
Journal of Traditional Medicine & Applications(JTMA)
ISSN: 2833-1389 | DOI: 10.33140/JTMA
Impact Factor: 1.02



Research Article - (2024) Volume 3, Issue 2
Knowledge, Attitude and Utilization of Traditional Medicine among the Communities of Arerti Town, Semen Showa Zone, Amhara Regional State, South East Ethiopia
2Department of Health, Rift Valley University, Addis Ababa, Ethiopia
Received Date: Sep 06, 2024 / Accepted Date: Sep 30, 2024 / Published Date: Oct 14, 2024
Copyright: ©Â©2024 Gossa Tassew Zeleke, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Zeleke, G. T., Negera, T. T. (2024). Knowledge, Attitude and Utilization of Traditional Medicine among the Communities of Arerti Town, Semen Showa Zone, Amhara Regional State, South East Ethiopia. J Traditional Med Applications, 3(2), 01-11.
Abstract
At different places various findings emphasize the need for further studies of the impact of multiple healthcare resources and treatments, as well as illicit drugs, on clinical outcome, chronic care and patient retention. Mostly Traditional Medicine (TM) is ignored in the research and contributions of modern drugs advancement. This study aimed at assessing the knowledge, attitude and factors affecting the utilization of traditional medicine among the communities of Arerti town, Semen Showa Zone, Amhara Regional State, and South East Ethiopia. A simple random sampling technique was used to select the study area and systematic random sampling technique was used to select households. A structured closed ended questionnaire was used to collect data through house to house interview among 490 participants identified for the study. The data was entered by using Epi-Data version 3.1 and analyzed using statistical package for social science (SPSS) version 25.The studies revealed four hundred and sixty-seven (97.3%) have heard about traditional medicine, while three hundred eighty (80%) of them have used traditional medicine in their life time. Study participant’s educational group of primary and secondary school were 0.230 and 0.317 times less likely utilize traditional medicine as compared to uneducated groups respectively. (AOR 0.230, 95% CI, (0.093, 0.569) and 0.317, 95% CI, (0.121, 0.833). Of the respondents age category 38-47, 48-57 and 58 and above years old were 0.246, 0.317 and 0.204 times less likely utilize traditional medicine than respondents of age 8-27 years.
Keywords
Traditional Medicine, Knowledge, Attitude, Utilization, Arerti Town, Ethiopia
Abbreviations
AOR: Adjusted Odd Ratio
EHCS: Ethiopian health Care System
MM: Modern Medicine
RVU: Rift Valley University
TM: Traditional Medicine
WHO: World Health Organization
Introduction
World health organization (WHO) defines traditional medicine(TM) as a health practice, approaches, and knowledge and beliefs incorporating plant, animal and mineral based medicines, spiritual, manual techniques and exercises, applied singularly or in combination to treat, diagnose and prevent illness and maintain well-being [1]. It is widely accepted and used in prevention a nd treatments of physical and mental disorder due to its intrinsic qualities, unique and holistic approaches as well as its accessibility [2]. WHO estimates that in many developed countries 70-80% of the population had used some form of alternative or complementary medicine including, homeopathic, naturopathic, traditional oriental and native American Indian medicine [3]. The wide spread use of traditional medicine has resulted in traditional health care becoming a lucrative, multinational business. Billions of United States dollars are spent annually on traditional medicine in many developed countries. For example, in 2012, 32 billion dollars were spent in the United States of America on dietary supplements, an amount expected to increase to 60 billion dollars in 20219 [4]. The WHO estimates that the global market of traditional medicine is approximately US$ 83 billion annually [5]. In China for example, traditional herbal preparation account for 30 to 50% of the total medicine consumption.
In Africa 80%of the population use traditional medicine as a primary health care (PHC). Many Africans, especially those in the rural areas rely on traditional medicine not only for their medicine value and promotion of good health and fortune but also their spiritual well-being [6]. The practice of traditional medicine in Africa is a method of healing founded on its own concept of indigenous knowledge systems that developed over a long period of time with in varies societies [2]. About 80% of Ethiopian people rely on traditional medicine to meet their health care needs which could be attributed to cultural acceptability, perceived efficacy against certain types of diseases, physical accessibility, and affordability as compared to modern medicine [7]. Studies have showed that Ethiopians use TM due to lack of access to modern health care facilities [8]. But the current Ethiopian health care system (EHCS) is PHC focused onto take appropriate controlling measures regarding the quality, safety and awareness of the practices. Since there is informal/illegal use of the TMs by many people, by knowing the awareness and practice of the community the study will help the government and the stakeholders to make it legal or cooperate with modern medicine (MM). The study will also provide the baseline data for researchers for further investigations. This improves Access to MM in a better way. But, both rural and urban populations continue to use TM. Even though it ignored in the national health system TM plays an important role in Ethiopian society, knowledge about the extent and characteristics of traditional healing practices and practitioners is limited. Based on the above situations the study focused mainly on identifying the knowledge, attitude, and utilization of TM through cross-sectional study in the communities of Arerti town, Amhara regional state, south east Ethiopia.
Methods
Study Design
A community based cross sectional study design was adopted to assess the knowledge, attitude and factors that affect the utilization of traditional medicine among the communities of Arerti town, Semen Showa zone, Amhara regional state.
Study Area
Minjar Shenkora is one of 28th Wereda in Semen Showa Zone, Amhara Regional state and its local government area is Arerti town. According to unpublished Arerti town municipality 2020 report, the total populations of the town were 53,870 (male 25,835, female 28,035). It has an area of 125km2 and has 135 kilo meters from kaliti, Addis Ababa.
Study Population
The study populations consisted of all men and women households who were 18 years and above and have been resident in the community in the year 2021.
Sampling Methods and Sample Size Calculation
Multistage sampling technique with simple random sampling was used to select the source and study population. Systematic random sampling and convenience sampling technique was used to select the households and study subjects respectively. Sample size was calculated based on the prevalence of knowledge, attitude and utilization of TM, based on the following assumption. p=73.8% prevalence of TM user in Jara Town, Bale Zone South East Ethiopia, Confidence level of 95%, margin of error (d) of 5%, and using the formula for estimation of single population proportion and adding anon response rate of 10% [9].
n= (za/2 )2p (1-p)/d2 n= minimum sample size requires for the study
Z= standard normal distribution (z=1.96) with confidence interval of 95% and (alpha=0.05)
P=prevalence of TM users
d=absolute precision or tolerable margin of error.
n= (1.96)2 0.738*0.262/ (0.05)2
n=297
Taking the design effect of 1.5 and adding 10%for non-response rate, the final sample size was 490.
Variables
The outcome variable/dependent variable of the study was utilization of traditional medicine, while the explanatory variable variables were Sex, age, marital status, ethnicity, religion, monthly income, educational status, and occupation, Social-structure-availability of traditional medicine in the market, Knowledge and attitude.
Operational Definitions
• Good (Positive) Attitude: any persons support the improvement of traditional medicine by integrating and solving the existing problem [10].
• Good Knowledge: Respondents who can answer 50+1 from questions related to knowledge [10].
• Traditional Medicine Users: those respondents who have used traditional medicine at least ones in the last 2 years [11].
• Traditional Healer (Practitioner): Someone who is recog¬nized by the community in which he lives as competent to provide health care by using vegetables, animal and mineral substances and certain other methods based on the social, cul¬tural and religious backgrounds [12].
Data Collection Technique and Data Quality Management
Before data collection, training was given for two days, for community leaders to support and disseminate information about the purpose of study to get real data and for data collector, on data collection technique, how to ask the questionnaire and for supervisors to control of day to day activities and to receive complete fill questionnaire. Pre-test was given in Arerti town Kebele5 for 5% of the total sample size to check clarity, completeness, consistency and length of the study before starting the data collection. Based on the findings obtained during the pre-testing of questionnaires, data collection tools were modified and immediate update also takes place. In addition, questions that posed difficulty or lack clarity was rephrase and correct to minimize errors during data processing. Principal investigator and supervisors during data collection, every day complete questionnaires were review and check for completeness and consistency. All the necessary feedback gives for all data collectors the next morning before the actual procedure.
Data Management and Analysis Plan
Data Management
During data collection, the principal investigator (PI) and supervisors was review and check the complete questionnaires in hard copy before data entry in to epidemiological information package (Epi-Info) version 3.1 and then exported to statistical package for social science (SPSS) version 25 for data analysis. At the time of data analysis cross-checking the soft copy of the questionnaire to ensure consistency. Finally, the data was clean thoroughly and double entered before analysis.
Data Analysis
The data was processed by using frequency, percentage, mean and standard deviation to analyses the data. Binary and multiple logistic regression analyses were applied to assess association between utilization of TM and the independent variables. Independent variables having p-value less than 0.3 in the bivariate logistic regression analysis were entered in to multivariable logistic regression analysis in order to control confounding effects. P-values of 0.05 and 95% confidence interval for adjusted odds ratio (AOR) can also be used to report statistical significance in the final model.
Ethical Clearance
The study was approved by the Ethical clearance committee of rift valley university institute of public health. A letter of support obtains from Arerti health offices and submits to Kebele1, 2, 3 and 5 communities ‘leaders. Inform that study participants were participated voluntarily and they have freedom to with draw at any time even during being interviewed. Confidentiality was assured by omitting personal identifiers, instead using codes during data collection, data analysis and reporting. Privacy during interviews can be maintained by conducting interviews at site free from any form of disturbance. Filled questionnaire were kept in private locked cabinets, easily access to for data processing purposes.
Results
Socio-Demographic and Economic Characteristics of Respondents
A total of 490 study participants were approved during this study, and data gathered from 475 respondents via face-to-face interviews with a structured questionnaire. Out of fifteen who were not interviewed, all are refusal to participate. The response rate for this study was 96.9% which keeps with the study’s assumption of a10% non-response rate. Two hundred thirty-two (48.8%) of the respondents are males while 243(51.2%) are females. Regarding the age of respondents 170(35.8%), 119(25.1%) 115(24.2%) 42(8.8%) and 29(6.1%) were aged between 18-27years, 28-37years, 38-47years, 48-57years and 58 and above years respectively. The mean age (±SD) of study participants were 35.24(±12.937). Majority of the respondents 249(52.4%) were married. Concerning respondents’ ethnic group 447(94.1%) were Amhara, 15(3.2%) were Oromo, 4(0.8%) were Tigre, 3(0.6%) were gurage and the rest 6(1.3%) were others. Of the respondents of the study 409(86.1%) were Orthodox, 39(8.2%) were Muslims, 25(5.32%) were protestants and 2(0.4%) of them were others. Large number of respondents 175(36.8%) have attended higher education, while 85(17.9%) were attended secondary school, 97(20.4%) were attended primary school and 118(24.8%) were illiterates. Of the study participants 88(18.5%) were unemployed, 51(10.7%) were self-employed and 138(29.1%) earned less than or equal to500 birr.
|
Variable |
Frequency |
Percentage |
|
Sex |
||
|
Male |
232 |
48.8 |
|
Female |
243 |
51.2 |
|
Age |
||
|
18-27 |
170 |
35.8 |
|
28-37 |
119 |
25.1 |
|
38-47 |
115 |
24.2 |
|
48-57 |
42 |
8.8 |
|
>=58 |
29 |
6.1 |
|
Marital status |
||
|
Single |
178 |
37.5 |
|
Married |
249 |
52.4 |
|
Widowed |
20 |
4.2 |
|
Divorced |
28 |
5.9 |
|
Ethnicity |
||
|
Amhara |
447 |
94.1 |
|
Oromo |
15 |
3.2 |
|
Tigre |
4 |
0.8 |
|
Gurage |
3 |
0.6 |
|
Other |
6 |
1.3 |
|
Religion |
||
|
Orthodox |
409 |
86.1 |
|
Muslim |
39 |
8.2 |
|
Protestant |
25 |
5.3 |
|
Others |
2 |
0.4 |
|
Occupation |
||
|
Unemployed |
88 |
18.5 |
|
Housewife |
63 |
13.3 |
|
Daily laborer |
58 |
12.2 |
|
Self employed |
51 |
10.7 |
|
Government employed |
85 |
17.9 |
|
Merchant |
54 |
11.4 |
|
Others |
76 |
16 |
|
Monthly Income |
||
|
0-500 |
138 |
29.1 |
|
501-1500 |
75 |
15.8 |
|
1501-2500 |
76 |
16 |
|
2501-3500 |
50 |
10.5 |
|
>=3501 |
136 |
28.6 |
Table 1: Socio Demographic and Economic Variables among Households in Arerti Town, 2021(N=475)
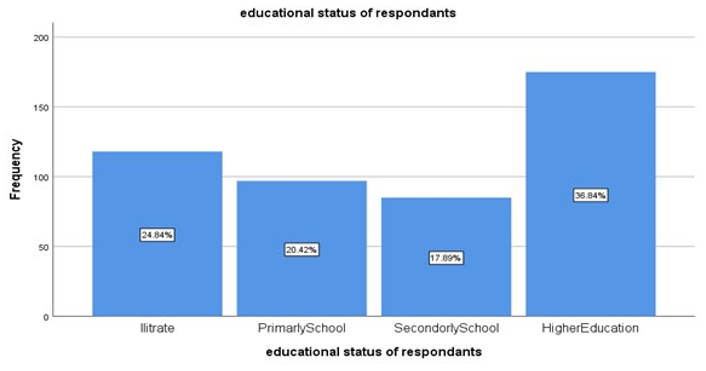
Figure 1: Educational Status of the Study Participants in Arerti Town, Semen Show Zone, Amhara Regional State, 2021
Knowledge of Traditional Medicine of Respondents
Among the respondents 467(98.3%) of them answered they have heard about traditional medicine. Regarding traditional medicine used, medicinal herbs 196 (41.3%), spiritual faith healing 118 (24.8%), bone setting146 (30.7%) and 15 (3.2%) were used others. Majority of the respondents, 398 (83.8%) were aware of the major side effects of complementary and alternative medicine, such as 164 (41.2%) diarrhea, 107 (26.9%) vomiting, 113 (28.4%) abdominal pain and 14 (3.5%) others. More than half of them had promotion on complementary and alternative medicine practice as shown in Table 2.
|
Variable |
Frequency |
Percentage |
|
Have you ever heard of TM? |
||
|
Yes |
467 |
98.3 |
|
No |
8 |
1.7 |
|
What are Forms of therapy that you know? |
|
|
|
Medical herbalist |
196 |
41.3 |
|
Spiritual/faith healing |
118 |
24.8 |
|
Traditional bone setting |
146 |
30.7 |
|
Others |
15 |
3.2 |
|
Are traditional medicines accessible with affordable cost in the community? |
||
|
Yes |
369 |
77.7 |
|
No |
54 |
11.4 |
|
I do not know |
52 |
10.9 |
|
Are Traditional medicines more effective and safer than modern health services? |
||
|
Yes |
186 |
39.2 |
|
No |
216 |
45.5 |
|
I do not know |
76 |
15.4 |
|
Is health education about risks and benefits of Traditional Medicines important? |
||
|
Yes |
395 |
83.2 |
|
No |
32 |
6.7 |
|
I do not know |
48 |
10.1 |
|
Are non-sterile Traditional Medicines harmful when given by injection? |
||
|
Yes |
382 |
80.4 |
|
No |
33 |
6.9 |
|
I do not know |
60 |
12.6 |
|
Do traditional medicines produce less adverse effect compared to Modern Medicine? |
||
|
Yes |
204 |
42.9 |
|
No |
173 |
36.4 |
|
I do not know |
98 |
20.6 |
|
Had promotional information on traditional medicine? |
||
|
Yes |
282 |
59.4 |
|
No |
193 |
40.6 |
|
What is your Source of information on traditional medicine? |
||
|
Formal |
96 |
33.9 |
|
Informal |
187 |
66.1 |
|
Do you Know harmful effects of traditional medicine? |
||
|
Yes |
398 |
83.8 |
|
No |
77 |
16.2 |
|
What harmful affects you know about traditional medicine? |
||
|
Diarrhea |
164 |
41.2 |
|
Vomiting |
107 |
26.9 |
|
Abdominal pain |
113 |
28.4 |
|
Others |
14 |
3.5 |
|
What Diseases you know which are treated by traditional medicine? |
||
|
Hemorrhoid |
141 |
29.7 |
|
Rabies |
59 |
12.4 |
|
Jaundice |
179 |
37.7 |
|
Bone fracture |
69 |
14.5 |
|
I Don’t know |
7 |
1.5 |
|
Others |
20 |
4.2 |
|
What diseases are failed to treat by TM? |
||
|
Cancer |
155 |
32.6 |
|
Malaria |
121 |
25.5 |
|
Tuberculosis |
101 |
21.3 |
|
I don’t know |
62 |
13.1 |
|
Other |
36 |
7.6 |
|
What is the problem of traditional medicine? |
||
|
Not integrate with modern medicine? |
177 |
36.6 |
|
Dosage |
156 |
32.8 |
|
No written document |
129 |
27.2 |
|
Others |
16 |
3.4 |
Table 2: Knowledge of Arerti Town House Holds Towards Traditional Medicine, Semen Showa Zone, and Amhara Regional State
Attitude of Study Participants to Complementary and Alternative Medicine Therapy (TM)
Regarding the effectiveness of traditional medicine 126 (26.5%) participants strongly disagree and 188 (39.6%) disagreed that that traditional medicine is more effective than modern medicine. More than half 238 (50.1%) of the respondents replied their disagreement that traditional medicine is safer than modern medicine. Nearly half 232 (48.8%) of the respondents agreed that complementary and alternative medicine should be integrated to modern medicine.
About 187 (39.4%) and 79 (16.6%)of the respondents disagreed and strongly disagreed about their first preference of visiting complementary and alternative medicine practitioner consecutively than modern medicine practitioners. Nearly half 215 (45.3%) of participants disagreed that to recommend visiting complementary and alternative medicine practitioners than first than modern medicine. A total of 223 (46.9%) of the study population agreed that complementary and alternative medicine is cheaper than modern medicine (Table3).
|
Items |
Strongly Disagree (%) |
Disagree (%) |
Neutral (%) |
Agree (%) |
Strongly Agree (%) |
|
Traditional medicine is more effective than modern medicine. |
126(26.5%) |
188(39.6%) |
42(8.8%) |
99(20.8%) |
20(4.2%) |
|
Traditional medicine is safer than modern medicine. |
100(21.1%) |
238(50.1%) |
36(7.6%) |
80(16.8%) |
21(4.4%) |
|
Traditional medicine should be integrated to modern medicine. |
38(8%) |
50(10.5%) |
45(9.5%) |
232(48.8%) |
110(23.2%) |
|
Prefer first to visit traditional medicine practitioner than modern medicine. |
79(16.6%) |
187(39.4%) |
51(10.7%) |
128(26.9%) |
30(6.3%) |
|
Recommend a sick person first to visit traditional medicine practitioner. |
77(16.2%) |
215(45.3%) |
46(9.7%) |
109(22.9%) |
28(5.9%) |
|
Complementary and alternative medicine is more affordable than modern medicine. |
44(9.3%) |
64(13.5%) |
49(10.3%) |
223(46.9%) |
95(20%) |
Table 3: Attitude of the Respondents towards Traditional Medicine in Arerti Town, Semen Showa Zone, Amhara Regional State, 2021
Utilization of Traditional Medicine among Study Partici-pants
Majority of study participants 380 (80%) had used TM in the last 2 years and the remaining 95 (20%) did not use TM which is shown in figure 2 bellow. Traditional medicine was most commonly given to every one 55 (11.6%) elderly, 144 (30.3%) adult, 211 (44.4%) children, 30 (6.3%) pregnant women,6(1.3%) for others and the remaining 29 (6.1%) did not for whom TM was most commonly given as shown in Table4.Majorty of the respondents 349 (71.6%) were disagreed about traditional medicine is given with combination of modern medicine. Mostly traditional medicine was used to treat headache with a frequency of more than two times a year.

Figure 2: Percentage Distribution of Study Participants on Utilization of Traditional Medicine in Arerti Town, Semen Showa Zone, Amhara Regional State, 2021
|
Variable |
Frequency |
Percentage |
|
Used TM in the last two years |
||
|
Yes |
380 |
80 |
|
No |
95 |
20 |
|
Adverse effect of TM |
||
|
Yes |
165 |
34.7 |
|
No |
310 |
65.3 |
|
For whom TM is most commonly given? |
||
|
Elderly |
55 |
11.6 |
|
Adults |
144 |
30.3 |
|
Children |
211 |
44.4 |
|
Pregnant women |
30 |
6.3 |
|
I don’t know |
29 |
6.1 |
|
Others |
6 |
1.3 |
|
Combines medication given in traditional system with MM |
||
|
Yes |
340 |
71.6 |
|
No |
135 |
28.4 |
Table 4: Utilization of Traditional Medicine among Households in Arerti Town, Semen Showa Zone, Amhara Regional State, 2021
Factors Affecting Traditional Medicine Utilization Among Study Participants
Table 5 provides an explanation of the association of socio-demographic factors related to utilization of traditional medicine. Variables with p<0.3 in the Bivariate analysis were included in the multivariate. On multivariate logistic regression model, after adjusting other variable, only educational status, age, ethnicity and marital status were significantly associated with utilization of traditional medicine. Study participants educational group of primary and secondary school were 0.230 and 0.317 times less likely utilize traditional medicine as compared to illiterate groups respectively. (AOR 0.230, 95% CI, (0.093, 0.569) and 0.317, 95% CI, (0.121, 0.833).Of the respondents age category 38-47, 48-57 and 58 and above years old were 0.246, 0.317 and 0.204 times less likely utilize traditional medicine than respondents of age 18-27 years. (AOR0.246, 95% CI, (0.113, 0.537), 0.317, 95% CI, (0.107, 0.938), 0.204, 95% CI, (0.059, 0.705). In this result finding study participants who were married and divorced had a statistically significant association with traditional medicine users, in multi-variate analysis study participants who were married and Divorced were 2.593 and 7.785 times more likely utilize traditional medicine than singles respectively. (AOR 2.593, 95% CI, (1.351, 4.976), 7.785, 95% CI (1.471, 41.207). In multivariate analysis, four variables: sex, income, religion, and occupation were factors not related to utilization of traditional medicine.
|
Variable |
Traditional medicine utilization |
COR(95%CI) |
AOR(95%CI) |
|
|
YES (%) |
No (%) |
|||
|
Sex |
|
|
|
|
|
Male |
184(79.3) |
48(20.7) |
1.0 |
1.0 |
|
Female |
196(80.7) |
47(19.3) |
1.088(0.694,1.706) |
1.081(0.603,1.937) |
|
Age |
|
|
|
|
|
18-27 |
135(79.4) |
35(20.6) |
1.0 |
1.0 |
|
28-37 |
104(87.4) |
15(12.6) |
1.798(0.932,3.466) |
1.053(0.478,2.317) |
|
38-47 |
85(73.9) |
30(26.1) |
0.735(0.420,1.284)** |
0.246(0.113,0.537)** |
|
48-57 |
34(81) |
8(19) |
1.102(0.469,2.591) |
0.317(0.107,0.939)** |
|
58 and above |
22(75.9) |
7(24.1) |
0.815(0.322,2.061) |
0.204(0.059,0.705)** |
|
Single |
130(73) |
48(27) |
1.0 |
1.0 |
|
Married |
208(83.5) |
41(16.5) |
1.873(1.170,3.000)** |
2.593(1.351,4.976)** |
|
Widowed |
16(80) |
4(20) |
1.477(0.470,4.639) |
3.509(0.870,14.159) |
|
Divorced |
26(92.9) |
2(7.1) |
4.800(1.097,20.998)** |
7.785(1.471,41.207)** |
|
Ethnicity |
|
|
|
|
|
Amhara |
360(80.5) |
87(19.5) |
1.0 |
1.0 |
|
Oromo |
12(80) |
3(20) |
0.967(0.267,3.500) |
0.375(0.054,2.620) |
|
Tigre |
3(75) |
1(25) |
0.725(0.075,7.055) |
0.233(0.018,3.037) |
|
Gurage |
2(66.7) |
1(33.3) |
0.483(0.043,5.391) |
0.290(0.018,4.638) |
|
Others |
3(50) |
3(50) |
0.242(0.048,1.218) |
0.044(0.005,0.355)** |
|
Religion |
|
|
|
|
|
Orthodox |
323(79) |
86(21) |
1.0 |
1.0 |
|
Muslim |
35(89.7) |
4(10.3) |
2.330(0.806,6.734) |
4.175(0.855,20.383) |
|
Protestant |
20(80) |
5(20) |
1.065(0.389,2.920) |
2.181(0.580,8.198) |
|
Others |
2(100) |
0(0) |
430126428.7(.000) |
411562203.7(000) |
|
Educational status |
|
|
|
|
|
Illiterate |
102(86.4) |
16(13.6) |
1.0 |
1.0 |
|
Primary school |
83(85.6) |
14(14.4) |
0.930(0.429,2.016) |
0.546(0.223,1.333) |
|
Secondary school |
61(28.2) |
24(71.8) |
0.399(0.196,0.809)** |
0.230(0.093,0.569)** |
|
Higher education |
134(76.6) |
41(23.4) |
0.513(0.272,0.965)** |
0.317(0.121,0.833)** |
|
Occupation |
|
|
|
|
|
Unemployed |
61(71.8) |
24(28.2) |
1.0 |
1.0 |
|
Housewife |
49(77.8) |
14(22.2) |
1.238(0.579,2.650) |
0.405(0.138,1.186) |
|
Daily Laborer |
52(89.7) |
6(10.3) |
3.067(1.163,8.087)** |
1.207(0.295,4.933) |
|
Self employed |
45(88.2) |
6(11.9) |
2.654(1.000,7.040)** |
1.263(0.242,6.591) |
|
Government |
61(71.8) |
24(28.2) |
0.899(0.460,1.758) |
0.344(0.086,1.374) |
|
Merchant |
45(83.3) |
9(16.7) |
1.769(0.749,4.178) |
0.621(0.153,2.528) |
|
Others |
63(82.9)) |
13(17.1) |
1.715(0.799,3.679) |
1.020(0.374,2.781) |
|
Income |
|
|
|
|
|
0-500 |
101(73.2) |
37(26.8) |
1.0 |
1.0 |
|
501-1500 |
60(80) |
15(20) |
1.465(0.743,2.892) |
1.141(0.433,3.008) |
|
1501-2500 |
67(88.2) |
9(11.8) |
2.727(1.236,6.016)** |
2.281(0.642,8.105) |
|
2501-3500 |
42(84) |
8(16) |
1.923(0.826,4.476) |
2.756(0.618,12.302) |
|
>=3501 |
110(80.9) |
26(19.1) |
1.550(0.877,2.740) |
3.599(0.896,14.457) |
|
NB: ** p-value less than 0.05 |
||||
Table 5: Bivariate Analysis of Factors Associated With Traditional Medicine Utilization among Households in Arerti Town, Semen Showa Zone, Amhara Regional State, 2021
Discussion
This cross-sectional study explored the knowledge, attitude and utilization of traditional medicine in Arerti Town, Semen Showa Zone, Amhara Regional State, and South East Ethiopia. The prevalence of TM use was 80%. The finding of this study different from the study carried out Jara Town, Bale Zone which is 73.8%. The observed high prevalence in the present study could be due to fact that majority 310 (65.3%) believes that traditional medicine and mostly given for high population group that is children [2]. Among the traditional medicine utilizes the commonest are medicinal herbalist (41.3%) and spiritual healing (24.8%). This is lower than herbal medicine utilizes (64%) and higher than spiritual healings (2.6%) in Merawi Town. This difference might be spiritual healing more in Arerti Town due to accessibility of spiritual healing in the river nearer to Arerti town. Majority of the respondents 395 (83.2%) of our study showed interest to acquire education regarding TM. But this is less than from the study in Merawi town (90.3%). This might be higher educated people found in Arerti compared to Merawi (3.6%) [4]. In this study the participants reported that 80.4% of non-sterile preparation of traditional medicines are harmful when given by injections and the finding is inconsistent with previously reported studies done in Debre tabor town, which is 80.8% and lower than the study was done in Merawi Town, North West Ethiopia, which is 96.7%. This little difference might be due to similar study design usage [4]. In this study 42.9% of the respondents believed that TM is less adverse effects compared to modern medicine. In contrast the study conducted in Nigeria, Lagos reported that the higher proportion (79.2%) of herbal medicine users believed that herbal medicines have no adverse effects and the rest of them (20.8%) had experienced one or more adverse effects. This difference might be knowledge gap in Nigeria traditional medicine practitioners [13].
In this study, only 39.2%of all the respondents who were aware of TM believed that traditional medicine is more effective than modern medicine. This is higher than the finding of the study conducted in wayu town 23.8% and Burka Jato Kebele, West Ethiopia 26.3%, inconsistent with the study conducted in Nigeria (42%) respondents believed [11,14]. The respondents of the study conducted in wayu town, and Burka Jato Kebele, West Ethiopia fear of traditional medicine might be due to its side effects as compared to our findings. In this study, 72% of the participants had positive attitudes towards the integration of traditional medicine and modern medicine which is lower than the study done in Shopa Bultu, South east Ethiopia, 92%92). From our study participants showed significant association from age 38-47 years (AOR=0.246, 95% CI (0.113, 0.537) and from age 48-57 years (AOR=0.317, 95% CI (0.059, 0.705) regarding utilization of traditional medicine taking 18-27 years a constant. This shows that respondents of age 38-47 years 85.4% times less likely utilize TM than age 18-27 years and 68.3% of age 48-57 less likely utilize TM. Participants with educational status, higher education (AOR=0.317, 95% CI (0.121, 0.833), and secondary school (AOR=0.230, 95% CI (0.093, 0.568) showed a significance association with traditional medicine utilization taking illiterate as constant. That is the higher educational status the lower utilization of traditional medicine. But the study done in Uganda show that the higher educational status the higher utilization of traditional medicine (AOR=1.78, 95% CI (1.01-3.12).This might be cultural differences in Uganda and Ethiopia [15]. Married participants showed a significance association towards utilization of TM (AOR=2.595, 95% CI (1.301, 4.976) as similar as divorced participants (AOR=7.785 (1.471, 41.207) taking single as constant. This showed that married and divorced participants 2.595 and 7.785 times more likely utilize TM than single individuals.
Conclusion
There was high traditional medicine utilization among households in this study (80%). Marital status, age, educational status and ethnicity were associated with utilization of TM in this study. Respondents of age 38-47 years 85.4% times less likely utilize TM than age 18-27 years and 68.3% of age 48-57 less likely utilize TM. Married and divorced participants 2.595 and 7.785 times more likely utilize TM than single individuals. Despite many of the respondent’s use TM (65.3%) did not get adverse effects, 34.7% had adverse effects after traditional medicine utilization.
Ethics Approval and Consent to Participant
Ethical approval was obtained from Rift Valley University (RVU) Research Review approval committee. Then permission was secured from the Arerti Town, Semen Showa Zone health office. The confidentiality and anonymity of the respondents wase protected. Verbal informed consent and consent form was obtained to make sure their willingness.
Availability of Data and Materials
The data that support the findings of this study are available but some restrictions may apply to the availability of these data as there are some sensitive issues. However, data are available from the corresponding authors upon reasonable request.
Authors’ Contributions
Gossa Tassew Zeleke and Tefera Tezera Negera were involved in the conception, design, analysis, interpretation, report, manuscript writing, the design, analysis, interpretation and report writing. Gossa Tassew Zeleke and Tefera Tezera Negera were involved design, analysis and interpretation of the data. All authors read and approved the final manuscript.
Acknowledgment
We would like to express our deepest heartfelt thanks to Rift Valley University for allowing the conduct of this study. Our especial thanks go to staffs of Arerti Town, Semen Showa Zone health office for their permission and support, and for providing us the necessary information.
Funding
This study is part of university research project, which has been made possible by the Rift Valley University, College of Health Science. The funding body had no role in the design of the study, the collection, analysis and interpretation of the data, or writing of the manuscript. The views presented in this study are not necessarily those of the Rift Valley University.
References
- Awulachew, M. T. (2021). Hand book of common Ethiopian traditional medicinal plants: their parts and uses for human and animal treatments. Journal of Diseases and Medicinal Plants, 7(3), 48-60.
- Mohammed, A. Y., Kasso, M., & Demeke, A. (2016). Knowledge, attitude and practice of community on traditional medicine in Jara Town, Bale Zone South East Ethiopia. Sci J Public Health, 4(3), 241.
- World Health Organization. (2002). The WHO strategy for traditional medicine: Review of the global situation and strategy implementation in the Eastern Mediterranean Region.
- Wassie, S. M., Aragie, L. L., Taye, B. W., & Mekonnen, L.B. (2015). Knowledge, Attitude, and Utilization of Traditional Medicine among the Communities of Merawi Town, Northwest Ethiopia: A Cross-Sectional Study. Evidence-Based Complementary and Alternative Medicine, 2015(1), 138073.
- Bekele, D., Asfaw, Z., Petros, B., & Tekie, H. (2012). Ethnobotanical study of plants used for protection against insect bite and for the treatment of livestock health problems in rural areas of Akaki District, Eastern Shewa, Ethiopia. Topclass Journal of Herbal Medicine, 1(2), 12-24.
- Nigussie, S., Godana, A., Birhanu, A., Abdeta, T., Demeke, F., Lami, M., ... & Dessie, Y. (2022). Practice of traditional medicine and associated factors among residents in eastern Ethiopia: a community-based cross-sectional study. Frontiers in Public Health, 10, 915722.
- Johnson, R. K., Appel, L. J., Brands, M., Howard, B. V.,Lefevre, M., Lustig, R. H., ... & Wylie-Rosett, J. (2009). Dietary sugars intake and cardiovascular health: a scientific statement from the American Heart Association. Circulation, 120(11), 1011-1020.
- Issel, C. J., & Cook, R. F. (1993). A review of techniques for the serologic diagnosis of equine infectious anemia. Journal of Veterinary Diagnostic Investigation, 5(1), 137-141.
- Oo, P. N. (2019). Study on the Uses of Traditional Medicine in Rural People based on their Knowledge, Attitude and Practice for Primary Health Care in Taungout Township.
- Aragaw, T. J., Afework, D. T., & Getahun, K. A. (2020). Assessment of Knowledge, Attitude, and Utilization of Traditional Medicine among the Communities of Debre Tabor Town, Amhara Regional State, North Central Ethiopia: A Cross-Sectional Study. Evidence-Based Complementary and Alternative Medicine, 2020(1), 6565131.
- Gari, A., Yarlagadda, R., & Wolde-Mariam, M. (2015). Knowledge, attitude, practice, and management of traditional medicine among people of Burka Jato Kebele, West Ethiopia. Journal of Pharmacy and Bioallied Sciences, 7(2), 136-144.
- Shankar, R., Lavekar, G. S., Deb, S., & Sharma, B. K. (2012). Traditional healing practice and folk medicines used by Mishing community of North East India. Journal of Ayurveda and integrative medicine, 3(3), 124.
- Oreagba, I. A., Oshikoya, K. A., & Amachree, M. (2011). Herbal medicine use among urban residents in Lagos, Nigeria. BMC Complementary and Alternative medicine, 11, 1-8.
- Belachew, N., Tadesse, T., & Gube, A. A. (2017). Knowledge, attitude, and practice of complementary and alternative medicine among residents of Wayu town, Western Ethiopia. Journal of evidence-based complementary & alternative medicine, 22(4), 929-935.
- Logiel, A., Jørs, E., Akugizibwe, P., & Ahnfeldt-Mollerup,P. (2021). Prevalence and socio-economic factors affecting the use of traditional medicine among adults of Katikekile Subcounty, Moroto District, Uganda. African Health Sciences, 21(3), 1410-1417.