



Case Report - (2019) Volume 4, Issue 3
Left Atrial Myxoma A Clinical Case
Received Date: Dec 07, 2019 / Accepted Date: Dec 16, 2019 / Published Date: Dec 31, 2019
Copyright: ©Juan Francisco Perez Salum. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Cardiac tumors are generally benign. But its danger lies not in its potential malignancy, but in its location. These tumors settle inside the cardiac cavities, at the origin or mouth of the great vessels or even on the valves. This can obviously lead to life-threatening complications, either due to mechanical causes or disturbances in the electrical conduction of the heart. Cardiac tumors are very rare and occur in both neonates and the elderly. These tumors can be confused with thrombi, abscesses or vegetations, so a correct diagnosis is essential [1]. Echocardiography is a very important diagnostic tool and its appearance allowed the early diagnosis of these tumors, which were previously diagnosed only post mortem [2]. Here I present a case of a Japanese 66 years old female, in treatment since March 2013 for hyperthyroidism, in use of metimazol 5 mg/24 hs, propanolol 10 mg/24 hs. She is not diabetic, nor hypertensive, but she has dyslipidemia [3].
Introduction
Cardiac tumors are generally benign. But its danger lies not in its potential malignancy, but in its location. These tumors settle inside the cardiac cavities, at the origin or mouth of the great vessels or even on the valves. This can obviously lead to life-threatening complications, either due to mechanical causes or disturbances in the electrical conduction of the heart.
Cardiac tumors are very rare and occur in both neonates and the elderly. These tumors can be confused with thrombi, abscesses or vegetations, so a correct diagnosis is essential [1].
Echocardiography is a very important diagnostic tool and its appearance allowed the early diagnosis of these tumors, which were previously diagnosed only post mortem [2].
Here I present a case of a Japanese 66 years old female, in treatment since March 2013 for hyperthyroidism, in use of metimazol 5 mg/24 hs, propanolol 10 mg/24 hs. She is not diabetic, nor hypertensive, but she has dyslipidemia [3].
She denies allergies. The patient does not have history of ethylic intake and she does not smoke. The functional class (NYHA) is II/ IV. Syncope in one opportunity eight years ago. Previous surgeries: appendectomy, two cesareans.
At 28 October 2014, by 5 P.M, the patient had felt left hand paralysis. She went to a Clinician, who recommended attention by a Neurologist. The Neurologist asked for a IRM where he saw an old and another new lacunar ischemia. He had ordered an echocardiography and vascular Doppler of Carotid and Vertebral arteries. The patient begun clopidogrel 75 mg + aspirin 100 mg/24 hs and atorvastatine 80 mg/24 hs.
She came to my laboratory by November 6th 2014 just to do those studies. In the vascular Doppler of Carotid and Vertebral arteries no significant lesions were reported. In the echocardiography it was possible to see a mass in left atrium with gelatinous aspect with approximately 4.2 cm by 2,5 cm. It seemed to had a base of implantation in the atrial septum and it was mobile.
The possible diagnosis was a left atrial myxoma. For this reason, referral to a cardiac surgeon is asked. She went to the Division of Cardiovascular Surgery of Jichi Medical University (Japan). There she was submitted to surgery in 19th November 2014, without complications; and the diagnose was confirmed. From this day until nowadays, she is assympthomatic.
Discussion
The clinical features of cardiac tumors are determined by their location, size and mobility. There is no pathognomonic sign or symptom. The most common symptom is systemic embolism (present in this patient). A common sign is heart failure, due to mitral valve obstruction. Also is possible sudden death after abrupt mitral valve obstruction [4].
Other complications described are heart rhythm disorders (absent in this patient). In the right atrial myxomas there is a higher incidence of atrial fibrillation, especially when they cause tricuspid stenosis [5]
In patients with myxomas, an increase in IL-6 levels has been seen to decrease after tumor removal, and which appears to be related to the synthesis of IL by tumor cells [6].
Valvular lesions occur when the tumor affects valvular structures, usually when they have their implantation base near the atrioventricular orifices [7].
Conclusion
Atrial myxomas are benign tumors, but similar to other cardiac tumors, their danger is mainly due to their anatomical location. Myxomas can pass silently for years and at the time of starting their clinical manifestations they can simulate various pathologies, from inflammatory disorders to embolic complications.
Despite its low incidence it is important to know the cardiac tumors and their possible clinical manifestations, as well as their differential diagnosis, because they are potentially curable conditions if the treatment is administered in a timely manner.
Acknowledgements
My special thanks to Prof. Hirotaka Sato, for sending me the photography of the surgical specimen and the history of the patient during her hospitalization at the Division of Cardiovascular Surgery of Jichi Medical University (Japan).
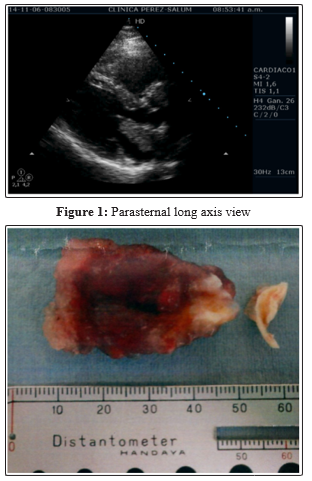
Figure 2: surgical specimen (courtesy of Prof. Hirotaka Sato, Division of Cardiovascular Surgery of Jichi Medical University, Japan)
References
- Masuda I, Ferreño A, Pasca J, Gustavo Pereiro, Hugo Lastiri (2004) Tumores cardiacos primarios. Mixoma auricular. Rev Fed Arg Cardiol 33: 196-204.
- Abad C (1998) Tumores cardiacos (I). Generalidades Tumores primitivos benignos. Rev Esp Cardiol 51: 10-20.
- Nizahel Estevez Alvarez, Vladimir Rodriguez, Angel M Paredes Cordero, Guillermo Mojena Morfa, Horacio Perez Lopez, et al. (2014) Tumores cardiacos primarios. Generalidades y particularidades clínicas. Revista Cubana de Cardiología y Cirugía Cardiovascular 20: 193-202.
- Bartoloni G, Pucci A (2013) Cardiac myxoma. In: Basso C, Valente M, Thiene G. Cardiac Tumor Pathology. Humana Press, London 31-44.
- Blanco A, Moreno A, González A, Romero-Berrocal A, García-Fernández J (2015) Tumores primarios cardíacos. Complicaciones y manejo anestésico. Revista Mexicana de anestesiología 38: 289-292.
- Mendoza CE, Rosado MF, Bernal L (2001) The role of interleukin-6 in cases of cardiac myxoma: clinical features, immunologic abnormalities, and a possible role in recurrence. Tex Heart Inst J 28: 3-7
- Ramírez M, Anguita M, Castillo J, Juan R Siles Rubio, Manuel Franco Zapata, et al. (1998) Mixoma ventricular izquierdo aislado descubierto casualmente por ecocardiografía. Rev Esp Cardiol 51: 763-765.