

Research Article - (2025) Volume 10, Issue 1
Knowledge, Perceptions, andAwareness of CRC Screening, Diagnoses, and Riskfactors Among Nurses working in Private Hospital a located in Sandton, South Africa
Received Date: Dec 05, 2024 / Accepted Date: Dec 29, 2024 / Published Date: Jan 08, 2025
Copyright: ©©2025 Ramatsimele Lerato Makgatho, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Makgatho, R. L., Mapungwana, P., Chadyiwa, M. (2025). Knowledge, Perceptions, and Awareness of CRC Screening, Diagnoses, and Risk factors Among Nurses working in Private Hospital a located in Sandton, South Africa. J Nur Healthcare, 10(1), 01-14.
Abstract
Colorectal cancer (CRC) is a significant public health concern on a global scale, and this includes South Africa. It ranks as the third most common form of cancer and the second leading cause of cancer-related deaths worldwide, with 1,931,590 new cases and 935,173 fatalities reported in 2020 alone. Early detection through screening plays an indispensable role in mitigating mortality rates associated with CRC. The objective of this study is to evaluate the perceptions, knowledge base, and awareness regarding CRC screening protocols, diagnoses and risk factors among nurses employed at Private in Sandton, South Africa.
Methods: A cross-sectional study was carried out on 200 nurses employed at Private Hospital A in Sandton, South Africa. The data pertaining to the nurses' perceptions, knowledge and awareness of CRC screening, diagnoses and risk factors were collected through a self-administered questionnaire. The strengths of each relationship were analyzed using SPSS software, while an assessment of the association between these relationships was conducted through both univariate and multivariate binary logistic analysis. In univariate analysis, variables with a p value of 0.1 or less were included in multivariate logistic regression model. Statistical significance was set at a p value of 0.05 or less. Logistic regression results were expressed as odds ratios (ORs) with 95% confidence intervals (CIs).
Result: The findings of this study revealed that a significant proportion of the participating nurses had insufficient knowledge about standard colorectal cancer (CRC)screening tests recommended by WHO guidelines. Specifically, many were unaware of the optimal frequency for colonoscopy or how occult blood tests should be administered. The absence of oncology-related CPD in this research was linked to inadequate understanding among nurses regarding CRC diagnoses and screening protocols. However, a satisfactory number of nurses demonstrated sufficient knowledge about CRC risk factors. The data derived from this research on assessing the receipt or availability of oncology-related CPD indicated that only a small percentage (6.5%) received such training in the last six months, while an overwhelming majority (93.5%) never did so during that period. Regarding what influences nurses' interest in conducting CRC screening and its overall impact on colorectal cancer screening results, it was found that those who feared having cancer had higher odds than others ('fear that I might have it'). This belief proved statistically significant at 95% CI (AOR:2.602, 95% CI 0.547 -12.368). Overall, the study results suggested that many nurses across different categories reported receiving no training in oncology, which negatively impacted their perception, knowledge and awareness about CRC screening procedures as well as diagnoses and risk factors associated with this disease.
Conclusion: There is currently a notable lack of knowledge pertaining to CRC screening and diagnosis among nurses employed at Private Hospital A in Sandton, South Africa. The study's findings highlight the pressing necessity for comprehensive training programs that are specifically tailored towards oncology, with an emphasis on CRC screening and diagnosis. It is crucial for both governmental bodies and educational institutions within South Africa to advocate for such initiatives in order to combat the concerning increase of CRC cases, as well as enhance nurses' awareness and understanding in this vital area.
Keywords
Colorectal Cancer, Diagnoses, Screening, Risk Factors, Nurses
Introduction
According to the World Health Organization (2023), cancer is the second leading cause of death globally, accounting for an estimated 9.6 million deaths, or 1 in 6 deaths1, in 2018. Catherine De Martel emphasized that the burden of cancer resulting in millions of deaths per year is rapidly growing [1]. Nagai and Kim (2017:448) also elaborated in their studies that cancer is one of the leading causes of morbidity and mortality worldwide following ischemic heart disease. In Africa, it was evident that cancer incidence increased from 715,000 in 2008 to 1.1 million in 2020 and cancer deaths increased from 542,000 in 2008 to 711,000 in 2020.By site, the main groups of breast, cervical, prostate, liver, and colorectal cancer accounted for 48% and 45% of new cases and deaths in Africa. In South Africa alone, cancer is also one of the health system challenges: it was found that cancer was responsible for 1.9 million deaths in South Africa in 2022 [2]. Among these cancers that inevitably lead to death, colorectal cancer (CRC) is the third most common cancer in men and the second most common in women, causing a high mortality rate worldwide. Also, in South Africa, a total of 33,232 CRC cases and 26,836 CRC deaths were reported during the population-based CRC study in 2002–2014 [3]. Despite this increase in colorectal cancer mortality rates, there is still inadequate knowledge about cancer in developing countries (Matteuzzi and Lippi, 2019) For society to be informed about public health problems, experts must identify, investigate, and educate about these problems and provide the necessary information [4,8]. This study investigated the perception, knowledge and awareness of colorectal cancer screening, diagnoses and risk factors among nurses working in the private hospital A in Sandton South Africa.
Awareness and Perception of Colorectal Cancer Amongst Nurses Regarding Screening
The World Health Organization (2020) defines screening as the presumptive identification of an unrecognized disease or defect by applying tests, examinations, or other procedures that can be used rapidly. It is executed to reduce mortality by early detection and treatment of a condition, to reduce the incidence of a disease by identifying and treating its precursors, and to reduce the severity of illness by identifying people with the disease and offering effective treatment [5]. A qualitative study was done in South Africa regarding how health professionals perceive the burden and screening of colorectal cancer, the study identified the impediments to CRC screening as follows: absence of a national screening program, the inadequacy of medical insurance, a remoteness of health facilities, inadequate health infrastructure, negative attitude towards screening, invasive procedures, and incompetence in service providers and unskilled health providers [6].
In 2016, another cross-sectional survey was conducted among nurses and physicians regarding their attitudes and knowledge as barriers to colorectal cancer screening [6]. The study found that more than 55% of nurses and physicians did not know how frequently certain screening procedures are performed, the upper age limit recommended for screening, and, most importantly, that patients are at high risk of colorectal cancer [6]. This then indicated a lack of knowledge about colon cancer screening. The author then recommended that improving health knowledge about colorectal cancer screening should be considered as a primary measure to promote colorectal cancer screening and prevention [6]. In 2018, a cross-sectional study of 450 medical and nursing students was conducted at the University of Jordan. The researchers found that the majority of students (65.1%) had little knowledge of colorectal cancer screening guidelines. However, knowledge scores increased significantly the higher the academic level and age of the students. The researcher recommended improving the curriculum and educational support through a review of the components of the cancer study (Rababah et al., 2018).
Poor CRC detection appears to be a major problem in Africa in general. One of the studies conducted by the World Bank in 108 middle-income countries showed CRC screening results in six lower-middle-income countries and 23 upper-middle-income countries (Michel and Pumpalova, 2023). The study highlighted that countries with organised screening programs have high participation in screening. Countries without the program have low screening uptake and, in most cases, nurses in primary health care settings are the driving force behind screening. In this sense, one of the obstacles was the lack of interest among physicians or the lack of acceptance of CRC screening programs (Michel and Pumpalova, 2023). However, nurses are considered advocates for the health of patients. If they had good insight and knowledge about colorectal cancer screening, diagnosis, and risk factors, the presentation of results would have been different. In conclusion of their study, researchers recommended addressing barriers, lack of knowledge, and lack of interest when a clinician initiates a program (Michel and Pumpalova, 2023).
The findings of Muliira., et al (2016) demonstrated that the participant's attitudes toward CRC screening was mostly positive, as indicated by their statements such as “CRC is preventable” (76.1%), and “CRC screening is beneficial” (83.1%) [6]. These findings show that the participants had good attitudes about CRC screening. Nevertheless, the problem was that their experiences and knowledge regarding CRC screening were inadequate. In addition, Magwaza, Van Hala, and Hoque’s (2023) recent descriptive cross-sectional study on “Health workers' knowledge, attitudes and practices on colorectal cancer screening in primary care in Durban, South Africa revealed that there was a lack of knowledge about colorectal cancer- screenings [4]. It was also stated by the same authors that health professionals (nurses) would be willing to carry out screenings only after training. However, it was also highlighted that there are no guidelines for national standards for colorectal cancer screening in South Africa.
Factors Affecting the Perceptions, Attitudes, and Awareness of Colorectal Cancer Risk Factors Amongst Nurses
There are various factors affecting screening behavior for CRC that impact the utilization of screening services, including the availability of national guidelines, service provider-related factors(knowledge, education, competencies, recommendation, availability, and functionality of equipment), and patient-related factors (age, ethnicity, gender, cancer personal and family history, education, income, distances of screening facilities, risk factors perception and procedure-related burdens)(Adonis et al.,2014). Colorectal cancer has disproportionately affected the black community, with the highest rates for any racial/ethnic group in Africa. Africans are about 20% more likely to get colorectal cancer and about 40% more likely to die from it than any other group (Augustus & Ellis,2018) [7]. The risk factors affecting CRC are vast, but in literature, inadequate oncology-related health literacy among patients is most mentioned when it comes to developing countries (Augustus & Ellis,2018) [7]. However, it is not clearly established if South African nurses have adequate knowledge about CRC risk factors as there are only very few studies conducted on nurses' perceptions and awareness relating to the risk of CRC in developing countries like South Africa. In a descriptive study conducted on 132 student nurses who are Asian assessing the awareness of risk factors for CRC, the study found that 75% of the nurses who were aware that long-term red meat consumption increases cancer risk were the junior student nurses and that those risk factors are less known by senior (Akduran & Cinar, 2015) [8]. Another study done in Saudi Arabia on knowledge and awareness regarding colorectal cancer among health sciences students. Their findings on knowledge about the various risk factors of CRC indicated that amongst the participants, only 34.4% could precisely mention five out of twelve CRC risk factors (Aga et al.,2021). Additionally, the overall adequacy of knowledge for the CRC was measured to be very low, with the majority, 65.6% of the respondents, failing to identify the risk factors correctly (Aga et al.,2021).
In a cross-sectional study that investigated breast, cervical, and colorectal cancer knowledge among nurses in Turkey, about 40.3% of the nurses were not aware that they could be at risk for colorectal cancer. In addition, 64.2% of the nurses were keen to have information about cancer and screening tests (Andsoy & Gul,2014) [9]. The author then recommended that nurses play an active role in health education and that they can be positive role models in society. Therefore, the increase in nurses’ self-awareness can increase society’s awareness. Special education about cancer screening programs may be helpful for nurses [9].
Fear, Cultural, Spiritual, and Cultural Beliefs as Some of the Factors that Impact Nurses' Perceptions and Awareness of Colorectal Cancer Screening, Diagnoses, and Risk Factors
Vrinten, Waller, von Wagner, and Wardle (2020) examined fear as a facilitator and barrier to participation in cancer screening and stated that fear of cancer was associated with higher and lower screening rates in different studies [10,11]. Muthukrishnan, Arnold, and James (2019) also stated that the main problem of CRC screening, especially in the developing population of the country, is cost and lack of insurance; However, when participants were asked open-ended questions about obstacles, fear was still a greater problem. In the conclusion of the study, they recommended the development of communication or intervention strategies to increase CRC screening and risk management rates in appropriate medical facilities in the public sector [11]. In one of the study findings participants had low knowledge levels about CRC and they misconceived colorectal cancer symptoms to be the result of hemorrhoids, karma, and heredity (Mahmood., 2023) [12]. Although the literature review could not precisely point out nurses' perceptions and awareness of CRC screening in terms of culture, religion, and spiritual beliefs, this study was able to investigate the nurse’s knowledge on colorectal cancer screening, diagnoses and risk factors amongst nurses working in one of the private hospitals in Sandton.
Methods
The study was conducted in one of the private hospitals in Sandton using a descriptive cross-sectional study design to describe the state of phenomena or the relationships between phenomena at a specified point in time. The researcher can use descriptive cross- sectional studies to examine the association or relationship between cancer perceptions, knowledge and awareness and other factors such as availability of training, ethnic groups, nursing, spiritual, religious, or cultural categories (Aggarwal and Ranganathan, 2019) [13]. The study design is known for its lower ethical implications and cost-effectiveness. It also allows the use of multiple variables, which is useful for increasing the precision of the study.
Results
This section presents the outcome or the results of the study.

Figure 1: Bar Chart on Work Division in Nursing Distribution
The bar chart shows an uneven distribution of respondents in the nursing work division survey, with the Intensive Care Unit having the highest percentage at 23.5%. The Emergency Department and Medical Unit follow with 15.5%to 16.7%. Other units/wards have around 5% each. The participants were selected regardless of their division within the institution.

Figure 2: Normality Curve on Category in Nursing Distribution
The bar graph shows that the distribution of nursing values in the study dataset is not normally distributed and lacks a trend of normality. The mean nursing value for respondents is 2.89, indicating registered nurses. However, the large standard deviation of 2.096 suggests that nursing values are not closely clustered around the mean, leading to skewed distribution where certain categories are larger than others.

Figure 3: Pie Chart on Gender Distribution
The above presentation shows that male participants were less when compared to females in this study. Statistical data of 34,5% males and 64.5% females as presented in the pie chart supports this assertion.
The data depicted the ethnicity of the nurses who
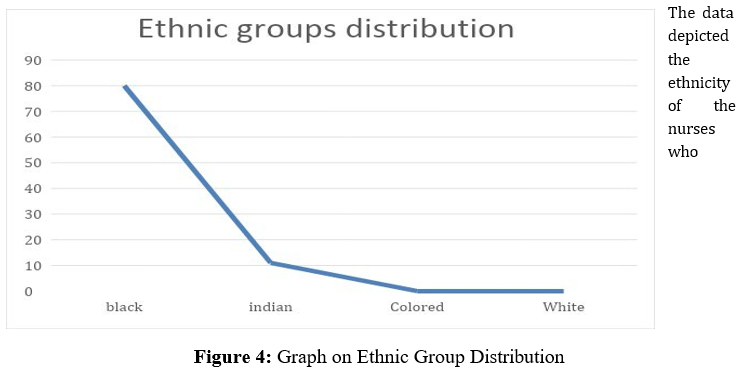
Figure 4: Graph on Ethnic Group Distribution
participated in this study. indicates that the study participants were predominantly black nurses, with only a small percentage of colored/white nurses. This is supported by the statistical data, which shows that only 4.5% of the participants identified as colored/white, while 80% identified as black. The line graph also corroborates this information, visually depicting the large proportion of black nurses compared to other ethnic groups. This finding is consistent with the reported demographics of nurses in South Africa. According to the South African Nursing Council, black nurses make up the majority of the nursing workforce, comprising approximately 85% of registered nurses. This is due to historical factors, such as apartheid and the lack of opportunities for colored/white nurses during that era. It is important to note that the study's findings are specific to the particular institution and may not necessarily reflect the demographics of nurses in other healthcare settings or regions of South Africa. However, the data does provide valuable insights into the ethnic composition of the nursing workforce in the context of the study.

Figure 5: Pie Chart on Oncology CPD Distribution
The data presented indicates a significant gap in oncology training among nurses who participated in the study. Only 6.5% of nurses reported receiving oncology continuing professional development (CPD) training, while a large majority of 93.5% didn't receive any CPD training. This suggests that many nurses have limited or outdated information about colorectal cancer. The pie chart visually represents this disparity, with a small segment representing the nurses who received oncology CPD training and large segment representing those who did not. This visual representation reinforces the conclusion that a substantial proportion of nurses lack up-to-date knowledge about colorectal cancer.

Figure 6: Normality Curve on the Necessity to Know About the Risk Factors of Colorectal Cancer Distribution
The results on this graph indicate that the data is normally distributed and shows a trend of normality. The mean response for the category "necessary to know about the risk factors of colorectal cancer" was 1.83, which is interpreted as a prevention of illness. The small standard deviation of 0.949 indicates that the values of the study dataset for this category are close to the mean value.
|
Characteristics |
Total |
|
|
N |
% |
|
|
Demographic data 1. Name your work division |
||
|
Medical unit |
32 |
16,0 |
|
Emergency department |
33 |
16,5 |
|
Theatre ward |
12 |
6,0 |
|
Maternity ward |
12 |
6,0 |
|
Orthopaedic ward |
12 |
6,0 |
|
Paediatric ward |
12 |
6,0 |
|
Surgical ward |
19 |
9,5 |
|
Gynae ward |
5 |
2,5 |
|
Dialysis |
9 |
4,5 |
|
Other |
3 |
1,5 |
|
ICU |
42 |
21,0 |
|
2. Tick your category in nursing. |
||
|
Registered Nurse |
87 |
43,5 |
|
Enrolled nurse assistant |
28 |
14,0 |
|
Nursing Student |
15 |
7,5 |
|
Nursing Managers |
3 |
1,5 |
|
Nursing specialist |
23 |
11,5 |
|
Enrolled nurse |
41 |
20,5 |
|
Nursing Educators |
2 |
1,0 |
|
3. Gender |
||
|
Female |
129 |
64,5 |
|
Male |
69 |
34,5 |
|
4. Ethnic group |
||
|
Black |
160 |
80,0 |
|
Indian |
22 |
11,0 |
|
Coloured |
9 |
4,5 |
|
White |
9 |
4,5 |
|
5. Employment status |
||
|
Permanent position |
182 |
91,0 |
|
Student |
18 |
9,0 |
|
Knowledge, perceptions, and awareness on CRC screening 1. What are the standard CRC screening tests |
||
|
Xray |
18 |
9,0 |
|
Colonoscopy |
85 |
42,5 |
|
Sonar |
11 |
5,5 |
|
Occult stool test |
16 |
8,0 |
|
don't know |
95 |
47,5 |
|
2. According to WHO protocol of colorectal cancer screening, how soon can healthy patients have a colonoscopy |
||
|
Every year |
86 |
43.5 |
|
Every second year |
51 |
25,5 |
|
Every third year |
62 |
31,0 |
|
3. When should patients with previous normal colonoscopies be screened |
||
|
Don't know |
5 |
2,5 |
|
Yearly |
99 |
49,5 |
|
After two years |
41 |
20,5 |
|
After three years |
43 |
21,5 |
|
After ten years |
4 |
2,0 |
|
Six months |
8 |
4,0 |
|
Measuring the availability of oncology-related training or educational programme Have you received a Continuous? Professional Development (CPD) in the last six months |
||
|
No |
187 |
93,5 |
|
Yes |
13 |
6,5 |
|
Measurements on knowledge Knowledge, perceptions and awareness of CRC diagnoses 1. The necessity to know about the risk factors of colorectal cancer |
||
|
Disease Prevention |
93 |
46,5 |
|
Health Education |
63 |
31,5 |
|
Health Promotion |
27 |
13,5 |
|
Early Detection |
16 |
8,0 |
|
Measurement of nurse’s perceptions, knowledge and awareness of CRC risk factors |
||
|
What are the risks of colorectal cancer |
||
|
Excessive alcohol consumption |
103 |
51,5 |
|
Smoking |
33 |
16,5 |
|
Obesity |
16 |
8,0 |
|
Positive history of polyps |
19 |
9,5 |
|
High red meat consumption |
69 |
34,5 |
|
Sedentary lifestyle |
21 |
10,5 |
|
High fatty diet |
68 |
34,0 |
|
All of them |
86 |
43,0 |
|
Should a person with a medical history of polyps worry about |
|
|
|
colorectal cancer |
81 |
40,5 |
|
Do you think you are at risk of colorectal cancer |
19 |
9,5 |
|
As a nurse what impact your interest in doing colorectal cancers screening |
||
|
Fear that I might have it |
97 |
48,5 |
|
The belief that cancer is not existing |
42 |
21,0 |
|
My religion or spirituality does not allow me to screen for cancer |
11 |
,5 |
|
Traditional treatment is the only way to manage or treat cancer according to my culture |
77 |
38,5 |
Table 1: Overall Frequency Distribution Table of the Study.
|
Variables intervals |
Crude odds ratios N |
95% confidence |
Adjusted Odds ratios |
95% confidence intervals % |
|
|
e intervals % |
N |
|
|
|
Category in nursing |
||||
|
Registered Nurse |
10.85 |
5.13 - 22.67 |
72.63 |
20.24 – 260.61 |
|
Enrolled nurse |
2.75 |
1.26 - 5.88 |
5.03 |
1.54 - 16.39 |
|
Nursing Student |
0.93 |
0.7 1- 1.21 |
3.24 |
1.44 - 7.29 |
|
Nursing Managers |
1.58 |
0.72 - 3.46 |
1.40 |
0.50 - 3.90 |
|
Nursing specialist |
0.24 |
0.10 - 0.55 |
3.71 |
1.02 - 13.43 |
|
Enrolled nurse assistant |
1.76 |
1.36 - 2.27 |
4.70 |
2.88 - 7.67 |
|
Nursing Educators |
Reference |
|
Reference |
|
|
Workdivision |
||||
|
Medical unit |
2.46 |
1.65 - 3.68 |
3.11 |
1.67 - 5.79 |
|
Emergency department |
2.27 |
1.45 - 3.56 |
10.18 |
4.78 - 21.86 |
|
Surgicalunit |
1,010 |
,874 - 1,168 |
1,050 |
,894 - 1,233 |
|
ICU |
7.34 |
4.87 - 11.0 6 |
11.11 |
4.08-16.14 |
|
Gynae |
Reference |
|
Reference |
|
|
Theatre |
3.12 |
1.97 - 4.93 |
4.76 |
2.48 - 9 - 14 |
|
Maternityunit |
1.43 |
0.96 - 2.13 |
1.02 |
0.55 - 1.89 |
|
Paediatricsunit |
Reference |
|
Reference |
|
|
Gender |
||||
|
Female |
32.40 |
15.15–69.30 |
20.23 |
6.25 – 65.50 |
|
Male |
Reference |
|
Reference |
|
|
Ethical group |
||||
|
Black |
3,45 |
2.39-4.97 |
7.99 |
2.80 - 22.80 |
|
Indian |
1.02 |
0.70-1.49 |
2.41 |
0.96 - 6.04 |
|
White |
0.73 |
0.44-1.19 |
0.64 |
0.28 - 1.42 |
|
Coloured |
Reference |
|
|
|
|
Employmentstatus |
||||
|
Permanent |
7.22 |
4.90–10.63 |
10.26 |
5.52 – 19.07 |
|
Student |
Reference |
|
|
|
Table 2: Crude and Adjusted Odds ratios for Nurses' Demographic Characteristic with Oncology
Registered nurses as a category was statistically significant at 95% CI using the nursing manager/Educators group as references even after adjusting for demographic characteristics. The odds of oncology CPD for participants in Enrolled nursing and Registered nursing were 5.0 and 72.6 times higher respectively than the odds for participants in the Nursing Educators group. The ICU unit was statistically significant at 95% CI (AOR: 11.11, 95% CI 4.08- 16.14) with the Gynecology unit used as the reference group. This means that the odds of receiving oncology CPD in ICU participants were 11.1 times higher than the odds of receiving oncology CPD in Gynecology unit participants. Regarding gender, being a female nurse was statistically significant at 95% CI (AOR: 20.23,95% CI 6.25 – 65.50).
The results of the logistic regression analysis showed that except for the category in nursing, the odds of female participants receiving oncology CPD were 20.2 times higher than the odds of receiving oncology CPD in male nurses. In the Ethnic group, the black group was statistically significant at 95% CI (AOR:7.99, 95% CI 2.80-22.80), all other groups were statistically significant at 95% CI and used the group as a reference Colored group of nurses, odds for Black nurse who receiving oncology CPD was 8.0 higher than others. Being a permanently employed nurse was statistically significant at 95% CI (AOR: 20.23,95% CI 6.25 – 65.50), meaning the odds of student nurse participants receiving oncology CPD were 20.2 times higher than the odds of receiving oncology CPD in student nurses.
|
As a nurse what impacts your interest in doing colorectal cancer screening? |
Crude odds ratios |
95% confidenc e intervals |
Adjuste d Odds ratios |
95% confidence intervals |
|
Fear that I might have it Yes |
2,202 |
0,641- 7,565 |
2,602 |
0,54 - 12,368 |
|
No |
Reference |
|
|
Reference |
|
The belief that cancer is not existing Yes |
1,067 |
0,547 - 2,083 |
2,019 |
0,418 - 9,754 |
|
No |
Reference |
|
|
Reference |
|
Traditional treatment is the only way to manage or Treat cancer according to my culture Yes |
0,823 |
0,591 - 1,145 |
1,229 |
0,277 -- 5,451 |
|
No |
Reference |
|
|
Reference |
Table 3: Crude and Adjusted Odds Ratios Measuring Fear, Cultural, Spiritual, and Religious Beliefs as Influential Factors for CRC Screening Amongst Nurses in Private Hospital an in Sandton
The findings on the impact of colorectal cancer screening reveal an increased likelihood of harboring apprehension about its potential presence. The statistical analysis indicates a significant correlation between the perception that cancer is non-existent and fear of its occurrence, with a 95% confidence interval (AOR:2.602, 95%CI 0.547-12.368). Numerous nurses share this belief, along with other notions regarding the absence of cancer.
Summary and Transition
This chapter presents a meticulous examination and interpretation of the research findings in light of the research questions and objectives. The collected data underwent thorough scrutiny to discern patterns, trends, and relationships. In the following chapter, an analysis will provide valuable insights into the significance of these results in addressing the research aims while also highlighting any limitations encountered during this study. Furthermore, suggestions for future research will be discussed to further advance knowledge in this field. This comprehensive understanding of the research findings is crucial for their proper interpretation and contributes significantly to knowledge advancement within this domain.
Discussion
To investigate Nurses' Perception and Knowledge Levels About Screening, Diagnoses, and Risk Factors of Colorectal Cancer Amongst Nurses Working in Private Hospital a in Sandton
As elucidated in the literature review, a qualitative investigation was conducted in South Africa to delve into healthcare professionals' viewpoints on the burden and screening of colorectal cancer. The research disclosed multiple hindrances to CRC screening, encompassing but not limited to the absence of a nationwide screening scheme, inadequate medical insurance coverage, far- flung health facilities, deficient health infrastructure, unfavorable attitudes towards screenings, invasive procedures and inadequacy among service providers and untrained healthcare personnel [6]. The findings from this current study buttress the notion that there exists insufficient awareness about CRC screening and diagnoses as previously mentioned in Magwaza's study et al.(2021) When evaluating nurses' perceptions, knowledge, and awareness of colorectal cancer screening, diagnosis, and risk factors across various work divisions, it was foundthat 42responses (or 21.0% of total responses) were received from the ICU unit - a significant number compared to other units which only had 31 responses.
Amongst these work divisions, registered nurses accounted for the highest frequency and percentage with a tally of 87(equivalent to 43.5%). This demographic finding highlights that the majority of respondents in this survey occupy positions where they are expected to possess essential information on patient screening procedures, diagnoses and risk factors as well as disease management. However, this study discovered that a substantial portion of these nurses lacked knowledge about standard colorectal cancer (CRC) screening tests recommended by WHO guidelines. Specifically speaking; many were unaware of the optimal frequency for colonoscopy or how occult blood tests should be used. The absence of oncology-related CPDs in this research was linked with inadequate understanding among nurses regarding CRC diagnoses and screening protocols. Registered Nurses play an essential role in diagnosing patients accurately; failure to comprehend symptoms related to colorectal cancer can endanger lives or prolonged hospital stays unnecessarily [14]. Hashemi et al.'s studies emphasised that at secondary care levels; nurse roles should include genetic counseling along with testing stool samples via sigmoidoscopy or colonoscopy while also conducting biopsies followed by screening test follow-ups chemotherapy interventions if necessary- whereas their tertiary level duties would involve pre-and post-operative care aimed at preventing further complications alongside rehabilitation & palliative care measures. Therefore, it is imperative that Registered Nurses receive comprehensive training in Oncology so they can cater holistically to their patients' needs effectively. Targeted strategies need implementation immediately addressing disparities within continuing professional development opportunities available equitably amongst all nursing staff members alike.
To Assess if there are Oncology Related Continuous Professional Development (Cpd) For Crc Screening Diagnoses and Risk Factor Awareness at Private Hospital a in Sandton South Africa
The results of this study indicate that a mere 6.5% of nurses received continued professional development (CPD) in the field of oncology, while a staggering 93.5% did not receive any CPD in the past six months. These findings suggest a significant knowledge gap among nurses with regards to colorectal cancer screening, as evidenced by their lack of awareness about standard screening tests and misconceptions about colonoscopy frequency. Shockingly, almost half (47.5%) were unaware of the recommended CRC screening test, with only8%selecting an occult blood test over colonoscopy (42%). When asked about WHO protocol for colorectal cancer screening intervals, only 10% correctly mentioned repeating colonoscopy after ten years if previous results are normal; instead, many believed it should be done annually or every three years. These low levels of knowledge about colorectal cancer screening underscore the need for stool- based tests to be prioritized as they are more convenient and non- invasive than other options like colonoscopy which may not be accessible or affordable in developing countries where resources may be scarce. Nurses must know that testing occult stool is the main recommended method for detecting early-stage 56 cancers or precancerous polyps according to WHO guidelines.
The absence of oncology education programs is undoubtedly linked with poor awareness and understanding around these issues - making them all the more critical moving forward. Regarding the quantification of the correlation between oncology-related CPD and nurses' perception, knowledge, and awareness of colorectal cancer diagnoses, this study's findings do not refute the null hypothesis. An overwhelming 97.2%of nurses expressed positivity towards learning about colorectal cancer risk factors, whileonlyamere 2.8% failed to acknowledge its necessity. When asked about their interest in understanding CRC risk factors, roughly 46.5% cited disease prevention as a primary motivator, whereas only 8.0% mentioned early detection as an incentive. In Terms of their knowledge regarding the risk factors associated with CRC, approximately 43.0% believed that all risk factors contributed to colorectal cancer development; however, merely 51.5% acknowledged excessive alcohol consumption as a contributing factor well. As per Kim et al.'s (2022) literature review on the health belief model perceived benefits (positive attributes of behavior), participants are more likely to modify their conduct by avoiding CRC risk factors if they recognize that doing so will benefit the mind some way or another.
To Determine the Factors that Can Influence Nurses ' Perceptions About Colorectal Cancer Screening, Diagnoses, and Risk Factors
As previously discussed in the literature review, Written and others (2020) emphasized that fear of cancer was linked to varying screening rates across different studies. In This Study, respondents' apprehension towards developing colorectal cancer had significant statistical association at 95% CI (AOR: 2.602, 95%CI 0.547 -12.368). The Absence of oncology education programs and CPD was identified as an underlying factor contributing to the fear surrounding CRC screenings. Specific barriers such as lack of knowledge about the disease were also noted to impact screening decisions; thus, intensive efforts on awareness campaigns will be necessary to overcome these obstacles [15].
Strength
Although many nurses are willing to learn about colorectal cancer screening, diagnoses, and risk factors, the outcome of this study revealed that there are no or very limited oncology training programs in one of the private hospitals in Sandton. While such findings cannot conclude that all hospitals are the same, it can at least prompt other researchers to research more about perceptions, awareness, and attitudes among nurses and healthcare workers about all major cancer screenings, diagnoses, and risk factors, as well as their treatment. More hypotheses can be generated from this study's study’s findings.
Limitation
This study has some potential limitations as it was only conducted with nurses working in one of the private hospitals in Sandton. Therefore, without empirical data, the result of the study cannot be generalized and completed for all nurses. Due to the nature of the study methodology (descriptive cross-sectional study) and skewed data, this study cannot be used to determine cause-effect relationships. Using an online survey might have limited choice as respondents were mostly provided with predefined.
Implications to Public Health
The current campaign by the WHO seeks to address the global issue of cancer and implement strategies aimed at reducing its impact. The WHO's approach involves creating awareness about cancer, prevention measures, strengthening detection and early diagnosis procedures, promoting health, building capacity in healthcare systems, conducting research and evaluations as well as coordinating collaborations between stakeholders. The vision of the WHO is to reduce cancer incidence globally while controlling it by promoting primary prevention methods such as early screening and diagnosis coupled with access to quality control and integrated management. Achieving these goals would not be possible without nurses being aware of new information related to colorectal cancer diagnosis, prognoses, and risk factors. Physicians play a crucial role in healthcare promotion through education early detection while nurses are equally important in executing this task. It is essential that nurses have an understanding of these areas; failure to do so can lead to significant consequences for patients' wellbeing such as:
• Delayed or missed screenings: Nurses may not effectively promote colorectal cancer screening to patients, resulting in missed opportunities for early detection and intervention.
• Limited patient education: Patients rely on nurses for accurate information about colorectal cancer signs, symptoms, and risk factors. Poor nurse knowledge may result in inadequate patient education, leading to missed symptoms or delayed seeking of medical attention.
• Reduced adherence to screening guidelines: Patients may be less likely to follow colorectal cancer screening guidelines if they are not properly informed and encouraged by healthcare professionals like nurses.
• Increased disease burden: Delayed diagnosis and treatment can lead to more advanced stages of colorectal cancer, resulting in poorer outcomes and increased healthcare costs. Government, and health stakeholders are urged to address these knowledge gaps among nurses through targeted education and training programs that can help improve public health outcomes by facilitating early detection, promoting adherence to screening guidelines, and ultimately reducing the burden of colorectal cancer.
Conclusion
The findings of this investigation suggest that deficient knowledge and awareness regarding colorectal cancer (CRC) screening and diagnoses may be linked to lack of oncology-related continuing professional development (CPD) training. Although respondents generally lacked familiarity with CRC screening, risk factor management, and awareness, they recognized the importance of oncology-related professional development in shaping their attitudes toward cancer. Since nursing staff members are primarily responsible for providing comprehensive patient care and play an instrumental role in non-communicable disease screening and treatment at community 59 health centers, it is crucial for them to educate patients about all diseases that contribute to high morbidity and mortality rates. Accurate implementation of primary prevention measures for non-communicable diseases requires assessment and supervision of nursing staff's attitudes, awareness levels, as well as perceptions towards cancer. Therefore, nurses must be equipped with relevant information covering context such as fear or cultural/religious/spiritual beliefs since these factors often influence cancer detection rates [16]. As Silva & Santos (2021) stated in their research studies better health literacy being associated with more positive attitudes towards disease prevention strategies; similarly, oncology-related health education/training can improve nurses' knowledge base while enhancing their overall attitudes/perceptions/awareness around colorectal or other forms of cancers-ultimately leading to lower morbidity/mortality rates among patients.
Recommendations
• Training and Education: government and educational institutions to advocate for comprehensive training programs and educational materials specifically tailored to CRC screening, including the importance of early detection and various screening methods available. Government to integrate cancer nursing education within all stages of nursing education. And to provide regular updates and refresher courses to ensure nurses stay informed about advancements in CRC screening guidelines and technologies.
• Promotion of colorectal cancer Awareness: Health institutions to increase awareness campaigns within healthcare facilities to emphasize the significance of CRC screening and dispel common myths or misconceptions.
• Clinical Practice Guidelines: Ensure nurses have easy access to and are familiar with evidence-based clinical practice guidelines for CRC screening, risk factors and its treatment modalities.
• Interdisciplinary Collaboration: Motivation to foster collaboration between nurses, physicians, and other healthcare professionals to create a multidisciplinary approach to CRC screening, diagnosis and management by facilitating knowledge exchange and best practices implementation.
• Utilization of Technology and media: Integrate technology solutions such as electronic health records (EHRs) and decision support tools to streamline CRC screening processes and provide real-time guidance to nurses. Use of media to spread awareness about colorectal cancer screening, risks and factors. one of the Nigerian studies, the use of film-based multimedia health education was effective and efficient in raising awareness and changing patients' perceptions and attitudes towards cervical cancer. These strategies can be applied to nurses and other healthcare professionals. Health media professionals should consider using various media methods to positively influence public perceptions, awareness, and attitudes toward cancer.
• Quality Improvement Initiatives: stakeholders and government to implement quality improvement initiatives to assess and address barriers to CRC screening implementation within healthcare settings, ensuring that systems are in place support nurses in delivering optimal care. By implementing these recommendations, healthcare organizations can enhance nurses' knowledge levels and perceptions of CRC screening, ultimately leading to improved patient outcomes and increased screening uptake.
• Several studies indicated that there is lesser oncology research output in Africa, therefore, more research on cancer screening, diagnosis, and management is recommended. Government and Healthcare stakeholders to encourage research on cancer screening, diagnosis, and management in under-researched regions like Africa.
• Nurses should also take the initiative in spreading awareness and supporting existing cancer health campaigns.
• Advocate for Policy Changes: Advocate for policy changes that support cancer screening and early detection, such as expanding access to screening services and raising awareness among underserved communities.
Institutional Review Board Statement: The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) University of Johannesburg (protocol code REC: -2025-2023) and (date of approval:1 August 2023).
Informed Consent Statement: Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Acknowledgments
I would like to express my sincere gratitude to the following people and organizations for their invaluable support and help in completing this research project: First, I would like to thank my supervisors, Dr. P. Mapungwana and Dr Martha Chadyiwa, for their guidance, support, and encouragement throughout the research process. Their ideas and comments significantly contributed to the direction and scope of this study. I would also like to thank the research committee members, Professor Nisha Naicker (REC), for their valuable comments and constructive criticism that helped me refine and improve the quality of this research. I wFinally, I would like to express my gratitude to the University of Johannesburg for allowing me to enroll in a Master of Public Health and for providing me with the resources to carry out this research. Thank you, everyone, for your invaluable contribution to this project.
References
- de Martel, C., Georges, D., Bray, F., Ferlay, J., & Clifford, G.M. (2020). Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. The Lancet global health, 8(2), e180-e190.
- Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre,L. A., & Jemal, A. (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians, 68(6), 394-424.
- Motsuku, L., Chen, W. C., Muchengeti, M. M., Naidoo, M., Quene, T. M., Kellett, P., ... & Singh, E. (2021). Colorectal cancer incidence and mortality trends by sex and population group in South Africa: 2002–2014. BMC cancer, 21, 1-11.
- Mattiuzzi, C., & Lippi, G. (2019). Current cancer epidemiology.Journal of epidemiology and global health, 9(4), 217-222.
- WHO International Agency for Research on Cancer. Estimated number of deaths in 2020, all cancers, sexes, a n d ages. Cancer today. Published 2020. Accessed January 14, 2022.
- Magwaza, S., Van Hal, G., & Hoque, M. (2021). Service providers and researchers perceptions on colorectal cancer burden and screening programme in South Africa: a qualitative study. Journal of community medicine & health education, 11(8), 1-13.
- Augustus, G. J., & Ellis, N. A. (2018). Colorectal cancer disparity in African Americans: risk factors and carcinogenic mechanisms. The American journal of pathology, 188(2), 291-303.
- Akduran, F., &Cinar, N. (2015). Effects of nursing education on awareness of risk factors for colorectal cancer. Asian Pacific Journal of Cancer Prevention, 16(14), 5763-5766.
- Andsoy, I. I., & Gul, A. (2014). Breast, cervix and colorectal cancer knowledge among nurses in Turkey. Asian Pacific Journal of Cancer Prevention, 15(5), 2267-2272.
- Vrinten, C., Waller, J., Von Wagner, C., & Wardle, J. (2015). Cancer fear: facilitator and deterrent to participation in colorectal cancer screening. Cancer Epidemiology, Biomarkers & Prevention, 24(2), 400-405.
- Muthukrishnan, M., Arnold, L. D., & James, A. S. (2019). Patients' self-reported barriers to colon cancer screening in federally qualified health center settings. Preventive medicine reports, 15, 100896.
- Demyati, E. (2014). Knowledge, attitude, practice, and perceived barriers of colorectal cancer screening among family physicians in National Guard Health Affairs, Riyadh. International journal of family medicine, 2014(1), 457354.
- Aggarwal, R., & Ranganathan, P. (2019). Study designs: Part 2–descriptive studies. Perspectives in clinical research, 10(1), 34-36.
- Hashemi, N., Bahrami, M., Tabesh, E., &Arbon, P. (2022). Nurse’s roles in colorectal cancer prevention: a narrative review. Journal of Prevention, 43(6), 759-782.
- Al-Hajeili, M., Abdulwassi, H. K., Alshadadi, F., Alqurashi, L., Idriss, M., &Halawani, L. (2019). Assessing knowledge on preventive colorectal cancer screening in Saudi Arabia: A cross-sectional study. Journal of family medicine and primary care, 8(10), 3140-3146.
- Aga, S. S., Khan, M. A., Alsulimani, E. F., Fallatah, M. A., Alquzi, A. S., Alzahrani, R. A., & Binyamin, M. T. (2021). Knowledge & Awareness regarding colorectal cancer among health and allied students of King Saud Bin Abdulaziz University for Health Sciences, Jeddah. Journal of family medicine and primary care, 10(6), 2284-2292.
- Adom, D., Hussein, E. K., &Agyem, J. A. (2018). Theoretical and conceptual framework: Mandatory ingredients of a quality research. International journal of scientific research, 7(1), 438-441.
- Akanle, O., Ademuson, A. O., & Shittu, O. S. (2020). Scope and limitation of study in social research. Contemporary issues in social research, 105, 114.
- Al-Azri, M. H. (2016). Delay in cancer diagnosis: causes and possible solutions. Oman Medical Journal, 31(5), 325.
- Al-Azri, M., Al-Saadi, W. I., Al-Harrasi, A., &Panchatcharam,S. M. (2019). Knowledge of cancer risk factors, symptoms, and barriers to seeking medical help among Omani adolescents. Asian Pacific journal of cancer prevention: APJCP, 20(12), 3655.
- Alregaibah, R. A., Almogbel, Y. S., &Alhowail, A. H. (2021). Associations of healthcare providers' awareness, perception, and knowledge of chemotherapy-induced cognitive impairment and their intentions to provide information about it to patients. European Review for Medical & Pharmacological Sciences, 25(21).
- Akanle, O., Ademuson, A. O., & Shittu, O. S. (2020). Scope and limitation of study in social research. Contemporary issues in social research, 105, 114.
- Akram, M., Iqbal, M., Daniyal, M., & Khan, A. U. (2017). Awareness and current knowledge of breast cancer. Biological research, 50, 1-23.
- Almadi, M. A., Mosli, M. H., Bohlega, M. S., Al Essa, M.A., AlDohan, M. S., Alabdallatif, T. A., ... &Mandil, A. (2015). Effect of public knowledge, attitudes, and behavior on willingness to undergo colorectal cancer screening using the health belief model. Saudi journal of gastroenterology, 21(2), 71-77.
- Althobaiti, A., &Jradi, H. (2019). Knowledge, attitude, and perceived barriers regarding colorectal cancer screening practices and risk factors among medical students in Saudi Arabia. BMC medical education, 19, 1-8.
- Astin, M., Griffin, T., Neal, R. D., Rose, P., & Hamilton,W. (2011). The diagnostic value of symptoms for colorectal cancer in primary care: a systematic review. British Journal of General Practice, 61(586), e231-e243.
- Bishop, D. J., Granata, C., &Eynon, N. (2014). Can we optimise the exercise training prescription to maximise improvements in mitochondria function and content?. Biochimica et Biophysica Acta (BBA)-General Subjects, 1840(4), 1266-1275.
- Boskey E. (2022). WhatIs theHealth Belief M o d e l ? Behavioural Psychology.
- Busolo, D. S., & Woodgate, R. L. (2015). Cancer prevention in Africa: a review of the literature. Global health promotion, 22(2), 31-39.
- Duangchan, C., Steffen, A., & Matthews, A. K. (2021). Perspectives and practices regarding colorectal cancer survivorship care: Online survey results from oncology nurses in Thailand. European Journal of Oncology Nursing, 55, 102048.
- Eldredge, J. D., Weagel, E. F., &Kroth, P. J. (2014). Defining and identifying members of a research study population: CTSA-affiliated faculty members. Hypothesis: the Newsletter of the Research Section of MLA, 26(1), 5.
- Elshami, M., Elshami, A., Alshorbassi, N., Alkhatib, M., Ismail, I., Abu-Nemer, K., ... &Bottcher, B. (2020). Knowledge level of cancer symptoms and risk factors in the Gaza Strip: a cross-sectional study. BMC Public Health, 20, 1-11.
- Elshami, M., Ayyad, M., Alser, M., Al-Slaibi, I., Ahmed Naji, S., Mohamad, B. M., ... &Bottcher, B. (2022). Awareness of colorectal cancer signs and symptoms: a national cross- sectional study from Palestine. BMC public health, 22(1), 866.
- Eldredge, J. D., Weagel, E. F., &Kroth, P. J. (2014). Defining and identifying members of a research study population: CTSA-affiliated faculty members. Hypothesis: the Newsletter of the Research Section of MLA, 26(1), 5.
- Elshami, M., Bottcher, B., Alkhatib, M., Ismail, I., Abu-Nemer, K., Hana, M., ... &Elshami, A. (2021). Perceived barriers to seeking cancer care in the Gaza Strip: a cross-sectional study. BMC Health Services Research, 21, 1-10.
- Fetters, M. D., Curry, L. A., & Creswell, J. W. (2013). Achieving integration in mixed methods designs—principles and practices. Health services research, 48(6pt2), 2134-2156.
- Ferlay, J., Colombet, M., Soerjomataram, I., Parkin, D. M., Piñeros, M., Znaor, A., & Bray, F. (2021). Cancer statistics for the year 2020: An overview. International journal of cancer, 149(4), 778-789.
- Garg, R. (2016). Methodology for research I. Indian journal of anaesthesia, 60(9), 640-645.
- Glanz, K., & Bishop, D. B. (2010). The role of behavioral science theory in development and implementation of public health interventions. Annual review of public health, 31(1), 399-418.
- Glied, S., Wittenberg, R., & Israeli, A. (2018). Research in government and academia: the case of health policy. Israel journal of health policy research, 7, 1-8.
- Goldvaser, H., Milman, Y., Dujovni, T., Stern, A., Mahamid, M., Hanovich, E., ... &Shepshelovich, D. (2016). Perception of prognosis of cancer patients by nonâ?oncologists. International Journal of Clinical Practice, 70(12), 1027-1032.
- Hann, K. E., Freeman, M., Fraser, L., Waller, J., Sanderson,S. C., Rahman, B., ... & PROMISE Study Team. (2017). Awareness, knowledge, perceptions, and attitudes towards genetic testing for cancer risk among ethnic minority groups: a systematic review. BMC public health, 17, 1-30.
- Helmenstine,AnneMarie,Ph.D.(2020). WhatIs a Hypothesis?
- Hedenstrom, M. L., Sneha, S., Nalla, A., & Wilson, B. (2021). Nursing student perceptions and attitudes toward patients with cancer after education and mentoring: integrative review. JMIR cancer, 7(3), e27854.
- In, J. (2017). Introduction of a pilot study. Korean journal of anesthesiology, 70(6), 601.
- Islami, F., Ward, E. M., Sung, H., Cronin, K. A., Tangka, F. K., Sherman, R. L., ... &Benard, V. B. (2021). Annual report to the nation on the status of cancer, part 1: national cancer statistics. JNCI: Journal of the National Cancer Institute, 113(12), 1648-1669.
- Muliira, J. K., Melba, S. D., Ahmed, S. M., Al-Dhahli, S. N., & Al-Jahwari, F. R. (2016). Barriers to colorectal cancer screening in primary care settings: attitudes and knowledge of nurses and physicians. Asia-pacific journal of oncology nursing, 3(1), 98-107.
- Zeigler-Hill, V., & Shackelford, T. K. (Eds.). (2020). Encyclopedia of personality and individual differences. Cham: Springer International Publishing.
- Kayamba, V., Mutale, W., Cassell, H., Heimburger, D. C., & Shu, X. O. (2021). Systematic review of cancer research output from Africa, with Zambia as an example. JCO global oncology, 7, 802-810.
- Kim, H. Y., Shin, S. H., & Lee, E. H. (2022). Effects of health belief, knowledge, and attitude toward COVID-19 on prevention behavior in health college students. International Journal of Environmental Research and Public Health, 19(3), 1898.
- Leyva, B., Nguyen, A. B., Allen, J. D., Taplin, S. H., & Moser,R. P. (2015). Is religiosity associated with cancer screening? Results from a national survey. Journal of Religion and Health, 54(3), 998-1013.
- Limburg, P. J., Ahlquist, D. A., Johnson, S., Jayasekar Zurn, S., Kisiel, J. B., & Smith, R. A. (2022). Multicancer early detection: International summit to Clarify the Roadmap. Cancer, 128, 859-860.
- Mubin, N., Bin Abdul Baten, R., Jahan, S., Zohora, F. T., Chowdhury, N. M., &Faruque, G. M. (2021). Cancer related knowledge, attitude, and practice among community health care providers and health assistants in rural Bangladesh. BMC health services research, 21, 1-11.
- Mukherjee, M., & Roy, S. (2017). Feasibility studies and important aspect of project management. International Journal of Advanced Engineering and Management, 2(4), 98- 100.
- Rababah, M. H., Alhassan, M. A., & Al-Motlaq, M. A. (2018). Knowledge of colorectal cancer screening guidelines and perceptions of barriers among nursing and medical students in a Jordanian university. Int J Cancer Research, 14(02), 70-76
- Maheri, M., Rezapour, B., &Didarloo, A. (2022). Predictors of colorectal cancer screening intention based on the integrated theory of planned behavior among the average-risk individuals. BMC Public Health, 22(1), 1800.
- Arulogun, O. S., & Maxwell, O. O. (2012). Perception and utilization of cervical cancer screening services among female nurses in University College Hospital, Ibadan, Nigeria. Pan African Medical Journal, 11(1).
- Fernández-Ortega, P., Cabrera-Jaime, S., & Estrada- Masllorens, J. M. (2016). The oncology nurse prescribing: a Catalonian survey. Asia-Pacific Journal of Oncology Nursing, 3(1), 108-114.
- Polit, D. F., & Beck, C. T. (2008). Nursing research: Generating and assessing evidence for nursing practice. Lippincott Williams & Wilkins.
- Sawicki, T., Ruszkowska, M., Danielewicz, A., Niedźwiedzka, E., ArÅ?ukowicz, T., &PrzybyÅ?owicz, K. E. (2021). A review of colorectal cancer in terms of epidemiology, risk factors, development, symptoms and diagnosis. Cancers, 13(9), 2025.
- Ploukou, S., Birtsou, C., Gavana, M., Tsakiridou, K., Dandoulakis, M., Symintiridou, D., ... &Smyrnakis, E. (2023). General Practitioners’ attitudes and beliefs on barriers to colorectal cancer screening: A qualitative study. Population Medicine, 5(March), 1-8.
- Rim, S. H., Zittleman, L., Westfall, J. M., Overholser, L., Froshaug, D., & Coughlin, S. S. (2009). Knowledge, attitudes, beliefs, and personal practices regarding colorectal cancer screening among health care professionals in rural Colorado: a pilot survey. The Journal of Rural Health, 25(3), 303-308.
- Tamminga, S. J., De Boer, A. G. E. M., Verbeek, J. H. A. M., & Frings-Dresen, M. H. W. (2010). Return-to-work interventions integrated into cancer care: a systematic review. Occupational and environmental medicine, 67(9), 639-648.
- Rejeski, W. J., & Fanning, J. (2019). Models and theories of health behavior and clinical interventions in aging: a contemporary, integrative approach. Clinical interventions in aging, 1007-1019.
- Sung, H., Ferlay, J., Siegel, R. L., Laversanne, M., Soerjomataram, I., Jemal, A., & Bray, F. (2021). Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians, 71(3), 209-249.
- Uygun, A., Caliskan, N. D., &Tezcan, S. (2023). Community pharmacists’ knowledge on cancer and screening methods. Journal of Oncology Pharmacy Practice, 29(2), 386-392.
- Wettergren, L., Eriksson, L. E., Nilsson, J., Jervaeus, A., &Lampic, C. (2016). Online focus group discussion is a valid and feasible mode when investigating sensitive topics among young persons with a cancer experience. JMIR Research Protocols, 5(2), e5616.
- Wintersberger, D., & Saunders, M. (2020). Formulating and clarifying the research topic: insights and a guide for the production management research community. Production, 30, e20200059.
- Woolley, M., & Propst, S. M. (2005). Public attitudes and perceptions about health-related research. JAMA, 294(11), 1380-1384.
- Balekouzou, A., Yin, P., Pamatika, C. M., Nambei, S. W., Djeintote, M., Doromandji, E., ... &Koffi, B. (2016). Assessment of Breast Cancer Knowledge among Health Workers in Bangui, Central African Republic a Cross- sectional study. Asian Pacific Journal of Cancer Prevention, 17(8), 3769-3776.