and age asymptomatic infections for most of the time Greenwood The increasing prevalence of lymphatic filariaris with age is due to repeated fly bites couple with possible disease immunity which indicate the long-term chronicity of filariasis [10]. This also confirm why age 55 and above appeared to have more manifestations. Occupations such as farming, fishing and domestic activities bring them close to breeding sites which are known to predisposed person to more biles [16]. The high illiteracy level of the communities implies that health education by print media is not visible, visual aids (pictures) and discussions in local languages are the optimal means to educate the communities [32]. Also, in similar study by on Sabo Penguin in same ecotype of Nigeria, people knowledge and perception of filariasis was just as poor as in this present study in Ilorin metropolis [33].
Factors that may support co-infection of the prevalence of Schistosomiasis and lymphatic filariasis in the study area includes:-Abundance presence of snails and female mosquito vectors, Temperature, humidity, stagnant body of water bushy environment, unhygienic environment and poor drainage, Poor sanitary disposal, Open air defecation, Usage of soil as fertilizer in farming. The occurrence of multiple infection is consistent with reporting other part of the country S. mansoni and S. haematobium had the highest prevalence (9.3), while S. mansoni and LF recorded the least number of infection 1(0.05), 4(0.21) of the subject had the three parasites [35]. This has reported been previously in children and adult and these infections indeed are considered some of the most common parasite diseases of mankind children with parasite co-infections and high parasite had lands to suffer more commonly from reduce cognitive funs, malnutrition, growth retardation iron deficiency, Anemia [25,32,34,43,44].
Conclusion
This finding reported co-infections namely S haematobium,S mansoni and LF, among volunteers in Ilorin Nigeria. The study identified a significant overall prevalence 33.3% for co-infection of these groups which could have a negative effect on the populations of the metropolis. The findings revealed that there were significant associated between co-infection rates and variables such as sex, age group and other factors includes abundance presence of snail vectors, poor sanitary disposal, open air defecation, intense water contact activities observed in this study areas.. play a more potential and critical roles in the prevalence of these infection.
Recommendations
To further explore the result found in this study, we recommend that further study with larger sample size and employing different methods on molecular study which will enable researchers to draw conclusion on Lymphatic filariasis and schistosomiasis.
Acknowledgement
The authors gratefully acknowledge the technical National Institute of Medical Reasearch Yaba Lagos. We also wish to express our profound gratitude to the parents and their children for their voluntary participations In this recent study. We acknowledge the teacher who facilitated the research and aided the translating English language to the local language (dialect).
Conflict of Interest Statement
The authors declared that there is no competing interest
Funding
This research work received no financially support by any institution and no external funding
Data Availability Statement
The data supporting the findings of this study are available from the corresponding auther upon request
Author Contributions
Omah p, performed inclusion, collected all study data and followed all patients. Omah P, Nmorsi O, Egwunyenga A conceptualized designed, analysed ,and involved in interpretation and drafting of the manuscript. All authors read, verified and analysed the data. Nmorsi O approved the final version of this manuscript for publication.
References
- World Health Organization. (2017). Integrating Neglected Tropical Diseases into Global Health and Development: Fourth WHO Report-Executive Summary.
- Vos, T., Flaxman, A. D., Naghavi, M., Lozano, R., Michaud, C., Ezzati, M., ... & Harrison, J. E. (2012). Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. The lancet, 380(9859), 2163-2196.
- Hotez, P. (2009). Neglected diseases amid wealth in the United States and Europe. Health Affairs, 28(6), 1720-1725.
- Farrell, S. H., Truscott, J. E., & Anderson, R. M. (2017). The importance of patient compliance in repeated rounds of mass drug administration (MDA) for the elimination of intestinal helminth transmission. Parasites & vectors, 10(1), 291.
- Xu, Z., Glass, K., Lau, C. L., Geard, N., Graves, P., & Clements, A. (2017). A synthetic population for modelling the dynamics of infectious disease transmission in American Samoa. Scientific reports, 7(1), 16725.
- Eigege, A., Noland, G. S., Adelamo, S. E., Nwodu, K., Sallau, A., Umaru, J., ... & Richards Jr, F. O. (2020). Post-treatment surveillance for lymphatic filariasis in Plateau and NasarawaStates, Nigeria: results of transmission assessment surveys. The American Journal of Tropical Medicine and Hygiene, 102(6), 1404.
- Salazar-Castañon, V. H., Legorreta-Herrera, M., & Rodriguez- Sosa, M. (2014). Helminth parasites alter protection against Plasmodium infection. BioMed research international, 2014(1), 913696.
- Pullan, R. L., Smith, J. L., Jasrasaria, R., & Brooker, S. J. (2014). Global numbers of infection and disease burden of soil transmitted helminth infections in 2010. Parasites & vectors, 7(1), 37.
- Evans, D., McFarland, D., Adamani, W., Eigege, A., Miri, E., Schulz, J., ... & Richards, F. O. (2011). Cost-effectiveness of triple drug administration (TDA) with praziquantel, ivermectin and albendazole for the prevention of neglected tropical diseases in Nigeria. Annals of Tropical Medicine & Parasitology, 105(8), 537-547.
- Kariuki, T., Phillips, R., Njenga, S., Olesen, O. F., Klatser, P. R., Porro, R., ... & Hanne, D. (2011). Research and capacity building for control of neglected tropical diseases: the need for a different approach. PLoS neglected tropical diseases, 5(5), e1020.
- Kastner, R. J., Sicuri, E., Stone, C. M., Matwale, G., Onapa, A., & Tediosi, F. (2017). How much will it cost to eradicate lymphatic filariasis? An analysis of the financial and economic costs of intensified efforts against lymphatic filariasis. PLoS neglected tropical diseases, 11(9), e0005934.
- Richards Jr, F. O., Eigege, A., Umaru, J., Kahansim, B., Adelamo, S., Kadimbo, J., ... & Miri, E. (2020). The interruption of transmission of human onchocerciasis by an annual mass drug administration program in Plateau and Nasarawa States, Nigeria. The American journal of tropical medicine and hygiene, 102(3), 582.
- Adegnika, A. A., & Kremsner, P. G. (2012). Epidemiology of malaria and helminth interaction: a review from 2001 to 2011. Current Opinion in HIV and AIDS, 7(3), 221-224.
- Eigege, A., Evans, D. S., Noland, G. S., Davies, E., Umaru, J., Adelamo, S. E., ... & Richards Jr, F. O. (2017). Criteria to stop mass drug administration for lymphatic filariasis have been achieved throughout Plateau and Nasarawa states, Nigeria. The American Journal of Tropical Medicine and Hygiene, 97(3), 677.
- Pavluck, A., Chu, B., Mann Flueckiger, R., & Ottesen,E. (2014). Electronic data capture tools for global health programs: evolution of LINKS, an Android-, web-based system. PLoS neglected tropical diseases, 8(4), e2654.
- King, J. D., Eigege, A., Umaru, J., Jip, N., Miri, E., Jiya, J., ... & Richards Jr, F. (2012). Evidence for stopping mass drug administration for lymphatic filariasis in some, but not all local government areas of Plateau and Nasarawa States, Nigeria. The American journal of tropical medicine and hygiene, 87(2), 272.
- Hotez, P. J. (2013). NTDs V. 2.0:“blue marble health”— neglected tropical disease control and elimination in a shifting health policy landscape. Plos Neglected Tropical Diseases, 7(11), e2570.
- Ojurongbe, O., Adegbayi, A. M., Bolaji, O. S., Akindele, A. A., Adefioye, O. A., & Adeyeba, O. A. (2011). Asymptomatic falciparum malaria and intestinal helminths co-infection among school children in Osogbo, Nigeria. Journal of research in medical sciences: the oficial journal of Isfahan University of Medical Sciences, 16(5), 680.
- Gyang, V. P., Chuang, T. W., Liao, C. W., Lee, Y. L., Akinwale,O. P., Orok, A., ... & Fan, C. K. (2019). Intestinal parasitic infections: current status and associated risk factors among school aged children in an archetypal African urban slum in Nigeria. Journal of Microbiology, Immunology and Infection, 52(1), 106-113.
- Ajayi, I. O., Afonne, C., Dada-Adegbola, H., & Falade, C.O. (2015). Prevalence of asymptomatic malaria and intestinal helminthiasis co-infection among children living in selected rural communities in Ibadan Nigeria. American Journal of Epidemiology and Infectious Disease, 3(1), 15-20.
- Turner, H. C., Truscott, J. E., Bettis, A. A., Hollingsworth, T. D., Brooker, S. J., & Anderson, R. M. (2016). Analysis of the population-level impact of co-administering ivermectin with albendazole or mebendazole for the control and elimination of Trichuris trichiura. Parasite epidemiology and control, 1(2), 177-187.
- Mupfasoni, D., Montresor, A., Mikhailov, A., & King,J. (2016). The impact of lymphatic filariasis mass drug administration scaling down on soil-transmitted helminth control in school-age children. Present situation and expected impact from 2016 to 2020. PLoS neglected tropical diseases, 10(12), e0005202.
- Kyu, H. H., Abate, D., Abate, K. H., Abay, S. M., Abbafati, C., Abbasi, N., ... & Breitborde, N. J. (2018). Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet, 392(10159), 1859-1922.
- Stone, C. M., Kastner, R., Steinmann, P., Chitnis, N., Tanner, M., & Tediosi, F. (2016). Modelling the health impact and cost-effectiveness of lymphatic filariasis eradication under varying levels of mass drug administration scale-up and geographic coverage. BMJ Global Health, 1(1).
- Afiukwa, F. N., Nwele, D. E., Uguru, O. E., Ibiam, G. A.,Onwe, C. S., Ikpo, A. U., ... & Odoemena, O. F. (2019). Transmission dynamics of urogenital schistosomiasis in the rural community of Ebonyi State, South Eastern Nigeria. Journal of Parasitology Research, 2019(1), 7596069.
- Nigeria Population Commission. (2019). Nigeria demographic and health survey 2018. NPC, ICF.
- Ugbomoiko, U. S., Ofoezie, I. E., Okoye, I. C., & Heukelbach,J. (2010). Factors associated with urinary schistosomiasis in two peri-urban communities in south–western Nigeria. Annals of Tropical Medicine & Parasitology, 104(5), 409-419.
- Sowemimo, O. A., & Asaolu, S. O. (2011). Current status of soil-transmitted helminthiases among pre-school and school- aged children from Ile-Ife, Osun State, Nigeria. Journal of helminthology, 85(3), 234-238.
- Aribodor, D. N., Bassey, S. A., Yoonuan, T., Sam-Wobo,S. O., Aribodor, O. B., & Ugwuanyi, I. K. (2019). Analysis of Schistosomiasis and soil-transmitted helminths mixed infections among pupils in Enugu State, Nigeria: Implications for control. Infection, Disease & Health, 24(2), 98-106.
- Bockarie, M. J., Kelly-Hope, L. A., Rebollo, M., Molyneux,D. H. (2013). Preventive chemotherapy as a strategy for elimination of neglected tropical parasitic diseases: endgame challenges. TRTMHS 2013 368:20120144.
- Akinwale, O. P., Ajayi, M. B., Akande, D. O., Gyang, P. V.,Adeleke, M. A., Adeneye, A. K., ... & Dike, A. A. (2010). Urinary schistosomiasis around Oyan Reservoir, Nigeria: twenty years after the first outbreak. Iranian Journal of Public Health, 39(1), 92.
- Rasoamanamihaja, C. F., Rahetilahy, A. M., Ranjatoarivony, B., Dhanani, N., Andriamaro, L., Andrianarisoa, S. H., & Jourdan, P. M. (2016). Baseline prevalence and intensity of schistosomiasis at sentinel sites in Madagascar: informing a national control strategy. Parasites & vectors, 9(1), 50.
- Ossai, O. P., Dankoli, R., Nwodo, C., Tukur, D., Nsubuga, P., Ogbuabor, D., ... & Eze, G. (2014). Bacteriuria and urinary schistosomiasis in primary school children in rural communities in Enugu State, Nigeria, 2012. The Pan African Medical Journal, 18(Suppl 1), 15.
- Akeh, A. M., Ejezie, G. C., Enyi-Idoh, K. H., Eja, M. E., Agba,A. O., & Ogbeche, J. O. (2010). Urinary schistosomiasis, perception and treatment-seeking behaviour in Sankwala, Cross River State, south-eastern Nigeria. Nigerian Journal of Parasitology, 31(1).
- Barnabas, B., Aliyu, M., Gbate, M., Obi, P., Ezeako, I., et al. (2011). prevalence of schistosomiasis and other Intenstinal Helminth parasites among school children in Bida, Niger State. Niger J Sci, 48, 621-626.
- Amuta, E. U., Houmsou, R. S., et al. (2014). prevalence, intensity of infection and risk of urinary schistosomiasis in pre- school and school aged children in Guma Local Government Area, Nigeria. Asian pac J Trop Med, 1, 34-39.
- Babatunde, T. A., Asaolu, S. O., & Sowemimo, O. A. (2013). Urinary schistosomiasis among pre-school and school aged children in two peri-urban communities in Southwest Nigeria. Journal of parasitology and vector biology, 5(7), 96-101.
- Senghor, B., Diallo, A., Sylla, S. N., Doucouré, S., Ndiath,M. O., Gaayeb, L., ... & Sokhna, C. (2014). Prevalence and intensity of urinary schistosomiasis among school children in the district of Niakhar, region of Fatick, Senegal. Parasites & Vectors, 7(1), 5.
- Mtethiwa, A. H., Bakuza, J., & Nkwengulila, G. (2015). Prevalence and intensity of Schistosomiasis in communities around water reservoirs in Malawi. J Trop Dis, 4(183), 2.
- Ugbomoiko, U. S., Ofoezie, I. E., Okoye, I. C., & Heukelbach,J. (2010). Factors associated with urinary schistosomiasis in two peri-urban communities in south–western Nigeria. Annals of Tropical Medicine & Parasitology, 104(5), 409-419.
- Mazigo, H. D., Nuwaha, F., Kinung’hi, S. M., Morona, D., de Moira, A. P., Wilson, S., ... & Dunne, D. W. (2012). Epidemiology and control of human schistosomiasis inTanzania. Parasites & vectors, 5(1), 274.
- Ekpo, U. F., Laja-Deile, A., Oluwole, A. S., Sam-Wobo, S. O., & Mafiana, C. F. (2010). Urinary schistosomiasis among preschool children in a rural community near Abeokuta, Nigeria. Parasites & vectors, 3(1), 58.
- Nworie, O., Nya, O., Anym, C., Okoli, C. S., Okonkwo, E. C., et al. (2012). Prevalence of urinary Schistosomiasis among primary school children in Arikpo North Local GovernmentArea of Ebonyi State. Annals Biol Res, 3(8), 3894-3897.
- James, S. L., Abate, D., Abate, K. H., Abay, S. M., Abbafati,C., Abbasi, N., ... & Briggs, A. M. (2018). Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The lancet, 392(10159), 1789-1858.