
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2022) Volume 7, Issue 2
Knowledge, Attitude and Practice of Prepucectomy among Medical Personnel in Omdurman Locality Obstetric and Gynecological Hospitals 2019
2Assistant Professor, Headmaster of Community Medicine Department University of Khartoum, Sudan
Received Date: Jun 20, 2022 / Accepted Date: Jun 11, 2022 / Published Date: Jul 21, 2022
Copyright: ©Saja Salah Mohamed Almahdi, et al. This is an openaccess article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Saja Salah Mohamed Almahdi, Asma Abdelaal Abdalla Osman. (2022). Knowledge, Attitude and Practice OF Prepucectomy among Medical Personnel in Omdurman Locality Obstetric and Gynecological Hospitals 2019. Int J Women's Health Care, 7(2), 104-109.
Abstract
Background: Female circumcision remains an endless public health problem in many societies and cultural groups, transcends religion, despite the concerted efforts and laws forbidding the practice. The study, aimed to assess the knowledge, attitudes and practice of prepucectomy among medical personnel.
Method: In this three obstetric and gynecological hospitals cross-sectional study, 190 medical personnel interviewed using a questionnaire containing and quantitative aspects after taking written consent. Data has been analyzed using SPSS software version 20. Uni-variate, bi-variety and multi-variety was conducted out and p-value at or <0.05 was taken as significant.
Results: The Overall, (82%) women and (17.2%) men were included. The mean age was 35 years (SD=11.5). A total of (33%) midwife, (56.2%) registrar (10.5%) obstetrician. Those who had inadequate knowledge of prepucectomy constitute (65.7%). Regarding attitude, out of 190 medical personnel (62.7%) had negative attitude toward prepucectomy. Out of 190 of participants (95%) had poor practice. There were highly significant association between practice and knowledge level (0.001), practice and attitude (0.0001), also between attitude and knowledge (0.368). Finally, there were significant correlation between practice and gender (1.957), practice and job in hospital (0.0001).
Conclusion: The researcher request from obstetric and gynecological society to conduct more research about prepucectomy(Case control, cohort study).
Introduction
Female circumcision is wildly practiced in African countries, WHO estimates that between 100 and 140 million girls and women worldwide have been subjected to one of the first three types of female genital mutilation. In Sudan, there is a very high prevalence rate of FGM ranged between (87%100%). Type is the most prevalent type in some area of Sudan including Kassel State [1]. Sauna circumcision is practiced and the Christians practice sauna circumcision at 46.2% when compared to Muslims at 14.5%. This clearly proves that the practice is a social tradition.
In accordance to that most areas in Sudan uncircumcised women were generally viewed as impure and thus un-marriageable. Given their lack of choice and the powerful influence of tradition, most women accept circumcision as necessary, and even naturally part of life, and adopt the rationales given for its existence.
Prepucectomy
It is the removal of superficial fore skin at the head of clitoris, without suture [2]. This procedure done by Sudanese consultant obstetrician by small trail done among Sudanese girls and it confirmed by histopathology for this taken part which imply it is pure skin [3].
Steps of the Prepucectomy
1. A child is psychologically prepared with a simplified explanation and reading the prayers and educates the mother healthily and religiously about this circumcision and be sure that there are no cases of hereditary bleeding in the family and the absence of congenital abnormalities of the genital organs.
2. The foreskin is numbed by a single injection of topical anesthesia with a small, simple injection. Bloating caused by anesthesia.
3. Move the foreskin back and forward until it separates any adhesions with the head of the clitoris and even show the upper end adhered to the skin of the clitoris body and this helps to cut the surface layer and the inner foreskin without cutting with anything from the head of the clitoris or the skin of the clitoris and even Do not grow the foreskin again and in case of difficulty separating The foreskin from the head of the clitoris The circumcision of the child should be postponed to an easier
4. The ancestral foreskin is pulled up from the front by peat dissection to remove it from the head of the clitoris.
Leave the peat compressed in place for 10 minutes until no bleeding occurs and then peat is remove. In case of bleeding, the wound is pressed again with peat or a stitch is placed from the cat where the bleeding is provided. The gauze can be removed after four hours. In case of bleeding at home, the wound is compressed with cotton again and consult a doctor if necessary The wound does not need any spare parts or antibiotics in terms of routine and follow the cleanliness of the wound in the following days with water, soap or water and salt. Treated physician [3].
Medical Causes
1. Membership reasons: Increase the size of the foreskin and inker length now
2. The presence of inflammation between them and the clitoris, which leads to severe sensitivity of the clitoris pain when touched.
3. Adhesion accumulation, which increases the multiplication of bacteria and infections of the urinary tract.
4. Adhesions that occur as a result of these infections, which lead to the closure of the urinary and reproductive tract, especially in children before puberty and in adulthood [3].
Sexual Reasons
1. Lack of sexual irritation due to narrow or large size of the foreskin and after the clitoris into the body.
2. The severity of sexual oestrus due to adhesions and itching and frequent preoccupation with the area and contact [3].
Psychological Reasons
Frigidity, hysteria, bedwetting, some cases of mental depression [3].
Benefits of prepucectomy
1. Go Glulam and oestrus (and means the intensity of lust and busy and excessive).
2. Prevent the unpleasant odours resulting from the accumulation of smear under the foreskin.
3. Low rate of urinary tract infections and low rate of genital tract infections [3].
Religious benefits
1 One Stabilization of God and Sunni
2. Taking into account the social and psychological aspects resulting from the absolute abandonment of FGM by fixing a healthy alternative that activates the fight against the illegal and harmful habit [2].
Knowledge
WHO Guidelines (2016) on the management of health complications from FGM/C, are useful for designing pre and in service professional training curricula for health care providers, and include the above- mentioned aspects. However, too often, FGM/C is not included in curricula on a systematic basis, and/or medicalization and the preventive role of health professional is not addressed at all building on how to resist pressures from the community, as well as communication techniques for social norm change are rare [4].
In similar study majority (91.3%) of the study participants had awareness and knowledge about ill heath effect of Female Genital Cutting/FGC [5].
In Sudanese study conducted in midwives, they were low level of awareness of types of FGM practice since only 7% identified the four types correctly [1].
Attitude
Cultural reasons were reported in studies, showing that many health¬care providers do perform FGM for non-scientific and non-health-related reasons, such as beliefs about the preference of husbands, cultural identity and beauty criteria. Most of the studies constituting this review were assessing the motivation of providers from countries where FGM is prevalent. It is therefore not surprising that despite their professional training, they would be influenced by their own cultural group’s convictions. The fact that some providers either have a positive attitude towards FGM, have undergone FGM themselves or have maintained the tradition for their daughters [Sudanese mid wife, 38-41, 46, 48] indicates that it is not always obvious to them to make a distinction between their personal beliefs and their professional obligations [6].
When we see thinking of Sudanese mid wife we found that the majority of them claimed that some forms of FGM are not harmful and some of midwifes said all types of FGM are harmful and little of them said it is useful [1].
In other study conducted in Sudanese mothers, 71.5%of them had negative attitude (encouraging). The most important reasons behind negative attitudes were related to many reasons (marriage, virginity, religious instructors, husband pleasure, cleaning, tradition, fertility297%, 27.4%, 19%, 11.4, %5.7%, 5.3%, 1.5% are respectively) and 28.5% of all the mothers participated in the study had positive attitude (discouraging). The reasons behind positive attitude among mothers regarding discouraging female circumcision were assigned t for many reasons [complication, gains, religion, affect education, dignity of women, easily uncircumcised girl get married, painful: 33, 4%, 21.9%, 16.2%, 13.3%, 9.5%, 5.7% respectively] [7].
Practice
FGM is usually practiced on girls younger than 15 years old. The reasons given to justify this custom are diverse, and mainly reflect cultural and social dimensions, including cultural ideals of beauty and “cleanliness”, and are a pivotal part of the rite of passage to adulthood [6].
The financial motivation should not be overlooked in high-income countries as well, particularly as it relates to cosmetic surgeries. In addition, any strategy aimed at ending medicalization of FGM should consider the financial aspect on the other hand; some health¬care providers are involved in the practice despite existing laws [Sudan] and choose to take the risk of being caught, since other motivations are important for them. For example, some providers admitted to discretely performing the act within the walls of the public healthcare canter where they work. In addition, “as most of the midwives and some physicians seemed to be involved in and aware of the procedures taking place”, this practice seems to be hidden or even tolerated [Sudan]. Likewise, some providers prefer to practice FGM underground, for example in their own home [6].
Methods
This was descriptive cross-sectional hospital based study, conducted in Omdurman locality which is the biggest locality in Khartoum state in Sudan, one of the largest country in Africa. Conducted in three local obstetric and gynecological hospitals from four local obstetrics and gynecological hospitals in Omdurman locality. Three hospitals selected randomly, one hospital for each province.
Sample method and sample size
Convenience sample of 157 women and 33 men working in obstetrics and gynecological hospitals invited to participate in the study. The inclusion criteria were obstetrician (consultant and specialist), registrar, midwifes during study period from (Nov 2018 – Jan 2019) in the selected hospitals. Medical personnel who refuse to participate or in their holidays were excluded from the study.
Data Collection
Using structured close ended self-administered questions about Knowledge, Attitude and Practice of prepucectomy, English version after obtained informed written consent, variables were scientific and professionalism base. Also in, consider of socioeconomic status.
Questionnaire consist of four parts; first for sociodemographic data (gender, age, marital status, job in hospitals, years of experience), knowledge (procedure of prepucectomy, possible complications, similarity with male circumcision), attitude (negative or positive and reasons behind attitude) and practice (place, man oeuvre, numbers of practices, circumstances around man oeuvre). Pretesting questionnaire was carried out to test the validity and consistency of the questionnaire, to yield out the expected results
Results
157 (82%) female, 33 (17.2%) male was included in study Table (1) with mean average of age was 35 years {11.5 SD} and mean experience years was [9.1+-12.2 SD] in three category of medical personnel; (33.3%) midwifes, (56.2%) registrar, (10.5%) obstetrician in three different hospitals
Table 1: Frequency of Knowledge, attitude and practice of prepucectomy among medical personnel in Omdurman locality obstetric and gynecological hospitals 2019, (n=190)
|
variables |
Frequency |
|
percentage |
|
Gender |
Male |
33 |
17.2% |
|
Female |
157 |
82% |
|
|
Position in hospital |
Mid wife |
63 |
33.2% |
|
registrar |
107 |
56.2% |
|
|
obestitrition |
20 |
10.5% |
|
|
Definition of prepucectomy |
Cut prepuce |
82 |
43.6% |
|
Excision of partor all of clitorios |
13 |
6.9% |
|
|
I don’t Know |
91 |
47.4% |
|
|
Possible complication of prepucectomy |
hemmorage |
17 |
16.2% |
|
infection |
17 |
16.2% |
|
|
Hemmorage and infection |
58 |
55.2% |
|
|
other |
13 |
12.4% |
|
|
Attitude toward prepucectomy |
positive |
68 |
37.8% |
|
negative |
112 |
61.7% |
Discussion
Sociodemographic results show most study participants were fe-male 82% out of (n=190), which differ from AUSTRALIAN pedi-atricians (female 48.7%), mean age of the participants [35+-11.5] years as same in Sudanese midwife study (32+_11.9) study, and mean of year experiences [9+_12.2], most study population were registrar (81.1%,), few of them were obstetrician (18.8%.), This results may be explained by the fact that female is more common in medical field in our society and in each hospital the main body are the registrars [1].
Regarding knowledge and it is measurements the population aware about prepucectomy (52.1%), it is lower in compare to re-sponse of mothers in ombada province in Sudan (100%) and low- er than aware in Ethiopian mothers (91.3%), in my opinion these differences are because it is a new form of female circumcision and the obestitrition who practice it is not popular and died and re¬sponse in define it correctly was very good (43.6%) like response of Sudanese mid wife in eastern Sudan just (7%), also Australian pediatricians (22%) know WHO FGM types also Flemish midwife (68.8%) have not informed about FGM, when we see the possibil¬ity of prepucectomy complication (yes: 54.8%), then which is the common prepucectomy hemorrhage and infection (55.2%), infec¬tion (16.2%), hemorrhage (16.2%) unlike response to FGM in Aus-tralian pediatricians (infection 45.1%, pain 39% sexual problems 26.8%,…) and in Flemish midwife (episiotomy 80.7%, caesarean section73.2, prolongation of hospital admission 56.5%) also (in¬fection and pain 52.6%,bleeding and pain 33.1%others 3.7%) in Ethiopians mothers, (hemorrhage 84.7% followed by infection and pain) in eastern Sudanese midwifes, (urinary tract infection 62%, pain 13.52%,tissue tear 6.52%, hemorrhage 1.52%, psychological problems 2.52%) in Sudanese mother the diversity of complication due to diversity of practicing FGM and prepucectomy and differ in population area and the inadequate knowledge about prepucec¬tomy in most of the medical personnel in the study (65.7%) and there is significance association between knowledge level and job in hospital (p=0.023) [1,3,5,7].
When we assess the attitude we found that (62.2%) of the partic-ipants with negative attitude (harmful) and 37.8% with positive attitude (useful); the reasons for negative attitude were (infection 66%, painful physically and psychologically 69%, sexual problem 61.9%, prevent passage of menstrual period 30.6%) not like dis-couraging reasons among Sudanese mother complication, [against religion, affect education, dignity of women, easily uncircumcised girl get married, painful :33,4%,21.9%,16.2%,13.3%,9.5%,5.7% respectively] also long complication of FGM (sexual problems 23.1%, psychological problems 20.1%, infertility and obstetrics problems 5.4%) mentioned by Australian pediatricians and there is a some difference in type of complication from this study which show milder side effect than other study due to difference of prepu¬cectomy in compare to other types of FGM [7]. Also, the reasons behind positive attitude (useful) were(religious practice 49.2%, decrease bacteria replication 39%, increased intersexual satisfac¬tion 12%, safer in comparing to other types of female circumci¬sion 57.6%) and [tradition (85%), suppressing high sexual drive (55.2%) and religious requirement (47%)] in Ethiopians mother thoughts, in Sudanese mid wife(19.1%) of the midwives believed that all types of FGM are harmful, 76.4% were of the opinion that some forms are not harmful and (4.5%) all types of FGM are not harmful. Likewise, while 74.5% of the midwives mentioned that the FGM is a legal practice only 25.5% were of the opinion that FGM is illegal practice [5,7]. The vast majority of the Sudanese midwifes (64.3%) have an opinion that FGM decreases the sexu¬al pleasure [1]. In Sudanese mother who were encouraging FGM (71.5%) the most common reasons behind their attitude :good for marriage 29.7%, preserve virginity 27.4%, religious instruction 19%; and the most popular FGM to them is type 1 because they be¬lieve [religious origin 55.1%, no complication 43.4%, safeguarded virginity 1.5%] it is clear there were some joining points in our study and previous studies in the most sensitive reason [religious] which sometimes appear with and against FGM reasons, and it has more details than to be discussed here, but we should not over¬come cultural and tradition reasons which come superior to reli¬gious reasons, and this indicates the deep effect of it in front of the decision maker of FGM are most probably taken by parents and relatives. Also, we found significant association between attitude and knowledge level (p=0.0001) [7].
The response of participants (190) is poor in practice of prepucec¬tomy (94%) of no practice, which is not matched with Sudanese mother (80.2%) practice FGM to their daughters due to different in knowledge and not with (66.2%) in west of Sudan midwifes intentions in the future, and similar with all Kurdistan professional in not practicing FGM and against it is continuation, also most common place home (100%) similar with Sudanese mothers study (98.6%), the instruments used are (syringe 25%, antiseptic 25%, scissor 25%, bicepce25%) which differ from (knives52%, razors 14.5%, scissor 0.93%) in the previous study due to different in who will perform the procedure, also the person who do the procedure in our study was (100%) midwifes, (47.8% traditional birth atten¬dance, 5% traditional fractions) perform FGM in Ethiopian study who not matching with our results but similar with (TBA 88%, 10% nurse, 1.9% old women) who perform FGM among Sudanese mothers due to differ in level of knowledge and type of procedure, the usage of local anesthesia before prepucectomy was low (56%) and analgesia after prepucectomy (55.56%) also was low due to the inadequate level knowledge other hand sterilization (90%) was good in compeer to (0.00%) of midwifes in western Sudan because they affirmed that FGM do not have risk of HIV transmission, after measuring possibility of learning prepucectomy (60%) can learn medical personnel if the insurance of it appear; the overall practice score was poor (95%) [1,5,7,8].
The reasons to practice prepucectomy was varies [medical, sexual, Increase size of genitalia, itching …] differ from reasons to FGM [cultural 51.2% religious 26%, economic 22.8%] as shown among western Sudan midwifes, and not matching [tradition 5.3% good for marriage 29.7%, preserve virginity 27.4%...] [1,7]. Sudanese mother vision due to differ in the concepts and goal of it. There were association between practice score and knowledge (p=0.23) attitude (p=0.0001) due to dependent of them in each other. It is clear that all good practices was exclusively among midwifes be¬cause of socio-economic impact on them hence Sudan is one of developing country, decrease amount of knowledge.
Conclusion
More than half of medical personnel had inadequate knowledge about prepucectomy
• More than half of medical personnel has negative attitude to¬ward prepucectomy
• Approximately hole of them had poor practice due to weak knowledge and hence attitude [9].
Table 2: Association Between Social Demographic Variables and Attitude of Medical Personnel in Omdurman Locality Obstetrics and Gynecological Hospitals 2019, (n=190) Are you think prepucec-tomy..
|
|
|
|
|
P value |
X2 |
|
|
|
Useful |
harmful |
|
|
|
gender |
male |
12 36.4 |
21 63.6 |
0.853 |
1 |
|
female |
56 38.1 |
91 61.9 |
|||
|
Position in hospital |
Midwife |
33 54.1 |
28 45.9 |
007* |
12.046 |
|
registrar |
32 31.7 |
70 63.3 |
|||
|
obestitrtien |
3 17.6 |
14 82.4 |
|||
|
Knowledge level |
Adequate knowledge |
41% |
15.8% |
0.000* |
0.000 |
|
Average knowledge |
18% |
4% |
|||
|
Not adequate knowledge |
41% |
80.2% |
|||
|
Year of experience |
[0-10] ys |
67.2% |
82.4% |
0.008* |
13.749 |
|
[11-20] ys |
8.2% |
4.9% |
|||
|
[21-30] ys |
16.4% |
2% |
|||
|
[31-40] ys |
6.6% |
5.9%3 |
|||
|
[41-50] ys |
1.6% |
4.9% |
Table 3: association between practice score and knowledge level, attitude of participants toward prepucectomyamong medical personnel in Omdurman, (n=190) LPractice score
|
|
|
Poor |
good |
X2 |
P value |
|
|
Knowl |
Not adquate |
105 97.29% |
32.8% |
15.850 |
0.0001* |
|
|
edge level |
|
|
||||
|
|
|
|
||||
|
|
Moderate |
10 |
4 |
|
|
|
|
|
ly adequate |
71.4% |
28.6% |
|
|
|
|
|
adequate |
39 |
2 |
|
|
|
|
|
|
95.1% |
4.9% |
|
|
|
|
Attitude |
harmful |
108 |
2 |
5.146 |
0.023* |
|
|
|
|
98.2% |
1.8 % |
|
|
|
|
|
useful |
59 |
6 |
|
|
|
|
|
|
90.8% |
9.2 % |
|
|
Table 4: Binary logistic test of practice with socio-demographic characteristics of participants in Khartoum state in 2019,(n=190)
|
|
B |
S.E. |
Wald |
df |
Sig. |
Ex-p(B) |
95% C.I.for EXP(B) |
|
|
Lower Upper |
||||||||
|
gender |
671 |
7049.530 |
000 |
1 |
1.000 |
1.957* |
000 |
|
|
Jop |
- |
3007.190 |
000 |
1 |
|
.000* |
000 |
|
|
|
18.694 |
15620.481 |
|
|
|
|
|
|
|
Constant |
|
|
000 |
1 |
|
|
|
|
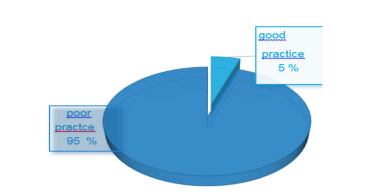
Figure 1: PRACTICE level of PREPUCECTOMY among MEDICAL PERSONNE in OMDURMAN LOCALITY obstetric and gynecological hospitals 2019, (n=190)
Recommendations
• Establishment of more studies in prepucectomy and it is ef-fects is mandatory.
• Closed Control, supervision over medical personnel should be established especially in rural areas.
Acknowledgements
The authors would like to thank all medical personnel who par-ticipated in this study. We would like to extend our thanks whom give me best cooperation; Dr Sit Albanat Khalid Mohammed Ali, nurse: Mada and Dr Sima. No words can describe my thanks to god for kindness, luck, help and blessing.
References
- Ali, A. A. A. (2012). Knowledge and attitudes of female genital mutilation among midwives in Eastern Sudan. Reproductive Health, 9(1), 1-4.
- Circumcision SF. They weren’t talking.
- Cappon, S., L’Ecluse, C., Clays, E., Tency, I., & Leye, E. (2015). Female genital mutilation: knowledge, attitude and practices of Flemish midwives. Midwifery, 31(3), e29-e35.
- Leye, E., Van Eekert, N., Shamu, S., Esho, T., & Barrett, H. (2019). Debating medicalization of Female Genital Mutilation/Cutting (FGM/C): learning from (policy) experiences across countries. Reproductive health, 16(1), 1-10.
- Hussein, M. A., Adem, A., & Mohammed, M. A. (2013). Knowledge, attitude and practice of female genital mutilation among women in Jigjiga Town, Eastern Ethiopia. Gaziantep Med J, 19(3), 164-8.
- González-Timoneda, A., Ros, V. R., González-Timoneda, M., & Sánchez, A. C. (2018). Knowledge, attitudes and practices of primary healthcare professionals to female genital mutilation in Valencia, Spain: are we ready for this challenge?. BMC health services research, 18(1), 1-13.
- Waggiallah, H. A., & Almosaad, Y. M. (2016). Knowledge, attitude, and practice among mothers towards female circumcision Ombada province Khartoum state, Sudan. International Journal of Community Medicine and Public Health, 3(7), 1788.
- Shabila, N. P., Ahmed, H. M., & Safari, K. (2017). Knowledge, attitude, and experience of health professionals of female genital mutilation (FGM): A qualitative study in Iraqi Kurdistan Region. Health care for women international, 38(11), 1202-1218.
- Abdulcadir, J., Say, L., & Pallitto, C. (2017). What do we know about assessing healthcare students and professionals’ knowledge, attitude and practice regarding female genital mutilation? A systematic review. Reproductive Health, 14(1), 1-13.