
Advances in Hematology and Oncology Research(AHOR)
ISSN: 2692-5516 | DOI: 10.33140/AHOR
Impact Factor: 1.2


Case Report - (2025) Volume 8, Issue 2
Left Supraclavicular Hodgkin Lymphoma: A Case Report and Literature Review
2ENT Consultant, Zain Hospital, Kuwait
3Professor of ORL-HNS, Alexandria University, Kuwait
Received Date: Sep 17, 2025 / Accepted Date: Oct 20, 2025 / Published Date: Oct 24, 2025
Copyright: ©Â©2025 Ahmad Alenezi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Alenezi, A., Zahran, M., Alsaidan, L. (2025). Left Supraclavicular Hodgkin Lymphoma: A Case Report and Literature Review. Adv Hema Onco Res, 8(2), 01-04.
Abstract
Herein, we report a case of classical Hodgkin’s lymphoma (HL) in an otherwise healthy 24- year-old female who came to the outpatient clinic in the otolaryngology-head and neck surgery department with flu like illness and left supraclavicular swelling of uncertain nature, without other symptoms. An ultrasound of the soft tissue detected an enlarged oval shaped left supraclavicular lymphadenopathy. Subsequent computed tomography scan of the chest and upper abdomen shows anterior mediastinal mass likely thymic origin. The diagnosis of classical Hodgkin’s lymphoma, ovoid firm nodular lymphoid piece, was made on a subsequent supraclavicular lymph node biopsy.
Introduction
The modern classification of Hodgkin’s disease was introduced by Lukes and Butler [1].
Hodgkin lymphoma is a lymphatic malignancy commonly found in cervical lymph nodes. The incidence and mortality were 0.98 and 0.26 per 100,000 in 2020. A higher incidence was observed in high income countries, while higher mortality was found in low-in- come countries. Despite the decreasing mortality trend, there was an increasing incidence, especially among females, younger pop- ulation, and subjects from Asian countries. Recently, the survival rate of Hodgkin lymphoma has been improved due to the advances in antibody therapy. Other promising therapies included vaccine therapies, checkpoint inhibitors, and cytotoxic T lymphocytes [2]. Here we will present a case of classical Hodgkin lymphoma of left supraclavicular lymph node in Kuwait.
Case Report
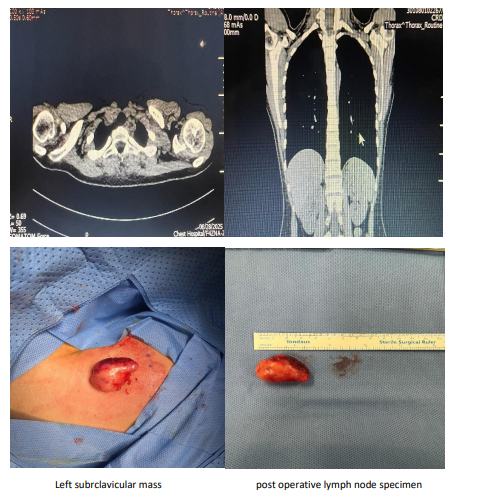
A 24-year-old female patient, previously healthy, presented to the out-patient-clinic with 2 months history of left sided supraclavic- ular swelling, her symptom associated with flu like symptoms which was generalized fatigue, recurrent fever and body ache. She also experienced a heavy breathing from time to time. Patient was on antibiotic which didn’t improved her symptoms. On physical examination, she was conscious, oriented and alert. Her vital signs were within normal range. She had a left supraclavicular swelling, which is about 2x1 cm in size. The facial sensation was intact. No other palpable lymph nodes in the submental, cervical, axillary and auricular region. Laboratory studies showed white count level of 8.8x109 /L, a hemoglobin level of 114 g/L, creat-nine level of 48.21 mmol/L, sodium of 136.37 mmol/L and potassium of 4.44 mmol/L. an ultrasound of soft tissue showed A left supraclavicular oval shaped discrete hypoechoic mass lesion with smooth surface measuring about 24x11 mm in cross diameters, likely representing enlarged lymph node. A contrast enhanced computed tomography scan of chest and upper abdomen showed anterior mediastinal well-defined smoothly-marginated soft tissue mass most likely thymic measuring 28x24 mm with mild post contrast enhance- ment, no calcification or breakdown. A pulmonary function test showed FEV1 of 3.02, FVC of 3.46 and FEV1 % FVC of 84.35.
Thus, the patient underwent mass excision under general anesthe- sia. The operation started by a 3cm incision made on the left lower part of the neck, dissection of the subcutaneous tissue with dissec- tion carefully around the left supraclavicular lymp node. Preser- vation of the surrounding structures and hemostasis achieved. The mass was sent for histopathology. Post-oper-atively the patient was doing well, kept on antibiotic (Augmentin) and pain killer (Adol), patient discharged the next day on same medications for 7 days. The histopathology result showed a single ovoid firm grey nodular lymphoid piece of tissue measuring 3.5x2.0x1.0 cm, weighing 4.0 grams, the cut section is nodular with occasional vague nodules.
Scattered atypical large cells are seen resembling RS cells, some multi-lobated and some mummified in a background of mixed in- flammatory cells composed of lymphocytes and some plasma cells. The atypical cells are predominantly negative for CD45, CD 20, OCT2, BOB1, while positive for CD30, MUM-1, PAX5 (weak, as compared to background reactive B cells), and CD15 (positivity in the atypical cells). CD3 is highlighting reactive T-lymphocytes. EBV (ISH) is negative. Diagnosis is a classical Hodgkin lympho ma of left supraclavicular lymph node. Later, the patient will be followed by Kuwait Cancer Center.
Discussion
HL has an incidence of approximately 15% and is characterized by the presence of Reed-Sternberg (RS) cells which are also CD 30 positive in all cases [3]. They are CD15 positive on immunohis- tochemical staining in 80%-85% of cases. Definitive diagnosis is made by the presence of RS cells and immunophenotyping. Fur large cell lymphoma (ALCL), and gray zone lymphoma are some differentials for CD-30 lymphomas. AVD-A (which is brentux- imab vedotin, doxorubicin, vinblastine, and dacarbazine) combination has been compared with ABVD combination in a prospective randomized phase III trial [3].

CD30 expression Scattered Reed-Sternberg cells (RS)
Because Hodgkin lymphoma is considered a curable malignancy and the differential diagnosis is broad, medico-legal problems may arise from failure to diagnose the disease in a timely manner, possibly due to the following factors: 1)The misinterpretation of B symptoms (fever, night sweats, weight loss), pruritis; A lack of follow-up for abnormal chest radiographs or physical examination findings; 3) A missed pathologic diagnosis because a needle biopsy was obtained rather than an excisional lymph node biopsy, An excisional lymph node biopsy is recommended because the lymph node architecture is important for histologic classification [4].
Furthermore, the Ann Arbor classification is used most often for Hodgkin lymphoma, as follows:
• Stage I: A single lymph node area or single extra-nodal site
• Stage II: 2 or more lymph node areas on the same side of the diaphragm
• Stage III: Lymph node areas on both sides of the diaphragm
• Stage IV: Disseminated or multiple involvement of the extra-nodal organs [4].
A definitive cytologic diagnosis of HD required the identification of classic Reed–Sternberg (R-S) cells in a reactive inflammatory background including normal appearing lymphocytes, esoinophils, histiocytes, and plasma cells. The classic R-S cells were characterized by a bilobed or binucleated nucleus with a prominent, inclusion-like nucleolus in each lobe or nucleus and variable amount of cytoplasm. The nucleoli were often the size of a red blood cell or larger. A diagnosis of suspicious for HD was made when only R-S cell variants were identified. Reed–Sternberg cell variants were similar to the classic R-S cells except that they could be mononucleated, hyperlobated, or multinucleated with complex infoldings or overlapping nuclear segments. Nucleoli ranged from single, small, and inconspicuous to multiple, large, and prominent. For patients with a previously established diagnosis of HD, the presence of R-S cell variants in the proper milieu was sufficient to document recurrence. The original cytologic diagnosis were clas- sified into the following subcategories: 1) positive for HD, 2) positive for malignant neoplasm, other than HD, 3) suspicious for HD, 4) atypical lymphoproliferative process, 5) benign conditions, and 6) nondiagnostic. Cases that were classified as “atypical” showed rare large atypical mononuclear and/or hyperlobated lymphoid cells in a mixed inflammatory background [5].
Treatment of early stage Hodgkin lymphoma
Combined chemotherapy and radiotherapy (combined modality treatment) are strongly recommended, which has the potential to achieve high primary tumor control with low treatment-related toxicity. The recommended regimen for combined modality treatment is two cycles of ABVD (doxorubicin, bleomycin, vinblas- tine, DTIC = dacarbazine), followed by involved-field radiothera- py (IF-RT) with a radiation dose of 20 Gy (5-year overall survival rate: 94%), (2.8% WHO grade III/IV acute toxicity).
Treatment of intermediate stage Hodgkin lymphoma
a combination of chemotherapy followed by IF-RT with a total dose of 30 Gy, two cycles of BEACOPP escalated (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarba- zine, prednisone) followed by two cycles of ABVD over four cycles of ABVD (5-year overall survival: 97.2% versus 96.8%), with comparable toxicity (WHO grade III/IV: thrombopenia 21.9%, leukopenia 79%, infections 7.3%, nervous system 3.2%).
Treatment of advanced stage Hodgkin lymphoma
treatment with six cycles of BEACOPP escalated is strongly recommended, after chemotherapy, consolidation radiotherapy of PET-positive residual mass ≥2.5 cm is strongly recommended, A positive finding should be irradiated with 30 Gy. This strategy has achieved a 5-year overall survival rate of 95.3%, and none of those patients experienced any radiotherapy-related WHO grade IV toxicities.
Treatment of recurrences
After first-line treatment, 15% to 20% of patients experience a primary progression or relapse [6]. The treatment recommendations for this group of patients are as follows: For patients up to the age of 60 with relapsed HL it is strongly recommended to administer high-dose chemotherapy with autologous stem-cell transplantation, There is currently no international standard for salvage therapy, but two cycles of intensive DHAP (dexamethasone, high-dose cytosine arabinoside [Ara-C], cisplatin) should be administered, based on an effective response rate of 89% and a relatively low complication rate of 48% WHO grade III/IV toxicity [6].
Conclusion
Hodgkin Lymphoma (HL) has an incidence of approximately 15% and is characterized by the presence of Reed-Sternberg (RS) cells, which are CD30 positive in all cases and CD15 positive in 80%-85% of cases based on immunohistochemical staining. The definitive diagnosis of HL is made through the identification of RS cells and immunophenotyping.The Ann Arbor classification is commonly used to stage Hodgkin Lymphoma, ranging from Stage I (a single lymph node area or site) to Stage IV (widespread in- volvement of extralymphatic organs).
In treatment comparisons, a phase III trial evaluated the AVD-A (brentuximab vedotin, doxorubicin, vinblastine, and dacarbazine) combination against the ABVD combination.
References
- Lukes, R. J., Butler, J. J., & Hicks, E. B. (1966). Natural his- tory of Hodgkin's disease as related to its pathologic picture. Cancer, 19(3), 317-344.
- Huang, J., Pang, W. S., Lok, V., Zhang, L., Lucero-Prisno III,D. E., Xu, W., ... & NCD Global Health Research Group, As- sociation of Pacific Rim Universities (APRU). (2022). Inci- dence, mortality, risk factors, and trends for Hodgkin lympho- ma: a global data analysis. Journal of hematology & oncology, 15(1), 57.
- Benn, G., Adidam, S., Ali, A., & Taddesse-Heath, L. (2021). A case of classical Hodgkin’s lymphoma presenting with intrac- table pruritus. Cureus, 13(11).
- Bolognesi, M., Bolognesi, D., & Pasini, G. A classical presen- tation of Hodgkin’s disease in a 27-year-old healthy female.
- Chhieng, D. C., Cangiarella, J. F., Symmans, W. F., & Cohen,J. M. (2001). Fine-needle aspiration cytology of Hodgkin disease: A study of 89 cases with emphasis on the false-negative cases. Cancer Cytopathology, 93(1), 52-59.
- Rancea, M., Engert, A., von Tresckow, B., Halbsguth, T., Behringer, K., & Skoetz, N. (2013). Hodgkin’s lymphoma in adults: diagnosis, treatment and follow-up. Deutsches Ärzteb- latt International, 110(11), 177.