
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2018) Volume 3, Issue 2
Knowledge, Attitude, and Practice of Health Professionals Towards Labor Companion in Health Institutions in Addis Ababa
2Shiferaw Negash, Associate professor of Obstetrics & Gynecology, School of Medicine, Addis Ababa University, Ethiopia
3Lukman Yusuf, Professor Emeritus, School of Medicine, Addis Abab University, Ethiopia
Received Date: Jul 07, 2018 / Accepted Date: Jul 13, 2018 / Published Date: Jul 23, 2018
Copyright: ©Shiferaw Negash, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: The day of giving birth is a time of unique and intense absorption and learning for every parturient woman because of the interplay of a variety of stressors associated with childbirth such as pain, medical intervention, and hospitalization. Thus, women in labor have a profound need for companionship, empathy, help, and emotional support especially from family members and friends to meet to their needs that the health professional may not be able to address. There is strong evidence showing that continuous support during labor effectively improves delivery outcomes. It is factual that most of the facilities in Ethiopia do not have a policy that allows a companion in the delivery room to accompany the mother despite the dire need. The knowledge and attitude of health professionals towards this support system has an immense effect on the implementation of this policy by the institutions.
Objective: To assess the knowledge, attitude, and practice of health professionals towards labor companion in the health institutions of Addis Ababa.
Methods: Facility-based cross-sectional study in 30 health institutions of Addis Ababa was conducted using self-administered structured questionnaire from March 1 to June 30, 2016. The results were summarized using descriptive statistics. Bivariate logistic regression analysis and odds ratio along with 95% confidence interval was used to assess the degree of association between dependent and independent variables. The variables with significant association were entered into multivariate logistic regression model.
Results: Among the total of 378 respondents, 275(72.8%) were females and 252(66.7%) were midwives. Most of the respondents, 239(93.4%) stated to have knowledge on the importance of labor companion but only 167(44.2%) had adequate knowledge. From the study participants, 239(63.2%) had positive attitude towards labor companion but only 139(36.8%) stated it is practiced in their institution. Having adequate knowledge is significantly associated with positive attitude. Health professionals working in private institutions and health centers have the practice of allowing labor companion better than those in government hospitals.
Conclusion and recommendation: This study concluded that less than half of the study participants have adequate knowledge regarding the benefits of labor companion though majority have positive attitude. Health professionals should be updated on evidence-based support of labor companionship; and all the stakeholders involved should make the effort in bringing change towards labor companion.
Keywords
Labor Companionship, Knowledge, Attitude, Practice, Ethiopia
Introduction
Across time and cultures, women have been supported during labor by other women who are skilled in providing continuous emotional and physical support. When childbirth moved to the hospital, this component of supportive care was largely lost. Widespread use of fetal monitors and other medical interventions for normal childbirth during the end of the 20th century changed the focus of intrapartum nursing to the technological rather than the supportive aspects of childbirth. Labor support is a term used to describe measures, and other forms of tangible assistance to help a woman cope with the stress of labor and childbirth in the presence of an empathic person who offers advice, information, and comfort [1].
Labor companionship is a human interactive process which provides emotional, cognitive and physical support during labor and delivery. The labor support process includes talking to the woman, and encouraging and recognizing the woman’s labor efforts, maintaining eye contact, providing information about the progress of labor, explaining procedures, answering questions honestly, and encouraging the woman to adopt the most comfortable position possible, suggesting how to relax, breathe and push when necessary, giving a massage, holding hands, gently caressing the woman, offering a bedpan, changing bed clothes, offering food or drink and distracting the woman from concentrating on her labor pain but focusing on the positive outcome of the labor pain. It is a general agreement that companionship during labor should be the norm rather than the exception [2, 3].
A woman develops a feeling of security in the presence of familiar people in an unfamiliar environment. A woman is likely to cope with labor stress and adapt to a “strange” environment when someone she knows is continuously present with her and is encouraging and appreciating her efforts. The dignity of the woman is maintained throughout the labor and delivery because labor and delivery are not reduced to a technical procedure but a psychosocial interaction of human beings through a normal developmental process. Labor and delivery viewed from the labor companion’s perspective is a social event and not a medical procedure. Labor companionship will encourage women and professionals to view labor and delivery as a natural process that must take place in a natural environment. It is important to state that labor support for pregnant women is a right that all women should have, regardless of where they come from or who they are. The Maternity Center Association in the United States stresses that the “consistent presence of a supportive provider during labor and birth should be a guaranteed right for all women” [4].
The supported woman is more likely to give birth without using analgesia, less likely to have a protracted labor, augmentation of labor, caesarean delivery or instrumental vaginal birth and less likely to report dissatisfaction with her childbirth experience. Furthermore, continuous support during labor and delivery is a key component to increased breastfeeding initiation. The presence of a companion of the woman’s choice had a positive influence on her satisfaction with the birth process and also it has a profound effect on lower prevalence of postpartum depression. In order for this support to be effective, it is important for the midwives and other health professionals to 4 understand the benefits of continuous support to women in childbirth and how it can enhance normal childbirth physiology [5 -12].
Hence, the objective of this study is to explore all aspects of labor companionship in our setup and forward recommendations for future practice.
Methods
This was an institution-based cross-sectional descriptive study carried out from March 1 to June 31, 2016. It was conducted in health institutions of Addis Ababa where delivery service is available. The city has ten sub cities and 116 Worde as. There are 7 hospitals under Addis Ababa Health Bureau and 4 hospitals under the Federal Ministry of Health. There are also 93 health centers and 34 private hospitals. The source population included all health professionals working in the labor wards in the aforementioned institutions.
The inclusion criteria included health professionals working in labor wards in Addis Ababa during the specified period. It comprised of gynecologists, general practitioners, nurses (BSC, diploma), health officers, midwives (diploma, degree graduates) and health professionals with experience of working in labor ward for at least six months or more.
The exclusion criteria were set as health professionals working outside the labor ward, no desire to participate, health professionals who were not available during the study period and health professionals with experience of working in labor wards for less than six months.
The minimum sample size was determined using the 30/7 WHO recommendation which can be used for non-vaccine related researches. From the 30 health institutions, seven health professionals were selected yielding a total of 210 respondents.
To minimize the design effect, the sample size was multiplied by 2. The final sample size thus calculated was 420. Three cluster groups were formed: government hospitals, private hospitals, and health centers. From each cluster, the institutions and the subjects were chosen by simple random sampling.
The total sample of 420 health professionals were distributed between 10 government hospitals, 10 private hospitals and 10 health centers by proportion, taking the average number of health professionals working in the labor ward in each institution and calculating the share of each institution for the total number of professionals. The studied health institution and the individuals from each institution were chosen by simple random sampling.
Data was collected using self-administered structured questionnaire. The questionnaire was prepared in English and it was then translated into Amharic. Data was collected using an appointed data collectors for the individual health institutions. Training on data completeness, cross-checking and correction actions was given to the data collectors. The data collectors reported and communicated with the principal investigators on daily basis throughout the data collection period to ensure quality of data. Questionnaire was pre-tested to determine the accuracy of the responses and the appropriateness of data collection tool.
The data collection instruments were coded and data was checked and entered using SPSS Version 21.0 and checked for missing values before analysis. The data was categorized and summarized using descriptive statistics like frequency tables, graphs, and proportions. Bivariate logistic regression analysis with the help of odds ratio along with the 95% confidence interval was used to assess the degree of association between dependent and independent variables and level of significance was set at P<0.05. The variables which had significant association with the outcome variable were entered into multivariate logistic regression model to identify the important determinants by controlling for possible confounding effects.
Ethical clearance was obtained from the Department Research and Publication Committee, and the Institutional Review Board of the College of Health Sciences, Addis Ababa University. The Addis Ababa Health Bureau was communicated through the support letter from the Department Of Obstetrics and Gynecology, CHS, AAU and then a written permission from the Bureau was submitted to the sub-cities and then to the respective health facilities. Each professional in selected health institution was approached with a written consent form for willingness to participate; and confidentiality was maintained at all levels of the study.
Results
From the initially planned sample size of 420 individuals, data was collected from 378 health professionals giving in a response rate of 90 %. Of the respondents, 148(39.2%) were below the age of 25 years and their age ranged from 20-60 years with a mean age of 28.37 (SD+ 6.65) years. As shown in Table 1, 275 (72.8%) were females, 270 (71.4%) were Orthodox Christians by faith and 236 (62.4%) were single.
Table 1: Socio-demographic characteristic of health professionals, March -June, 2016
|
Characteristics |
Number |
Percentage |
|
|
Age |
<25 |
148 |
39.2 |
|
25-29 |
125 |
33.1 |
|
|
30-34 |
49 |
13.0 |
|
|
35 and above |
56 |
14.8 |
|
|
Sex |
Male |
103 |
27.2 |
|
Female |
275 |
72.8 |
|
|
Marital status |
Single |
236 |
62.4 |
|
Married |
137 |
36.2 |
|
|
Divorced |
3 |
0.8 |
|
|
Widowed |
2 |
0.5 |
|
|
Religion |
Orthodox Christians |
270 |
71.4 |
|
Protestant |
66 |
17.5 |
|
|
Muslim |
33 |
8.7 |
|
|
Catholic |
1 |
0.3 |
|
|
Others |
8 |
2.1 |
|
Nearly two thirds, 252(66.7%) of the subjects were midwives, followed by clinical nurses 86 (22.8%), and only 25(6.6%) were obstetrician-gynecologists. Of the midwives, the majority 153(60.7%) were diploma holders. Most of the study subjects 264(70%) had a length of experience ranging from one to ten years. The duration of experience of the study subjects ranged from six months to 40 years with a median of 4 years. The majority, 209(55.3%) of the participants were from government hospitals followed by 95(25.1%) from private institutions. Of the study participants, 95(25.1%) of them had been in their current working place for the last 5-10 years (Table 2).
Table 2: Level of education, institution, work experience, and opinion of health professionals
March- June, 2016
|
Characteristics |
Number |
Percentage |
|
|
Educational level |
Obstetrician/Gynecologist |
25 |
6.6 |
|
|
Health officer |
11 |
2.9 |
|
|
General practitioner |
4 |
1.1 |
|
|
Clinical nurse degree |
27 |
7.1 |
|
|
Clinical nurse diploma |
59 |
15.6 |
|
|
Midwife degree |
99 |
26.2 |
|
|
Midwife diploma |
153 |
40.5 |
|
Health institution |
Government Hospital |
209 |
55.3 |
|
Private Hospital |
95 |
25.1 |
|
|
Health Center |
74 |
19.6 |
|
|
Professional experience (years) |
Less than one year |
75 |
19.8 |
|
|
One to three years |
77 |
20.4 |
|
|
Three to five years |
92 |
24.3 |
|
|
Five to ten years |
95 |
25.1 |
|
|
More than 10 years |
39 |
10.3 |
Most health professionals in the study, 353(93.4%) have good knowledge on the importance of labor companionship, while only 167(44.2%) of the respondents admitted to have adequate knowledge (respondents who scored above the mean, >5.7), on the clinical benefits of the companionship. When sex adjusted analysis was done, 60 (63.2%) of males and 107(41.5%) of females have adequate knowledge regarding labor companion, but the knowledge difference between the two sexes was statistically significant, COR 2.419 95% CI 1.490-3.929. The difference is not significant after adjusting for the confounders, with the AOR 1.648 95% CI 0.960-2.827. Regarding the practice by the health professionals, 239(63.2%) did not allow a labor companion to the delivery room, whereas 139(36.8%) were lenient on the presence of a companion. Similarly, 226(59.8%) of the participants agree that such an approach should be implemented as opposed to 127(33.6%) of the health professionals who did not agree that the health institutions should adopt a policy of allowing a companion to the labor ward as illustrated in Table 3.
Table 3: Health professionals’ opinion and practice of allowing labor companion. March-June, 2016
|
Characteristics |
Frequency |
Percentage |
|
Role of companionship during labor |
||
|
Emotional support |
339 |
89.7 |
|
Physical support |
242 |
64.0 |
|
Information |
162 |
42.9 |
|
Give assistant to the staff |
153 |
40.5 |
|
Take care of new born |
180 |
47.6 |
|
Early initiation of breast feeding |
172 |
45.5 |
|
Benefit of labor companion on labor process |
||
|
Shorter duration of labor |
157 |
41.5 |
|
Less pain |
215 |
56.9 |
|
Less caesarean section rate |
192 |
50.8 |
|
Less low 5-minite APGAR score |
85 |
22.5 |
|
Increased satisfaction with childbirth experience |
203 |
53.7 |
|
Less augmentations |
102 |
27.0 |
|
Less instrumental deliveries |
77 |
20.4 |
|
Less postpartum depression |
233 |
61.6 |
|
Labor companion allowed in their setup N=378 |
||
|
Yes |
139 |
36.8 |
|
No |
239 |
63.2 |
|
Why labor companion allowed N=135 |
||
|
Institution policy |
104 |
77.0 |
|
For decision making |
98 |
72.6 |
|
Maternal request |
97 |
71.9 |
|
Mother in critical condition |
65 |
48.1 |
|
Why labor companion not allowed N=239 |
||
|
Institution policy |
104 |
43.5 |
|
Crowding of labor ward |
179 |
74.9 |
|
Loss of privacy of mothers |
122 |
51.0 |
|
Spread of infection |
125 |
52.3 |
|
Do mothers request for companion? N=378 |
||
|
Yes |
325 |
86.0 |
|
No |
53 |
14.0 |
|
How many? N=325 |
||
|
Less than one-quarter |
55 |
16.9 |
|
One-quarter |
45 |
13.8 |
|
Half |
113 |
34.8 |
|
Three-quarter |
54 |
16.6 |
|
More than three-quarter |
58 |
17.8 |
Three quarters of the professionals 104(74.8%) stated that it is the institution’s policy to allow labor companion in contrast to 98(70%) who affirmed that it is allowed for decision making and maternal request purposes. Furthermore, as shown in Table 3, the respondents have put some reasons why a labor companion is not allowed in their setup. Crowding of the labor ward is the most frequent reason pointed out by three quarter of health professionals 179(74.9%). Regarding maternal request for labor companion, 325(86%) of them do so It was found out that of the 239 study subjects who accept allowing a labor companion to the delivery room, 205(85.7%) of them agree that a companion should be present during the first stage of labor while 114 (47.6) agree that labor companion be present at all levels of labor. Almost all, 234(97.9%) of the participants agree that labor companion should be practically allowed after delivery. Among the respondents who accepted labor companion (N=239), 221(92.5%) preferred the mother as a companion of choice followed by 177(74%) who recommended the husband as a companion (Table 4).
Table 4: Health professionals’ acceptance of labor companion and the recommended companion during labor, March- June, 2016
|
Characteristics |
Strongly disagree |
Disagree |
Neutral |
Agree |
Strongly agree |
|||||
|
|
No |
% |
No |
% |
No |
% |
No |
% |
No |
% |
|
Acceptance of companionship |
52 |
13.8 |
83 |
22.2 |
4 |
1.1 |
205 |
54.2 |
34 |
9 |
|
Preferred companions |
||||||||||
|
Mother |
6 |
2.5 |
10 |
4.2 |
2 |
0.8 |
150 |
62.7 |
71 |
29.7 |
|
Husband |
44 |
18.4 |
17 |
7.1 |
1 |
0.4 |
129 |
519 |
48 |
20 |
|
Sister |
10 |
4.2 |
43 |
18 |
61 |
25.5 |
98 |
41 |
27 |
11.3 |
|
Friend |
20 |
8.3 |
78 |
32,6 |
F3 |
38.9 |
38 |
15.9 |
10 |
4.2 |
|
Doula |
12 |
5 |
48 |
20 |
91 |
38 |
72 |
30 |
F |
7 |
Among the participants who disagreed (N-135) on allowing labor companion to the delivery room, about three quarters of them, 107 (79%) stated their reasons to be crowding of the labor ward, loss of privacy to the mothers, increased spread of infection, interference with the job of professional care givers by the companion, and increased anxiety of health professionals in case of an emergency situation. It was shown that a good segment of the study population accounting for 70 (52%) stated that the policy of the institution per se, violence by the companion, and creation of negative image against the health professional to be the predominant reasons for not allowing a labor companion (Figure 1).
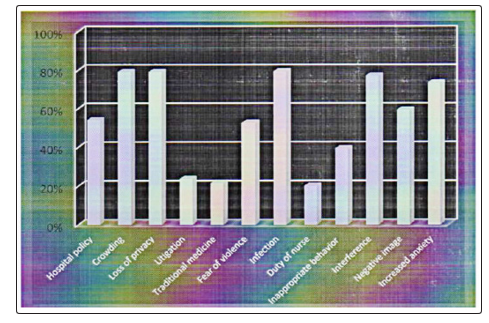
Figure 1: Reasons of health professionals for refusing companionship, March- June, 2016
Health professionals have also forwarded suggestions on how to change this practice and the majority, 190(79.5%) proposed that there should be separate room for each laboring mothers since crowding of the labor ward is a major problem followed by giving health education to the companion 170(71.1%) as presented in Figure 2.
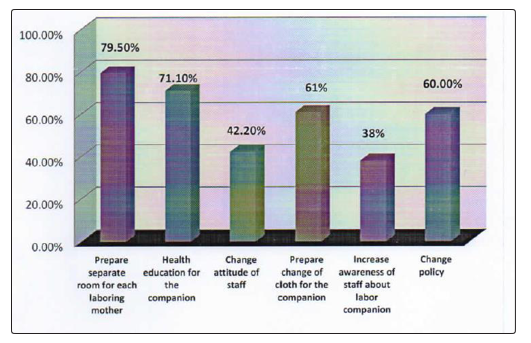
Figure 2: Recommendations forwarded by health professionals, March- June, 2016
The participants above the age of 35 years, 39(69.7%), had better knowledge about labor companion compared to the age group less than 25 years, 50(37.3%), COR 3.854 95% CI 1.975-7.521 and AOR. 4.304 95% CI 1.352-13.700. Considering educational level of the study subjects, obstetrician and gynecologists, 32(82%), have better knowledge than midwives 108(45.7%) and nurses 27(34.6), with the COR 8.63595% CI 3.368-22.138 and the AOR of 5.015 95% CI 1.832-13.727. There is a statistically significant difference in the knowledge relating to labor companion in professionals who served for more than 10 years 24(61.5%) compared to those who have served for less than one year 25(37.3%), COR 2.68895% CI 1.192-6.062. However, this difference is lost after adjusting for other variables. Those professionals who practice allowing labor companion to the delivery unit have adequate knowledge accounting for 119(55%) than those who do not 67(49%), but the difference is not statistically significant (Table 5).
Table 5: Factors of selected variables by mean knowledge score of health professionals for labor companion, Mar- Jun, 2016
|
Variables |
Adequate mean knowledge score >5.7) |
Inadequate mean knowledge score <5.7 |
COR (95% CI) |
AOR(95% CI) Number (%) |
|
|
Number (%) |
Number (%) |
|
|
|
Sex |
||||
|
Male |
60(63.2) |
35(36.8) |
2.419(1.490-3.929)* |
1.648(0.960-2.827)** |
|
Female |
107(41.5) |
151(58.5) |
|
|
|
Age |
||||
|
<25 |
50(37.3) |
84(62.7) |
|
|
|
25-29 |
53(46.1) |
62(53.9) |
1.436(0.865-2.384 |
1.497(0.840-2.667) |
|
30-34 |
23(50) |
23(50) |
1.826(0.938-3.554) |
1.724(0.788-3.771) |
|
>35 |
39(69.7) |
17(30.3) |
3.854(1.975-7.521)* |
4.304(1.352-13.700)** |
|
Religion |
||||
|
Orthodox |
121(46) |
142(54) |
0.749(0.430-1.304) |
|
|
Muslim |
13(46.4) |
15(53.6) |
0.762(0.311-1.863) |
|
|
Protestant |
33(54.1) |
29(45.9) |
|
|
|
Education |
||||
|
Gynecologist |
32(82) |
7(18) |
8.635(3.368- |
5.015(1.832-13.727)** |
|
Midwives |
108(45.7) |
128(54.3) |
1.594(0.936-2.713) |
1.982(1.116-3.518)** |
|
Nurses |
27(34.6) |
51(65.4) |
|
|
|
Year of |
||||
|
experience Less than one |
25(37.3) |
42(62.7) |
|
|
|
1-3 years |
31(46.3) |
36(53.7) |
1.447(0.726-2.884) |
1.337(0.652-2.738) |
|
3-5 years |
43(49.4) |
44(50.6) |
1.642(0.858-3.143) |
1.391(0.692-2.798) |
|
5-10 years |
44(47.3) |
49(52.7) |
1.509(0.795-2.864) |
1.032(0.482-2.211) |
|
>10 years |
24(61.5) |
15(38.5) |
2.688(1.192-6.062) |
0.703(0.194-2.551) |
|
Practice |
||||
|
Yes |
119(55) |
97(45) |
0.780(0.508-1.198) |
|
|
No |
67(49) |
70(51) |
|
|
*P<0.05
*Statistically significant after adjusted for age, sex, education and year of experience
As shown in Table 6, 235(62.2%) of the participants had a positive attitude towards labor companion (mean attitude score >24.16). There was no significant difference in attitude between male and female subjects. Age and years of experience have significant association with positive attitude. Those individuals above the age of 35, 41(73.2%) were more positive about labor companion than those younger than 25, 77(42%), COR 2.520 95% CI 1.285-4.943. But this was not shown to be significant after adjusting for different variables. There is significant difference in positive attitude between professionals with experience of 5-10 years, 71(75%) compared to those less than one year 38(50.7%), COR 2.880 95% CI 1.508-5.503. However, the difference was not significant after adjustment.
*P
Table 6: Factors of selected variables by mean Attitude score of health professionals for labor companion, March- June, 2016
|
Variables Sex |
Positive (mean Attitude score |
Negative (mean Attitude score <24.16 |
COR (95% CI) |
AOR(95% CI) |
|
|
Number (%) |
Number (%) |
|
|
|
Male |
64(62.2) |
39(37.8) |
0.998(0.626-1.592) |
|
|
Female |
171(62.2) |
104(37.8) |
|
|
|
Age |
||||
|
<25 |
77(42) |
71(48) |
|
|
|
25-29 |
84(67.2) |
41(32.8) |
1.889 (1.153-3.094) |
1.644(0.804-3.363) |
|
30-34 |
33(67.4) |
16(32.6) |
1.902(0.965-3.749) |
0.977(0.352-2.708) |
|
>35 |
41(73.2) |
15(26.8) |
2.520(1.285-4.943) |
0.808(0.168-3.891) |
|
Marital status |
||||
|
Unmarried |
143(59.3) |
98(40.7) |
|
|
|
Married |
92(67.2) |
45(32.8) |
1.401(0.903-2.174) |
0.851(0.429-1.687) |
|
Education |
||||
|
ObGyn |
30(75) |
10(25) |
1.607(0.692-3.730) |
.0.659(0.138- |
|
Midwives |
149(59.2) |
103(40.8) |
0.775(0.466-1.290) |
0.611(0.303-1.233) |
|
Nurses |
56(65.2) |
30(34.8) |
|
|
|
Knowledge on labor companion |
||||
|
Below the mean |
103(55.4) |
83(44.6) |
|
|
|
Above the mean |
132(80) |
35(20) |
3.039(1.896-4.871)* |
3.107(1.697-5.689)** |
|
Experience |
||||
|
Less than one year |
38(50.7) |
37(49.3) |
|
|
|
1-3 years |
43(46) |
34(44) |
1.231(0.651-2.331) |
0.963(0.402-2.308) |
|
3-5 years |
58(63) |
34(37) |
1.661(0.894-3.087) |
1.238(0.535-2.862) |
|
5-10 years |
71(75) |
24(25) |
2.880(1.508-5.503) |
1.639(0.649-4.140) |
|
>10 years |
25(64) |
14(36) |
0,785-3.853) |
1.008(0.186-5.468) |
|
Children |
||||
|
No |
99(57.2) |
74(42.7) |
|
|
|
Yes |
73(71.6) |
29(28.4) |
1.882(1.113-3.181) |
0.695(0.357-1.352) |
|
Companion |
||||
|
No |
30(73) |
11(26.8) |
|
|
|
Yes |
43(70.5) |
18(29.5) |
0.876(0.362-2.119) |
|
*P
As presented in Table 7, those professionals with adequate knowledge towards labor companion 132(80%) had positive attitude than those with inadequate knowledge 103(55.4%), COR 3.039 95% CI 1.896-4.871. This association remains statistically significant after adjusting for other variables, AOR 3.107 95% CI 1.697-5.689. From the female participants, those who had children, 73(71.6%) had more positive attitude towards labor companion than those who did not, 99(57.2%), COR 1.882 95% CI 1.113-3.181 though this association was lost after adjusting for confounders.
Table 7: Factors of selected variables by practice of health professionals on allowing labor companion, March-June, 2016
|
Variables |
Yes |
No |
COR(95% CI) |
AOR(95% CI) |
|
Sex |
||||
|
Male |
42(40.8) |
61(59.2) |
1.263(0.794-2.010) |
|
|
Female |
97(35.3) |
178(64.7) |
|
|
|
Institution |
||||
|
Government |
50(24) |
159(76) |
|
|
|
Private |
56(59) |
39(41) |
4.566(2.721-7.663)* |
3.847(2.849-6.662)** |
|
Health center |
33(44.5) |
41(55.5) |
2.560(1.465-4.475)* |
1.913(1.015-3.180)** |
|
Education |
||||
|
Obstetrician gynecologist |
14(35) |
26(65) |
1.115(0.506-2.460) |
|
|
Midwives |
97(38.5) |
155(61.5) |
1.296(0.773-2.175) |
|
|
Nurses |
28(32.5) |
58(67.5) |
|
|
|
Knowledge related to labor companion |
||||
|
Below the mean |
67(36) |
119(64) |
|
|
|
Above the mean |
70(42) |
97(58) |
1.282(0.835-1.969) |
|
|
Attitude towards labor companion |
||||
|
Below the mean |
46(32.2) |
97(67.8) |
|
|
|
Above the mean |
93(39.6) |
142(60.4) |
1.381(0.892-2.139) |
1.403(0.869-2.264) |
Having adequate knowledge 70(42%) and positive attitude 93(39.6%) are not significantly associated with allowing labor companion. The only variable which showed significant association is the type of institution. Those study participants who work at health center 33(44.5%) and private setups 56(50%) allow a labor companion for the laboring women more than those who work at government hospitals, 50(24%), COR 2.560 95% CI 1.465-4.475 and COR 4.566 95% CI 2.721-7.66, respectively. This difference remains statistically significant after adjusting for other variables, AOR 1.913 95% CI 1.0153.180 and 3.847 95% CI 2.849-6.662, for the health center and private setups respectively (Table 7).
Finally, inward analysis of the overall self experiences highlights that out of a total of 275 female study participants, 102(37%) had given birth and 70 (68.6%) of them have had vaginal birth while the rest 32(31.4%) did so by caesarean section. Their report revealed that 61(59.8%) had labor companion during their own delivery. From those who had a companion, more than two third of them 42(68.8%) had their husband as a companion followed by 17(27.8%), 13(21.3%), and 11(18%) their mothers, friends, and sisters respectively. Out of the 61 female participants who had labor companion in their own delivery, the majority, 55(90.2%) stated that having a companion gave them strength during labor. Of the 24 female participants who were not allowed to have labor companion during their own childbirth, because the facility did not possess such a policy and moreover about half of them showed regret for not having a labor companion.
Discussion
One of the indicators in the FIGO guideline of 2015 on Mother-baby friendly birthing facilities is that the health facility has a written policy in place that encourages women to have at least one person of their choice to be with her throughout labor and birth [13]. The Federal Ministry of Health of Ethiopia has also endorsed these principles and adopted it; and streamlined the package in keeping with the launching of the Respectful Maternity Care. This is the first ever conducted clinical research in our setup addressing labor companionship in laboring women involving all cadres of health professionals engaged in attending to them and who were randomly selected from governmental and non-governmental health institutions.
The mean age of the respondents was 28.3 years; in similar thematic publications it was reported as 23.7, 36.5, and 37 years [14,15,16]. This variation is the reflection of our study design that included a total of 378 health professionals which is quantitatively higher and diverse than all the qualitative researches done in this area that merely comprised of 11, 18, 20, 60, and 76 candidates [14-19]. It is interesting and impacting to note that the study done in Brazil included nurses, obstetricians and general practitioners while the output in three Arab states recruited obstetricians, midwives and nurses (31, 36) and only midwives in Botswana, India, Malawi and Zambia [4,15, 16,20].
The findings in our study that 44.2% of the respondents have adequate knowledge on the benefits of labor companion was much lower than the studies from Malawi and Egypt of but higher than a publication from India where only 25% of the health professionals understood the benefits of having companion for reasons specified above [16,19,15]. However, it is documented that all healthcare providers were knowledgeable about evidence supporting labor companionship in qualitative studies done in Botswana, Brazil, China, Zambia and three Arab states, which is comparable to our report of 93.4% [4, 14, 17, 18, 20].
The study revealed that 90% of the participants agree that a companion would give an emotional support is comparable to the report from Egypt 100%, in contrast to 33% from Malawi. Regarding physical support, 64% of the health professionals in our study corroborated it as one of the benefits which is far lower than the 100% in Egypt, but higher than the 18.3% in Malawi [16,19]. It is noted that 63.2% are not in favor of labor companion. In several other qualitative studies,most health professionals were overwhelmingly shown to have a positive attitude towards labor companion which is lacking in our undertaking [4,14-20]. This difference could be due to the population thus studied, as the professionals for example in Malawi are older with several years of experience making them more appreciative of the benefits of labor companion. It is very true that most of the labor wards in the different health institutions in Addis Ababa are very often simultaneously occupied by many laboring mothers and this creates crowding and loss of privacy for the mothers in addition to the existing policy of the institution not conducive of allowing a companion; making it harder for these professionals to accept a labor companion compared to a similar setup [16]. Hence, crowding remains the main reason pointed out by the health professionals in this study for not permitting labor companion in the labor ward, though not so pronounced, like the 100% of the health professionals in the Egyptian study. Interference of care by the companion 77% was another factor described in the current study which was found out to be higher than the study in Egypt (53.8%) and Malawi (23%). The presence of labor companion would create a negative attitude towards health care providers that is reflected in the current study is quite comparable to the study in Egypt but lower than the report from Malawi [16,19].
In India, where the study was undertaken in a university hospital, the only reason for not accepting labor companion was the belief that all professionals think that such a support could only be given by the professionals themselves in comparison to the 20% of the professionals in the current study.
This may be due to the fact that nurses working in India may be more familiar with the labor support measures that the laboring woman might need than the health professionals in our setup [15].
The preference of the health professional to the mother (92.5%) followed by the husband (74%) as labor companion in our study is in conformity with that of Egypt where 100% of the health care providers favored mothers and only 9% stated husbands to serve as a companion [19]. This choice of companion is also in agreement with the result of the research done in Ethiopia concerning parturients’ need of labor companion, where 54% and 37% of laboring women chose their mothers and partners respectively during labor and delivery [22]. In contrast to this, the study done in India, 60% of the professionals stated a close friend to be a companion and 30% preferred the husband. This could be due to cultural differences and in our culture women especially mothers play a vital role during labor and delivery; and it is also presumed that husbands/partners lack experience and objectivity due to their emotional involvement [15].
As to the stage of labor, 85.5% of the health professionals documented that a companion should be present during the first stage of labor whereas 98% agreed for the presence of the companion after delivery. This result is also similar with the study done in Egypt, where 81.8% and 100% of health professionals agree on the presence of companion in the first stage of labor and after delivery respectively. In another study done in Lebanon, Syria, and the West Bank, health professionals stated to always allow labor companion in 74%, 47%, and 60% respectively during first stage of labor, which is lower than the current study. In the same study, only 33% in Lebanon and 11% in Syria detailed to allow companion during delivery which is far lower than our result [19,23]. In a qualitative study in Botswana, all the professionals elaborated that labor companion must be present at all stages of labor and delivery as opposed to the current study where only 47.6% of the health professionals agree to allow labor companion at all stages of labor [4]. As a matter of principle, it is prudent that a companion of one’s choice should be available and enabled to provide a continuum of support throughout the labor and delivery processes though there exist paradoxical practices.
The world literature accentuates that support to women during childbirth from a birth companion point of view is a worldwide practice and worth deserving attention. The reasons to allow labor companion in general are based on institution policy, empowerment of decision making ability from rights perspective and maternal request per se [10, 15, 17-19, 21, 24-29]. Moreover, it is to be underlined that labor companion is not allowed in significant centers in the African setup for reasons that include fear of infection, crowding of the labor wards, lack of space, lack of privacy, non-existent institutional policy and guidelines as well as cultural factors which is in conformity with a number of similar studies [4,16,19,20,26].
It is asserted that supportive companionship was highly acceptable among health professionals both before and after its implementation and the healthcare professionals have also been seen to overcome their worries and concerns regarding provision of such support after they themselves experience it. Hence, it is deducible that if the practice of labor companion was possible in our setup, the attitude of the health professionals might improve bringing a better care for laboring mothers wherever and whenever possible.
The health professionals have forwarded some recommendations in order to improve the practice of allowing labor companion in our health institutions like preparing separate rooms for each laboring mothers, health education for the companion, increasing awareness to staff about labor companion and changing the institution’s policy regarding labor companion.
Studies revealed that women preferred home deliveries because they want to be with a relative, emphasize trust ship in traditional birth attendance or relatives and expression of their dislike towards the behavior of health professionals. Seventy three percent of women had fear of labor at the health institutions in one study in Ethiopia, for fear of being among unfamiliar people or unfamiliar environment and strangers. Hence, there is a need to address the quality of obstetric care in government facilities to improve the uptake of services by making the care and delivery more humane [22,26,29].
Healthcare providers play a profound role at the time of birth facilitating attachment between mothers and newborns, as well as family closeness. Health professionals should aim to understand the needs and care of a woman during labor and birth so as to ensure a positive experience for the woman and her family, while maintaining their health, preventing complications and responding to emergencies. The finding of this research gives valuable information on the benefits of labor companion and the knowledge, attitude and acceptance and practice of health professionals towards this program in our institutions. Changing clinical practice might be difficult to achieve and likely to require multifaceted approaches including changing institution’s policy, remodeling the available infrastructures, and motivating policy makers and health professionals into practical adaptability with updated protocols and positive attitude. Considering the benefits of having labor companion and the woman’s need of companion shown in previous study, responsible bodies should make the effort to make this program a reality.
References
- Hodnett ED, Gates S, Hofmeyr GJ. Sakala C (2012) Continuous support for women during childbirth. Cochrane Database Systematic Review 10: 4.
- Arnorim MMR, Katz L Continuous support for women during childbirth: RHL commentary (2012). The WHO Reproductive Health Library: Geneva: World Health Organization.
- Maria Iliadou (2012) Supporting women in labor. Health science Journal Basis for The Ten Steps of Mother-friendly Care. The Journal of Perinatal Education 2007 6: 385-391.
- Makhutsisa Martha Mothibe (2001) Obstacles to labor companionship at Bamalete Lutheran hospital Ramotswa, Botswana. Unpublished paper.
- Morhason-Bello IO, Adedokun BO, Ojengbede OA (2009) Social support during childbirth as a catalyst for early breastfeeding initiation for first-time Nigerian mothers. IntBreasifeed J 10: 16.
- Dolman W, Chalmers B, Hofmeyr G. Nikodem V.C (1993) Postpartum depression and companionship in the clinical birth environment: A randomized, controlled study. American Journal of Obstetrics & Gynecology 168: 1388-1393.
- Madi B, Sandal J, Bennett R, Macleo C (1999) Effects of female relative support in labor: A randomized controlled trial. Birth 26: 4-8.
- Campbell D, Scott IUD, Klaus MI-I, Falk M (2007) Female relatives or friends trained as labor doulas: Outcomes at 6 to 8 weeks postpartum. Birth 34: 220-227.
- Scott IUD, Berkowitz O, Klaus MA (1999) A comparison of intermittent and continuous support during labour: A meta-analysis, American Journal of Obstetric Gynecology 180: 1054-1059.
- Odalea MB, Mary A P, Maria JD, OsisJose GC (2007) Support to woman by a companion of her choice during childbirth: A randomized controlled trial. Reproductive Health 4: 5.
- Donna J, Sauls RN (2002) Effects of Labor Support on Mothers, Babies, and Birth Outcomes. JOGNN 31: 733-741.
- Holder K (2011) Birthing support and breastfeeding initiation in Somaliland: Experiences at the Edna Adan Maternity Hospital in Hargeisa. East Africa J Public Health 8: 38-41.
- FIGO Guideline (2015) Mother—baby friendly birthing facilities. International Journal of Gynecology and Obstetrics 128: 95-99.
- Odalea MB, Mary AP, Maria JD, Osis Jose (2007) Support during childbirth: Perception of health care providers and companions chosen by women. Rev. Public Health 41: 28-35.
- Xu Qian, Helen Smith, Li Zhou, Ji Kiang, Paul Gamer (2001) Evidence-based obstetrics in four hospitals in China: An observational study to explore clinical practice, women’s preferences and provider’s views. BMC Pregnancy and Childbirth 1: 1.
- Pravati T, Prasanna B (2013) Comparing opinion on needs of laboring women among mothers & midwives working in labor room at a University Medical College Hospital. India Journal of Nursing and Health Science 2: 5-9.
- Kabakian-Khasholian A, El-Nemer A, Bashour H (2015) Perceptions about labor companionship at public teaching hospitals in three Arab countries, International Journal of Gynecology and Obstetrics 129: 223-226.
- Nagwa I, Mustafa E, Hanan A, Moawad E, Amiria M, et al. (2015) Feasibility and Acceptability of Labor Companionship at Mansuora University Hospital / Egypt. Journal of Nursing and Health Science 4: 39-45.
- Banda O, Kafulafula G, Nyirenda E (2011) Acceptability and experience of supportive companionship during childbirth in Malawi. BJOG 117: 937-945.
- Maimbolwa MC, Sikazwe N, Mamba B, Diwan V, Ransjo Arvidson AB (2001) Views on involving a social support person during labor in Zambian maternities. J Midwifery Women’s Health 46: 226-234.
- Murray M, Huelsman CM (2009) Labor and delivery nursing: A guide to evidence based practice. New York Springer 5: 22-27.
- Million T, Ahmed A, Solomon K (2007) Parturients’ need of continuous labor support in labor wards. Ethiop Health Dev 21: 35-39.
- Karima K, Tamar K-K, NahedM, Hyam B (2005) Routines in facility-based maternity care: evidence from the Arab World. Choices and Challenges in Changing Childbirth Research Network. BIOG.- an International Journal of Obstetrics and Gynecology 112: 1270-1276.
- Hunter LP (2002) Being with Women: A Guiding Concept for the Care of Laboring Women. Journal of Obstetric, Gynecologic, and Neonatal Nursing 31: 650-657. 25. Audu BM, El-Nafaty AU, Bako BG, Melah GS, Mairiga AG, et al. (2008) Attitude and preferences of Nigerian antenatal women to social support during labor. Journal of Biosocial Science 40: 553-562.
- Heather B, G Justus H, V Cheryl N, Helen S, Paul G (2007) Promoting childbirth companions in South Africa: A randomized pilot study. BMC Medicine 5: 7.
- Roxana B, Marie H, William F, Lise G, Masako hand CM (2010) Facilitators and barriers in the humanization of childbirth practice in Japan. BMC Pregnancy and Childbirth 10: 25.
- Heather ER, Pamela FL, Catherine C, Veronica R, Jim R, et al. (2015) Direct observation of respectful maternity care in five countries: a cross-sectional study of health facilities in east and southern Africa, BMC pregnancy and childbirth 15: 306.
- Ethiopian mini demographic and health survey. Central statistical Agency Addis Ababa Ethiopia, 2014.
- Ethiopian mini demographic and health survey. Central Statistics Agency, Addis Ababa, Ethiopia, 2014.