
Journal of Electrical Electronics Engineering(JEEE)
ISSN: 2834-4928 | DOI: 10.33140/JEEE
Impact Factor: 1.2

Research Article - (2023) Volume 2, Issue 3
Knowledge Attitude and Practice about Hepatitis C Virus and Associated Factors among Waste Handlers at Public Hospitals of Sidama Region, Ethiopia: Facility Based Cross Sectional Study
Research Article J Electrical Electron Eng, 2023 Volume 2 | Issue 3 | 328; DOI: 10.33140/JEEE.02.03.16
Birhanu Betela Warssamo1* and Mehretu Belayneh2
1Department of Statistics, College of Natural and Computational Science, Hawassa University, P.O. Box, 05, Hawassa, Ethiopia
2College of Health and Medical Sciences, School of Public Health, Hawassa University, P.O. Box, 05, Hawassa, Ethiopia.
*Corresponding Author : Birhanu Betela Warssamo, Department of Statistics, College of Natural and Computational Sciences, Hawassa University.
Submitted: 2022, Aug 11; Accepted: 2022, Sep 23; Published: 2023, Sep 19
Citation: Warssamo, B. B., Belayneh, M. (2023). Knowledge Attitude and Practice about Hepatitis C Virus and Associated Factors among Waste Handlers at Public Hospitals of Sidama Region, Ethiopia: Facility Based Cross Sectional Study. J Electrical Electron Eng, 2(3), 317-327.
Abstract
Background: Hepatitis C (HCV) is worldwide community health problem that gives rise to liver cancer. Even though prevalence of HCV is higher and waste handlers being at high risk for HCV, there is scarcity of information on knowl- edge, attitude and practice (KAP) concerning HCV among waste handlers.
Methods: Quantitative cross-sectional study from Oct 2021 to 30 July 2022 in different public Hospitals of Sidama Region aimed to evaluate KAP of HCV among randomly selected waste handlers was undertaken amongst 282 respon- dents. KAP regarding HCV were assessed using standardized structured questionnaire. Descriptive summary measures were done. Multivariate logistic regression was accompanied with 95% confidence interval and P-value < 0.05 was confirmed statistically significant. To assess the association between the KAP, Spearman’s rho correlation were used.
Results: Mean scores for KAP were 22.24±8.15, 46.75±10 and 4.19±1.72 respectively. Educational level (OR = 2.427; 95% CI = [1.116 –37.89], P = 0.042), monthly income (OR = 1.001; 95% CI = [1.000–10.002], P = 0.029), use of media (OR = 2.461; 95% CI = [2.688–8.799], P = 0.006), marital status (OR = 22.961; 95% CI = [1.203–38.157], P = 0.037) and residence (OR = 6.332; 95% CI = [1.703–23.544], P = 0.006) contributed significantly to the prediction of knowledge. Spearman rank correlation revealed significant positive correlations between knowledge-attitude (r = 0.57, P < 0.037), knowledge-practice (r = 0.265, P = 0.00) and attitude-practice (r = 0.72, P = 0.02).
Conclusions: Although the study highlighted optimal KAP with regards to several aspects of HCV, educational cam- paigns should emphasize the necessity of continued education about HCV in order to more improve attitudes, knowl- edge and practices of waste handlers regarding HCV.
Keywords: Hepatitis C, KAP, Waste Handler
1. Introduction
Inflammation of the liver has historically been regarded as hepatitis, and eleven viruses are associated with hepatitis in humans with nine being hepatotrophic and two, transient in nature [1]. Hepatitis B (HBV) and C viruses’ infection pose a major public health challenge globally and has been reported by [2] to be more prevalent in the developing countries. Globally, it has been reported that about two billion people are infected with hepatitis C virus and approximately 350-400 million others suffer from the chronic form [3].
The way of transmission of the infection is largely via insecure sex, mama-to-child transmission, polluted blood and blood products and use of polluted tools, contact with infected body solutions such as blood, semen, and percutaneous injuries [4]. Wrong management of wastes created in the course of healthcare activity carries a great risk of environmental threats and community health risks [5]. Work-related contacts to percutaneous needle sticks hurts during isolation, causes a risk of work-related transmission of blood borne pathogens such as hepatitis B virus (HBV) and hepatitis C virus (HCV) particularly among waste handlers [6].
WHO estimates that there are 350 million people with chronic HCV infection worldwide? HBV is estimated to result in 563,000 deaths annually [7]. Hepatitis B virus infection is the major global health problem. About 60,000 deaths occur globally every year as a result of HBV. Chronic Hepatitis B is leading causes of cirrhosis and Hepatocellular carcinoma (HCC) which is considered as the third Cancer associated cause of deaths worldwide. WHO estimated that the prevalence of infection in Africa is on average more than 10%. However, a study conduct on Addis Ababa showed that the mean prevalence of HBsAg was 6.1 percent [8]. Hepatitis has no symptoms, so infected people pass it on other without knowing. The majority of infected persons might not be aware of their infection because it mimics a typical illness and the co-infected stigma attached to the disease prompts secrecy resulting in no treatments.
Waste handlers are greatly participate in health care waste management including waste segregation, transportation, storage, treatment, and final disposal of all types of waste generated in the health care facilities that require a high standard of training [9,10]. High prevalence of HBV infection occurred in public health center cleaners and exposure increased with the amount of waste generated that increase [11].
Regardless of nationwide and worldwide efforts to lessen or reduce professional hazard via raising awareness and looking for solutions to the complications associated with healthcare waste management for several years, health care waste management was unsuccessful and health care workers particular waste handlers are continuing to be at increased risk of HCV infection [12]. Studies from developed countries have shown that professional exposure to waste may result in HCV infection [13]. Recently a study from the UK reported 40 incidents of sharps injuries associated with waste handling [14]. In Africa, some investigators accept 5% of all HIV infections are due to unsafe injections of which unsafe waste disposal is a component [15]. There is limited data about level of knowledge, attitude and practice of waste handlers toward HCV and its associated factors in Sidama region, Ethiopia. Therefore, this study was conducted to identify level of knowledge, attitude and practice (KAP) among waste handlers in different public hospitals of Sidama National and Regional State (SNRS) and identify associated factors.
2. Methods and Materials
2.1 Study Design and Setting
A facility-based cross-sectional quantitative study was conducted in different governmental hospitals found in SNRS, Ethiopia from Oct 2021 to 30 July 2022. According to the information found from the respective health offices, there were around 4 hospitals.
2.2 Data Collection and Data Quality Control
A pretested structured questionnaire was used for data collection from waste collectors. The questionnaire was settled after studying diverse literature and pretested on 8% of sample size working at hospitals, which were not included in the study. The questionnaire was converted to local language (Sidamic and Amharic). In data collection, the data was checked for its completeness each day by supervisors and investigators after it was collected.
2.3 Sampling Design
The sampling technique used for this data collection was stratified sampling where stratification was based on the geographical proximity/location of hospitals and the strata uses for this study was hospitals in selected cities of Sidama region administrations.
2.4 Target Population
Waste handlers from different public hospitals in SNRS including workers who clean the class rooms, administrative staffs, dining room, residence house, and handle non clinical wastes generated from this compounds like: dusts particles, leftover foods dead plant tissues and other non-clinical wastes. Participation in this study was based on voluntary base and all the respondents were given informed written consent.
2.5 Sample Size Determination
The appropriate sample size used for this study was obtained using the following formula [16].
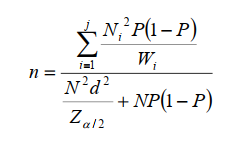
The probability of successes is considered 0.2. The level of precision preferred for this study was 3%. The desired sample size from the target population was 256 study subjects. With additional assumption of 10 percent non-response rate, the total sample size becomes 282
2.6 Data processing and Analysis
Gathered data was go in to SPSS version 20 statistical packages for analysis. Descriptive statistics were made using frequency table, percentage, mean and standard deviation. Pearsons chi-square and likelihood ratio test were used to assess factors of association.
The variables with a p-value of less than 0.05 in the bivariate analysis were included in the multivariable analysis. Multivariable logistic regression (adjusted odds ratio with 95% confidence interval) analysis was used to find explanatory variables associated with knowledge adjusting for other variables. Model fitness was checked using Hosmer Lemeshow goodness of fit and variables with P-value < 0.05 at 95% CI was professed statistical significance.
2.7 Ethical Consideration
Ethical clearance (IRBH/258/2022) was obtained from Institutional Review Board at Hawassa University College of Medicine and Health Sciences. The purpose and importance of the study was explained and informed written consent was secured from each participant.
3. Result
3.1 Socio-Demographic Characteristics of the Study Participants
A total of 282 (100%) waste collectors have participated in this study. 246 (87.2%) participants were females. The mean age of the study participant was 37.13 years with standard deviation of 14.42. The majority (60.3%) of the study participants were married whereas the mean years of service was 8.01 years with standard deviation of 4.59 (Table 1).
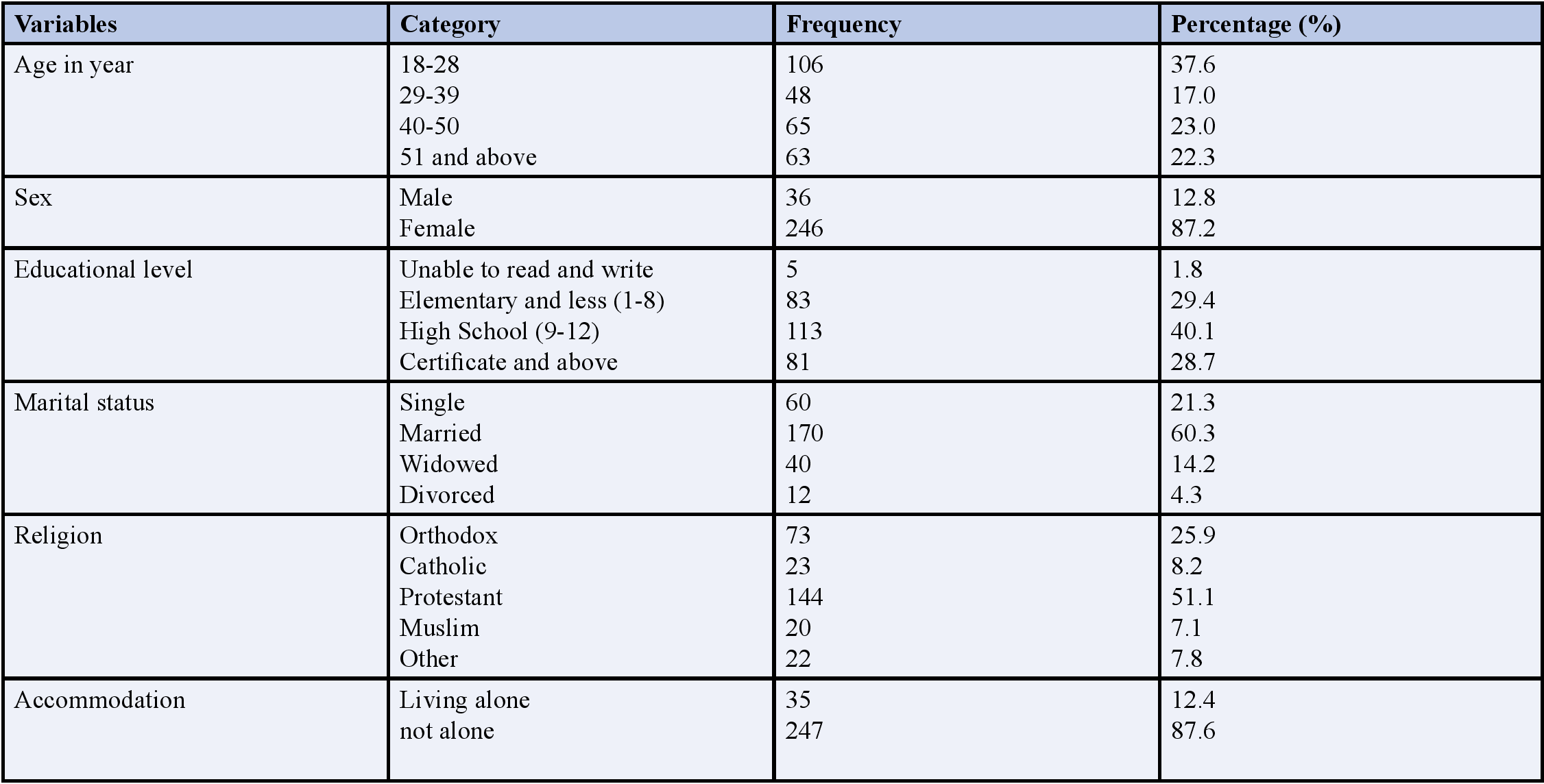
Table 1: Socio Demographic Characteristics the Study Participants in Public Hospitals in Sidama region, Ethiopia, 2022 (n=282)
The average hepatitis C knowledge score was 22.24 (SD = 8.15, min = 0, max = 35). Out of 282 participants, 97.2% heard about hepatitis and 94.3% heard about hepatitis C virus. Almost more than eighty-one percent of the total participants (81.6%) knew that hepatitis is epidemic. 85.8% knew that hepatitis C could affect any age group. About 74.8% of the respondents knew that nausea, jaundice, vomiting, joint pain and abdominal pain are symptoms of hepatitis C virus. More than 70% of the respondents knew that loss of appetite and dark urine are symptoms of hepatitis C virus. Only 65.2% of the respondents knew that though someone is infected with the diseases, symptoms might not be seen. More than 75.9% of the respondents knew that the diseases are transmitted by contaminated blood. The misconception that close personal contact for example living in the same house hold, sharing foods and drinks can spread hepatitis C is shared by 62.4% of the respondents and 200 (70.9%) of the participant wrongly believe that hepatitis B vaccine can prevent hepatitis C transmission. About 64.9% of the respondents were aware that hepatitis C infections are curable or treatable (Table 2).
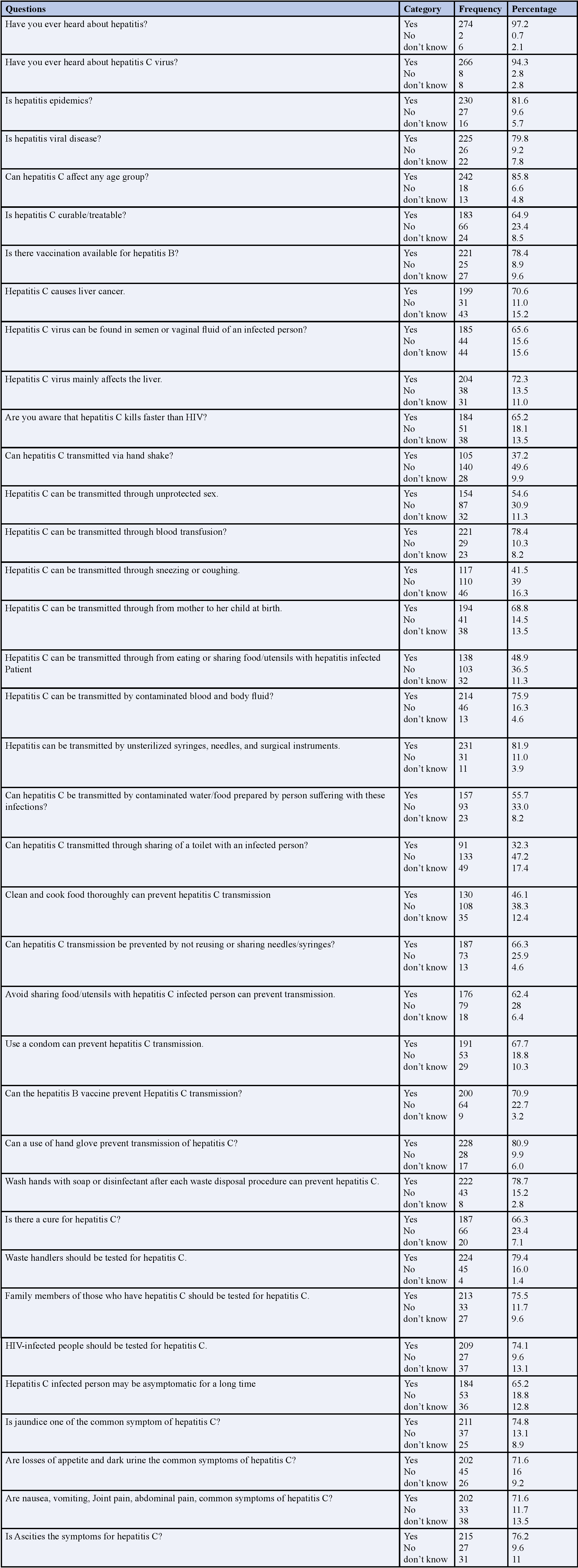
Table 2: Waste Handlers Responses to Questions Regarding Knowledge of Hepatitis C in public Hospitals in Sidama region, Ethiopia, 2022 (n=282)
There is low level (44%) of testing/screening practice among the respondents. Only 40.4% of the study participants’ changes glove during waste collection. Although 70.9% of the participants reported they were exposed to blood, only 50% take immediate action after blood exposure. Although more than 78% of the respondents reported that they faced needle stick injury, only 49.3% report for needle stick injury and only 34.8% are tested after needle stick injury.
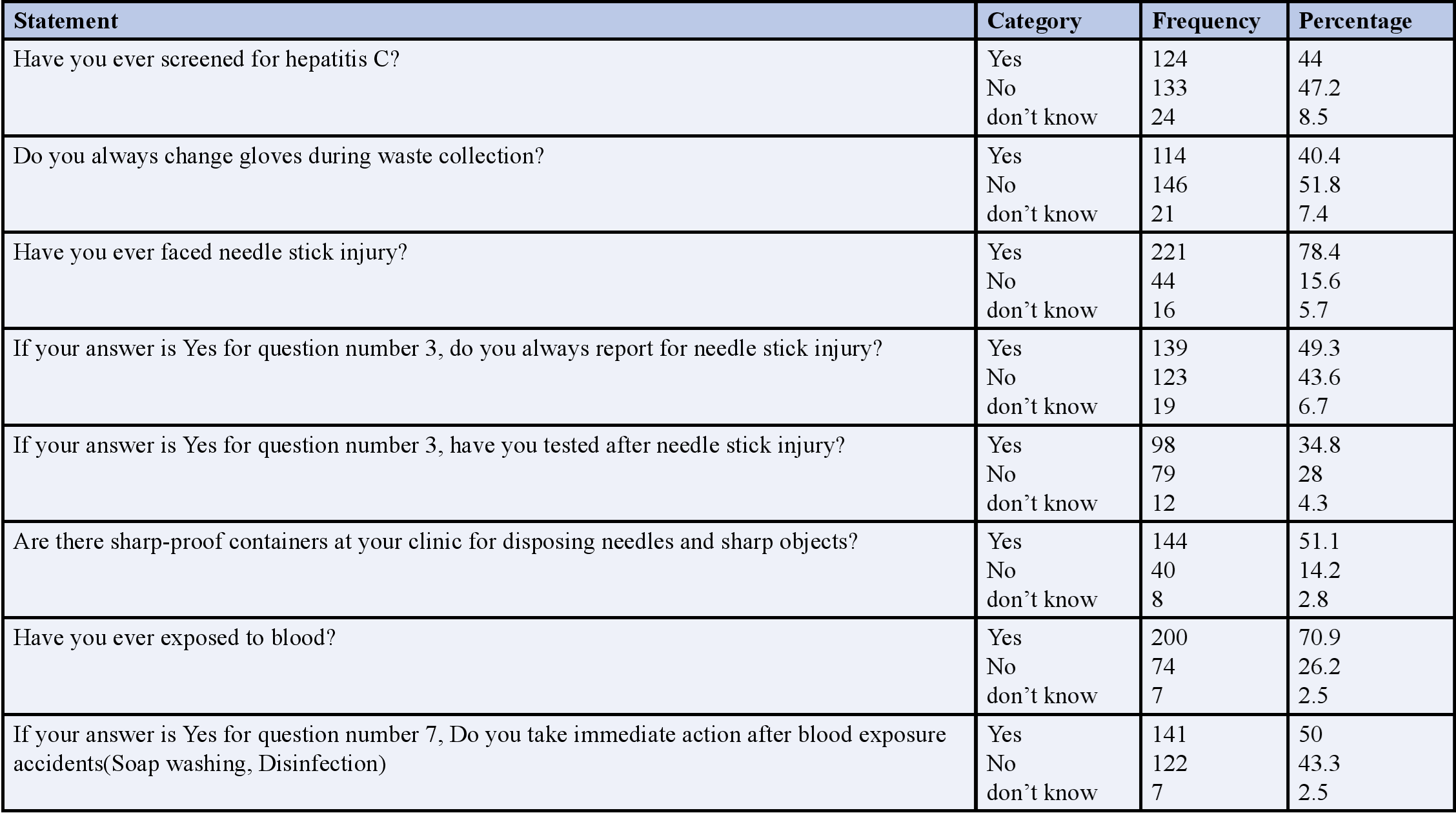
Table 3: Waste handlers practice towards hepatitis C in public Hospitals in Sidama region, Ethiopia, 2022 (n=282)
We employed eighteen questions to assess attitude of respondents toward hepatitis C. Each of the respondents was asked to give ratings for each question (measures). From the results we can see that among respondents included in this study, 126 (44.7%) of them strongly agree that their job put them at greater risk of hepatitis infection while 10 (3.5%) them strongly disagree that their job put them at greater risk of hepatitis C infection. 83 (29.4%) of the respondents strongly agree that hepatitis B vaccine is very effective to prevent hepatitis C and none of the respondents disagree that hepatitis B vaccine is effective to prevent the infection. Among the respondents in this study 30 (10.6%) strongly disagree and 27 (9.6%) disagree that wearing gloves is important to prevent transmission of hepatitis C while 162 (57.4%) agree and 19 (6.7%) strongly agree that wearing glove can prevent transmission of hepatitis C infection. Among the study subjects 73 (25.9%) of them strongly disagree and 73 (25.9%) disagree that working with hepatitis infected person in the same working place dangerous while 39 (13.8%) strongly agree and 88(31.2%) agree that working in the same place with hepatitis C infected person is dangerous (Table 4).
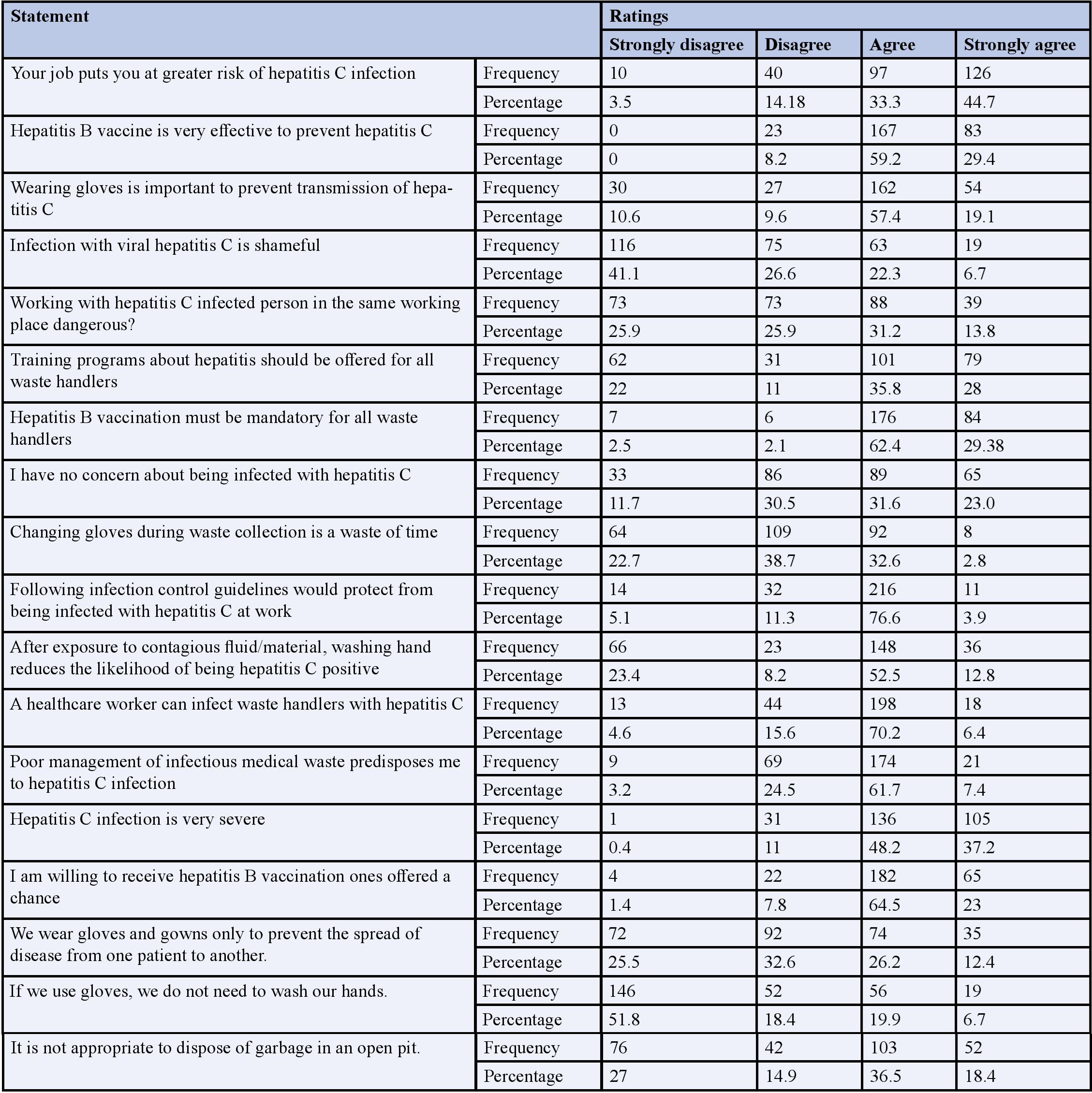
Table 4: Waste handlers attitude toward hepatitis C at different government hospitals of Sidama region, Ethiopia, 2022 (n=282)
Spearman rank correlation revealed significant positive correlations between knowledge attitude (r = 0.57, p = 0.037), knowledge-practice (r = 0.265, p = 0.00) and attitude practice (r = 0.72, p = 0.02) Table 5.
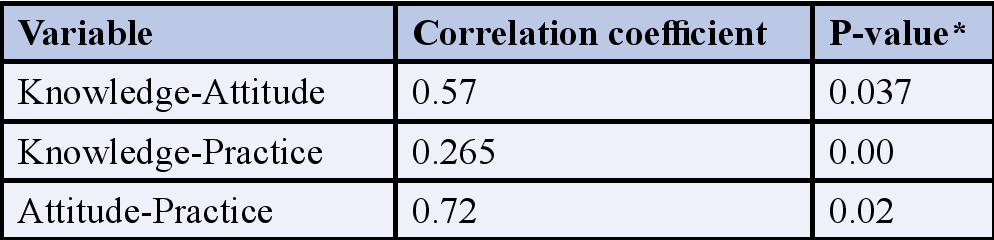
Table 5: Correlation between KAP
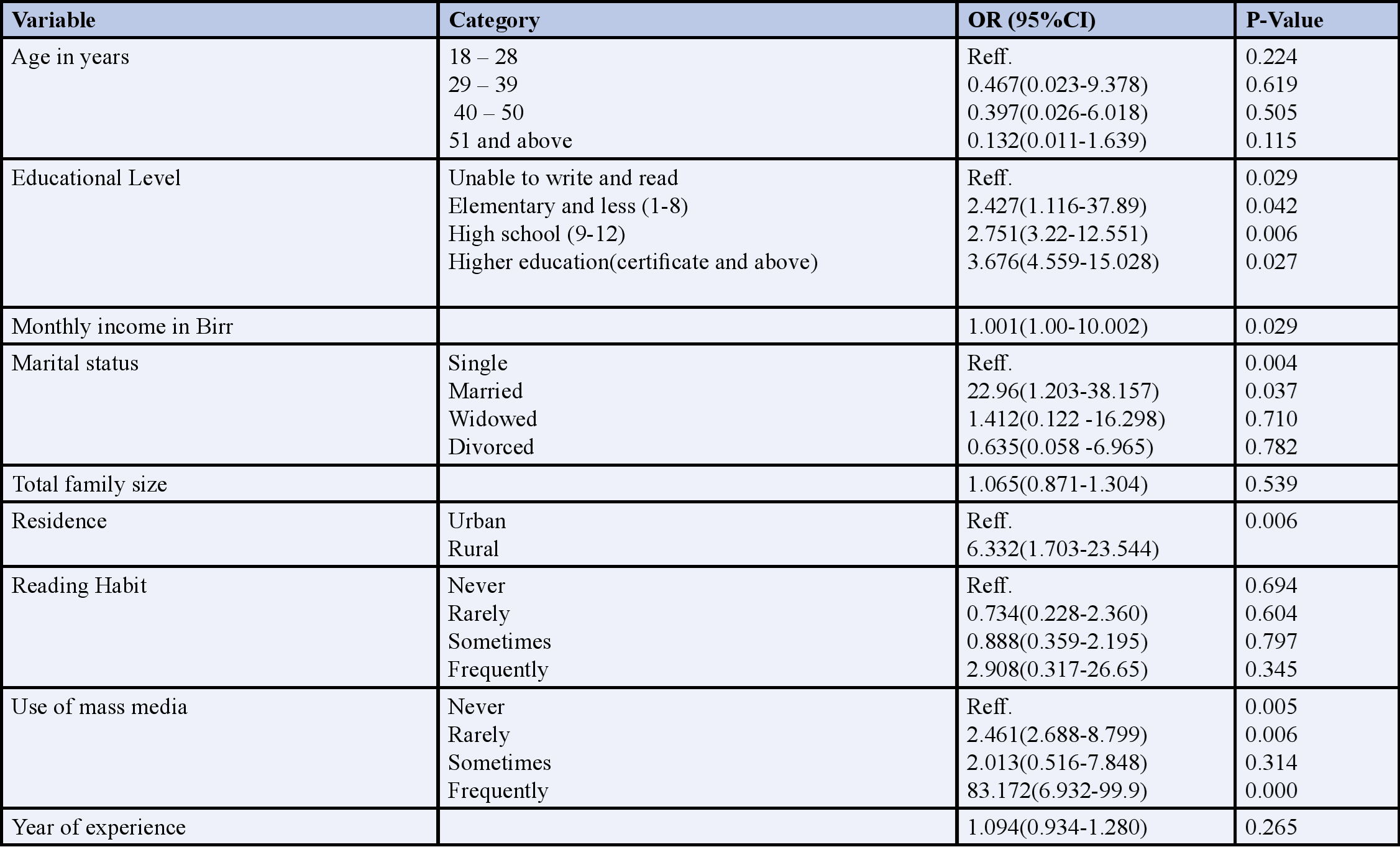
Table 5: Association of Explanatory Variables with Knowledge Level of Waste Handlers at Government Public Hospitals at Sidama Region, Ethiopia, 2022 (n=282)
Odds of knowledge of waste handlers whose educational level was elementary and less are increased by the factor 2.427 times as compared with reference category with P= 0.042 which was statistically significant. And odds knowledge was increased by the factor 2.751 times and 3.676 times for respondents whose educational level was high school and higher education with P= 0.006 and 0.027 respectively which were statistically significant (Table 5).
4. Discussion
HCV is one of the most significant occupational infection that waste handlers may face, as they are repeatedly exposed to blood and blood products, body fluids, saliva, and even suffer nee¬dle stick injuries [17]. Accordingly, in order to redu¬ce or stop the distribution of such infection to waste handlers, infection control strategies should be practical. This study was conducted to assess the level of knowledge, attitudes, and practice among waste handlers at different governmental hospitals in SNRS.
Overall, waste handlers in this study showed adequate knowledge (63.5%), positive attitude (54.3%) and good practice (69.5%) toward hepatitis C. Comparable results were also reported in other studies [18]. Based on the results of this study, we can deduce that waste handlers have a satisfied level of knowledge regarding HCV infection above 63%. This is in an agreement with some other studies that showed satisfied level of knowledge among waste handlers regar¬ding HCV infection [19].
In a study conducted by [20] about 81.7% of the study subjects knew about the likelihood of HCV transmission via contaminated blood and body fluid, while in our study the figures were lower 75.9%. The vast majority of our study subjects knew vaccination availability for hepatitis B (78.4%). This result is much lesser than the result (95.1%) Among waste handlers in Al Jouf province in. This may reflect the importance of constant medical education programs in improving the health behaviors of waste handler workers [20].
The result of the this study showed a low rate (44%) of HCV screen practice for hepatitis C. which could be an indication to, HCV screening is not mandatory requirement by the waste handlers in public hospitals in different part of SNRS. This rate is much lower to that reported by other studies in UAE (98.8%), Brazil (90.8%) and Canada (100%) and Saudi Arabia (90%) [21]. However, this rate is higher than that reported in other studies reported in India (38%) [22].
The positive correlations between knowledge-attitude, knowledge-practice and attitude practice in this study confirm the relationship between knowledge attitude and practice with infection control measures. It is concluded that satisfactory knowledge can bring about a positive attitude, which leading to good practices. The findings are consistent with the results of some other studies [23].
The present results showed that 157 (55.7%) of the participants thought incorrectly that HCV can be transmitted by contaminated water/food prepared by person suffering with these infections, similarly another study conducted on Vietnamese Americans on knowledge and the prevalence of hepatitis C showed that there was a inadequate knowledge about HCV, 32.9% thought incorrectly HCV transmitted by contaminated water/food prepared by person suffering with these infections. The results also showed that there was a lack of knowledge regarding the treatment, 42.7 % knew that there was treatment for HCV [24]. Contrary, the current study found that the majority of the respondents 183 (64.9%) knew that there was treatment for HCV.
Another study done by Gürakar, Idilman, Keskin and Malik in Turkey reported that 60% of the study subjects had knowledge that hepatitis C was a transmissible infection and a major cause of serious liver cancer. This study showed more knowledge that 199 (70.6%) of respondents knew that HCV was a major cause of serious liver cancer and had adequate knowledge 230 (81.6%) that hepatitis is epidemics. This may be because the hospitals deliver different training for waste handlers at different time [25].
The study findings posited that the level of knowledge was not significantly associated with age and gender but it was significantly associated with education level of an individual. A study conducted among waste handlers in two maternity hospitals in Khartoum, Sudan on the contrary showed that the level of knowledge was not significantly associated with educational level [26]. The differences may be due to the inclusion of a wider range of education level from illiteracy to tertiary in the current study compared to mentioned study, which focused on waste handlers, which have all attained tertiary education.
In this study, 86 (30.5%) of the study participates showed bad practice and 196 (69.5%) showed good practice. 124 (44%) had screened for hepatitis C, 114 (40.4%) always change gloves during waste collection and 139 (49.3%) report for needle stick injury. The findings were much higher than the findings reported by which showed that 20.3% of study participants had good practice and 85.9% had not screened for HCV. Another study conducted in Honiara, Solomon Islands, in 2015 showed that 26.3% of study participants had good practice [27, 28]. This good practice in the current study could be as results of adequate of knowledge of respondents on HCV 179 (63.5%).
The results of this study showed that the respondents that had positive attitude towards hepatitis C is 153 (54.3%) and 129 (45.7%) of the respondents had negative attitude. In this study 220 (78.01%) of the respondents reported that they believe that they were at risk of contracting HCV by virtue of their work as waste handlers. 247 (87.5%) were approved to receive hepatitis vaccination ones offered a chance. These findings were slightly lower than a study findings done by which found that the respondents had good attitude (91%) and 82.7% were willing to get vaccinated [26].
The findings of the current study was consistence with study conducted in Ethiopia on pregnant women attending antenatal care at the University of Gondar comprehensive specialized hospital which reported 54% had positive attitude [27]. In addition, a study conducted in Bangladesh in 2012 showed that 50% of study participants had positive attitude. Having a positive attitude means that respondents may be willing to take preventive measures to help combat HCV infection. This willingness was seen in this study as 180 (63.8%) of the respondents proved to take training about HCV.
4.1 Limitations of the Study
Besides, data on knowledge, practice and attitude were self-reported; it could be subject to individual bias. Although this study provides some very useful information on hepatitis C to waste handlers, the limitations include; lack of focused group discussion and in-depth interviews may diminish the transferability of the findings. Further research in this respect could be very useful.
5. Conclusions
There was adequate knowledge, attitude and practice among waste handlers at different government hospitals of Sidama region, Ethiopia compared to other studies. Educational level, monthly income, use of media, marital status and residence were significant factors associated with knowledge of waste handlers toward HCV. HCV related inadequate of knowledge on mode of transition and prevention can be contributory towards increasing frequency of HCV. Hence, educational campaigns among waste handlers should be intensified with focus being on attitude change and behavior modification. There was less level of screening practice among the participants, thus governments should make screening programs for the infection free of charge. The result of this study showed the majority of the participants had more than average knowledge on hepatitis C virus. The result showed a significant difference between the knowledge with attitude. Those who had knowledge had good attitude and practice. The practice aspect of HCV was generally good and this was as a result of respondents had adequate knowledge about how to fully protect oneself from acquiring HCV. Therefore, improving more than the knowledge obtained in this study about HCV can contribute to improve the waste handlers’ health by getting lower rate of cases with HCV. HCV practices as a performed conduct were influenced by the attitude of the waste handlers towards HCV. Therefore, it is concluded that adequate knowledge leads positive attitude, which in turn results in a positive change in the practices of waste handlers.
Authors’ Contributions
B.B conceived the study and drafted the proposal and had substantial contributions to the study design and development of the data collection checklist. M.B drafted the manuscript, wrote, and corrected the manuscript. All authors read the manuscript and approved it.
Funding
Research Affairs Office of Hawassa University funded this work.
Availability of Data and Materials
Most of the data analyzed during this study are included in this article. The full datasets used and/or analyzed during the current study is available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study protocol was approved by Institutional Health Research Ethics Review Committee (IHRERC) of Hawassa University, College of Health and Medical Sciences (CHMS) (Reference number: IHRERC/127/2021) and permission for study proceeding was accepted by respective health institutions. All methods were carried out in accordance with relevant guidelines and regulations of Hawassa University. Thus, informed, written and signed consent was obtained from each participant. Consent to participate from study subjects were written and signed individually on hard copy.
Competing Interests
The authors declare that they have no competing interests.
References
- Mboto, C. I., & Edet, E. J. (2012). Prevalence and risk factors of hepatitis B virus infection among students in University of Uyo. International Journal of Modern Biology and Medicine, 2(2), 101-111.
- Ott, J. J., Stevens, G. A., Groeger, J., & Wiersma, S. T. (2012). Global epidemiology of hepatitis B virus infection: new estimates of age specific HBsAg seroprevalence and endemicity. Vaccine, 30(12), 2212-2219.
- Portilho, M. M., Martins, P. P., Lampe, E., & Villar, L. M. (2012). A comparison of molecular methods for hepatitis B virus (HBV) DNA detection from oral fluid samples. Journal of Medical Microbiology, 61(6), 844-851.
- Eke, A. C., Eke, U. A., Okafor, C. I., Ezebialu, I. U., & Ogbuagu, C. (2011). Prevalence, correlates and pattern of hepatitis B surface antigen in a low resource setting. Virology journal, 8(1), 1-8.
- Amsalu, A., Worku, M., Tadesse, E., & Shimelis, T. (2016). The exposure rate to hepatitis B and C viruses among medical waste handlers in three government hospitals, southern Ethiopia. Epidemiology and health, 38.
- Alter, M. J. (2006). Epidemiology of viral hepatitis and HIV co-infection. Journal of hepatology, 44, S6-S9.
- Abel, G., & Solomon, G. S. (2012). Sero-prevalence of HBV and HCV among chronic liver disease patients visiting OPD in public hospitals in Addis Ababa. ISRN, 2013(563821), 1-7.
- Abebe, A., Nokes, D. J., Dejene, A., Enquselassie, F., Messele, T., & Cutts, F. T. (2003). Seroepidemiology of hepatitis B virus in Addis Ababa, Ethiopia: transmission patterns and vaccine control. Epidemiology & Infection, 131(1), 757-770.
- Farzadkia, M., Moradi, A., Mohammadi, M. S., & Jorfi, S. (2009). Hospital waste management status in Iran: a case study in the teaching hospitals of Iran University of Medical Sciences. Waste Management & Research, 27(4), 384-389.
- Harhay, M. O., Halpern, S. D., Harhay, J. S., & Olliaro, P. L. (2009). Health care waste management: a neglected and growing public health problem worldwide. Tropical Medicine & International Health, 14(11), 1414-1417.
- Debere, M. K., Gelaye, K. A., Alamdo, A. G., & Trifa, Z. M. (2013). Assessment of the health care waste generation rates and its management system in hospitals of Addis Ababa, Ethiopia, 2011. BMC public health, 13(1), 1-9.
- Otovwe, A., & Adidatimi, P. O. (2017). Knowledge, Attitude and Practice of standard precaution among health care workers in Federal Medical Centre Yenagoa, Nigeria. IOSR Journal of Pharmacy and Biological Sciences (IOSR-JPBS), 79-86.
- World Health Organization. (2000). Aide-mémoire for a national strategy for the safe and appropriate use of injections.
- Blenkharn, J. I., & Odd, C. (2008). Sharps injuries in healthcare waste handlers. Annals of occupational hygiene, 52(4),281-286.
- Crabb, C. (2003). Researchers argue that unsafe injections spread HIV more than unsafe sex. Bulletin of the World Health Organization, 81(4),307.
- Cochran, W. G. (1977). Sampling techniques. John Wiley & Sons.
- Mutters, N. T., Hägele, U., Hagenfeld, D., Hellwig, E., & Frank, U. (2014). Compliance with infection control practices in an university hospital dental clinic. GMS Hygiene and Infection Control, 9(3).
- Li, X., Kang, H., Wang, S., Deng, Z., Yang, T., Jia, Y., & Yang, Y. (2015). Knowledge, attitude, and behavior of hepatitis B virus infection among chinese dental interns. Hepatitis monthly, 15(5).
- Al-Hazmi AH. (2015). Knowledge, attitudes and practice of waste handlers con¬cerning the occupational risks of hepatitis C virus in Al Jouf Provin¬ice, Saudi Arabia. Niger J Clin Pract. 18:276-81.
- Alavian, S. M., Mahboobi, N., Mahboobi, N., Savadrudbari, M. M., Azar, P. S., & Daneshvar, S. (2011). Iranian dental students’ knowledge of hepatitis B virus infection and its control practices. Journal of dental education, 75(12), 1627-1634.
- McCarthy, G. M., & Britton, J. E. (2000). A survey of final-year dental, medical and nursing students: occupational injuries and infection control. Journal-canadian dental association, 66(10), 561-561.
- Singh, A., Purohit, B. M., Bhambal, A., Saxena, S., Singh, A., & Gupta, A. (2011). Knowledge, attitudes, and practice regarding infection control measures among dental students in Central India. Journal of dental education, 75(3), 421-427.
- Haq NU, Hassali MA, Shafie AA, Saleem F, Farooqui M,. (2012). A cross sectional assessment of knowledge, attitude and practice towards Hepatitis B among healthy population of Quetta, Pakistan. BMC Public Health.12(1):692.
- Mergler, M. J., Omer, S. B., Pan, W. K., Navar-Boggan, A. M., Orenstein, W., Marcuse, E. K., & Salmon, D. A. (2013). Association of vaccine related attitudes and beliefs between parents and health care providers. Vaccine, 31(41), 4591-4595.
- Gürakar, M., Malik, M., Keskin, O., & İdilman, R. (2014). Public awareness of hepatitis B infection in Turkey as a model of universal effectiveness in health care policy. Turk J Gastroenterol, 25(3), 304-8.
- Mursy, S. M. E. M., & Mohamed, S. O. O. (2019). Knowledge, attitude, and practice towards Hepatitis B infection among nurses and midwives in two maternity hospitals in Khartoum, Sudan. BMC public health, 19(1), 1-7.
- Gebremeskel, T., Beshah, T., Tesfaye, M., Beletew, B., Mengesha, A., & Getie, A. (2020). Assessment of knowledge and practice on hepatitis B infection prevention and associated factors among health science students in Woldia University, Northeast Ethiopia. Advances in preventive medicine, 2020.
- UNAIDs, U., & World Health Organization. (2011). Global HIV/AIDS response: epidemic update and health sector progress towards universal access: progress report 2011. Global HIV/AIDS response: epidemic update and health sector progress towards universal access: progress report 2011.
Copyright:
Copyright: ©2023 Birhanu Betela Warssamo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.