
Archives of Clinical and Medical Microbiology(ACMMJ)
ISSN: 2835-9968 | DOI: 10.33140/ACMMJ
Impact Factor: 1.0

Research Article - (2024) Volume 3, Issue 1
Knowledge of Pregnant Women Regarding Premature Birth at the Intermediate Hospital Antenatal Care Clinic in Namibia: A Quantitative Study
2MNSc School of Nursing and Public Health, Faculty of Health Sciences and Veterinary, Medicine, University of Namibia, Namibia
Received Date: Jan 10, 2024 / Accepted Date: Feb 12, 2024 / Published Date: Feb 26, 2024
Copyright: ©Â©2024 Joseph Galukeni Kadhila, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Shikongo, E. K., Nuumbosho, H. T., Kadhila, J. G. (2024). Knowledge of Pregnant Women Regarding Premature Birth at the Intermediate Hospital Antenatal Care Clinic in Namibia: A Quantitative Study. Archives Clin Med Microbiolo, 3(1), 01-07.
Abstract
Background: The knowledge and information awareness among expectant mothers on the conditions that have adverse outcomes on the pregnancy is crucial. A body of knowledge exist on the knowledge about preterm births among obstetricians, patients, couples, midwives, clinical officers and community health care workers. However, no study exists that assess pregnant women knowledge on the premature births.
Methods: The study adopted a quantitative descriptive design. A probability simple random sampling method was used to select the participants. Data collection took place at the study antenatal care clinic. Fifty-five participated in the study and completed the questionnaire in front of the researcher. Competence was based on 50% because, data was collected on the participants of whom some may not have any educational or medical background. Descriptive statistics was used to analyse the data.
Results: The study found n= 49 (89%) participants knowledge competent about pre-term births by obtaining a knowledge score of above 50%.
Conclusion: Therefore this, study can conclude that the expectant mother attending antenatal care at Katutura Intermediate hospital have good knowledge about the causes, risks factors, prevention and management of preterm births.
Keywords
Preterm Birth, Prematurity, Knowledge, Neonatal Morbidity, Mortality.
Introduction
A normal full-term pregnancy usually lasts from 38 to 42 weeks, whilst labour that begins before the completed 37 weeks of pregnancy is considered as preterm labour [1]. Globally preterm birth is now the second leading cause of neonatal death after pneumonia [2]. Preterm birth is actually the leading cause of newborn deaths in their first four weeks of life [3]. A global research by Liu et al. (2015), revealed that about two fifths of deaths in children younger than five years occurred in the first 28 days of their life. This indicates the crucial importance of addressing the problem of preterm birth [2]. Countries need to realize one of the Sustainable Development Goal (SDG) which aimed at reducing neonatal mortality by 12/ 1000 per live births by 2030 which will also reduce child mortality rate (United Nations International Children's Emergency Fund. According to WHO (2013), preterm birth is one of the leading causes of infant morbidity and the leading cause of infant mortality in Namibia [3]. It accounts for >70% of neonatal deaths and almost half of long-term neurological disabilities. The Centres for Disease Control and Prevention (CDC) in USA is collaborating with state health departments, universities, communities, and healthcare providers to understand why preterm births occur and how to address preterm birth risk factors.
According to 2010 statistics on preterm birth, Namibia reported 14.4% preterm births and it is ranked among the top six African countries with high prevalence of preterm birth [4]. In Windhoek preterm birth rate rose from 8.9% in 2012 to 11.1% in 2014 [5]. Evidenced based statistics collected from the Ministry of Health and Social Service at Katutura state hospital shows that in 2019 from January to December, a total number of 149 premature births were recorded. In 2020 a total number of 388 were documented. In 2021, 546 preterm births were recorded which shows a massive increase in premature births at Katutura State hospital in Windhoek, Namibia.
Aim of the Study
The aim of the study was to investigate the knowledge of pregnant women regarding premature birth at Katutura State Hospital ANC in Namibia.
Methods
The proposed study design for this study was a quantitative descriptive design. Quantitative research is conducted to define new events, scrutinize relationships among variables and conclude the success of treatments [6]. A descriptive design was used to identify problems with the current practice, make judgments or determine what others in similar situations are doing. The accessible population in this study included all pregnant women of child bearing age 15-49 years. About 450 pregnant women are attending ANC at Katutura State Hospital antenatal clinic. The researcher used probability simple random sampling method, for fair selection of participants. A structured self-administered validated questionnaire in English with four sections A to D was developed based on the study objectives to obtain information about regarding preterm births among pregnant women attending ANC at Katutura state hospital in Namibia.
Ethical Approval
Ethical clearance was obtained through the structures of the University of Namibia SoN 106/2022. Therefore, the following ethical considerations were written, informed consent was obtained from each participant after the procedure was explained and risks were pointed out after adequate information were conveyed, possible risks were pointed out. Voluntary participation without penalty for withdrawal was pointed out.
Data Collection
At first the researcher requested for permission from the unit manager of Katutura state hospital maternity ward as well as the Midwife in-charge of ANC. The participants were informed about the research project and were required to complete a consent from prior to partaking in the study. Data were collected at Antenatal Clinic on both first visit dates and follow up dates in the morning hours from 08H00-10H00. Participants completed the questionnaire at Katutura ANC in the presence of the researcher as knowledge on premature births was tested.
Data Analysis
In this study descriptive statistical analysis strategy whereby the variables were identified, and the interval and ratio data of each variable were described by using frequency distribution, and the data were presented in a table or a chart form. The supervisor assisted in analysing the data.
Results
Demographical Data
This section comprised of five biographical questions of the participants n=55. The data presented in this section are; age, gender, level of education, occupation and religion.
Age
The mean age of the participants was 29, The youngest participant was 15 years and the oldest pregnant women were 38 years of age. Figure 4.1 shows the participants’ age.
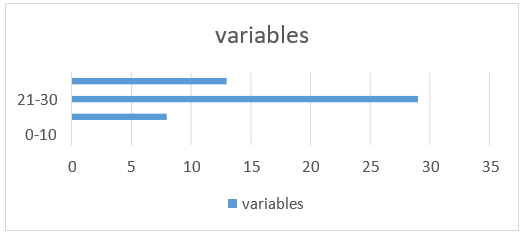
Figure: 1 Age=55
Marital Status
Marital status plays a major role during pregnancy for all women. The study evaluated the impact of maternal marital status among pregnant women attending ANC at KSH and investigated these women with or without marital ties at the point of pregnancy journey invited to participate in this study. Among 55 participants, n=39 (71%) =single, n=12 (22%) =married and n=4 (7%) = other. The pie chart below will demonstrate the frequency value.
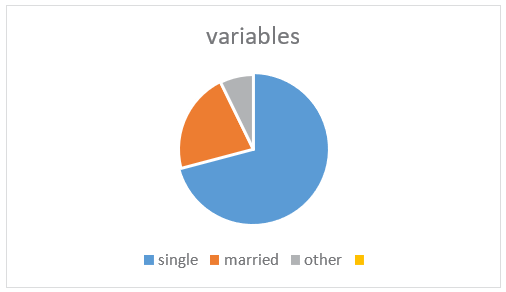
Figure: 2 Marital Status
Level of Education
Mother's education is linked to an appreciable risk of preterm births across the whole world. The risk of preterm births associated with low maternal education is therefore assessed in this questionnaire in regards to the knowledge of pregnant women regarding preterm birth at Katutura State Hospital ANC. Among the 55 pregnant women assessed, no formal education= 0, primary education= 8 (15%), secondary education= 31 (56%) and tertiary education=16 (29%).
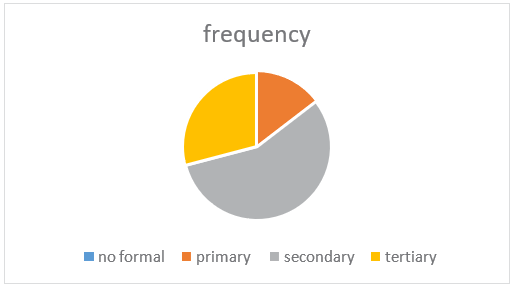
Figure: 3 Level of Education
Occupation Status
Research considering underlying differences in occupational to explain disparities in risk for preterm births and has largely not considered nativity. Thus, the hypothesized that occupational exposure is related to preterm delivery and that the odds ratios may be higher among pregnant women with effects potentially further modified according to nativity. Among the assessed 55 pregnant women indicated; employed=15 (27%), unemployed=25 (46%) and self-employed=15 (%27) as illustrated in the pie chart below.
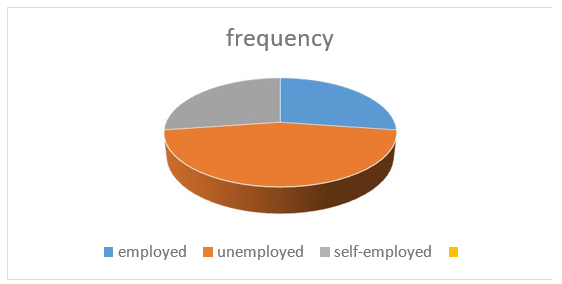
Figure: 4 Occupation Status
• Section B
Section B focused on questions pertaining causes and risk factors of premature births. This aimed to achieve an objective on finding out if these pregnant women attending ANC at Katutura State Hospital have knowledge regarding preterm births. Among 55 women on whom the research was conducted, n=49 (89%) indicated that they are aware of what is preterm birth and n=6 (11%) of them have never heard of it. On the other hand, n=26 (47%) pregnant women indicated that they have been informed about the signs and symptoms of preterm birth but n=29 (53%) did not. Regarding the questions pertaining the causes and risk factors of preterm births, the competence pass rate was 50% because the research was done on patients whom may not have any medical background. The questions were marked and categorised in percentages. The findings were as follows; less than n=6 (50%), 60%= 8, 70%= 11, 80%=13, 90%= 8 and 100%=9 and illustrated in a graph below.
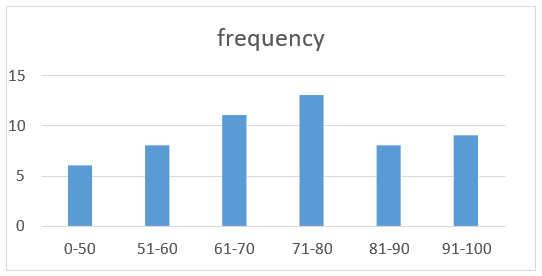
Figure: 5 Causes and Risk Factors in Frequency
|
Causes & risk factors of preterm birth related questions Correct n (%) Incorrect n (&) Total n (%) |
||
|
a) Woman with high blood pressure is at risk |
n=43 (78%) n=12(22%) |
n=55(100%) |
|
b) Twin pregnancy increases the risks |
n=39(71%) n=16(29%) |
n=55(100%) |
|
c) Vaginal infections can cause preterm births |
n=50(91%) n=5(9%) |
n=55(100%) |
|
d) Preterm labour can be re-current |
n=47(85%) n=8(15%) |
n=55(100%) |
|
e) Alcohol abuse is a risk factor |
n=48(87%) n=7(13%) |
n=55(100%) |
|
f) Smoking is not a risk factor |
n=55(100%) n=0(0%) |
n=55(100%) |
|
g) Fetal abnormalities can cause preterm birth |
n=35(64%) n=20(36%) |
n=55(100%) |
|
h) Women with good nutrition are at risk |
n=48(87%) n=7(13%) |
n=55(100%) |
|
i) Primigravida are at risk of preterm birth |
n=43(78%) n=12(22%) |
n=55(100%) |
|
j) Pregnant womam who falls accidentally |
n=49(89%) n=6(11%) |
n=55(100%) |
|
are at risk |
|
|
Table B: Overall Mean Score of Section B Questions
• Section C
This section focused on questions pertaining the prevention of preterm birth. Patients were asked to choose between true and false questions to assess their knowledge regarding prevention of preterm births. Questions were marked and categorised in percentages as per answer chosen by the patients as follows: less than 50% =4, 60%= 5, 70%= 18, 80%=20, 90%=0 and 100%= 8.
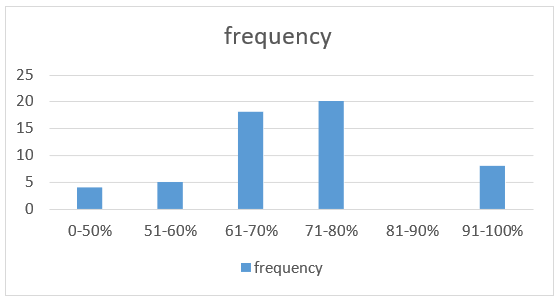
Figure: 6 Preventative Measures of Preterm Labour
|
Prevention of preterm labour related questions |
Correct n (%) Incorrect n (%) Total n(%) |
||
|
a) Avoid alcohol abuse |
n=54 (98%) |
n=1 (2%) |
n=55 (100%) |
|
b) No need to stop smoking when pregnant |
n=50 (91%) |
n=5 (9%) |
n= 55(100%) |
|
c) Attending ANC to rule out the risks |
n=37 (67%) |
n=18 (33%) |
n= 55(100%) |
|
d) Healthy amount of weight |
n=20 (36%) |
n= 35 (64%) |
n=55 (100%) |
|
e) DM and HPT is not necessary |
n=27 (49%) |
n= 28 (51%) |
n=55 (100%) |
|
f) Reporting GBV cases to reduce trauma |
n= 49 (89%) |
n=6 (11%) |
n= 55(100%) |
|
g) Eating sweets can prevent |
n= 47 (85%) |
n=8 (15%) |
n= 55 (100%) |
|
h) Using protection during coitus |
n=49 (89%) |
n=6 (11%) |
n= 55(100%) |
|
i) Treatment of uterine myomas is not |
n= 25 (45%) |
n=30 (55%) |
n=55 (100%) |
|
Necessary |
|
|
|
Table C: Overall Mean Score of Section C
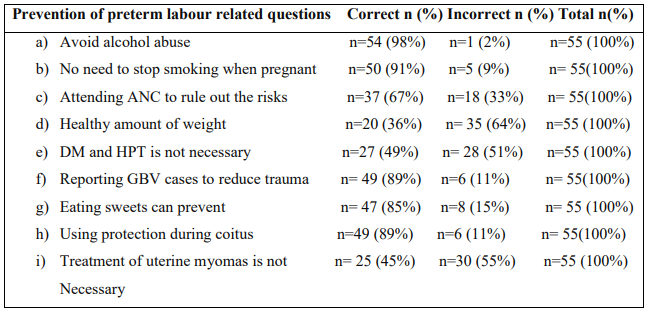
Table C: Overall Mean Score of Section C
• Section D
Section D aimed at assessing the knowledge of pregnant women regarding management of preterm birth either at home or hospital. The objective was to choose between true and false, the correct answers were mixed with wrong to avoid patients to guess the answer instead of expressing their knowledge.The answers were marked and categorised in percentages, the passing rate was >50. The results are as follows: less than 50%= 12, 60%= 9, 70%= 11, 80%= 12, 90%=0 and 100%= 11.
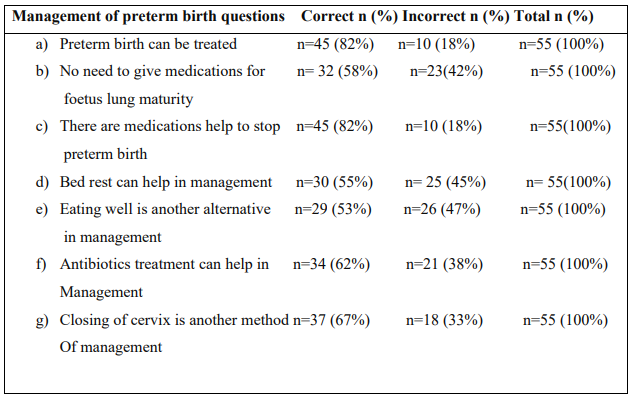
Table D: Overall Mean Score of Section D
Conclusion
The results indicated that the researcher successfully explored the research question which was: What is the knowledge regarding premature birth among pregnant women attending (ANC) at Katutura state hospitals in Namibia? The result indicates that 87% of the pregnant women were found to have knowledge regarding the causes and risk factors, prevention and management of preterm birth.
Discussion
Determine Associations Between the Biographical Data and the Knowledge Scores of Pregnant Women Regarding Preterm Birth.
Age of the Participants
The results reveal that among the 55 participants, the youngest participant was 15 years of age and the oldest were two participants who are 38 years old. Age is one of obstetric risk factors associated with preterm birth. The average age of first-born child has been considerably increased and this increase is most commonly seen in women around 35 - 39 years in comparison to mothers between 20 - 35 years’ adolescent mothers and mothers more than 35 years have shown a greater risk for preterm birth, teenage and older mothers are reported to have a higher degree of preterm birth.
Marital Status
Regarding marital status, the results shows that among the 55 participants, n=39 (71%) were single, n=12 (22%) were married and n=4 (7%) fell on category of other. The study shows that unmarried mothers have lack of social emotional support and hence they receive less antenatal care, poor nutrition and they have more complications during pregnancy that lead to preterm delivery. In relation to marital status, the study reveals that it is the single women who are more represented 71% followed by married women with 22% and it was important that marital status of the participants was investigated.
Level of Education
The risk of preterm births associated with low maternal education is therefore assessed in this questionnaire in regards to the knowledge of pregnant women regarding preterm birth at Katutura State Hospital ANC. Among the 55 participants assessed, no formal education scored= 0, primary education indicates n=8 (15%), secondary education indicates n= 31(56%) and tertiary education indicates n=16 (29%).
Occupation Status
Among the assessed 55 pregnant women indicated; employed=15 (27%), unemployed=25 (46%) and self-employed=15 (27%). No found literature related to the relationship between occupation and preterm labour.
Objective 1: To Determine if Pregnant Women have Knowledge Regarding the Causes and Risk Factors of Preterm Birth.
The results of the study indicate that the overall knowledge mean score about the assessment of patients for causes and risk factors (the passing percentage is 50%) with 90% and failing percentage was 10%.The passing score (90%) positively indicates that the mothers attending ANC at KSH have knowledge regarding the causes and risk factors of preterm birth.
Objective 2: To Determine Whether the Pregnant Women Attending ANC at Katutura State Hospital have Knowledge Regarding Prevention of Preterm Birth.
The results indicate a positive feedback that n=51 (92%) obtained an overall mean score knowledge score of more than 50%, as shown in paragraph 4.5. Further results also indicate that the participants had little knowledge in prevention methods of preterm birth n=4 (7%) by obtaining an overall knowledge mean score below 50%.
Objective 3: To Determine if the Pregnant Women Attending ANC at Katutura State Hospital have Knowledge Regarding Management of Preterm Birth Either at Home or Hospital.
The results indicate that n=43 (78%) obtained a knowledge score of more than 50%, as shown in paragraph 4.5. Further results also indicate that the participants had insufficient knowledge regarding management of preterm labour by obtaining an overall knowledge mean score of n=12(22%), which was below 50%.
Conclusion
Namibia is challenged with high preterm birth rates caused by premature labour nearly. The study found that 87% of participants assessed regarding causes and risk factors, prevention and management of preterm birth with a passing rate of more than 50%. Thus, this study concludes that despite 87% knowledge assessed, increased preterm birth rates are on the rise every year at Katutura state hospital in Namibia. Therefore, the MoHSS must put in place the multiple recommended measures to ensure that all pregnant women are equipped with the necessary knowledge about preterm labour [7-12].
Limitation to the Study
The study was conducted at antenatal clinic of Katutura State Hospitals in Namibia yet, many women attending ANC at other hospitals also required to have adequate preterm birth knowledge during pregnancy. The results from this study are limited to Katutura State Hospital in Namibia only. Patients were enrolled from a single medical centre; thus the results cannot be generalized based on a small population.
Acknowledgements
The authors would like to acknowledge the pregnant mothers from the State hospital.
Consent to Publish
Not applicable
Funding
None
Availability of Data Materials
The data base is available on request from the corresponding author.
Competing Interest
The authors declared no conflict of interest.
References
- Alexander, L. L., LaRosa, J. H., Bader, H., & Garfield,S. (2020). New dimensions in women's health. Jones & Bartlett Learning.
- Liu, L., Oza, S., Hogan, D., Perin, J., Rudan, I., Lawn, J. E., ... & Black, R. E. (2015). Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. The lancet, 385(9966), 430-440.
- World Health Organisation. (2013). Preterm birth fact sheet.
- Kinney, M. V., Lawn, J. E., Howson, C. P., & Belizan,J. (2012). 15 Million preterm births annually: what has changed this year?. Reproductive health, 9(1), 1-4.
- Namibia Ministry of Health and Social Services (MoHSS), & ICF International. (2014). The Namibia demographic and health survey 2013.
- Grove, S. K., & Gray, J. R. (2018). Understanding nursing research e-book: Building an evidence-based practice.Elsevier health sciences.
- Dean, S. V., Mason, E. M., Howson, C. P., Lassi, Z. S., Imam, A. M., & Bhutta, Z. A. (2013). Born too soon: care before and between pregnancy to prevent preterm births: from evidence to action. Reproductive health, 10(1), 1-16.
- Grove, S. K., Burns, N., & Gray, J. (2012). The practice of nursing research: Appraisal, synthesis, and generation of evidence. Elsevier Health Sciences.
- Annamma, J. (2012). A comprehensive textbook of midwifery and gynaecological nursing. Edisi ke, 3.
- Ministry of Health and Social Services, (2016). District Health Information System database. MOHSS, Namibia.
- Rubens, C. E., Sadovsky, Y., Muglia, L., Gravett, M. G., Lackritz, E., & Gravett, C. (2014). Prevention of preterm birth: harnessing science to address the global epidemic. Science translational medicine, 6(262), 262sr5-262sr5.
- Sættem, B. (2015). Preterm Labour in Malawi. Prevention, treatment, complications. A literature study.