
Journal of Educational & Psychological Research(JEPR)
ISSN: 2690-0726 | DOI: 10.33140/JEPR
Impact Factor: 1.4

Research Article - (2026) Volume 8, Issue 1
“Lost in the System”: Australian Primary School Teacher Perspectives on ADHD Inclusion, a Bioecological, Qualitative Study
Received Date: Nov 11, 2025 / Accepted Date: Dec 19, 2025 / Published Date: Feb 23, 2026
Copyright: ©2026 Melanie Porter, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Vamos, F., Porter, M., Lu, S. (2026).
Abstract
In Australia, students with Attention-Deficit/Hyperactivity Disorder (ADHD) are marginalised learners who often face barriers to school participation that can compromise long-term social, academic, and mental-health outcomes. ADHD diagnostic criteria specify symptom onset before age 12 years, making primary school a critical period for recognition and support. Teachers’ professional judgment is, therefore, central to identifying attentional and behavioural difficulties, initiating referrals, and mitigating risk. Despite national commitments to inclusion, ADHD remains insufficiently recognised in disability frameworks, making support difficult to access and placing greater pressure on teachers to respond without adequate resources. This study aimed to: (1) clarify how current inclusion policy is experienced in classroom practice and (2) identify the supports that teachers view as necessary for the inclusion of these students. Semi- structured interviews were conducted with six primary teachers from mainstream and special educational settings across New South Wales, representing independent, Catholic, and public sectors. A critical realist stance and the bioecological person-process-context-time model guided an interpretative phenomenological analysis [1]. Three superordinate themes were identified: (1) ADHD inclusion’s blind spot, where teachers described ADHD as simultaneously invisible and excluded from policy; (2) systemic constraints and pedagogical gaps, highlighting unmet training needs and systemic barriers; and (3) meaningful change through relationships, collaboration, and lived experience, demonstrating how these factors may enable inclusion. This is the first Australian study to qualitatively explore primary teacher perspectives on ADHD. Findings expose the gap between policy aspiration and classroom reality, providing evidence for explicit ADHD policy recognition, accessible and ADHD-specific teacher training, and system-wide collaboration to achieve sustainable and meaningful inclusion for students with ADHD in Australian classrooms.
Keywords
Teacher, Education, Training, Development, Qualitative, Interviews, InclusionIntroduction
This thesis explores how primary school teachers understand and enact the inclusion of students with Attention-Deficit/ Hyperactivity Disorder (ADHD) in primary school classrooms. Throughout, the researcher adopts person-first language, which centres the individual rather than the diagnosis, consistent with the Australian ADHD Professionals Association language guidelines [2]. At the same time, it is acknowledged that some neurodivergent individuals prefer identity-first terminology as a form of self-advocacy.
Inclusive education has emerged as a core priority in contemporary schooling reforms, emphasising that all students, regardless of ability, background, or need, should have equitable access to participation in mainstream classrooms [3]. In Australia, this principle is embedded in legislation such as the Disability Standards for Education, which mandate reasonable adjustments, removing barriers that restrict students with disability from accessing education on the same basis as their peers [4]. Despite these commitments, ADHD remains insufficiently addressed within the Australian educational system [5].
ADHD is the most commonly diagnosed neurodevelopmental disorder of childhood, affecting approximately 8.2% of Australian school-aged children [6]. As such, students with ADHD represent a substantial proportion of mainstream classrooms, yet they encounter disproportionate barriers to inclusion. This under-recognition is reflected in ADHD’s exclusion from the Australian Government Department of Education’s Nationally Consistent Collection of Data on School Students with Disability, despite the close alignment between its adjustment categories and the supports typically required by students [7]. The consequences are significant: Students with ADHD face heightened academic, social, and developmental risks [8]. Evidence highlights primary school as a promising window for intervention, when patterns of learning, belonging, and self-concept are established [9,10]. Ultimately, this prevalence-policy disconnect raises questions regarding how ADHD inclusion is conceptualised and implemented in Australia, particularly considering inclusive educational reforms articulated by the Disability Royal Commission into Violence, Abuse, Neglect and Exploitation of Persons with Disability [11].
Understanding ADHD inclusion requires a theoretical lens that captures how individual, environmental, cultural and temporal factors interact to shape child development. While sociocultural theory and developmental systems theory emphasise reciprocal child-context influences, they offer limited attention to the multilevel systemic forces operating within schools [12,13]. Accordingly, the refined bioecological person-process-context-time (PPCT) framework is adopted as the guiding theoretical lens for this thesis [1,14]. Extending on the original bioecological model, the PPCT framework emphasises proximal processes, conceptualised as the enduring, bidirectional interactions through which child development occurs [15]. Crucially, it links these processes to wider systems, illustrating how macro-level forces (e.g., policy agendas) cascade into school and classroom conditions, shaping children’s experiences (see Figure 1). Within this framework, teachers’ interpretations are situated within institutional and temporal contexts that constrain or enable inclusion, emphasising their influential role as proximal figures in child development. Importantly, teacher interpretations can determine whether a child receives support, is referred for assessment, or is instead subjected to discipline [16,17]. The following section critically examines the diagnostic constructs and theoretical framings that shape how ADHD is understood within educational contexts, providing the foundations for exploring how teachers experience and enact inclusion in practice.

Note. Adapted from Bronfenbrenner and Morris, informed by Butcher and Lane [1,18]
Figure 1: The Bioecological PPCT Model Situating the Child with ADHD
ADHD Diagnostic and Theoretical Critique
ADHD, as defined by the Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM-5-TR), is characterised by persistent, developmentally inappropriate symptoms of inattention and/or hyperactivity-impulsivity, with onset before age 12 years [19]. Diagnosis typically occurs between ages five and nine, aligning with the primary school years in Australia [20]. This positions teachers as central to recognising early difficulties and commonly initiating assessment and management [16]. Diagnostic assessment relies partially on behavioural checklists and rating scales completed by parents, teachers, and, in some cases, the child, making it vulnerable to sociocultural and gender-related biases [19,21,22].
Early theoretical models have shaped how ADHD is conceptualised in schools, often through deficit-based framings that influence teacher expectations and classroom responses [23]. Barkley’s model posited deficits in behavioural inhibition, the ability to suppress inappropriate or impulsive behaviours, at the core of ADHD [24]. Later work extended this model to broader executive functioning deficits, including challenges with working memory, planning, and self-regulation [25]. These cognitive processes are critical for everyday functioning and are implicitly required in classroom contexts where students must sustain attention, follow instructions, wait turns, and remain seated [26,27].
Executive dysfunction is often misinterpreted in school contexts, where behavioural manifestations are often attributed to defiance or poor motivation rather than neurodevelopmental differences [27]. For example, in Moore et al.’s qualitative United Kingdom study, teachers attributed children’s difficulties to individual deficits without considering how classroom structures compounded such challenges [28]. Similarly, a qualitative systematic review by Gwernan-Jones et al.’s found that rigid behavioural expectations in classrooms could trigger ADHD symptoms [29]. Educators often overlooked these contextual factors and misattributed difficulties to the student or family, thereby perpetuating misunderstanding and stigma, and limiting support [29]. This mismatch between students’ executive capacities and school behavioural norms leaves ADHD-related behaviours particularly vulnerable to punitive and exclusionary responses [27,29]. ADHD Australia’s national inquiry reported that one in four students with ADHD had been suspended for behaviours associated with their diagnosis [30]. Together with documented higher rates of detention, suspension, and expulsion, this illustrates how executive function difficulties are frequently misconstrued. Mainstream classrooms therefore present substantial challenges for students with ADHD [8,31].
Symptom variability presents an additional barrier to recognition, influencing how readily difficulties are noticed, interpreted, and addressed in schools [32]. The DSM-5-TR recognises three clinical presentations: inattentive, hyperactive/impulsive, and combined, each of which can manifest differently in any given child [19]. Inattentive symptoms, such as distractibility, disorganisation, and forgetfulness, are often internalised and can be overlooked, particularly among female students [33,34]. By contrast, hyperactive/impulsive symptoms such as excessive movement, interrupting others, and difficulty waiting, are more overt and prevalent among male students, prompting earlier referral and reinforcing gendered diagnostic biases that privilege observable behaviours [21]. Combined presentations, characterised by both inattentive and hyperactive/impulsive traits, are associated with overlapping inattentive and hyperactive/impulsivity challenges [19]. Symptom heterogeneity may complicate ADHD identification; without ADHD-specific training, teachers may misattribute ADHD symptoms to shyness, laziness, defiance, or moral failings, thereby reinforcing stigma and delaying timely support [35,36].
Beyond symptom heterogeneity, recognition is complicated by intersecting factors. Ethnicity and perceived intellectual ability may bias teacher perceptions of the students’ needs [37-40]. Common coexisting conditions may complicate early detection: autism spectrum disorder, anxiety and mood disorders, and specific learning disorders can obscure ADHD symptoms and delay intervention [19,41,42]. Additionally, the phenomenon of masking, whereby students may consciously suppress or conceal ADHD traits to conform to perceived norms, further contributes to underrecognition [43]. Without adequate teacher knowledge, these complexities may be misunderstood or overlooked, particularly in students who internalise symptoms or lack family support [34,44,45]. These issues reflect the limitations of diagnostic systems built on narrow, unrepresentative samples and underscore the interpretive role of teachers [21].
Debates over the legitimacy of ADHD present an additional layer of complexity. Some sociocultural critiques argue that ADHD reflects the medicalisation of behaviours that deviate from normative expectations within specific cultural contexts [46-48]. While such perspectives highlight the influence of social norms in shaping diagnostic criteria, they risk overlooking the lived realities of those affected. Individuals with ADHD consistently report long¬term academic struggles, social exclusion, and internalised shame arising from feeling different in systems that are not designed to accommodate neurodevelopmental difference [8]. These accounts highlight the risks of dismissing ADHD as a socioculturally constructed label and underscore the need for educational responses grounded in both critical analysis and lived experience. Collectively, diagnostic limitations, theoretical framings, and legitimacy debates shape how ADHD is understood and addressed by teachers, positioning their perspectives as central to improving inclusive practice [49].
Key Research on ADHD at School
Quantitative systematic reviews consistently demonstrate the academic, social, and developmental risks associated with ADHD [8]. Compared with neurotypical peers, children with ADHD demonstrate lower academic achievement, reduced school engagement and higher rates of incomplete schoolwork [50]. They are also at greater risk of experiencing social difficulties, including increased vulnerability to peer rejection, victimisation, and bullying [51-53]. These challenges are often compounded by strained teacher-student relationships, which can undermine school belonging, a recognised protective factor for both mental health and educational success [26,54]. In contrast, positive teacher-student relationships promote resilience, belonging, academic participation, and engagement. Together, this evidence positions belonging and teacher-student relationships as important mediators of outcomes for students with ADHD [54]. However, systematic reviews, while methodologically rigorous, cannot account for how varied developmental pathways lead to similar outcomes [55]. This limitation overlooks the principle of equifinality, whereby multiple pathways converge on similar outcomes, an essential concept for understanding the diversity of ADHD trajectories [55,56].
Longitudinal studies extend this evidence by demonstrating how early challenges compound across the lifespan [57-59]. ADHD in childhood has been linked to later coexisting mental health conditions, social exclusion, unemployment, and criminal justice involvement [57,60-62]. By following children over time, these studies confirm the sequencing of early symptoms into later risks [63]. However, these studies cannot completely account for how structural, educational, and policy environments shape these trajectories, leaving the mechanisms of disadvantage only partially understood [64].
Neurodevelopmental accounts emphasise childhood as a critical intervention window, and emerging evidence supports the value of school-based approaches during this period [10]. A systematic review and meta-analysis of 26 school-based randomised controlled trials (1980-2024) found that school interventions (e.g., a combination of school-adjustments and skill-training for children) improved ADHD symptoms, inattention, academic performance, social skills, and externalising behaviours [9]. Although effect sizes were small, interventions delivered in primary school demonstrated greater impact on combined symptom presentations and academic skills than those delivered in high school [9]. Despite this promise, policy omission and systemic barriers limit access to support, constraining teachers’ capacity to respond effectively.
Australian Policy Critique
Despite the well-documented risks and the promise of early intervention, ADHD remains marginalised within Australian disability policy [8,9]. This omission has tangible consequences: Sciberras et al. estimated that ADHD imposes an annual economic burden of US$12.76 billion in Australia, underscoring the urgency of explicit policy recognition [65]. The ADHD Senate Inquiry represented a significant step towards such recognition, with 700 submissions highlighting barriers to support, particularly in education [66]. Despite this, children with ADHD continue to face substantial difficulty securing funded educational support. Under current policy frameworks, a diagnosis of ADHD alone does not meet eligibility criteria for disability support; access generally depends on the presence of a recognised coexisting condition [67]. For example, while the NCCD formally recognises diagnoses such as autism, ADHD is subsumed under broad, non-specific categories [7]. As a result, students without coexisting diagnoses are less likely to attract funding, with only 4% estimated to qualify [68]. These policy gaps intersect with a teacher workforce experiencing significant strain. High workloads and unsustainable stress levels are key drivers of national teacher shortages, prompting the National Teacher Workforce Action Plan [7,69]. Importantly, in the absence of funded supports, teachers’ capacity to meet the educational needs of students with ADHD is compromised.
The Disability Royal Commission reignited debates about Australia’s capacity for inclusive education [11,70,71]. Recommendation 7.14 proposed phasing out special educational settings in favour of a fully inclusive mainstream system by 2052, generating significant debate [70-73]. Armstrong argued that the Commission’s framing of inclusion was constrained by a binary logic of ‘mainstream’ versus ‘special’ settings, diverting attention from the systemic and pedagogical reforms needed for authentic inclusion [70]. Likewise, Iacono contended that the Commission failed to engage adequately with existing inclusive education research or evidence-based models of interdisciplinary support [71]. These critiques are pertinent to ADHD: despite extensive evidence of risk, and the promise of early intervention, ADHD remains relatively absent in current funding and policy structures [8,9].
Importantly, The ADHD Senate Inquiry, the Disability Royal Commission, and the National Teacher Workforce Action Plan occurred concurrently, yet show limited evidence of integration. The absence of a coordinated political agenda represents a significant barrier to systemic reform. From a PPCT perspective, inclusion is a multisystemic process shaped by interactions between policy, institutional conditions, and proximal relationships [1]. Effective reform must, therefore, respond to the teaching workforce, and to the distinct needs of students with ADHD [49,69]. In this context, teachers’ perspectives are essential for understanding how policy gaps manifest in practice and for identifying the changes required for authentic and sustainable inclusion. However, these perspectives remain largely absent from policy discourse, reinforcing the need to examine how teachers make sense of ADHD inclusion
Teachers: On the Frontline of Inclusion
Positioned at the intersection of policy and practice, teachers are required to interpret and enact policy expectations within the everyday realities of accommodating diverse learner needs [49]. However, Australian pre-service programs devote little time to ADHD-specific training, leaving many graduates underprepared to recognise and support neurodivergent students [74]. Consistent with this, Australian studies report low baseline knowledge and confidence among teachers in supporting students with ADHD [75,76]. Targeted professional learning has been shown to improve teacher knowledge, confidence, and practice, as evidenced in Latouche and Gascoigne’s study involving 274 teachers, and Porter et al.’s mixed-methods study involving over 2,000 Australian teachers [75,76]. However, access to such training is constrained by workload demands and time pressures. Rural teachers in particular describe training opportunities as inaccessible, despite motivation to upskill [77]. This misalignment between teacher intent and feasibility remains a barrier to inclusion.
Beyond pedagogy, teacher-student relationships are central to student outcomes. Attachment theory conceptualises teachers as secondary attachment figures who provide emotional security and stability in schools [78,79]. Strong and secure teacher-student relationships promote engagement and belonging, whereas conflictual relationships, especially in the context of disruptive behaviours, undermine these benefits for students with ADHD [67,80,81]. The coping-competence-context theory links disruptive behaviours to teacher stress, a pathway supported by meta-analytic evidence associating student misbehaviour with teacher stress and burnout [82,83]. These issues are of concern in the Australian context, where stress and burnout are identified contributors to high attrition rates [69]. Moreover, stress can reduce teacher self-efficacy, defined in social cognitive theory as an individual’s perceived capacity to achieve a goal, which is critical for managing challenging behaviours [84,85]. Reduced self-efficacy not only affects teachers’ wellbeing but can diminish the quality of support provided to students [86].
Teachers play a key role in building home-school partnerships, which are particularly important for early intervention yet are frequently strained in the context of ADHD [87]. Teachers report difficulty navigating varied caregiver responses to support-seeking and pharmacological intervention, while parents often feel blamed by teachers for their children’s challenges [29,88]. In ADHD Australia’s national inquiry, parents reported that teachers lacked the knowledge needed to support their children effectively [30]. These divergent perspectives can undermine cohesion and leave students without consistent support [29].
Addressing these challenges requires moving beyond quantification to examine how teachers interpret and negotiate their responsibilities within policy and classroom constraints. Qualitative approaches are well suited to exploring meaning-making, offering insight into how teachers navigate systemic pressures, relational dynamics, and accountability expectations [89]. Teachers’ voices are central to authentic inclusion, as they are the professionals working in closest proximity with students [90]. Despite this, few qualitative studies have centred their voices [91].
International and Australian Qualitative Research
International qualitative research has highlgihted the systemic and relational challenges that teachers face when accommodating ADHD in classrooms. Common findings include inadequate preparation and access to training, insufficient ADHD knowledge, and the emotional toll of disruptive behaviours, particularly within teacher-student relationships [38,91-94]. Collectively, these accounts converge on the inadequacy of systemic supports for meaningful inclusion [92,94]. Wilson et al., for example, examined Scottish teachers’ attitudes towards ADHD inclusion and identified a gap between policy expectations and classroom realities [49]. Despite legislative commitments to inclusion, teachers reported that ADHD was often deprioritised relative to other conditions, with some even questioning its legitimacy [49]. While such studies enrich quantitative research with lived experience, few have focused exclusively on teachers or situated their experiences within the broader educational ecology, limiting understanding of the structural and contextual factors that may constrain practice [18,28,49]. Moreover, research from Western, Educated, Industrialised, Rich, and Democratic (WEIRD) contexts may be thematically relevant, however, generalisability is limited by differences in education, policy and funding frameworks [95].
In Australia, teacher-centred qualitative research on ADHD is limited. Existing studies have largely focused on parents or students or used survey methods that constrain nuance (e.g., [17,96-98]. In the high school context, Gibbs identified disparities between school leaders’ and teachers’ understandings of differentiated instruction, underscoring the importance of systemic collaboration for inclusive practice [99]. However, to the researcher’s knowledge, no prior study has qualitatively examined Australian teachers’ perspectives on ADHD in primary schools. This is a notable omission given primary school is the developmental period during which attentional and behavioural challenges typically emerge, and formal identification often occurs [16]. The current context of inclusive education reform amplifies the need for such inquiry. Without insight from those responsible for enacting policy in classrooms, reforms risk misalignment with practice and may overlook the needs of students with ADHD during foundational educational years [16].
The Present Study
In response to the identified gap, the present study is the first in Australia to qualitatively explore primary school teachers’ perspectives on ADHD inclusion. Using interpretative phenomenological analysis (IPA), the study had two aims: (1) clarify how current inclusion policy is experienced in classroom practice, and (2) identify the supports that teachers view as necessary for the inclusion of students with ADHD. Consistent with IPA’s exploratory nature, no a priori hypotheses were posited [100]. Instead, the study was guided by the research question: How do Australian primary school teachers make sense of inclusion reforms in relation to supporting students with ADHD?
Methods
Research Design
IPA is a qualitative approach that generates detailed, idiographic accounts of how individuals make sense of their lived experiences within specific sociocultural and institutional contexts, capturing both shared and unique aspects among a homogenous group [101]. By accessing individuals’ subjective meaning-making, IPA transcends the limits of quantitative methods in educational research [102]. Its contextual sensitivity, participant-led focus, and depth of exploration make IPA well suited to this exploratory study. IPA rests on a strong theoretical foundation that shapes its methodology, analysis, and interpretation of findings, and its integrity is bolstered by firm epistemological and ontological commitments [100]. Alternate qualitative approaches were considered but deemed less suitable; for example, descriptive phenomenology focuses solely on describing lived experience without interpretative engagement [103]. Similarly, thematic analysis, while useful for identifying patterns, does not provide the idiographic depth required to explore each teacher’s unique experiences [104].
Ontology and Epistemology of IPA
Ontology concerns the nature of reality, what exists and how it is structured, while epistemology addresses how that reality is accessed and understood [105]. This study adopts critical realism as its ontological position, assuming that material and systemic structures (e.g., NCCD funding criteria and broader reforms) exist independently of human perception and exert real effects on teachers’ experiences [106-108]. Epistemologically, critical realism holds that although reality is stable, our knowledge of it is necessarily subjective and mediated by human interpretation, since all information is filtered through language, culture, and perception [109]. This distinction is key as epistemology is not reducible to ontology under critical realism, meaning that while a stable reality is assumed, our access to it remains partial and situated. This stance underpins the use of IPA, which embraces the double hermeneutic, where participants interpret their experiences and the researcher makes sense of these interpretations [101]. The methodology employed in this thesis explicitly recognises the researcher’s interpretative role and uses reflexive and transparent practices to produce contextually grounded insights [110].
Theoretical and Philosophical Background of IPA
IPA integrates the theoretical tenets of phenomenology, hermeneutics, and idiography to explore how individuals make sense of lived experience. Phenomenology, as a philosophical approach, emphasises first-person experience as a way of understanding the essence of a phenomenon. Drawing on Husserl’s descriptive focus and Heidegger’s concept of ‘being-in-the-world’, phenomenology highlights how context, history, and relationships shape perception [101,111-113]. In this study, this lens directs attention to how primary educators experience and interpret inclusion reforms while supporting students with ADHD, considering their unique perspectives, varied experiences and meaning making. Hermeneutics, a theoretical approach to interpretation, is foundational to IPA as it emphasises that understanding is always interpretative. Gadamer’s notion of ‘horizons’ illustrates how a researcher’s own context and preconceptions can shape interpretation, prompting reflexive acknowledgment of the researcher’s role in co-constructing meaning [100,114]. Accordingly, the researcher’s position and context are made explicit in the reflexive statement (Appendix A).
The hermeneutic circle describes the iterative movement between the parts (e.g., individual statements) and the whole (e.g., participants’ broader narratives), allowing each to inform the other and deepen understanding [114,115]. Applied to this study, the hermeneutic circle guided analysis and enabled each transcript to be revisited iteratively and analysed individually before identifying shared patterns across cases [101]. Finally, idiography distinguishes IPA from nomothetic approaches that seek generalisability by prioritising depth over breadth. It involves detailed, case-by-case analysis before progressing to cross-case synthesis, ensuring that individual meaning is preserved [101].
Recruitment
Recruitment took place during April-September 2025 via professional networks and prior school connections. A poster outlining inclusion criteria (special or mainstream primary school teachers experienced with ADHD) was emailed to eligible teachers. It was determined a priori that sample adequacy would be achieved once teachers from all school systems and both mainstream and special settings had been included. This ensured the deliberate capture of both convergent and divergent perspectives. This purposive approach aligned with both IPA’s idiographic commitment and the recommendation of four to ten participants for depth and cross-case analysis [101].
Participants
Self-reported demographics were collected to contextualise teachers’ perspectives (see Table 1). Teaching experience (measured as years in service and the estimated number of students with ADHD taught), socioeconomic status (SES), and professional details (sector and mainstream or special) were considered important details, as these may shape professional understandings of ADHD [116]. The final sample comprised six female, White Australian teachers employed across NSW primary school sectors.
|
Participant (Pseudonym) |
Katie |
Lara |
Sally |
Zoe |
Jenny |
Bec |
|
Teaching Experience (Years) |
18 |
31 |
33 |
9 |
8 |
23 |
|
Number of Students with ADHD Taught ( ≈ n) |
20 |
150 |
70 |
15 |
20 |
100 |
|
*SES |
99th |
96th |
94th |
90th |
95th |
90th |
|
School Sector |
Catholic |
Catholic |
Catholic |
Public |
Public |
Independent |
|
Teaching Role |
Mainstream |
Mainstream |
Special |
Special |
Mainstream |
Mainstream and Special |
|
Note. *SES reported using Australia-wide percentile ranking from the Australian Bureau of Statistics Postal Area Index of Relative Socio-Economic Disadvantage [117]. |
||||||
Table 1: Participant Demographic Summary
Procedure
Ethics approval was obtained from Macquarie University’s Human Research Ethics Committee (#520251261663595), and the study was deemed low risk. Following informed consent and the collection of self-reported demographics, interviews were scheduled around teaching commitments. One-on-one semi-structured interviews were conducted via Zoom video conferencing, chosen for accessibility, flexibility, and suitability for IPA’s conversational style [101]. With participant permission, interviews were video recorded and initially transcribed verbatim using Microsoft Word dictation function. Transcripts were subsequently cleaned, with non-verbal nuances noted to preserve the idiographic quality central to IPA [101].
All transcripts were de-identified using pseudonyms and any identifying details were removed to protect confidentiality [101]. A second coder, covered by ethics approval, signed a confidentiality agreement prior to accessing the audio recordings and transcripts. Member checking was conducted two weeks post-interview by emailing transcripts back to participants, who were invited to review, clarify, or withdraw statements. All participants confirmed accuracy without requesting changes. All recordings, transcripts, and consent forms were stored securely in a password-protected SharePoint folder, with transcripts and consent forms stored separately for confidentiality.
Once transcripts were verified, recordings and correspondences were deleted, and final data were stored securely in the Macquarie University Data Repository in line with institutional requirements. Participants who requested updates were emailed a plain language summary of the study and its findings.
Materials
Semi-Structured Interview
Thirty semi-structured interview questions were developed (see Appendix B). Scaffolded by the PPCT model, the schedule systematically explored multiple layers of the educational ecology [1]. Several items were adapted for either special or mainstream teachers, consistent with IPA’s idiographic commitment [101].
Questions explored teaching experiences, training opportunities, professional identity, structural barriers, policy perceptions, and student management strategies. The schedule was refined in consultation with the research supervisor, a Senior Clinical Neuropsychologist experienced in ADHD. Given the sensitive nature of discussing professional challenges and workplace experiences, participants were reassured of their anonymity and supported through well-being check-ins embedded throughout the interviews. Interviews lasted between 63 and 75 minutes, consistent with Smith et al.’s recommendation of at least 60 minutes to generate rich insights, allow for real-time clarification, and enable iterative probing [101].
Data Analysis
Analysis followed Smith et al.’s six-step process: (i) immersive reading and re-reading transcripts, descriptive and exploratory noting, (ii) identification of experiential statements, (iii) subtheme development, (iv) synthesis into personal experiential themes, (v) idiographic case analysis, (vi) cross-case analysis to derive group experiential themes [100]. This iterative and inductive approach allowed the researcher to stay close to the data while engaging in layered interpretation. The hermeneutic circle facilitated reflexive engagement, allowing individual cases to be revisited and reinterpreted as insights emerged from the broader research context [101].
Methodological Integrity
Methodological integrity in IPA is achieved through transparency, reflexivity, and fidelity to participants’ meaning making [110].
To ensure that the study remained authentic, ethically grounded, and methodologically coherent, Yardley’s principles; sensitivity to context, commitment and rigour, transparency and coherence, and impact and importance, guided the study design and analysis [118]. This is documented throughout the present thesis, in line with qualitative reporting best practice [110].
Validity and Reliability
In qualitative research, validity and reliability are often reframed as trustworthiness, comprising credibility, transferability, dependability, and confirmability [119]. Credibility, or confidence in the findings’ truth, was enhanced through dual coding and consensus discussions with a trained research assistant and the research supervisor, supporting intersubjective agreement on themes [119].
Although not a core IPA requirement, this decision was based on the primary researcher’s positionality to minimise interpretative bias (see Appendix A). Bracketing, via reflexive journalling further reduced interpretative bias, while member checking, which involves inviting participants to verify the researchers’ interpretations, further strengthened credibility [110,111]. Transferability, the extent to which findings can be applied to other settings, was supported through thick description of participants’ contexts, allowing readers to assess relevance to alternate settings. Sample adequacy was confirmed through the inclusion criteria, ensuring both experience quality and contextual diversity [120]. Dependability, the consistency of findings over time, was addressed through a comprehensive audit trail documenting analytic decisions and theme development [119]. Finally, confirmability, or the extent to which findings reflect participants rather than researcher bias, was achieved by grounding all themes in verbatim excerpts [120].
Findings
In line with IPA guidelines, the results and discussion are integrated [100]. The analysis revealed three group experiential themes, each comprising several subthemes (see Figure 2). These themes are illustrated through participant quotations, annotated by transcript page and line numbers. As Noon describes, a dualistic tension exists between the need to identify cross-case patterns and IPA’s idiographic commitment, which risks overgeneralising and obscuring the richness of individual meaning [121]. To overcome this, a conscious effort was made to maintain fidelity to each participant’s unique perspective by delineating and capturing both nuanced individual elements, alongside shared patterns. Although themes are presented separately for clarity, they are closely interrelated and should be understood as forming a connected, overarching picture of teachers’ experiences, reflecting the dynamic interplay of contextual dimensions of the educational ecology as described by the PPCT model [1,101].
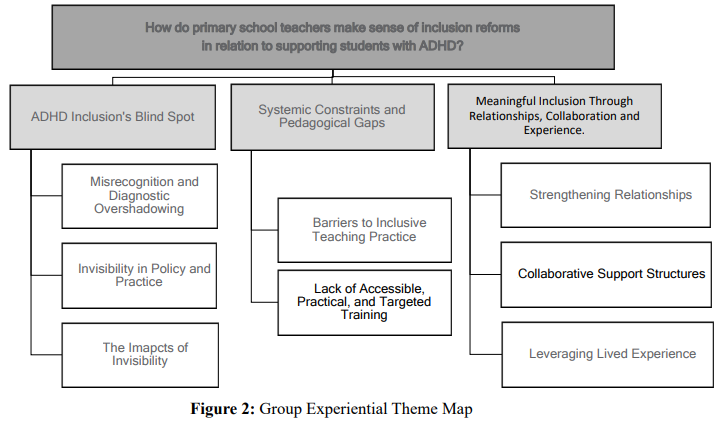
Figure 2: Group Experiential Theme Map
Group Experiential Theme 1: ADHD Inclusion’s Blind Spot
This group experiential theme is captured by three subthemes, described as follows:
Subtheme 1.1: Misrecognition and Diagnostic Overshadowing
Teachers described ADHD as misunderstood in the classroom and overlooked within systemic structures, producing a hierarchy where symptoms were interpreted as misbehaviour and subordinated to coexisting conditions. Zoe, an inclusive classroom teacher, reflected on how a lack of ADHD knowledge can lead teachers to misattribute ADHD symptoms as moral flaws, eliciting authoritarian responses that prioritise compliance over support: “I think when there's a lack of understanding, those kids do get missed or labelled as the ‘naughty’ kid, or it becomes about behaviour rather than their learning needs because they don’t understand what it means to have ADHD in a classroom. So, there's no compassion there. It's just black and white. I'm an authority, you're not following my rules, you're being defiant” (9.219-223). This interpretative pattern reflects well-established links between teacher knowledge and negative stigma towards ADHD [49,122]. Moore et al.’s qualitative study found that teachers with limited ADHD knowledge often attributed classroom difficulties and student behaviours to deficits within the child rather than to contextual factors such as those within the classroom environment [28]. Attribution theory provides explanatory depth: when behaviour is judged as controllable, teachers are more likely to respond with anger and punishment, whereas behaviour understood as less controllable elicits sympathy and support [123,124]. Zoe’s account shows how teacher epistemic positioning regarding ADHD shapes the quality of support that students receive. Sally, a diversity team leader, described the advocacy involved in her role, particularly in reframing ADHD symptoms as disability driven with classroom teachers: “I know there are times it is frustrating having some of these students in your class, but I say to them, we’ve got to think about the disability, the ADHD, the big functional impact that’s driving their behaviour” (7.166-169).
Another form of misrecognition arose in relation to coexisting conditions, with ADHD frequently rendered secondary to other diagnoses. As Zoe explained: “ADHD is often second to if they’re autistic and they've got ADHD, so the comorbidity thing, it’s always second fiddle, whereas it's often the first piece in the puzzle for kids with ADHD" (8.194-196). This illustrates diagnostic overshadowing, a process where one diagnosis masks or deprioritises another set of needs [125-127]. Bec similarly described how support access operated on hierarchical positioning of neurodiversity profiles: “I think it becomes hierarchical on the level of neurodiversity in their profile” (11.277-283). Wilson et al. found similar patterns in their Scottish qualitative study, noting that teachers often viewed ADHD as less deserving of resources than other disabilities, leading to its de-prioritisation in practice [49].
Based on teachers’ accounts, a cycle of misrecognition is apparent. Limited teacher knowledge leads to moral mislabelling and exclusionary practices, while systemic hierarchies and diagnostic overshadowing reduce ADHD’s visibility. In the context of inclusion, such misrecognition complicates reform aspirations, suggesting that without both cultural and structural change, ADHD may continue to remain misunderstood and overlooked.
Subtheme 1.2: Invisibility in Policy and Practice
Teachers described ADHD support as complicated by its invisibility in classroom presentation and policy positioning. Zoe reflected: "ADHD is a really unique one, because it's an invisible one. We have specific classes for autistic children, for children who are intellectually moderate, severe, mild, or with physical disabilities, but we don't have classes for children who ‘just’ have ADHD. The impacts can be enormous on their learning, so I feel like it's the one that's left behind the most, but it can have a huge impact on a kid’s school journey, their self-worth, and their whole life really" (8.188-193). Jenny and Sally described this invisibility as being most acute for inattentive presentations and girls, who were more likely to: “Slip through the cracks” (Jenny, 11.269-273). Sally described how this pattern emerges in classroom dynamics: “The little compliant or the inattentive ADHD student that you forget about because she's just doing the right thing and she's sitting there. And then you realise that the hyperactive ADHD is bouncing off the walls. And then just trying to get to all these kids because the ones that are ‘out there’ are grabbing your attention more, it’s tricky” (8.202-209). These teacher observations mirror research demonstrating that girls with ADHD face barriers to recognition and access to support at school, and are frequently misidentified as shy or unmotivated, delaying diagnosis and intervention [33,34,128]. Gender bias in the ADHD literature remains well documented, with estimates suggesting up to 75% of girls with ADHD remain undiagnosed [129,130]. Such disparities highlight the need for explicit education and health professional training on differential gendered presentations, which may not be captured by DSM-5-TR criteria [21,131].
Teachers also stressed that ADHD’s invisibility is compounded by its policy level omission, particularly its exclusion from the NCCD. As Zoe explained: "You can't get funding for a kid who's got ADHD and nothing else. ADHD really falls under the radar, really gets a bad rap, or doesn’t get the attention it needs because the other ones have specific funding categories” (9.228-230). Lara similarly described how structural omissions place further pressure and responsibility on teachers to bridge these gaps: “I feel very disappointed that there is no support. They actually don't fall under the NCCD, and I think that is appalling, because they have needs that are really beyond what a classroom teacher can do quite often, and there is no financial support for occupational therapy, speech therapy, or any of those things. And having access to cheaper or free educational assessments - I think it's vital. I feel very sorry for children in some areas because they are not diagnosed, or they’re poorly diagnosed. There’s no support in place; therefore, it falls on us teachers who haven't had suficient training in occupational therapy and speech therapy to really hone our skills to support them in the classroom" (14.361-369). Lara further described the resulting implementation gap: “Well, I definitely think that there is a lot of paperwork that goes on, there's a lot of thinking that goes on, but what we'd like to do on paper is not what we can actually do” (15.386-388) reiterating later that: "Because it doesn't attract any NCCD funding, it's sort of forgotten.” (16.415-416).
Concerns were raised about the implications of the Disability Royal Commission’s aspirations for fully inclusive mainstream classrooms. Teachers questioned whether, under current resourcing, such ideals might further marginalise those with less visible needs. Lara expressed concerns for students with ADHD under these circumstances: “I just hope that they don't get lost” (12.301-303). Katie anticipated: “If you get children with higher complex needs or more diverse needs, that support is going to be withdrawn from the current children and given to the higher needs” (11.267-270). She continued to describe the potential for resource triaging, leading teachers to de-prioritise students with ADHD: “I do think their attention will be drawn to children with more complex needs and greater needs, because their adjustments will be more and would be more often. So, I do worry that children with less visible needs might be – not left not left behind – but will instead of being first on the priority list might become second or third” (13.334-339).
When considered alongside the literature, these perspectives align with stigma theory: when disability is invisible or not immediately apparent, needs are more vulnerable to de-prioritisation [132]. Evidence beyond schooling demonstrates that individuals with invisible disabilities face less favourable attitudes than those with visible disabilities [133]. Theoretically, the invisible nature of ADHD provides a compelling explanation for why it is systematically undervalued in support prioritisation and funding. This dynamic echoes Mulholland’s critique of policy-level definitional bias, whereby narrow state definitions exclude ADHD despite its coverage under federal disability law [5]. This mismatch denies students vital support and leads schools to manage ADHD under behaviour policies rather than learning support frameworks, reinforcing the misconception that ADHD is a discipline issue rather than a disability. Such bias systematically disadvantages students with ADHD and underscores the urgent need for policy reform in which ADHD is explicitly acknowledged and resourced.
Subtheme 1.3: The Impacts of Invisibility
Teachers anticipated that a continued lack of recognition and resourcing would initiate and compound existing risks across academic, social, and mental-health domains. The concept of developmental cascades suggests that early challenges, such as academic difficulties, initiate cascading effects across domains of functioning [134]. Katie considered how early gaps may cumulate over time: "If your gaps in learning are getting bigger and bigger, but also if your gaps in your social skills are lagging behind your classmates, it can really impact self-esteem, self-belief, and that negative talk, which is already a trait for a lot of ADHD children -it will just intensify as children get older, reach puberty. I just think it's going to be more detrimental to their health” (10-11.256-265). Longitudinal research supports this trajectory, showing that ADHD symptoms are associated with declines in self-esteem during adolescence, even after controlling for peer difficulties, which are frequently cited in adolescent literature as a key contributor to self-esteem declines [135,136].
Zoe similarly reflected on how systemic neglect compounds over time: “It’s the one that’s left behind the most, but it can have a huge impact on kids’ school journey, their self-worth and their whole life” (8.188-193). She continued to share concerns and to stress the importance of intervention in primary school, identifying risks beyond education which extended into justice system involvement, and substance misuse: “I mean, we all know that kids with ADHD are at much higher risk of getting into trouble with the law or with things like addiction, holding down jobs. So, if they're not supported when they're in school or the dialogue doesn't change around ADHD, and what it means, it has a negative impact on long-term prospects. Anecdotally, I do know that kids with ADHD leave school a lot earlier. As I said, they get lost in the system, especially in high school, where the behaviours that are tolerated in primary school are not tolerated in high school. I think there's more opportunity in primary school for one-on-one support and for giving kids a bit of space and a bit of a break, whereas in high school, there’s just not. So, the impact for kids continuing their high school journey is negative. And if you're constantly getting in trouble for disruptive or restless behaviour, it's really going to impact your ability to learn, your ability to stay at school, your desire to stay at school, and feel like you belong” (10-11.252-266). Bec similarly described concerns as children reached adolescence and stressed the importance of early intervention: “If you’re being missed, that’s going to have a knock-on effect long-term on learning if you’re not able to engage. I think from a social perspective as well, sometimes they've kind of been able to keep up with their peers when they were younger, but as they get older, that's gonna have an impact as they continue into high school. Just thinking about how lots of students with ADHD often have mental health issues when they go through teenage years, so understanding why that's happening, whether it's an eating disorder or self-harm, all these different things. It's going to have a long-term impact if people haven't worked out what's going on and tried to put the supports around the child" (12.297-314). Minority stress theory contextualises teachers’ concerns [137]. Originally developed to explain disproportionate mental health burdens among marginalised groups, it has been applied to include individuals with disabilities, explaining how distal (i.e., policy omissions or resource denial) and proximal stressors (i.e., anticipated rejection or internalised stigma) accumulate to affect mental health and general functioning [138]. Psychophysiological evidence also supports this interpretation: children with ADHD show stress-response dysregulation, including lower basal and morning cortisol consistent with chronic strain associated with anticipating unsupportive environments [139]. In line with the PPCT model, these insights highlight how systemic neglect reverberates through children’s developmental trajectories, having detrimental consequences [1]. This reiterates the need for policy recognition to enable resources and early intervention.
Group Experiential Theme 2: Pedagogical Gaps and Systemic Constraints
This group experiential theme is captured by two subthemes described as follows:
Subtheme 2.1: Barriers to Inclusive Teaching Practice
Teachers described interrelated systemic and relational barriers that constrained their capacity to meet ADHD needs, compounding inequities in support provision. Lara and Jenny linked these barriers to broader systemic shifts towards mainstreaming reforms without commensurate preparation or resourcing. Lara reflected: “[Students have needs] beyond our scope that we’ve never been trained for” (3.59-60), describing how: “The start and finish line keep getting further and further apart” (4.97). Jenny similarly described: “It’s just all this, add, add, add, and there’s no breathing space” (16.420-423). These perspectives align with Australian and international education reviews, noting inclusive education policies often outpace workforce capacity and support structures [140,141].
Class size also emerged as a barrier. Katie argued that: “For some children with their different needs, they just won’t cope in a classroom of say 28 [children] with one teacher” (3.66-68). Zoe contrasted her small specialist setting to mainstream classrooms: “So, with the mainstream classroom, where you’ve got 30 kids in the classroom. If a kid’s acting up, or they’re restless, and they’re unable to focus… then you're not going to have the patience, or the bandwidth, or the resources, to just sit with that child, help them regulate and help them get back on track. So, I've got a lot more patience, because I’ve got flexibility in that I've only got seven kids… so I can have an SLSO [school learning support oficer] work with other children, while I focus my attention on the child with ADHD who's not able to regulate or do their work. I guess I'm privileged in that way, that I do have the resources to do that “(8.203-211). Sally similarly argued:” Reducing our class sizes is probably the biggest thing. And we’re told, it’s not about the class size, it’s about the teaching. And I totally disagree with that” (8.195-196). Despite being a widely researched topic, peer-reviewed evidence on class size effects on teaching quality remains inconclusive [142]. However, ADHD focused studies involving teacher reports consistently identify class size as a barrier to providing students with adequate support [92,143].
Staffing constraints were also salient. Katie reflected on the teacher shortage, concluding that even if funding was increased: “You may still not be able to get the support because [it’s] a real issue” (5.103-106). Sally made sense of the teacher shortage: "If you have a child with complex needs, we've got to jump through hoops just to get support for them. I think that's why we're losing a lot of teachers. We're having trouble attracting them, we’re having trouble keeping them. I really believe that it's because of additional needs and behaviours, which probably a lot of them stem from ADHD…” (13.317-321). Education research supports these perspectives, linking staff shortages to increased teacher stress and attrition [144,145]. Sally described how staff shortages lead to support inequities: “The most vulnerable students are left with the most unqualified, because we’re so short-staffed, especially with the teacher shortage” (10.250-252).
Unrealistic expectations emerged as a major stressor and barrier to students accessing support. Lara described working with families who had high expectations but took no responsibility: “It’s all on us, but they’re not willing to go and seek the help that their child needs. It’s that battle. We can’t solve all the problems”(5.118-122). Lara’s experiences highlight that parent expectations about the level of help or support that teachers should provide, can leave teachers managing complex needs without adequate home-school collaboration. From a job demands and resources perspective, the convergence of large classes, staffing shortages, and unrealistic expectations represents a cluster of high demands that deplete energy and heighten stress and burnout risk [146]. These accounts reveal how barriers extend beyond logistical constraints to directly shape the feasibility of inclusive pedagogy. Within the PPCT model, such contextual forces at the ecosystem and macrosystem levels intersect with teacher practice, impacting the quality of support that students receive [1]. These conditions not only constrain practice, but contribute to Australia’s teacher shortage, accelerating attrition and further challenging recruitment in an under-resourced profession [147].
Subtheme 2.2: Lack of Accessible, Practical, and Targeted Training
Teachers consistently described the need for training that was practical, feasible, and specific to ADHD. Katie emphasised the importance of building diagnostic literacy as a foundation for inclusion: "I think the most prevalent ones that we'll see in a mainstream school are probably ADHD and ASD. So, just starting with what these diagnoses are, how do they get diagnosed? Because a lot of teachers have to fill in forms from the paediatrician or psychologist, so, even background knowledge on what you are doing with these forms or what information you are giving with these forms” (7-8.177-18I). Lara stressed that training must address the heterogeneity of ADHD: "Not all students with ADHD present in the same way. Within families, children with ADHD don't present in the same ways. And that's okay, but it's about meeting the child where they're at" (11.275-279). She critiqued existing professional learning as superficial, advocating for evidence-based approaches: "The band-aid approach, you know, where they send you off for a day. But that doesn’t help. That’s a short-term solution. To understand it, we need more background on it. We need that research base. Looking at research and programmes that have been successful” (14.352-360).
Several teachers called for in-vivo modelling and expert consultation. Katie suggested: “It would be great to have an expert on site, whether it's a psychologist or paediatrician, I’m not sure, but to come and just observe and give schools pointers would be amazing” (7.164-16). Sally, who had taught for 33 years, reflected on the past availability of professional expertise: “Once upon a time we had speech therapists [at school]. That was someone I could go to, to get help or ideas” (6.143-145). Her account reflects policy and practice changes following the COVID-19 pandemic, which reduced or restricted clinician access in schools. These reflections mirror qualitative findings by Ward et al., where teachers identified in-vivo coaching as a preferred form of professional development [93]. A recent meta-analysis demonstrated the benefits of modelling, finding this component of instructional coaching significantly enhanced teacher practice compared to coaching without modelling [148].
Despite the recognised need for training, teachers reported structural barriers to access, echoing findings from Australian inclusive education research [77]. Sally explained: “They’re like 20-hour courses that you do in your own time, and I think for teachers, especially young mums who have kids and are working full-time, that's unattainable. And really, from my perspective, schools have their agendas for professional development and special education or diversity – it’s not high on the priority. It’s frustrating” (6.150-155). Lara described that training is often: “financially out of our reach” (14.358). These insights mirror recent findings in the Australian ADHD literature, where teachers described the need for accessible, brief and flexible training [17].
Concerns also extended to pre-service preparation. Lara believed that: “the level of training for teachers must change” (4.94-95) and worried about “…teachers coming in. The expectation is enormous now” (6.117-118). Katie described similar concerns: “I believe, especially new teachers coming out of university, with the workload and the stressors that are already on teachers. I think [fully inclusive classrooms] could be a tipping point for some teachers" (3.73-75). She reflected her view that: “Inclusive education is a degree on its own, you probably need to bring into the mainstream university courses” (5.107.110). These insights are consistent with international evidence that current teacher education programs are not adequately preparing graduates for the complexity of contemporary classrooms, leaving teachers underprepared to manage diverse needs and implement inclusive pedagogy [35,93].
Katie and Jenny explained that the increasingly diverse nature of their classrooms had led them to contemplate pursuing further teaching qualifications. Katie reported that she was considering: “a masters of inclusive education” (7.154-156), while Jenny was likewise contemplating: “potentially doing some additional university study around it” (12.304-305). While teachers framed upskilling as essential, pursuing further qualifications presents the risk of drawing experienced teachers out of classrooms, intensifying workforce shortages and reducing the availability of skilled teachers to enact inclusion. Collectively, these narratives indicate a misalignment between broader ecological levels and the microsystemic demands of contemporary classrooms (see Figure 1) [1].
Group Experiential Theme 3: Meaningful Inclusion Through Relationships, Collaboration, and Experience
This group experiential theme is captured by three subthemes, described as follows:
Subtheme 3.1: Strengthening Relationships
Teachers stressed that building trusting relationships with students and caregivers was foundational to the inclusion of students with ADHD. Ecological accounts of belonging emphasise that proximal teacher-student relationships are critical to engagement, motivation and wellbeing [1,149,150]. Sally reflected on one child’s experience, demonstrating how teacher understanding can be decisive for relational quality: “We had a little boy - he's in Y2 now - but when he was in Kindy, he could tell that the teacher didn't like him. And I was like, just jump on the good, even say good morning to him, and just say I'm so happy to see you. But he was hard work for her. The teacher loves him this year and he has really settled a lot" (13.339-346). This account aligns with the Pygmalion effect and demonstrates the salience of teacher expectations, capturing how warmer teacher expectations and attuned interactions promote school engagement and achievement, while negative expectations can become self-fulfilling and detrimental to students [139,151].
Katie emphasised the importance of understanding student needs from the outset: "I guess it's about really getting to know that child, whether it's through their reports that are given to the school, or parent meetings. You don't want to leave a child a month without getting to know them” (9.210-212). Katie linked this knowledge as foundational to teacher confidence: “Once you know those children, you know the triggers, you know what the child needs, children with ADHD can really thrive” (12.292-297). Zoe similarly stressed that “Context is everything. Knowing the whole child is important, and ADHD is a big part of the puzzle for some kids” (12.291-293). Supporting this perspective, McDougal et al.’s qualitative study found a misalignment between teachers’ and students’ perceptions of the students’ strengths, highlighting that relational quality is crucial for uncovering what students feel confident about and leveraging those strengths to enhance engagement and learning [152]. Similarly, teachers in Ward et al.’s qualitative study reported that knowing the child was central to pre-empting triggers and intervening proactively [93]. Positive teacher-student relations were described as reducing conflict and promoting cooperative behaviours. Together, these findings illustrate that a strong understanding of students’ needs is foundational to ADHD inclusion and to enhancing children’s educational experiences.
Sally extended these insights by explaining proactive relational strategies, noting the importance of informal, positive interactions: “Connecting with them on the playground. When they’re just on the playground. So that when you have to have that tricky conversation, you’ve already got that good rapport” (9.230-236). Through the PPCT lens, teacher-student relationships are a core developmental driver that can either protect against or exacerbate the risks associated with ADHD [1]. Research supports this, demonstrating that positive teacher-student relationships predict increased engagement, improved self-regulation, and fewer behavioural difficulties in students with ADHD [153,154].
Sally and Jenny described the importance of strong home-school partnerships and being able to communicate openly with caregivers about students’ needs. Sally reflected on the complexity of communicating concerns to parents, especially regarding behavioural challenges linked to ADHD: “When you have to make those calls to parents, especially [about] behaviour problems. You’re still trying to do the right thing, be honest and open with the parent… it’s not an attack” (5.104-110). Jenny spoke to the emotional labour involved when raising concerns with parents about possible learning needs, and how this falls on teachers in the absence of other support systems: “There are experienced teachers who think that parents need to look into understanding their [child’s] needs better, but teachers really struggle with how to vocalise that. Schools sometimes use the school counsellor, but public schools, we get the counsellor for half a day” (388-393). Epstein’s ‘six types of involvement’ framework, describes effective home-school partnerships as reciprocal, trust-based, and solution oriented [155]. Yet teachers’ accounts suggest a need for more structured professional learning to navigate these interactions - training more akin to the therapeutic alliance used in clinical settings, whereby rapport, mutual respect, and goals are co-constructed [156]. Without explicit guidance on building constructive teacher-student relationships and teacher-caregiver partnerships, communication risks becoming strained and further exacerbating pressures on teachers.
Subtheme 3.2: Collaborative Support Structures
Teachers described the importance of collaboration on many fronts, particularly within the school environment. Zoe believed: “From the top down, people [must be] aware. So, if they see [a child] in the playground having a meltdown, they’re identified as needing extra support” (12-13.316-332). Zoe stressed that support must extend to unstructured social contexts, which present additional challenges without staff awareness: “You can almost contain it within the classroom to the best of your ability, but then the social aspect throws another thing out there. So, having a whole school approach to support them" (12-13.316-332). Meta-analytical evidence demonstrates that whole-school programs can meaningfully improve student social, emotional, and behavioural outcomes, especially when supported by community engagement. While recent Australian teacher studies have similarly called for school-wide collaboration [17,76,157].
Teachers also highlighted the importance of collaborating with students in decisions about their support and learning: Bec explained: “We’ve been trialling having their voice more in it” (13.32-325). Zoe similarly described: “It might be that they’re a visual learner, or it might be through music…so finding another pathway around what you’re trying to get them to do. Having them have a say in what that is and what that looks like " (12.310-315). The benefits of student involvement can be understood through self-determination theory, which identifies autonomy, competence, and relatedness as key psychological needs that enhance motivation and engagement [158]. Student-led individualised education plans have been shown to improve goal-setting skills, increase the personal relevance of accommodations, and lead to greater adherence to mutually agreed supports [159]. In the broader inclusive education literature, student voice is seen as a mechanism for enhancing school belonging and cultural responsiveness, ensuring that interventions are not only tailored to student needs but are also co-constructed with the learner’s identity and lived experience [160-162].
Beyond school-wide and student collaboration, Jenny articulated the disconnect between health and education sectors, calling for greater interdisciplinary collaboration: “I feel like there is also a disconnect between the health system and the education system” (9.222-223). She argued for: “More integrated allied health in schools. Parents really struggle with access, teachers don’t know where to send them” (16.403-407). Lara similarly called for more practical and considered recommendations from clinicians: “I really cringe at some of their recommendations. It’s just an easy way to slam out a report, and it really isn’t meeting needs” (15.378-382). Katie also spoke to this: “It’s very common to get a report from a psychologist or a paediatrician with lots of recommendations for the school. But it's not evident in those reports that they've considered the rest of the class, or they've considered the environment, or they've considered the timetable at the school. So, the sustainability of these adjustments I don't think gets considered in a holistic school environment” (8.193-199). Recent Australian research by Gibbs and Le reported that three quarters of the studies’ Australian teachers (N = 1,024) desired more opportunities to engage in interdisciplinary collaboration with allied health, community organisations and parents [17]. Moreover, broader evidence supports that interdisciplinary collaboration, particularly involving psychologists, speech therapists, and occupational therapists, enhances teacher efficacy and student outcomes when embedded in the school environment [163,164]. Evidently, collaboration on various fronts of the educational ecology is essential for cohesive and responsive support for students.
Subtheme 3.3: Leveraging Lived Experience
Lara, Zoe, and Bec drew on their lived experience as a parent of children with ADHD, as family members, or through their own learning difficulties, highlighting lived experience as a powerful asset for inclusive practice. In a qualitative South African study exploring ADHD inclusion, Braude and Dwarika found that teachers with personal experiences of ADHD engaged in more supportive and informed pedagogy [92]. Lara, Zoe, and Bec similarly described that such experiences enhanced their ability to identify ADHD, interpret behaviour, adapt teaching strategies, and work effectively with families. Lara reflected on how her own academic struggles in primary school shaped both her motivation to teach and her empathy for students: "I really struggled in primary school. I didn't find it easy. I was probably an undiagnosed child of some things…So, I’m able to come into the classroom understanding how kids feel in that world” (1.6-10). Lara explained: “A lot of it is based on experience and observation, and the ability to look past the surface level. Not all teachers are able to do that. It's usually linked to the experience they've had or life. Your own personal life experience" (17.427-429). Zoe reflected on parenting a child with complex needs: “I just think having a bit of life experience under your belt, having a family of my own, and with complex needs has really helped me in the classroom" (1.19-22). Bec felt that having ADHD in her family enhanced her patience in the classroom: “I understand, and I get the level of need they require, and the patience because I live it every day” (13-14.342-344). She explained that her dual role as a parent and teacher deepened her teaching practice: “Because I do have two children with [ADHD] as their profile, I put on both hats as being a mother and a teacher” (14.346-347). Zoe described how lived experience held value at the policy level, urging policy makers to engage with classroom realities: "Talk to teachers in support units and inclusive classes that have real lived experience. See what it's like on the ground" (7.178-184).
Lived experience offers a form of experiential expertise that can bridge the gap between policy ideals, classroom realities, and the needs of students. Isenor et al. found that ADHD training workshops led by a presenter with ADHD were most effective in shifting 75 pre-service teachers’ attitudes, reducing deficit-based views and fostering empathy [165]. Personal narratives prompted reflection on classroom strategies and helped teachers empathise and understand the heterogeneity of ADHD. Framed through relational pedagogy, these findings suggest that care, trust, and understanding are foundational to effective teaching, with lived experience offering an insider perspective that deepens empathy though contextual insight [166]. Embedding lived experience within teacher education and professional development may strengthen inclusive practice, particularly for supporting frequently misunderstood disabilities such as ADHD.
Thesis Strengths and Limitations
This is the first Australian study to qualitatively explore primary teacher perspectives on ADHD, thus, contributing novel insights at a critical juncture of inclusive educational reform, and being a key strength of the study. Applying a multi-systemic lens enriched the interpretative process and illuminated how teachers negotiate policy obligations in practice for students with ADHD. Analytic rigour was also a strength, achieved through dual-coding, consensus discussions, and reflexive engagement, enhancing both credibility and fidelity to participants’ voices, consistent with qualitative best practice [110].
Another strength was the high level of expertise: teachers averaged 20 years of professional experience. Also, three teachers brought lived experience of complex needs, or ADHD, offering valuable insider perspectives [167]. While some research has questioned whether longer tenure reliably equates to higher teaching quality, the longevity of teachers’ careers provides distinct advantages in revealing aspects of the influence of the ‘time’ component of the PPCT model (see Figure 1) [168]. Long-service teachers have lived through successive reforms in curriculum, assessment and policy, as well as shifting discourses surrounding inclusion, neurodiversity, and ADHD. Their experience affords a capacity to contextualise current challenges against prior systemic shifts, providing nuanced insights into how recognition of neurodivergent learners and the teacher workforce has evolved and adapted to change over decades. Additionally, the inclusion of mainstream and special teachers from diverse educational sectors facilitated convergent and divergent perspectives; an important consideration given the sectoral differences in funding, inclusion policies and pedagogies.
Despite these strengths, several study limitations must be acknowledged. Firstly, the small sample, while appropriate for IPA’s idiographic focus, may have constrained diversity, particularly regarding socioeconomic, cultural and gender representation [169]. All teachers were White Australian, from higher-SES areas (see Table 1), where resources, education, and attitudes towards ADHD may differ from those in lower-SES, rural, or more culturally diverse communities [169]. This may have limited the generalisability of findings to contexts where structural disadvantage or resource scarcity may create additional barriers. Furthermore, all participating teachers were female. While this reflects the broader Australian workforce, where 82% of primary school teachers are women, the absence of male (and other gender) perspectives on ADHD inclusion represents a notable omission, particularly given the recent rise in non-female enrolments [170]. Importantly, the voluntary nature of participation introduces the potential for self-selection bias, which may have attracted teachers who were motivated to share frustrations, advocate for reform, or reflect on job tensions, a tendency documented in qualitative research [171]. Finally, although the study explored teachers’ experiences in depth, findings are interpretative and situated within a specific context [101]. Caution should be exercised in generalising to other school settings, without considering differences in state policy, resourcing, or school demographics.
Future Directions and Implications
This thesis offers timely insights into how ADHD inclusion is navigated in Australian primary schools and identifies several actionable implications. Mainstream teachers reported feeling underprepared to support students with ADHD, signalling the need for professional learning that is both evidence-based, and manageable within current workforce constraints. Integrating ADHD-specific content into existing structures (i.e., collaborative planning sessions, staff meetings) could strengthen teacher capacity without increasing burden. Three teachers drew on personal or family experience of ADHD or complex needs, demonstrating how lived experience can enhance practice. Schools may benefit from involving willing staff with such expertise in informal mentoring or professional dialogue. Despite valuing collaboration, teachers described working in isolation and expressed a desire for consistent, whole-school practices. Their accounts suggest that coordinated internal processes could reduce fragmented support and teacher stress. Immediate steps may include allocating time for collaborative planning and clarifying internal referral pathways. Telehealth models could assist schools in re-establishing relationships with allied health professionals where access has been restricted following COVID-19 policy shifts.
At the policy level, the findings highlight the need for explicit ADHD-recognition within funding and accountability frameworks, particularly the NCCD. Teachers described ADHD as “invisible” in current models, leaving students without coexisting diagnoses at disadvantage, and increasing pressure on staff. Several linked these omissions to workforce strain, noting that unmanageable behavioural challenges may contribute to attrition. Embedding ADHD-specific provisions within the NCCD would promote equitable access to support, align reforms with student needs, and reduce strain on the teaching workforce. Professional learning reform also emerged as a priority, with teachers calling for preservice and ongoing training that is practical, evidence-based, and workload sensitive. Such training could improve teacher preparedness, reduce stigma, and reframe ADHD from a deficit-based to a strengths-oriented perspective. Involving individuals with lived experience in the co-design of policy and training may further enhance the relevance and impact of reforms. Teachers expressed concern that the Disability Royal Commission’s vision for fully inclusive schooling may unintentionally marginalise students with less visible needs if resourcing does not increase. They stressed that schools must be resourced with adequate staffing, funding, and clinical integration to prevent additional burden falling onto teachers Importantly, recent Australian qualitative studies involving adolescents with ADHD, similarly called for ADHD-specific teacher training, and stronger home-school collaboration [97,98]. This alignment strengthens the credibility of the present study, indicating systemic issues rather than isolated teacher views. Together, the findings demonstrate that meaningful ADHD inclusion requires both structural reform and context-sensitive practice, rather than relying on individual teacher effort.
Future research can extend on this study in several ways. Larger, more representative samples would capture variation across cultural, socioeconomic, regional, and educational contexts. Delphi consensus methodologies could assist in developing actionable, contextually relevant frameworks by integrating diverse stakeholder priorities where empirical evidence remains emergent [172,173]. Inclusive consensus-building can also dismantle ableist research practices by incorporating the expertise of families, health professionals, teachers, and importantly, neurodivergent individuals. Finally, further inquiry into early childhood, high school, and tertiary settings is warranted, where distinct developmental and social dynamics shape experiences [174]. Such work is essential to tailoring training, policy and resourcing across the educational lifespan.
Conclusion
This study is the first to explore how Australian primary teachers interpret and navigate ADHD inclusion. Using the PPCT model and a critical realist stance, the IPA illuminated the systemic, relational, and personal challenges when navigating the inclusion of students with ADHD, addressing the first study aim of clarifying how current inclusion policy is experienced in classroom practice [1]. Teachers described three key experiential domains: the persistent risk of exclusion and its developmental consequences, limited preparedness and professional learning, and the systemic and pedagogical adaptations required for meaningful inclusion. In line with the second study aim, findings identified supports that enable teachers to move beyond individual responsibility and enact sustainable inclusion. These include targeted and accessible training, adequate resourcing, interdisciplinary and school-wide collaboration, and the explicit recognition of ADHD in funding and accountability structures. While multiple ecological processes shape inclusion, responsibility has rested disproportionately on teachers. As this study demonstrates, meaningful change requires recognition and accountability across all systemic levels [1,175-179].
References
- Bronfenbrenner, U., & Morris, P. A. (2006). The bioecological model of human development. In R. M. Lerner & W. Damon (Eds.), Handbook of child psychology: Theoretical models of human development (6th ed., pp. 793–828). John Wiley & Sons.
- Australian ADHD Professionals Association. (2025). Talking about ADHD.
- United Nations. (2006). United Nations Convention on the Rights of Persons with Disabilities.
- Australian Government Department of Education. (2005).Disability Standards for Education. Australian Government.
- Mulholland, S. M. (2017). ADHD: The untold truths of the ADEP (Australian Deficit in Educational Policy). International Journal of Disability, Development and Education, 64(1), 1-18.
- Australian Institute of Health and Welfare. (2022). Australian Institute of Health and Welfare.
- Australian Government Department of Education (2022). Nationally consistent collection of data for school students with disability.
- French, B., Nalbant, G., Wright, H., Sayal, K., Daley, D., Groom, M. J., ... & Hall, C. L. (2024). The impacts associated with having ADHD: an umbrella review. Frontiers in psychiatry, 15, 1343314.
- Yegencik, B., Bell, B. T., & Deniz, E. (2025). School-based randomized controlled trials for ADHD and accompanying impairments: a systematic review and meta-analysis. Frontiers in Psychology, 16, 1611145.
- Halperin, J. M., Bédard, A. C. V., & Curchack-Lichtin,J. T. (2012). Preventive interventions for ADHD: a neurodevelopmental perspective. Neurotherapeutics, 9(3), 531-541.
- Commonwealth of Australia. (2023). Final report. Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability. Our Public Hearings [Transcripts].
- Vygotsky, L. S. (1978). Mind in society: The development of higher psychological processes (Vol. 86). Harvard university press.
- Ford, D. H., & Lerner, R. M. (1992). Developmental Systems Theory. SAGE Publications, Incorporated.
- Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design (Vol. 352). Harvard university press.
- Tong, P., & An, I. S. (2024). Review of studies applying Bronfenbrenner's bioecological theory in international and intercultural education research. Frontiers in psychology, 14, 1233925.
- Efron, D. (2017). The role of schools in the diagnosis of ADHD. The Lancet Psychiatry, 4(11), 825-826.
- Gibbs, K., & Le, L. (2025). Australian teacher’s perceptions about teaching students with attention deficit hyperactivity disorder (ADHD). Emotional and Behavioural Dificulties, 1-11.
- Butcher, L., & Lane, S. (2025). Neurodivergent (Autism and ADHD) student experiences of access and inclusion in higher education: an ecological systems theory perspective. Higher Education, 90(1), 243-263.
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR).
- Sainsbury, W. J., Carrasco, K., Whitehouse, A. J., McNeil, L., & Waddington, H. (2023). Age of diagnosis for co-occurring autism and attention deficit hyperactivity disorder during childhood and adolescence: A systematic review. Review Journal of Autism and Developmental Disorders, 10(3), 563-575.
- Musullulu, H. (2025). Evaluating attention deficit and hyperactivity disorder (ADHD): a review of current methods and issues. Frontiers in psychology, 16, 1466088.
- Shore, C., Posey, S. M., Berkower, C., Ontjes, N., & Babik, K.R. (2024). The Impact of Misdiagnosis, Bias, and Stigma. Adult attention-deficit/hyperactivity disorder: Diagnosis, treatment, and implications for drug development: Proceedings of a workshop (pp. 21–36) National Academies Press.
- Prosser, B. J. (2008). Beyond ADHD: A consideration of attention deficit hyperactivity disorder and pedagogy in Australian schools. International Journal of Inclusive Education, 12(1), 81-97.
- Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychological bulletin, 121(1), 65-94.
- Barkley, R. A. (2012). Executive functions: What they are, how they work, and why they evolved. Guilford Press.
- Ewe, L. P. (2019). ADHD symptoms and the teacher–student relationship: A systematic literature review. Emotional and behavioural dificulties, 24(2), 136-155.
- Staff, A. I., Oosterlaan, J., Van der Oord, S., van den Hoofdakker, B. J., & Luman, M. (2023). The relation between classroom setting and ADHD behavior in children with ADHD compared to typically developing peers. Journal of Attention Disorders, 27(9), 939-950.
- Moore, D. A., Russell, A. E., Arnell, S., & Ford, T. J. (2017). Educators' experiences of managing students with ADHD: a qualitative study. Child: care, health and development, 43(4), 489-498.
- Gwernan-Jones, R., Moore, D. A., Cooper, P., Russell, A. E., Richardson, M., Rogers, M., ... & Garside, R. (2016). A systematic review and synthesis of qualitative research: The influence of school context on symptoms of attention deficit hyperactivity disorder. Emotional and Behavioural Dificulties, 21(1), 83-100.
- ADHD Australia. (2023). Understanding ADHD: Breaking down barriers to ADHD communities thriving (May 2023).
- Kos, J. M., Richdale, A. L., & Hay, D. A. (2006). Children with attention deficit hyperactivity disorder and their teachers: A review of the literature. International Journal of Disability, Development and Education, 53(2), 147-160.
- Luo, Y., Weibman, D., Halperin, J. M., & Li, X. (2019). A review of heterogeneity in attention deficit/hyperactivity disorder (ADHD). Frontiers in human neuroscience, 13, 42.
- Milner, V. L., Mohamed, L., & Happé, F. (2025). ‘Beyond the Stereotype’: Neurodivergent Students’ Experience and Peer and Teacher Understanding of Neurodiversity in a Mainstream Girls’ School. Neurodiversity, 3, 27546330251326056.
- Young, S., Adamo, N., Ásgeirsdóttir, B. B., Branney, P.,Beckett, M., Colley, W., ... & Woodhouse, E. (2020). Femaleswith ADHD: An expert consensus statement taking a lifespan approach providing guidance for the identification and treatment of attention-deficit/hyperactivity disorder in girls and women. BMC psychiatry, 20(1), 404.
- Lynch, A., & Davison, K. (2024). Tensions and contradictions: Exploring postâ?ÂÂprimary teachers' perspectives and experiences of students with Attention Deficit Hyperactivity Disorder. Journal of Research in Special Educational Needs, 24(3), 519-529.
- Metzger, A. N., & Hamilton, L. T. (2021). The stigma of ADHD: Teacher ratings of labeled students. Sociological perspectives, 64(2), 258-279.
- Diener, T. S. L., Jackson, M., Lee, M. A., Grové, C., & Nguyen,V. (2025). Cross-cultural disparities in teachers’ reports of ADHD symptoms and behavior: a scoping review. Social Psychology of Education, 28(1), 1-47.
- Lawrence, K., Estrada, R. D., & McCormick, J. (2017). Teachers' experiences with and perceptions of students with attention deficit/hyperactivity disorder. Journal of pediatric nursing, 36, 141-148.
- McClemont, A. J., Fredrick, S. S., Heidelburg, K., & Moore,C. (2025). Racial disparities in teacher ratings of ADHD symptoms and behavior: A systematic review. School Psychology Review, 54(3), 328-342.
- Degroote, E., Brault, M. C., & Van Houtte, M. (2024). Suspicion of ADHD by teachers in relation to their perception of students’ cognitive capacities: do cognitively strong students escape verdict?. International Journal of Inclusive Education, 28(9), 1740-1754.
- Asherson, P., Buitelaar, J., Faraone, S. V., & Rohde, L. A. (2016). Adult attention-deficit hyperactivity disorder: key conceptual issues. The Lancet Psychiatry, 3(6), 568-578.
- Jensen, C. M., & Steinhausen, H. C. (2015). Comorbid mental disorders in children and adolescents with attention-deficit/ hyperactivity disorder in a large nationwide study. ADHD Attention Deficit and Hyperactivity Disorders, 7(1), 27-38.
- Ginapp, C. M., Greenberg, N. R., MacDonald-Gagnon, G., Angarita, G. A., Bold, K. W., & Potenza, M. N. (2023). “Dysregulated not deficit”: A qualitative study on symptomatology of ADHD in young adults. PloS one, 18(10), e0292721.
- Gnanavel, S., Sharma, P., Kaushal, P., & Hussain, S. (2019). Attention deficit hyperactivity disorder and comorbidity: A review of literature. World journal of clinical cases, 7(17), 2420.
- Claussen, A. H., Holbrook, J. R., Hutchins, H. J., Robinson,L. R., Bloomfield, J., Meng, L., ... & Kaminski, J. W. (2024). All in the family? A systematic review and meta-analysis of parenting and family environment as risk factors for attention-deficit/hyperactivity disorder (ADHD) in children. Prevention Science, 25(Suppl 2), 249-271.
- De Block, A., Dewitte, S., & Hens, K. (2023). Causes or Cures: What makes us think of attention issues as disorders?. New Ideas in Psychology, 69, 101008.
- Harwood, V., Jones, S., Bonney, A., & McMahon, S. (2017).Heroic struggles, criminals and scientific breakthroughs:ADHD and the medicalization of child behaviour in Australian newsprint media 1999–2009. International Journal of Qualitative Studies on Health and Well-being, 12(sup1), 1298262.
- Honkasilta, J., & Koutsoklenis, A. (2022). The (un) real existence of ADHD—Criteria, functions, and forms of the diagnostic entity. Frontiers in sociology, 7, 814763.
- Wilson, C., Green, C. N., Toye, M. K., & Ballantyne,C. (2024). Teachers’ perceptions and practices towards inclusive education for children with ADHD in Scotland: A qualitative investigation. International Journal of Disability, Development and Education, 71(7), 1061-1075.
- Loe, I. M., & Feldman, H. M. (2007). Academic and educational outcomes of children with ADHD. Journal of pediatric psychology, 32(6), 643-654.
- Gardner, D. M., & Gerdes, A. C. (2015). A review of peer relationships and friendships in youth with ADHD. Journal of attention disorders, 19(10), 844-855.
- binti Marsus, N., Huey, L. S., Saffari, N., & Motevalli, S. (2022). Peer relationship difficulties among children with ADHD: a systematic review. International Journal of Academic Research in Business and Social Sciences, 12(6), 1265-1276.
- Neprily, K. M., Climie, E. A., McCrimmon, A., & Makarenko,E. (2025). Why can't we be friends? A narrative review of the challenges of making and keeping friends for children and adolescents with Attention-Deficit/Hyperactivity Disorder. Frontiers in Developmental Psychology, 2, 1390791.
- Jong, A., Odoi, C. M., Lau, J., & J. Hollocks, M. (2024). Loneliness in young people with ADHD: A systematic review and meta-analysis. Journal of attention disorders, 28(7), 1063-1081.
- Wang, X., & Cheng, Z. (2020). Cross-sectional studies: strengths, weaknesses, and recommendations. Chest, 158(1), S65-S71.
- von Bertalanffy, L. (1977). General system theory: Foundations, development, applications. Leonardo, 10(3), 248.
- Carter, L., Speyer, L., Caye, A., Rohde, L., & Murray, A. L. (2025). Late adolescent outcomes of different developmental trajectories of ADHD symptoms in a large longitudinal study. European child & adolescent psychiatry, 34(2), 709-719.
- Eme, R. (2017). A review of the most recent longitudinal studies of ADHD. Journal of Memory Disorders and Rehabilitation, 2(1), 1004.
- Sciberras, E., Roos, L. E., & Efron, D. (2009). Review of prospective longitudinal studies of children with ADHD: Mental health, educational, and social outcomes. Current Attention Disorders Reports, 1(4), 171-177.
- Harpin, V., Mazzone, L., Raynaud, J. P., Kahle, J., & Hodgkins,P. (2016). Long-term outcomes of ADHD: a systematic review of self-esteem and social function. Journal of attention disorders, 20(4), 295-305.
- Fletcher, J., & Wolfe, B. (2009). Long-term consequences of childhood ADHD on criminal activities. The journal of mental health policy and economics, 12(3), 119.
- Shaw, M., Hodgkins, P., Caci, H., Young, S., Kahle, J., Woods,G., & Arnold, L. E. (2012). A systematic review and analysis of long-term outcomes in attention deficit hyperactivity disorder: effects of treatment and non-treatment. BMC medicine, 10(1), 99.
- Caruana, E. J., Roman, M., Hernández-Sánchez, J., & Solli, P. (2015). Longitudinal studies. Journal of thoracic disease, 7(11), E537.
- Anstey, K. J., & Hofer, S. M. (2004). Longitudinal designs, methods and analysis in psychiatric research. Australian & New Zealand Journal of Psychiatry, 38(3), 93-104.
- Sciberras, E., Streatfeild, J., Ceccato, T., Pezzullo, L., Scott,J. G., Middeldorp, C. M., ... & Coghill, D. (2022). Social and economic costs of attention-deficit/hyperactivity disorder across the lifespan. Journal of attention disorders, 26(1), 72-87.
- Commonwealth of Australia. (2023). Executive summary of ADHD Senate inquiry.
- Zendarski, N., Guo, S., Sciberras, E., Efron, D., Quach, J., Winter, L., ... & Coghill, D. (2022). Examining the educational gap for children with ADHD and subthreshold ADHD. Journal of attention disorders, 26(2), 282-295.
- O'Connor, M., Chong, S., Quach, J., & Goldfeld, S. (2020). Learning outcomes of children with teacherâ?ÂÂidentified emerging health and developmental needs. Child: Care, Health and Development, 46(2), 223-231.
- Cuervo, H., & Vera-Toscano, E. (2025). Teacher retention and attrition: Understanding why teachers leave and their post-teaching pathways in Australia. Asia Pacific Journal of Education, 1-18.
- Armstrong, D. (2025). Anatomy of policy failure? Implications of the Australian Disability Royal Commission Inquiry for inclusive education. Journal of Education Policy, 1-21.
- Iacono, T. (2024). A critique of the Disability Royal Commission’s approach and recommendations for educational inclusion in schools. Research and Practice in Intellectual and Developmental Disabilities, 11(2), 160-175.
- Bigby, C., & Hough, A. (2024). “Old problems and old solutions”: snapshots of the Disability Royal Commission and people with intellectual disabilities. Research and Practice in Intellectual and Developmental Disabilities, 11(2), 145-159.
- Collings, S., Spencer, M., & Mills, R. (2024).Alost opportunity: did the Disability Royal Commission let down parents with intellectual disabilities and their children?. Research and Practice in Intellectual and Developmental Disabilities, 11(2), 211-224.
- Auhl, G., & Bain, A. (2025). Do pre-service teachers build capacity for inclusive classroom teaching during their teacher education program?. International Journal of Disability, Development and Education, 72(8), 1423-1438.
- Latouche, A. P., & Gascoigne, M. (2019). In-service training for increasing teachers’ ADHD knowledge and self-efficacy. Journal of attention disorders, 23(3), 270-281.
- Porter, M., Briscoe, L., Blackwell, H., Sach, L., Tsoumbris,S., Hoang, A., & Cheng, S. (2024). The impact of a blended learning course in ADHD on teacher knowledge and self-efficacy, and improved teaching practices: some preliminary findings. Journal of Psychological and Educational Research, 6(1), 1-41.
- Fox, R. A., Sharma, U., Leif, E. S., Stocker, K. L., & Moore, D.W. (2021). ‘Not enough time’: Identifying Victorian teachers’ perceptions of the facilitators and barriers to supporting improved student behaviour. Australasian Journal of Special and Inclusive Education, 45(2), 205-220.
- Bowlby, J. (1969). Attachment and loss: Attachment. New York: Basic Books.
- Fabris, M. A., Roorda, D., & Longobardi, C. (2022, October). Student-teacher relationship quality research: Past, present and future. In Frontiers in education (Vol. 7, p. 1049115). Frontiers Media SA.
- MacLean, J., Krause, A., & Rogers, M. A. (2023). The student-teacher relationship and ADHD symptomatology: A meta-analysis. Journal of school psychology, 99, 101217.
- Herman, K. C., Hickmon-Rosa, J. E., & Reinke, W. M. (2018). Empirically derived profiles of teacher stress, burnout, self-efficacy, and coping and associated student outcomes. Journal of positive behavior interventions, 20(2), 90-100.
- Herman, K. C., Reinke, W. M., & Eddy, C. L. (2020). Advances in understanding and intervening in teacher stress and coping: The Coping-Competence-Context Theory. Journal of school psychology, 78, 69-74.
- Aloe, A. M., Amo, L. C., & Shanahan, M. E. (2014). Classroom management self-efficacy and burnout: A multivariate meta-analysis. Educational psychology review, 26(1), 101-126.
- Bandura, A. (1977). Self-efficacy: toward a unifying theory of behavioral change. Psychological review, 84(2), 191.
- Collie, R. J., Shapka, J. D., & Perry, N. E. (2012). School climate and social–emotional learning: Predicting teacher stress, job satisfaction, and teaching efficacy. Journal of educational psychology, 104(4), 1189.
- Peterson, J. M., & Jensen, M. T. (2025, May). Teacher self-efficacy in relation to cultural and linguistic diversity in K–12 settings: A systematic review. In Frontiers in Education (Vol. 10, p. 1531481). Frontiers Media SA.
- Morris, S. H., Nahmias, A., Nissley-Tsiopinis, J., Orapallo, A., Power, T. J., & Mautone, J. A. (2019). Research to practice: implementation of family school success for parents of children with ADHD. Cognitive and Behavioral Practice, 26(3), 535-546.
- Carrâ?ÂÂFanning, K. (2024). Meaningâ?ÂÂmaking within inclusion: Exploring parents, teachers and students lay theories of ADHD and their implications for inclusive practice. Journal of Research in Special Educational Needs, 24(1), 133-144.
- Tenny, S., Brannan, J., & Brannan, G. (2022). Qualitative Study. National Library of Medicine; StatPearls Publishing.
- Lawson, G. M., Owens, J. S., Mandell, D. S., Tavlin, S., Rufe, S., So, A., & Power, T. J. (2022). Barriers and facilitators to teachers’ use of behavioral classroom interventions. School mental health, 14(4), 844-862.
- Tavlin, S., Ariol, M., & Lawson, G. M. (2025). Strengthening relationships with students with ADHD symptomology: A qualitative study about teacher perspectives. Teaching and teacher education, 153, 104820.
- Braude, S., & Dwarika, V. (2020). Teachers' experiences of supporting learners with attention-deficit hyperactivity disorder: Lessons for professional development of teachers. South African Journal of Childhood Education, 10(1), 1-10.
- Ward, R. J., Kovshoff, H., & Kreppner, J. (2021). School staff perspectives on ADHD and training: Understanding the needs and views of UK primary staff. Emotional and behavioural dificulties, 26(3), 306-321.
- Aldabbagh, R., Daley, D., Sayal, K., & Glazebrook, C. (2024). Exploring the unmet needs of teachers of young children with ADHD symptoms: A qualitative study. Children, 11(9), 1053.
- Henrich, J., Heine, S. J., & Norenzayan, A. (2010). The weirdest people in the world?. Behavioral and brain sciences, 33(2-3), 61-83.
- Ghosh, M., Fisher, C., Preen, D. B., & Holman, C. D. A. J. (2016). “It has to be fixed”: a qualitative inquiry into perceived ADHD behaviour among affected individuals and parents in Western Australia. BMC Health Services Research, 16(1), 141.
- Sach, L. M., & Porter, M. A. (2025). That’s not what ADHD is”: Australian Schooling Experiences of Female Students with ADHD: An Interpretative Phenomenological Analysis. J Edu Psyc Res, 7(2), 01-20.
- Starkey, J., & Porter, M. (2025). Beyond labels: Students’ perspectives of ADHD in schools. Global Journal of Intellectual & Developmental Disabilities, 14(3), 1-14.
- Gibbs, K. (2023). Australian teachers and school leaders’ use of differentiated learning experiences as responsive teaching for students with ADHD. Emotional and Behavioural Dificulties, 28(1), 18-31.
- Smith, J. A., Flowers, P., & Larkin, M. (2009). Interpretative phenomenological analysis: Theory, method and research. SAGE.
- Smith, J. A., Flowers, P., & Larkin, M. (2022). Interpretative phenomenological analysis. SAGE.
- Denzin, N. K., & Lincoln, Y. S. (2011). The SAGE handbook of qualitative research (4th ed.). Sage Publications.
- Giorgi, A. (2012). The descriptive phenomenological psychological method. Journal of Phenomenological Psychology, 43(1), 3-12.
- Braun, V., & Clarke, V. (2013). Successful qualitativeresearch: A practical guide for beginners. Sage.
- Crotty, M. (1998). The foundations of social research: Meaning and perspective in the research process. London: SAGE Publications Inc.
- Bhaskar, R. (1976). A realist theory of science. Philosophy and Phenomenological Research, 37(2), 282.
- Fletcher, A. J. (2017). Applying critical realism in qualitative research: methodology meets method. International journal of social research methodology, 20(2), 181-194.
- Grace, J. D., & Priest, H. (2015). Ontology to outcome: a critical analysis of psychology research. The Journal of Critical Psychology, Counselling and Psychotherapy, 15(4), 204-213.
- Danermark, B., Ekström, M., & Karlsson, J. Ch. (2019).Explaining society. Routledge.
- Levitt, H. M., Bamberg, M., Creswell, J. W., Frost, D. M., Josselson, R., & Suárez-Orozco, C. (2018). Journal article reporting standards for qualitative primary, qualitative meta-analytic, and mixed methods research in psychology: The APA Publications and Communications Board task force report. American Psychologist, 73(1), 26.
- Husserl, E. (1980). Phenomenology and the foundations of the sciences: Third book, ideas pertaining to a pure phenomenology and to a phenomenological philosophy. M. Nijhoff Publishers.
- Heidegger, M. (1962/1927). Being and Time (J. Macquarrie & E. Robinson, Trans.). Blackwell.
- Finlay, L. (2011). Phenomenology for therapists: Researching the lived world. Wiley- Blackwell.
- Gadamer, H.G. (1976). Philosophical hermeneutics (Vol. 88). University of California Press.
- Montague, J., Phillips, E., Holland, F., & Archer, S. (2020). Expanding hermeneutic horizons: Working as multiple researchers and with multiple participants. Research Methods in Medicine & Health Sciences, 1(1), 25-30.
- Doyle, L., Easterbrook, M. J., & Harris, P. R. (2023). Roles of socioeconomic status, ethnicity and teacher beliefs in academic grading. British Journal of Educational Psychology, 93(1), 91-112.
- Australian Bureau of Statistics. (2021). Socio-economic indexes for areas (SEIFA).
- Yardley, L. (2017). Demonstrating the validity of qualitative research. The journal of positive psychology, 12(3), 295-296.
- Guba, E. G., & Lincoln, Y. S. (1994). Competing paradigms in qualitative research. Handbook of qualitative research. (pp. 105-117). Sage Publications, Inc.
- Korstjens, I., & Moser, A. (2018). Series: Practical guidance to qualitative research. Part 4: Trustworthiness and publishing. European Journal of General Practice, 24(1), 120-124.
- Noon, E. J. (2018). Interpretive phenomenological analysis:An appropriate methodology for educational research?. Journal of perspectives in applied academic practice, 6(1), 75-83.
- Toye, M. K., Wilson, C., & Wardle, G. A. (2019). Education professionals’ attitudes towards the inclusion of children with ADHD: The role of knowledge and stigma. Journal of Research in Special Educational Needs, 19(3), 184-196.
- Graham, S., & Weiner, B. (1996). Theories and principles of motivation. Prentice Hall.
- Weiner, B. (1985). An attributional theory of achievement motivation and emotion. Psychological review, 92(4), 548.
- Hendriksen, J. G. M., Peijnenborgh, J. C. A. W., Aldenkamp,P., & Vles, J. S. H. (2015). Diagnostic overshadowing in a population of children with neurological disabilities: a cross sectional descriptive study on acquired ADHD. European Journal of Paediatric Neurology, 19(5), 521-524.
- Katzman, M. A., Bilkey, T. S., Chokka, P. R., Fallu, A., & Klassen, L. J. (2017). Adult ADHD and comorbid disorders:clinical implications of a dimensional approach. BMC psychiatry, 17(1), 1-15.
- Pehlivanidis, A., Papanikolaou, K., Mantas, V., Kalantzi, E., Korobili, K., Xenaki, L. A., ... & Papageorgiou, C. (2020). Lifetime co-occurring psychiatric disorders in newly diagnosed adults with attention deficit hyperactivity disorder (ADHD) or/and autism spectrum disorder (ASD). BMC psychiatry, 20(1), 423.
- Mowlem, F. D., Rosenqvist, M. A., Martin, J., Lichtenstein, P., Asherson, P., & Larsson, H. (2019). Sex differences in predicting ADHD clinical diagnosis and pharmacological treatment. European child & adolescent psychiatry, 28(4), 481-489.
- Faraone, S. V., Bellgrove, M. A., Brikell, I., Cortese, S., Hartman, C. A., Hollis, C., ... & Buitelaar, J. K. (2024). Attention-deficit/hyperactivity disorder. Nature Reviews. Disease Primers, 10(1), 11.
- Walters, A. (2018). Girls with ADHD: Underdiagnosed and untreated. The Brown University Child and Adolescent Behavior Letter, 34(11), 8-8.
- Lynch, A., & Davison, K. (2024). Gendered expectations on the recognition of ADHD in young women and educational implications. Irish Educational Studies, 43(1), 61-81.
- Goffman, E. (1963). Stigma: Notes on the Management of Spoiled Identity. Touchstone.
- Granjon, M., Pillaud, N., Popa-Roch, M., Aubé, B., & Rohmer,O. (2025). Attitudes towards invisible disabilities: Evidence from behavioral tendencies. Current Research in Behavioral Sciences, 8, 100164.
- Masten, A. S., & Cicchetti, D. (2010). Developmentalcascades. Development and psychopathology, 22(3), 491-495.
- Russell, A., Hoxha, D., & Murray, A. (2025). Developmental relations between ADHD and self-esteem: evaluating peer problems as a mediating mechanism. European Child & Adolescent Psychiatry, 34(11), 3463-3473.
- Mullan, V. M., Golm, D., Juhl, J., Sajid, S., & Brandt, V. (2023). The relationship between peer victimisation, self-esteem, and internalizing symptoms in adolescents: A systematic review and meta-analysis. PLoS one, 18(3), e0282224.
- Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychological bulletin, 129(5), 674.
- Lund, E. M. (2021). Examining the potential applicability of the minority stress model for explaining suicidality in individuals with disabilities. Rehabilitation psychology, 66(2), 183.
- Chang, J. (2011). A Case Study of the" Pygmalion Effect": Teacher Expectations and Student Achievement. International education studies, 4(1), 198-201.
- Beamish, W., Gibbs, K., Toomey, M., & McGarrigle, L. (2022). Inclusive education in Australia: An unfolding reform. In The inclusion for students with special educational needs across the Asia pacific: The changing landscape (pp. 189-207). Singapore: Springer Nature Singapore.
- Chow, W. S. E., de Bruin, K., & Sharma, U. (2024). Ascoping review of perceived support needs of teachers forimplementing inclusive education. International Journal of Inclusive Education, 28(13), 3321-3340.
- Bondebjerg, A., Dalgaard, N. T., Filges, T., & Viinholt, B. C. A. (2023). The effects of small class sizes on students' academic achievement, socioemotional development and wellâ?ÂÂbeing in special education: A systematic review. Campbell Systematic Reviews, 19(3), e1345.
- Szép, A., Dantchev, S., Zemp, M., Schwinger, M., Chavanon,M. L., & Christiansen, H. (2021). Facilitators and barriers of teachers’ use of effective classroom management strategies for students with ADHD: A model analysis based on teachers’ perspectives. Sustainability, 13(22), 12843.
- Creagh, S., Thompson, G., Mockler, N., Stacey, M., & Hogan, A. (2025). Workload, work intensification and time poverty for teachers and school leaders: A systematic research synthesis. Educational Review, 77(2), 661-680.
- Madigan, D. J., & Kim, L. E. (2021). Towards an understanding of teacher attrition: A meta-analysis of burnout, job satisfaction, and teachers’ intentions to quit. Teaching and teacher education, 105, 103425.
- Bakker, A. B., & Demerouti, E. (2007). The job demandsâ?ÂÂresources model: State of the art. Journal of managerial psychology, 22(3), 309-328.
- Rahimi, M., & Arnold, B. (2025). Understanding Australia’s teacher shortage: The importance of psychosocial working conditions to turnover intentions. The Australian Educational Researcher, 52(1), 383-409.
- Schachter, R. E., Knoche, L. L., Lu, J., Goldberg, M. J., Wernick, P. D., Piasta, S. B., & Lancaster, H. S. (2025). A meta-analysis of the effectiveness of coaching and the contribution of coaching processes to learning outcomes for early childhood teachers and children. Early Childhood Research Quarterly, 72, 156-169.
- Korpershoek, H., Canrinus, E. T., Fokkens-Bruinsma, M., & De Boer, H. (2020). The relationships between school belonging and students’ motivational, social-emotional, behavioural, and academic outcomes in secondary education: A meta-analytic review. Research papers in education, 35(6), 641-680.
- Roorda, D. L., Jak, S., Zee, M., Oort, F. J., & Koomen, H. M. (2017). Affective teacher–student relationships and students' engagement and achievement: A meta-analytic update and test of the mediating role of engagement. School psychology review, 46(3), 239-261.
- Rosenthal, R., & Jacobson, L. (1966). Teachers' expectancies: Determinants of pupils' IQ gains. Psychological reports, 19(1), 115-118.
- McDougal, E., Tai, C., Stewart, T. M., Booth, J. N., & Rhodes,S. M. (2023). Understanding and supporting attention deficit hyperactivity disorder (ADHD) in the primary school classroom: Perspectives of children with ADHD and their teachers. Journal of autism and developmental disorders, 53(9), 3406-3421.
- DuPaul, G. J., Gormley, M. J., & Laracy, S. D. (2014). School-based interventions for elementary school students with ADHD. Child and adolescent psychiatric clinics of NorthAmerica, 23(4), 687-697.
- Owens, J. S., Qi, H., Himawan, L. K., Lee, M., & Mikami,Y. (2021, January). Teacher practices, peer dynamics, and academic enablers: A pilot study exploring direct and indirect effects among children at risk for ADHD and their classmates. In Frontiers in Education (Vol. 5, p. 609451). Frontiers Media SA.
- Epstein, J. L. (2010). School/family/community partnerships: Caring for the children we share. Phi Delta Kappan, 92(3), 81-96.
- Bordin, E. S. (1979). The generalizability of the psychoanalytic concept of the working alliance. Psychotherapy: Theory, research & practice, 16(3), 252.
- Goldberg, J. M., Sklad, M., Elfrink, T. R., Schreurs, K. M., Bohlmeijer, E. T., & Clarke, A. M. (2019). Effectiveness of interventions adopting a whole school approach to enhancing social and emotional development: a meta-analysis. European Journal of psychology of Education, 34(4), 755-782.
- Deci, E. L., & Ryan, R. M. (2000). The" what" and" why" of goal pursuits: Human needs and the self-determination of behavior. Psychological inquiry, 11(4), 227-268.
- McNaught, J., Biegun, D., & Swartzentruber, K. (2024). Student-led Individualized Education Programs: A gateway to self-determination. Language, Speech, and Hearing Services in Schools, 55(2), 276-302.
- Fox, L. (2013). Success factors 40 years later: The pioneer postsecondary program for students with learning disabilities, attention deficit hyperactivity disorder, and executive function. Learning Disabilities: A Multidisciplinary Journal, 19(1), 18-28.
- Ju, S., Zeng, W., & Landmark, L. J. (2017). Self-determination and academic success of students with disabilities in postsecondary education: A review. Journal of Disability Policy Studies, 28(3), 180-189.
- Lapidot-Lefler, N. (2025). Teacher responsiveness in inclusive education: A participatory study of pedagogical practice, wellbeing, and sustainability. Sustainability, 17(7), 2919.
- Griffiths, A. J., Alsip, J., Hart, S. R., Round, R. L., & Brady, J. (2021). Together we can do so much: A systematic review and conceptual framework of collaboration in schools. Canadian Journal of School Psychology, 36(1), 59-85.
- Jeremy, J., Spandagou, I., & Hinitt, J. (2025). Similarities and differences between perceptions and practices in occupational therapist-teacher collaborations: results from a mixed-methods study. Journal of Occupational Therapy, Schools, & Early Intervention, 18(3), 528-549.
- Isenor, K., Mazerolle, E., & Barker, C. (2021). Pay attention to this: A knowledge translation study of ADHD and its brain basis to preservice and in-service teachers. in education, 27(1),80-97.
- Noddings, N. (2012). The caring relation in teaching. Oxford review of education, 38(6), 771-781.
- Mehrabadi, A., Austin, N., Keyes, K. M., & De Vera, M.(2024). It’s personal: navigating research questions that stem from our lived experiences. International Journal of Epidemiology, 53(6), dyae132.
- Gore, J., Rickards, B., & Fray, L. (2023). From performative to professional accountability: Re-imagining ‘the field of judgment’through teacher professional development. Journal of Education Policy, 38(3), 452-473.
- Simoni, Z. (2021). Social class, teachers, and medicalisation lag: a qualitative investigation of teachers' discussions of ADHD with parents and the effect of neighbourhood-level social class. Health Sociology Review, 30(2), 188-203.
- Australian Bureau of Statistics. (2025). Schools.
- Robinson, O. C. (2014). Sampling in interview-based qualitative research: A theoretical and practical guide. Qualitative research in psychology, 11(1), 25-41.
- Diamond, I. R., Grant, R. C., Feldman, B. M., Pencharz, P. B., Ling, S. C., Moore, A. M., & Wales, P. W. (2014). Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. Journal of clinical epidemiology, 67(4), 401-409.
- Okoli, C., & Pawlowski, S. D. (2004). The Delphi method as a research tool: an example, design considerations and applications. Information & management, 42(1), 15-29.
- Donaldson, C., Moore, G., & Hawkins, J. (2023). A systematic review of school transition interventions to improve mental health and wellbeing outcomes in children and young people. School Mental Health, 15(1), 19-35.
- Holmes, A. G. D. (2020). Researcher Positionality--A Consideration of Its Influence and Place in Qualitative Research--A New Researcher Guide. Shanlax International Journal of Education, 8(4), 1-10.
- Australian Government Department of Education. (2023).National teacher workforce action plan.
- Johnston, O., & Palamara, P. (2025). Are Australian schools becoming less inclusive? Changes to class ability grouping practices in Australian secondary schools. International Journal of Inclusive Education, 1-23.
- Mulholland, S., Cumming, T. M., & Lee, J. (2023). Accurately assessing teacher adhd-specific attitudes using the scale for ADHD-specific attitudes. Journal of Attention Disorders, 27(5), 554-568.
- Young, K., & Clerke, T. (2024). Inclusion of students with disability in qualitative education research–a scoping review. International Journal of Qualitative Methods, 23, 16094069241244869.
Appendix A: Reflexive Statement
As a researcher and mother of three children diagnosed with ADHD, I enter this study with both professional curiosity and deeply personal insights into the complexities of navitating ADHD within the educational system. My lived experience has given me a nuanced understanding of challenges families face in advocating and accessing appropriate support within mainstream settings, as well as the systemic barriers that can shape the daily realities of students with ADHD. I am acutely aware of the emotional labour, advocacy and persistent navigation required to secure meaningful inclusion and the critical role teacher understanding, attitudes and their investment in fostering a supportive and trusting relationship with students, play in shaping these experiences. I am also incredibly fortunate in that the teachers supporting my children have been incredibly responsive and committed to their unique needs, at the same time, I acknowledge that this may not always be the case for others in negotiating school interactions.
While this positionality provides me with empathy and insight into the lived realities of students and families, I acknowledge that my personal connection to ADHD may shape how I interpret and engage with the stories and narratives shared by teachers [175]. I hold a strong belief in the potential of inclusive education to create meaningful opportunities for students with ADHD, and I recognise the emotional, relational and systemic complexities teachers navigate within this context. To address the potential for bias, I am committed to practicing reflexivity throughout the research process, using journalling and supervision to bracket my assumptions and remain attentive to the perspectives presented by participants [100].
Guided by IPA, I recognise that this research involves a double hermeneutic process, whereby I seek to make sense of how teachers themselves make sense of their experiences within evolving inclusive policies [100]. I aim to create a respectful, non-judgmental space for teachers to share their reflections, challenges and insights, valuing their expertise as central to understanding how inclusive practices for students with ADHD are enacted in practice. Through this research, I intend to honour teachers’ voices while remaining critically aware of my positionality, ensuring the findings authentically represent participants lived experiences so they can dependably contribute to informing policy and practice within the vision of an inclusive Australia.
Appendix B: Interview Schedule
Interview Schedule:
Note: [MS] – questions for mainstream [SE] questions for special education teachers
Opening Remarks
Good [morning/afternoon/evening], [Teacher’s Name]. Thank you for taking the time to participate in this interview. My name is [XXX]. I am a researcher hoping to gain insights from primary school teachers surrounding the changes to the education system proposed by the 2023 disability royal commission. Specifically, its proposal to phase out all special facilities and transform mainstream schools into inclusive learning environments. I’m interested in understanding your perspective on these changes and to draw on your experience and expertise to allow for insights into how these changes may be positively facilitated. I’m also interested in understanding your perspective on how this reform will impact students with ADHD.
During this interview I will be asking questions about various aspects of your experience as a teacher, more specifically, what tools and strategies you have found helpful in your practice. Please feel free to skip any questions you don’t wish to answer and please take your time answering any of these questions as this is integral to ensuring that your experience is accurately captured today. I also wanted to inform you that our chat will be recorded to review later, but your name or any identifiable details will be removed. Is that okay with you? To reiterate, this conversation will be anonymous and any potentially identifiable information will be removed from the final transcript to ensure your privacy and confidentiality is maintained. If at any point you feel uncomfortable or stressed during our chat, please just let me know and you are welcome to take a break, or we can adjust or skip the question and even stop the interview as your wellbeing is a priority. Additionally, if there is anything you wish to keep private or would prefer to discuss further, please just let me know and we can amend the transcript accordingly, You are more than welcome to stop me and ask questions along the way, but before we begin, is there anything further I can clarify for you or any other questions you would like to ask about today's conversation?Background and Teaching Motivations
1. Can you tell me about your journey to become a teacher?
2. What motivated you to pursue this career path?
3. How long have you worked as a teacher?
4. What characteristics, skills or strengths do you think enable you to be an effective teacher?
5. What does inclusivity mean to you? Perceptions of the Proposed Changes For a bit of context: In October 2023, the Australian Disability Royal Commission announced its proposal to phase out all special education facilities by 2052 with its long-term vision to make all mainstream schools inclusive.
6. What is your current understanding of the royal commission and how do you feel this will impact your school?
7. Specifically, how do you feel about the proposed phase-out of specialised facilities?
8. How do you think these changes will impact your role as a teacher??
9. How do you think these changes may impact your wellbeing?
10. What impacts might these changes have on: Probe: teacher workload, job satisfaction
11. Are there any specific concerns or questions you have regarding the implementation of these changes?
12. Are there any potential benefits or drawbacks to the proposed changes that you think have not been considered at a government level?
Advice for transforming mainstreams into inclusive learning environments
13. What advice would you give to other educators and policy makers to ensure that these changes are implemented in a way that benefits students with special needs?
14. [SE] What specific resources, training or professional development opportunities do you think mainstream educators would benefit from to effectively support the inclusion of students with special needs?
15. [MS] What specific resources, training or professional development opportunities do you think you would benefit from to support students with special needs?
16. What key considerations or priorities do you think should guide the implementation process?
17. What topics or areas of focus do you think would be most relevant for teachers who may not yet have experience with children with special needs? Impacts on Students with ADHD
18. Describe your experiences working with students with ADHD. Probe: Can you tell me more about your interactions with these students? Management of these students?
19. [SE] How would you describe your experiences working with mainstream educators and how do you feel your approaches to students with ADHD may be similar or different?
20. What do you think are the potential benefits, drawbacks of the reform for students with ADHD?
21. How might these changes affect the following areas for ADHD students in the long term?
Probe: vocationally, mental health, socially, academically 22. [SE] Do you feel that mainstream educators have the appropriate training?
23. [MS] Do you feel you have received adequate training for working with students with ADHD?
(Probe if: Yes- Can you please give more specific details about this training? (Probe if No - What training would you like to receive?
24. How confident to you feel about teaching students with ADHD?
25. Based on your experience, what does the ideal inclusive classroom look like for students with ADHD?
(Probes: Support systems, structures, accommodations, seating arrangements, learning aids, technology.)
26. [SE] How is this similar/ different to the typical mainstream classroom setup?
27. Are there any specific strategies or evidence-based interventions that you think will be particularly effective in supporting students with ADHD in an inclusive classroom?
28. How do you think the proposed changes will impact a teacher’s ability to provide individualised support to students with ADHD?
29. How do you think the proposed changes will impact the identification and diagnosis of ADHD in students?
30. Is there anything else you would like to share about your experiences or perceptions regarding the proposed changes to the education system?
Closing Comments
Thank you so much, [Teacher’s Name], for sharing your thoughts and experiences with me today. Your insights are incredibly valuable for our research, and I appreciate your openness. As for the next steps, once I have transcribed and our discussion, I will email it to you so you can have a read through, and if there is anything you would like removed or added please let me know. Before we finish, I want to check in on your experience. How did you feel about our conversation? Was there anything that made you uncomfortable or anything you would like to discuss further? If there is nothing else you would like to add or discuss, I want to thank you once again for your time and thoughtful participation. Take care, and if you ever have more questions don’t hesitate to reach out.