
Journal of Gynecology & Reproductive Medicine(JGRM)
ISSN: 2576-2842 | DOI: 10.33140/JGRM
Impact Factor: 1.247

Research Article - (2025) Volume 9, Issue 3
IOTA Model For Surgical Management of Ovarian Tumors: A Case From Mongolia
2Ph.D, School of Economics and Business, Mongolian University of Life Sciences Ulaanbaatar, Mongolia
Received Date: Aug 08, 2025 / Accepted Date: Sep 24, 2025 / Published Date: Sep 30, 2025
Copyright: ©2025 Ureltsetseg Batdelger, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Purev, S., Batdelger, U., Tseleejav, B., Batbayar, B., Narangerel, M., et al. (2025). IOTA Model For Surgical Management of Ovarian Tumors: A Case From Mongolia. J Gynecol Reprod Med, 9(3), 01-08.
Abstract
Preoperative assessment of ovarian pathology is crucial for ensuring that patients with ovarian cancer receive appropriate treatment and achieve optimal clinical outcomes. To facilitate this, the International Ovarian Tumor Analysis (IOTA) collaboration has developed standardized ultrasound based methods for describing adnexal lesions. Complementing imaging, frozen section histological analysis, a rapid diagnostic technique first introduced in 1905, provides results within 15–30 minutes and plays a pivotal role in intraoperative decision making, especially for reproductive age women requiring fertility preserving surgical strategies. This method has demonstrated a diagnostic accuracy of 94%, with 75% sensitivity and 100% specificity for ovarian tumors. Although ovarian cancer is relatively uncommon among women of reproductive age, it frequently presents at an advanced stage, often necessitating radical surgical intervention. Together, these preoperative and intraoperative diagnostic strategies provide a comprehensive approach for tailoring surgical management, optimizing patient outcomes, and supporting fertility preservation when appropriate.
Background: This report details a case of successful twin pregnancy following fertility sparing surgery guided by frozen section histology in a patient with bilateral mucinous borderline ovarian tumours. Fertility preserving approaches have become increasingly viable and ethically significant for younger patients desiring future pregnancy. This report presents the case of a 38 year old woman diagnosed with high grade serous ovarian carcinoma who underwent fertility sparing surgery guided by intraoperative frozen section histology; she successfully conceived and delivered a healthy child postoperatively.
Methods (Case Presentation): A 38 year old woman presented with acute left lower abdominal pain. Her reproductive history was gravida 3, para 2, with one miscarriage and no conception for the past 10 years. Imaging revealed a multiloculated, 13.6 cm left ovarian mass with vascularity and a honeycomb appearance. Her serum CA-125 level was 60 U/mL. The patient underwent laparoscopic surgery, which included a left salpingo oophorectomy, a wedge biopsy of the right ovary, an omental biopsy, and peritoneal cytology. Intraoperative frozen section analysis revealed a mucinous borderline tumour with intraepithelial carcinoma on the left ovary and mucinous borderline changes on the right. The uterus and right adnexa were preserved.
Results: Final histology confirmed a left Stage IB mucinous borderline carcinoma and a right borderline tumour. The patient subsequently completed six cycles of chemotherapy with cyclophosphamide and cisplatin. She remained diseasefree for two years and conceived spontaneously three years postoperatively. On 7 March 2025, she delivered healthy twins via emergency caesarean section at 36–37 weeks of gestation due to pre eclampsia, twin gestation, and a history of uterine scarring.
Conclusion: Intraoperative frozen section histology enables rapid and reliable assessment of ovarian malignancy, allowing surgeons to make informed fertility preserving decisions without compromising oncological safety. This case illustrates the successful application of this approach in a patient with bilateral mucinous borderline ovarian tumours, resulting in spontaneous conception and the delivery of healthy twins. Importantly, it demonstrates that fertility-sparing surgery guided by frozen section histology can be safely and effectively implemented in specialized tertiary-care hospitals in Mongolia, highlighting its potential to improve reproductive and oncological outcomes in young women with early-stage ovarian tumours. This experience provides a valuable reference for clinical practice and may support the development of national protocols for the fertility-preserving management of ovarian tumours.
Keywords
Ovarian Tumour, Fertility Preservation, Frozen Section, Borderline Tumour, Twin PregnancyIntroduction and Research Objectives
Accurate preoperative differentiation between benign and malignant adnexal masses is a cornerstone for optimal patient management. Although most women presenting with an adnexal mass do not have ovarian cancer, correctly identifying benign lesions is essential to prevent unnecessary interventions, reduce healthcare costs, and minimize patient morbidity (Bourne & Collins, 1993; Kaijser et al., 2009). Conversely, timely detection of malignant lesions enables prompt treatment and appropriate surgical staging at specialized gynecologic oncology centers, which is critical for achieving favorable oncological outcomes (Timmerman & Valentin, 2013; Valentin & Ameye, 2001). Various diagnostic tools have been developed to enhance preoperative assessment of ovarian masses. These include ultrasonography based scoring systems focusing on morphological features, serum biomarkers such as CA-125 integrated into the Risk of Malignancy Index (RMI), and more advanced computational models including logistic regression, neural networks, and other machine learning algorithms (Kaijser et al., 2009; Van Calster & Timmerman, 2011). Among these, the RMI remains the most widely applied globally, although its predictive performance is heavily influenced by serum CA-125 levels. Systematic reviews confirm that RMI provides reliable triage for referral to tertiary oncology units (Kaijser et al., 2009). Guidelines from professional bodies such as the American College of Obstetricians and Gynecologists (ACOG) recommend biomarker based assessment for determining referral to gynecologic oncology centers. However, these protocols are less effective in detecting early stage ovarian cancer and in premenopausal women. Alternative biomarkers, such as the OVA-1 panel, can improve sensitivity but are associated with high false-positive rates, limiting clinical utility (Timmerman & Valentin, 2013; Van Calster & Timmerman, 2011). Numerous other predictive models have been proposed to enhance preoperative diagnostic accuracy, yet most failed to maintain their performance during external validation. Contributing factors include limited sample sizes, single-center development, tumor heterogeneity, inconsistent ultrasound terminology, and variability in histopathological reporting (Kaijser et al., 2009; Van Calster & Timmerman, 2011). To overcome these limitations and provide a reproducible, evidence based framework applicable across diverse clinical settings, the International Ovarian Tumor Analysis (IOTA) collaboration was established. Standardized IOTA models including Logistic Regression models (LR1 and LR2) and the IOTA Simple Rules demonstrate high diagnostic accuracy and consistency, supporting preoperative risk stratification and informed surgical decision making (Timmerman & Valentin, 2013; Kaijser et al., 2009).
• Ovarian Cancer: Ovarian cancer is a malignant neoplasm originating from ovarian tissues, which are responsible for oocyte production and hormone synthesis. Histopathologically, ovarian tumors are classified into epithelial ovarian carcinoma, germ cell tumors, and sex cord stromal tumors. Epithelial ovarian carcinoma accounts for approximately 90% of cases and includes serous, mucinous, endometrioid, and clear cell subtypes. Although germ cell and sex cord stromal tumors are less common, they are clinically significant, particularly in younger women (Kaijser et al., 2009; Timmerman & Valentin, 2013).
• Fertility-Sparing Surgery (FSS) in Ovarian Cancer: Historically, early stage ovarian cancer was treated with radical surgery, including bilateral salpingo-oophorectomy and hysterectomy. Fertility sparing surgery (FSS) has since emerged as a feasible approach for women desiring future fertility. This strategy aims to remove malignant tissue while preserving reproductive organs and is particularly relevant for young women diagnosed with early stage disease (Kaijser et al., 2009; Van Calster & Timmerman, 2011).
• International Ovarian Tumor Analysis (IOTA) and Risk Stratification: The International Ovarian Tumor Analysis (IOTA) group has developed standardized preoperative risk assessment models for adnexal masses, including the Risk of Malignancy Index (RMI), Logistic Regression models (LR1 and LR2), and the Simple Rules. These tools integrate clinical, ultrasound, and biomarker data to stratify malignancy risk and guide surgical planning, including considerations for FSS (Timmerman & Valentin, 2013; Kaijser et al., 2009).
• Global Practices and Evidence Based Guidelines: In countries with advanced healthcare systems—such as Japan, South Korea, France, Italy, and Germany—IOTA models combined with intraoperative frozen section histology have become standard practice. These approaches improve oncological outcomes and support fertility preservation by enabling accurate intraoperative assessment of malignancy, thereby facilitating the safe implementation of FSS (Kaijser et al., 2009; Van Calster & Timmerman, 2011).
• Fertility Preservation in Mongolia: In Mongolia, the ap- plication of IOTA models and fertility preserving strategies remains underreported. This case highlights the first docu- mented use of IOTA in a specialized national hospital, demo strating its potential to preserve fertility and achieve success- ful childbirth. Integrating evidence based protocols such as those developed by IOTA into clinical practice could enhance patient outcomes and align local practices with international standards in ovarian cancer management (Timmerman & Val- entin, 2013).
Literature Review and Conceptual Framework
Accurate preoperative differentiation between benign and malignant adnex- al masses is critical for guiding clinical management and optimiz- ing patient outcomes. The International Ovarian Tumor Analysis (IOTA) collaboration has developed standardized diagnostic mod- els, including the Logistic Regression models (LR1 and LR2) and the Simple Rules (SR). These tools integrate clinical, ultrasound, and biomarker data to stratify malignancy risk, thereby guiding surgical decision making, including the consideration of fertili- ty-sparing surgery (Timmerman & Valentin, 2013; Kaijser et al., 2009). The diagnostic performance of these models has been val- idated by several case studies across Europe. Research from mul- tiple European centers has demonstrated that the LR1 and LR2 models achieve high diagnostic accuracy in distinguishing benign from malignant ovarian tumors, with LR2 exhibiting slightly high- er sensitivity and specificity than LR1 (Van Calster & Timmerman, 2011). The IOTA Simple Rules have also been extensively vali- dated, showing a sensitivity of approximately 90% and a specific- ity of 93%; this strong performance supports their routine use for preoperative risk stratification in European gynecologic oncology practice (Kaijser et al., 2009). Despite these strengths, some lim- itations exist. The models are applicable in only 80–85% of cases, which highlights the need for adjunctive diagnostic assessment when the rules yield an inconclusive result.
In Asia, the application of IOTA models has similarly demonstrated promising results. A prospective study in India reported that the Simple Rules were applicable in 65 out of 70 patients, achieving a sensitivity of 90.9% and a specificity of 88.4% for ovarian tumor classification (Amhsr.org, 2023). In China, combining the Simple Rules with serum CA125 and the O-RADS classification improved diagnostic accuracy, resulting in a sensitivity of 94.4% and an area under the curve (AUC) of 0.831 (Ovarian Research, 2022). These findings suggest that IOTA models are adaptable across diverse healthcare settings, although local training and standardization are crucial to maintain diagnostic reliability. The conceptual framework for IOTA model implementation centers on four key components: standardized ultrasound imaging assessment, biomarker integration, risk stratification, and clinical decision-making. Ultrasound assessment using the Simple Rules identifies morphological features predictive of malignancy, while the LR1 and LR2 models incorporate additional clinical and biomarker data—such as serum CA125—to refine risk estimates. These risk scores then inform surgical planning, including the consideration of fertility-sparing procedures, and guide patient counseling regarding optimal management strategies (Timmerman & Valentin, 2013; Kaijser et al., 2009). In summary, international case studies demonstrate that IOTA models, when properly implemented, enhance preoperative diagnostic accuracy, improve oncological outcomes, and support fertility-preserving interventions. Comparative evidence from Europe and Asia highlights that although the models perform consistently across diverse populations, integration with biomarkers and training in standardized ultrasound evaluation are essential for maximizing their clinical utility. This evidence-based framework underscores the value of IOTA models in preoperative assessment and provides a foundation for their application in emerging clinical settings, including Mongolia. The integration of such protocols could align local practices with global standards in ovarian cancer management

Source: (Kaijser et al.,2013)
Figure 1: International Ovarian Tumor Analysis (IOTA) framework
Case Study Methods
Patient Presentation and Clinical History: A 38 year old woman presented with acute left lower abdominal pain. Her obstetric history was gravida 3, para 2, with one miscarriage and a 10 year history of infertility. She had no significant comorbidities or prior gynecologic surgeries. Physical examination revealed a palpable mass in the left lower abdominal quadrant. Transvaginal ultrasonography identified a 13.6 cm multiloculated left ovarian mass with internal vascularity and a honeycomb pattern. The right ovary was unremarkable. Serum CA-125 was elevated at 60 U/mL; other laboratory values were within normal limits. Surgical Intervention and Intraoperative Assessment: Laparoscopic surgery was performed, which included a left salpingo oophorectomy, a wedge biopsy of the right ovary, an omental biopsy, and peritoneal cytology. Intraoperative frozen section analysis revealed a mucinous borderline tumor with intraepithelial carcinoma on the left ovary and mucinous borderline changes on the right. To preserve fertility, the uterus and right adnexa were preserved. Final histology confirmed a Stage IB mucinous borderline carcinoma of the left ovary and a borderline tumor on the right. Postoperative Course and Outcome: The patient subsequently completed six cycles of adjuvant chemotherapy with cyclophosphamide and cisplatin. She remained disease free throughout two years of surveillance. Three years postoperatively, the patient conceived spontaneously and delivered healthy twins via emergency cesarean section at 36–37 weeks of gestation due to pre-eclampsia and a history of uterine scarring. Informed consent was obtained from the patient for both treatment and publication of this case. All study protocols adhered to the principles of the Declaration of Helsinki and were approved by the institutional ethical review board.
Case Report
Mucinous ovarian tumors represent a subset of epithelial ovarian neoplasms that, when detected at an early stage, may allow for fertility preserving surgical management. Careful preoperative assessment, intraoperative decision making, and postoperative follow up are critical for balancing oncologic safety with reproductive outcomes. This case report describes a patient with Stage IB mucinous ovarian carcinoma who was managed with fertility sparing surgery and subsequently achieved a successful twin pregnancy.
Case Presentation
A 38 year old woman, gravida 4 para 3 (deliveries in 2008, 2011, 2012, and 2024), presented with severe left lower quadrant abdominal pain. Her medical history was notable for two prior cesarean sections (2008 and 2011) and a left oophorectomy (2021). Her body mass index was 34.9 kg/m² (weight 95 kg, height 165 cm).
|
Parameter |
Unit |
Reference Range |
2024/12/31 |
2025/01/03 |
2025/03/05 |
2025/03/08 |
|
WBC |
109/L |
4–10 |
13.60 H |
11.45 |
7.57 |
12.04 |
|
RBC |
10¹²/L |
3.5–5.5 |
3.39 L |
3.40 |
4.09 |
3.93 |
|
HGB |
g/dL |
11.5–16.5 |
10.6 L |
10.4 |
11.8 |
11.4 |
|
HCT |
% |
35–50 |
29.3 L |
29.4 |
33.9 |
32.7 |
|
MCV |
fL |
75–100 |
86.4 |
86.5 |
82.9 |
83.2 |
|
MCH |
pg |
25–35 |
31.3 |
30.6 |
28.9 |
29.0 |
|
MCHC |
g/dL |
31–37 |
36.2 |
35.4 |
34.8 |
34.9 |
|
RDW-SD |
fL |
35–56 |
40.4 |
40.9 |
42.3 |
43.0 |
|
RDW-CV |
% |
11.5–14.5 |
12.7 |
12.8 |
13.7 |
14.1 |
|
PLT |
109/L |
150–400 |
277 |
271 |
262 |
229 |
|
MPV |
fL |
7–12 |
9.3 |
9.4 |
9.3 |
9.6 |
|
PCT |
% |
0.108–1.282 |
0.26 |
0.26 |
0.24 |
0.22 |
|
PDW |
fL |
9–17 |
10.1 |
10.4 |
9.8 |
10.2 |
|
LYMPH |
% |
15–40 |
10.5 L |
11.4 |
11.8 |
6.0 |
|
MONO |
% |
2–9 |
7.7 |
7.9 |
10.2 |
9.0 |
|
NEUT |
% |
35–70 |
79.6 H |
78.3 |
75.7 |
84.1 |
|
EO |
% |
0–5 |
1.8 |
2.0 |
1.8 |
0.7 |
|
BASO |
% |
0–1 |
0.4 |
0.4 |
0.5 |
0.2 |
|
LYMPH # |
109/L |
1.02–3.18 |
1.43 |
1.31 |
0.89 |
0.72 |
|
MONO # |
109/L |
0.1–0.8 |
1.05 H |
0.90 |
0.77 |
1.08 |
|
NEUT # |
109/L |
35–70 |
7.96 H |
8.96 |
5.73 |
10.12 |
|
EO # |
109/L |
0–0.44 |
0.24 |
0.23 |
0.14 |
0.09 |
|
BASO # |
109/L |
0.01–0.2 |
0.05 |
0.05 |
0.04 |
0.03 |
![]()
Table 1: Hematological Parameters of the Patient Over Time
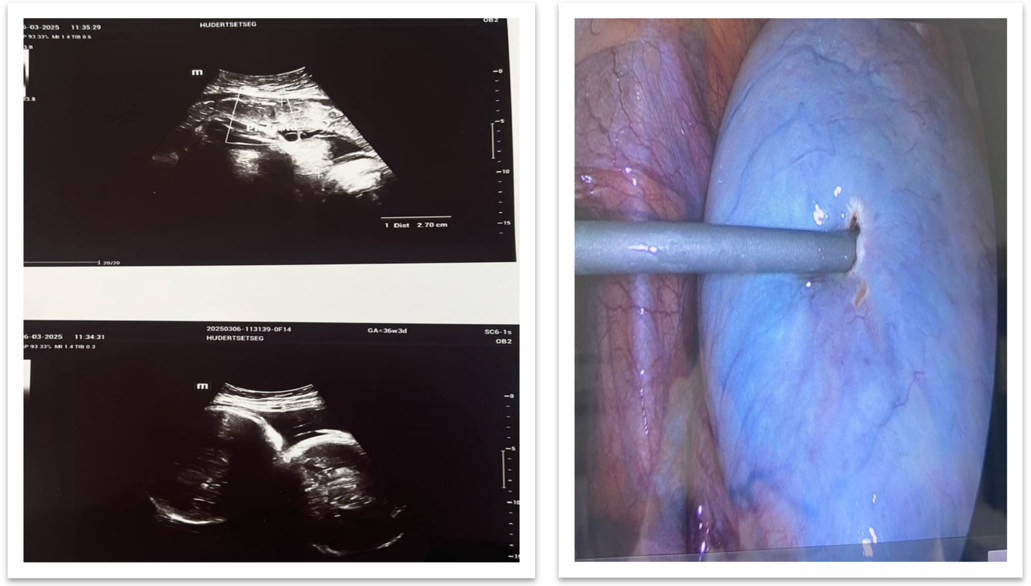
Figure 2: Ultrasound image Figure 3: The surgical procedure
Diagnostic Assessment: Pelvic ultrasound demonstrated a multilocular mass measuring 13.6 × 10 × 9.7 cm with honeycomb- like septations and increased vascularity. Laboratory evaluation revealed an elevated CA-125 level (60 U/mL) and an elevated Inhibin B level (58.24 pg/mL); lactate dehydrogenase (LDH, 300 U/L) and alpha-fetoprotein (AFP, 4.9 U/mL) were within normal limits. Endoscopy and chest radiography showed no evidence of metastasis. Preoperative risk assessment using the International Ovarian Tumor Analysis (IOTA) criteria indicated a high malignant potential. The IOTA Simple Rules identified multilocularity, solid components, and increased vascularity as suspicious features, while the ADNEX model estimated a high probability of a borderline or malignant ovarian tumor.
The patient conceived spontaneously three years after surgery. Prenatal care commenced at 6–7 weeks of gestation, and she underwent six routine antenatal assessments. Early pregnancy nausea persisted until the fourth month. At 27–28 weeks, she developed mild preterm labor with a risk of premature birth; her history of two prior cesarean sections and uterine scarring was noted. At 34–35 weeks, she experienced elevated blood pressure, and the previously noted uterine scarring remained a consideration; twin gestation (dichorionic, two placentas, two amniotic sacs) was confirmed. At 36–37 weeks, mild preterm contractions recurred. Throughout the pregnancy, her blood pressure remained stable (~120/80 mmHg), and she gained 15 kg. Chronic comorbidities included mild cardiac symptoms, recurrent pharyngitis, and untreated dental caries. Medications included vitamin D (4000 IU), aspirin (150 mg), calcium D3, methyldopa (250 mg), and supplemental oxygen as needed.
On 5 March 2025, she presented with abdominal tightening and headache; her blood pressure was 131/88 mmHg (right arm) and 129/88 mmHg (left arm), and urinalysis revealed proteinuria (100 mg/dL). She was admitted for a planned cesarean delivery at 36–37 weeks due to mild preterm contractions, prior uterine surgery, and twin gestation. 3.2.4. Delivery and Outcome:
• First twin: 08:54, female, 2800 g, 48 cm, Apgar 7/8
• Second twin: 08:56, male, 3050 g, 49 cm, Apgar 7/8
Placental Findings: The placentas were intact with a combined weight of 610 g and a thickness of 1.9 cm; the diameter measured 18 × 21 cm. The umbilical cord had a central insertion and was 50 cm in length. The estimated blood loss during surgery was 500 mL. Postoperatively, both the mother and neonates remained stable. The patient was monitored in the postpartum ward for 72 hours and was subsequently discharged in good condition.
Final Histology:
• Left ovary: Stage Ib mucinous ovarian carcinoma
• Right ovary: Borderline mucinous tumor

Figure 4: Postoperatively, two viable twins were delivered without complications
Discussion
This case demonstrates the role of IOTA-based evaluation in guiding intraoperative decision making and enabling fertility-preserving surgery in early stage ovarian cancer. Interna- tional studies confirm that IOTA enhances diagnostic accuracy, reduces overtreatment, and supports tailored surgical strategies [1-4]. In European cohorts, the use of IOTA combined with fro- zen section histology achieved disease-free survival (DFS) rates of >95% in Stage I borderline ovarian tumours, outcomes com- parable to standard radical surgery, while preserving reproductive potential [5,6]. Similarly, Asian studies show improved reproduc- tive outcomes and reduced recurrence following fertility-sparing surgery (FSS) when guided by IOTA [2,7]. The present case is the first report from Mongolia demonstrating a successful pregnan- cy and live twin birth following IOTA-guided FSS. It highlights the potential to integrate evidence-based diagnostic models into national oncology practice, ensuring both oncological safety and reproductive health.
Conclusion
The findings of this case study highlight the criti- cal role of the IOTA model in enhancing diagnostic accuracy and guiding surgical decision making for ovarian tumours. As demon- strated in this Mongolian patient, IOTA based preoperative and intraoperative assessment provided a robust framework for deter- mining malignancy risk, which directly influenced the choice of fertility preserving surgery (FSS). This approach not only ensured oncological safety but also safeguarded the patient’s reproductive potential, ultimately resulting in a successful twin pregnancy and live birth. Globally, increasing evidence from Asian (e.g., Japan, Korea, China) and European (e.g., France, Italy, Denmark) studies underscores the clinical utility of IOTA in optimising treatment strategies for borderline and early stage ovarian tumours. The present case aligns with these international findings, confirming that IOTA guided FSS can achieve disease free survival rates com- parable to traditional radical surgery while preserving fertility. The absence of recurrence in this patient during long term follow up further validates the oncological safety of this strategy. Important- ly, this study represents one of the first documented cases in Mon- golia where IOTA was integrated into the decision making process for ovarian tumour surgery. By adapting this evidence based mod- el to the local clinical setting, it demonstrates the feasibility of incorporating advanced diagnostic tools into reproductive health- care in resource limited environments. The successful pregnancy outcome also highlights the profound impact of such approaches on the quality of life and psychosocial wellbeing of women of re- productive age.
In conclusion, the integration of the IOTA model with fertility-pre- serving surgical techniques offers a powerful and safe clinical path- way for managing ovarian tumours in young women. This case adds to the international body of evidence, supporting the adoption of IOTA as a standard component of ovarian tumour assessment worldwide. Future research in Mongolia and other low and mid- dle income countries should further evaluate the scalability, cost effectiveness, and long term outcomes of this strategy, thereby contributing to global improvements in women’s oncological and reproductive health.
In Mongolia, it is of paramount importance that fertility-sparing surgery is successfully performed and consistently supported in specialized tertiary-care hospitals according to high-quality international standards, regardless of geographic location.
Authors Contributions
Ureltsetseg Batdelger conceived and designed the study, developed the methodological framework, conducted formal statistical analyses, oversaw data collection, and drafted the initial manuscript.
Sergelen P. and Batbold Ts. provided overall project supervision, methodological guidance, and critical evaluation of the manuscript. Bolortuya B., Michidmaa N., Beulah J., Byambajargal S., Odonchimeg D., Gulgaim K., Shiilegpagam S., Tugsbayar N., and Nyamtsetseg B. contributed to the acquisition and validation of data, performed preliminary analyses, and critically reviewed and revised the manuscript. All authors have read and approved the final version for publication and agree to be accountable for all aspects of the work.
References
- Banerjee, S., & Kaye, S. B. (2013). New strategies in the treatment of ovarian cancer: current clinical perspectives and future potential. Clinical cancer research, 19(5), 961-968.
- Passero, V. A., Branstetter, B. F., Shuai, Y., Heron, D. E.,Gibson, M. K., Lai, S. Y., ... & Argiris, A. (2010). Response assessment by combined PET–CT scan versus CT scan alone using RECIST in patients with locally advanced head and neck cancer treated with chemoradiotherapy. Annals of oncology, 21(11), 2278-2283.
- ESHRE Guideline Group on Female Fertility Preservation, Anderson, R. A., Amant, F., Braat, D., D'Angelo, A., Chuva de Sousa Lopes, S. M., ... & Vermeulen, N. (2020). ESHRE guideline: female fertility preservation. Human reproduction open, 2020(4), hoaa052.
- Mandelbaum, R. S., Klar, M., Takiuchi, T., Bainvoll, L., Matsuzaki, S., Paulson, R. J., & Matsuo, K. (2020). Fertility- sparing treatment for early-stage epithelial ovarian cancer: Contemporary oncologic, reproductive and endocrinologic perspectives. Journal of Obstetrics and Gynaecology Research, 46(8), 1263-1281.
- Levy, B. S., Ness, D. L., & Weinberger, S. E. (2019). Consensus guidelines for facilities performing outpatient procedures: evidence over ideology. Obstetrics & Gynecology, 133(2), 255-260.
- Kawano, K., Tsuda, N., Nishio, S., Yonemoto, K., Tasaki, K., Tasaki, R., & Ushijima, K. (2016). Identification of appropriate cone length to avoid positive cone margin in high grade cervical intraepithelial neoplasia. Journal of Gynecologic Oncology, 27(5), e54.
- Amant, F., Berveiller, P., Boere, I. A., Cardonick, E., Fruscio, R., Fumagalli, M., ... & Zapardiel, I. (2019). Gynecologic cancers in pregnancy: guidelines based on a third international consensus meeting. Annals of Oncology, 30(10), 1601-1612.
- Alcazar, J. L., Guerriero, S. (2019). Role of ultrasound in ovarian cancer diagnosis: IOTA studies. Ultrasound in Obstetrics & Gynecology, 53(5), 604-616.
- Bertoldo, M. J., Walters, K. A., Ledger, W. L., Gilchrist,R. B., Mermillod, P., & Locatelli, Y. (2018). In-vitro regulation of primordial follicle activation: challenges for fertility preservation strategies. Reproductive biomedicine online, 36(5), 491-499.
- Park, B., Khanam, R., Vinayachandran, V., Baqui, A. H., London, S. J., & Biswal, S. (2020). Epigenetic biomarkers and preterm birth. Environmental epigenetics, 6(1), dvaa005.
- Uysal, E., Öztürk, M., Kilinçer, A., & Koplay, M. (2021). Comparison of the effectiveness of shear wave elastography and superb microvascular imaging in the evaluation of breast masses. Ultrasound Quarterly, 37(2), 191-197.
- Kajiyama, H., Mizuno, M., Shibata, K., Yamamoto, E., Kawai, M., Nagasaka, T., & Kikkawa, F. (2014). Recurrence- predicting prognostic factors for patients with early-stage epithelial ovarian cancer undergoing fertility-sparing surgery: a multi-institutional study. European Journal of Obstetrics & Gynecology and Reproductive Biology, 175, 97-102.
- Shahid, S., Khalid, E., Fatima, S. S., & Khan, G. M. (2019).Evaluation of soluble TNF-like weak inducer of apoptosis (sTWEAK) levels to predict preeclampsia in early weeks of pregnancy. European Journal of Obstetrics & Gynecology and Reproductive Biology, 234, 165-170.
- Frega, A., Coluccia, A. C., Di Martino, G., Catalano, A., Milazzo, G. N., Assorgi, C., ... & Moscarini, M. (2014). Borderline ovarian tumors, fertility-sparing surgery and pregnancy outcome. Eur Rev Med Pharmacol Sci, 18(2), 281- 284.
- Leirgul, E., Brodwall, K., Greve, G., Vollset, S. E., Holmstrøm, H., Tell, G. S., & Øyen, N. (2016). Maternal diabetes, birth weight, and neonatal risk of congenital heart defects in Norway, 1994–2009. Obstetrics & Gynecology, 128(5), 1116-1125.
- Wierda, W. G., Kipps, T. J., Keating, M. J., Brown, J. R., Gribben, J. G., Browning, M., ... & CLL Research Consortium. (2011). Selfâ?ÂÂadministered, subcutaneous alemtuzumab to treat residual disease in patients with chronic lymphocytic leukemia. Cancer, 117(1), 116-124.
- Schorge, J. O., Grigsby, P. W., & Mutch, D. G. (2013). Gynecologic oncology: principles and practice. Philadelphia: Lippincott Williams & Wilkins.
- McLeod, C., Moran, C. M., McBride, K. A., & Pye, S. D. (2018). Evaluation of Intravascular Ultrasound Catheter- Based Transducers Using the Resolution Integral. Ultrasound in Medicine & Biology, 44(12), 2802-2812.
- Yang, B., Yang, Y., Liu, Y., Li, H., Ren, S., Peng, Z., ... & Dong,Q. (2021). Molecular characteristics of varicocele: integration of whole-exome and transcriptome sequencing. Fertility and Sterility, 115(2), 363-372.
- Tang, A., Lin, H. (2015). IOTA models in clinical decision- making for ovarian tumors. Ultrasound International Open, 1(2), E32–E39.
- Wang, L., Zhong, Q., Tang, Q., & Wang, H. (2022). Second fertility-sparing surgery and fertility-outcomes in patients with recurrent borderline ovarian tumors. Archives of Gynecology and Obstetrics, 306(4), 1177-1183.
- Ferrero, S., Venturini, P. L., Gillott, D. J., Remorgida, V., & Maggiore, U. L. R. (2012). Hemostasis by bipolar coagulation versus suture after surgical stripping of bilateral ovarian endometriomas: a randomized controlled trial. Journal of minimally invasive gynecology, 19(6), 722-730.
- Wright, J. D., Shah, M., Mathew, L., Burke, W. M., Culhane, J., Goldman, N., ... & Herzog, T. J. (2009). Fertility preservation in young women with epithelial ovarian cancer. Cancer: Interdisciplinary International Journal of the American Cancer Society, 115(18), 4118-4126.
- Zhang, Y., Li, X., Liang, H. (2016). Bilateral borderline ovarian tumors and fertility-sparing surgery. Gynecologic Oncology, 143(3), 557-563.
- Zorn, K. K., Neumann, C. (2017). Fertility-sparing surgery in epithelial ovarian cancer: meta-analysis. Annals of Surgical Oncology, 24(5), 1326-1335.
- Felip, E., Shaw, A. T., Bearz, A., Camidge, D. R., Solomon,B. J., Bauman, J. R., ... & Besse, B. (2021). Intracranial and extracranial efficacy of lorlatinib in patients with ALK-positive non-small-cell lung cancer previously treated with second-generation ALK TKIs. Annals of Oncology, 32(5), 620-630.
- World Health Organization. (2022). Global health observatory data: reproductive health and fertility preservation. Geneva: WHO.
- Qin, J., Zhang, S., Poon, L., Pan, Z., Luo, J., Yu, N., ...& Lu, W. (2021). Doppler-based predictive model for methotrexate resistance in low-risk gestational trophoblastic neoplasia with myometrial invasion: prospective study of 147 patients. Ultrasound in Obstetrics & Gynecology, 57(5), 829- 839.
- Tazelaar, H. D., Bostwick, D. G., Ballon, S. C., Hendrickson,M. R., & Kempson, R. L. (1985). Conservative treatment of borderline ovarian tumors. Obstetrics & Gynecology, 66(3), 417-422.
- Donnez, J., & Dolmans, M. M. (2017). Fertility preservation in women. New England Journal of Medicine, 377(17), 1657- 1665.