
Advancements in Journal of Urology and Nephrology(AJUN)
ISSN: 2689-8616 | DOI: 10.33140/AJUN
Impact Factor: 1.0



Research Article - (2019) Volume 1, Issue 1
Investigation of Nutritional Status of Hemodialysis Patients in Istanbul/Turkey
2Research Assistant, PhD, Marmara University, Department of Nutrition and Dietetics, Faculty of Health Sciences, Istanbul, Turkey
3Research Assistant, MSc, Marmara University, Department of Nutrition and Dietetics, Faculty of Health Sciences, Istanbul, Turkey
4Associate Professor, PhD, Marmara University, Department of Nutrition and Dietetics, Faculty of Health Sciences, Istanbul, Turkey
Received Date: Nov 15, 2019 / Accepted Date: Nov 20, 2019 / Published Date: Dec 04, 2019
Copyright: ©Zehra Margot Celik, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: This study aims to determine protein, sodium, potassium, phosphorus consumptions and energy intake in endstage renal disease (ESRD) patients undergoing hemodialysis 3 times a week and compare these quantities with recommended requirements.
Methods: This study was conducted with 198 end-stage renal disease patients between the ages of 20 and 65 who underwent hemodialysis 3 times a week. Data were obtained via a survey form and Food Frequency Questionnaire.
Results: No significant relationship was identified between gender and protein consumption (p>0.05). However, a significant relationship was found between the body mass indices (BMI) and protein consumption of the patients (p<0.05); when groups were compared, protein consumption reduced while the BMI increased (p<0.01). When age and protein consumption were examined, protein consumption was found to be higher in patients aged 20-44 as compared to patients aged 56-65 (p<0.05).
Conclusion: The protein consumption and energy intake of hemodialysis patients appears to be below the recommended level. This suggests that hemodialysis patients are receiving insufficient nutrition in Istanbul/Turkey. Hemodialysis patients should be given better nutritional education and their nutritional status should be optimized.
Keywords
Chronic Kidney Disease, End-Stage Renal Disease, Hemodialysis, Nutritional Status, Nutrition Therapy
Introduction
End-stage renal disease (ESRD) is the last stage of chronic kidney disease (CKD) and it is a disease with a high rate of mortality and morbidity. ESRD has an adverse effect on quality of life, while there is a lower awareness and lower early onset of diagnosis. This is a costly disease that can be prevented or delayed. CKD is characterized by a gradual decrease in renal function over a period of months [1, 2]. The conservative treatment of Chronic Kidney Disease includes blood pressure control, dietary sodium restriction, HbA1c <7% with Type 2 diabetes patients, LDL <100 mg/dL, hemoglobin 10-12 g/dL, control of bone diseases and non-use of cigarettes [2]. According to the Clinical Practice Guidelines for the Evaluation and Management of Chronic Kidney Diseases (KDIGO), published in 2012, CKD is an abnormality in kidney structure or function that has health effects for over at least 3 months [3]. CKD is an increasing health problem worldwide and leads to ESRD (4). In population-based studies, the prevalence of CKD in patients over age 30 was 7.2%, while for patients over 64 the rate was determined as 23.4-35.8% [2]. In 2014, the prevalence of ESRD, including renal replacement therapy, in both pediatric patients and adult patients in Turkey, was reported as being 918 per every million persons [5].
At the beginning of the disease, medication and diet therapy are sufficient, but when the kidneys become unable to function completely, renal replacement therapy is performed for those patients whose uremic signs and symptoms cannot be controlled by preventive therapy. Renal replacement therapy consists of dialysis or kidney transplantation. Clinical dialysis means that certain harmful substances in the dialysate are transferred through a semipermeable membrane into the dialysate fluid. There are two main types of dialysis applications, hemodialysis and peritoneal dialysis [6]. The most commonly used method in renal replacement therapy in Turkey is hemodialysis, at a rate of 78.4 % [5].
Nutrition plays an important role in the treatment of hemodialysis patients. The purpose of medical nutrition therapy in the first three stages of CKD is to maintain a good nutritional status, to slow down the process of renal failure and to reduce the risk factors for comorbidities [7]. Adverse changes in fluid-electrolyte balance (hyperkalemia, hyperphosphatemia, peripheral and pulmonary edema) can be seen in patients who do not comply with their diet. The purpose of dietary therapy for patients undergoing hemodialysis treatment is to provide an optimal nutritional status and prevent malnutrition without disturbing the fluid-electrolyte balance or increasing uremic symptoms [8]. Consumptions of excessive fat, excessive salt or insufficient fiber may lead to atherogenic results in dialysis patients. Dialysis patients who have such nutritional habits are at a 40 times greater risk of cardiovascular disease than the healthy population [9]. It has been observed that dietary practices with low-protein content can slow the progression of CKD. However, one of the causes of malnutrition in patients with this disease is that they cannot adequately meet their energy needs and the daily amount of protein they consume is inadequate [10]. Inadequate uptake, losses, metabolic and endocrine disorders, increased protein catabolism are some of the common causes of nutrition-related problems in these patients. Clinical trials have shown that hemodialysis patients often receive protein and energy below the recommended levels [11]. Among the causes of insufficient intake are nausea, vomiting and loss of appetite, diabetic or uremic gastroparesis, esophagitis, gastritis, susceptibility to infections and increased infectious frequency, depression, anemia, oral and dental problems caused by uremic toxins and socioeconomic causes [12]. Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines suggest 30 to 35 kcal/kg/day energy intake for hemodialysis patients; it is recommended that 15% of this energy should be supplied from proteins, 55-60% from carbohydrates, and less than 30% from lipids. At least 0.75 g/kg protein intake per day is required for a healthy adult. In accordance with nitrogen balance studies this value has been established at 1.2 g/kg for hemodialysis patients [13]. Protein intake that is under these quantities has been shown to cause a negative nitrogen balance. The protein source must be animal originated, and more particularly of a high biological value. Sufficient energy intake is necessary to prevent the protein being used as an energy source by gluconeogenesis. If the caloric intake is not sufficient, despite high protein uptake, it is not possible to achieve a positive nitrogen balance [3, 14]. During hemodialysis, protein, amino acid and peptide losses occur with the intake of the dialysis fluid. Because of these losses, metabolic disorders occur and protein catabolism increases. It is necessary to replace the lost amount of amino acids to prevent a negative nitrogen balance [15]. As mentioned above, the limitations of protein consumption in dialysis patients are of great importance. This study aims to determine the nutritional status of the ESRD patients undergoing hemodialysis 3 times a week in Istanbul/Turkey and compare these quantities with the recommended requirements.
Methods
This study was conducted as a cross-sectional descriptive study to evaluate the nutritional status of end-stage renal disease (ESRD) patients undergoing hemodialysis. A total of 220 patients with ESRD between the ages of 20 and 65 who underwent hemodialysis 3 times a week were surveyed from two different nephrology clinics in Istanbul/Turkey. Twenty-two of the patients in the survey left the study before the completion of the survey and 198 patients were examined. The gender distributions of the patients were equal.
Evaluation Criteria
The research data were gathered by interviewing the patience twice. Data were obtained via a survey form and Food Frequency Questionnaire (FFQ). The survey form consisted of 29 questions and was prepared to determine the demographic characteristics of the patients (9 questions), hemodialysis/disease related characteristics (6 questions) and nutritional characteristics (14 questions). The FFQ consisted of 7 food groups that included a total of 46 foods and beverages; these were meat, meat and products (6), vegetable-fruit (7), bread-cereals (6), sugar (6), fats (6) and beverages (7). After these two questionnaires were completed, patients were asked to fill a 3-day food record; this information was obtained during the second interview. The questionnaire form and FFQ were recorded by the researchers. The estimated duration of this data collection was 15-20 minutes. Also, the latest laboratory test results (serum potassium, sodium, phosphorus, calcium, uric acid) of patients were taken from the patient files.
Statistical Analysis
The statistical analysis of the data obtained in the study was calculated by using the SPSS (IBM SPSS Statistics Version 20, 2011) package program. Normal distribution of the variables was checked by Kolmogorov Smirnov test. The Mann-Whitney U test was used for the normal distribution of the two groups and the Chi-square test (χ2) was used for the comparison of qualitative variables among the groups. The results were evaluated at a 95% confidence interval and a significance level of p<0.05. The data on nutrition consumption in the study were evaluated in the Nutrition Information System (Bebis 7.1) program. Ethical Principles of Research The study was evaluated by Marmara University Faculty of Medicine Clinical Research Assessment Commission. It was decided that the study was ethically appropriate by the commission (Protocol No: 09.2016.037-70737436-050.06.04). The necessary permissions from various state and private dialysis centers that are located in Istanbul/ Turkey was collected by researchers. Participants in the study were informed that the information would only be used for research purposes and verbal and written approval was taken.
Results
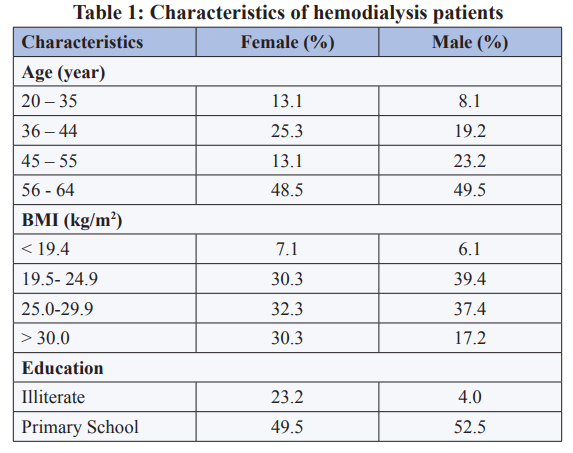
This study included 198 ESRD patients (99 females, 99 males) who were being treated with hemodialysis 3 times a week. The general characteristics of the study group are shown in Table 1.
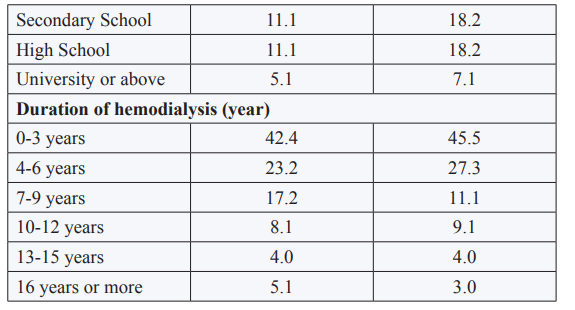
The average energy intake of patients was 20.2±5.9 kcal/kg/day, while the average protein intake was 0.8±0.25 g/kg/day (Table 2). The average sodium, potassium and phosphorus consumptions of the patients were 3371.2±1113.4, 1638.7±464.9 and 954.7±257.1, respectively.
No significant relationship between gender and protein consumption was identified (p>0.05). However, a significant relationship was found between the body mass indices (BMI) and protein consumption of the patients (p<0.05); when groups were compared, protein consumption had reduced while the BMI increased (p<0.01) (Table 3).
Table 3: Assessment of protein consumption by Body Mass Index (BMI)
|
BMI (kg/m2) |
n |
Min. – Max. |
Median ± SD |
x2 |
p |
|
< 19.4 |
13 |
0.74 – 1.70 |
1.10 ± 0.31 |
51.047 |
< 0.001 |
|
19.5-24.9 |
69 |
0.34 – 1.60 |
0.89 ± 0.25 |
||
|
25.0-29.9 |
69 |
0.39 – 1.20 |
0.76 ± 0.18 |
||
|
> 30.0 |
47 |
0.39 – 1.04 |
0.65 ± 0.16 |
When age and protein consumption were examined, protein consumption was found to be higher in patients aged 20-44 as compared to patients aged 56-65 (p<0.05) (Table 4).
Table 4: Assessment of protein consumption by age
|
Protein Consumption (g/kg/day) |
|||||
|
Age (year) |
n |
Min. – Max. |
Median ± SD |
x2 |
p |
|
20 – 35 |
21 |
0.46 – 1.70 |
0.89 ± 0.33 |
12.414 |
0.006 |
|
36 – 44 |
44 |
0.39 – 1.41 |
0.89 ± 0.20 |
||
|
45 – 55 |
36 |
0.39 – 1.48 |
0.83 ± 0.23 |
||
|
56 – 65 |
97 |
0.34 – 1.64 |
0.73 ± 0.24 |
||
There was no significant relationship between protein consumption of patients on a specific diet for ESRD and patients not on a diet (p>0.05) (Not shown in table).
Discussion
While obesity is a risk factor for the progression of disease in hemodialysis patients, malnutrition is related to increased morbidity and mortality rates. Hemodialysis is associated with increased energy and protein requirements [8]. Hemodialysis patients are often exposed to a number of dietary restrictions related to dietary phosphorus, potassium, sodium, fluid intake, and macronutrients, including carbohydrate and fat [10]. Most hemodialysis patients have inadequate energy, protein and micro-nutrient intakes, which compromises their nutritional statuses [16]. According to recent publications, the recommended energy (kcal/kg) intake for adult hemodialysis patients is 30-35 kcal/kg for patients who are aged 60 or younger and 35 kcal/kg for patients who are over 60 years old; the recommended protein consumption is 1.2 g/kg for adult hemodialysis patients [17]. Protein intake below the recommended rate will be a risk factor that increases mortality in hemodialysis patients. In a study conducted with 53,933 hemodialysis patients, it was found that more than half of the participants’ protein intake was below the level recommended by KDOQI [18]. A study conducted with dialysis patients found that protein and energy intake was below the recommended level, but there was not a significant difference. They were also found to be prone to lower levels of protein and energy intake on dialysis days [19]. In a study with 130 hemodialysis patients, it was found that only 6% of the participants could meet their energy needs and only half could attain the recommended protein level [9]. In another study conducted by Alvarenga et al. with hemodialysis patients, the average energy intake was 20.52±11.74 kcal/kg/day and the protein intake were 0.87±0.50 g/kg [20]. In addition, research with this population has shown that hemodialysis patients do not get adequate or effective nutrition education in Turkey [21]. The data obtained in our study is similar; the energy intake of the patients was 20.2±5.9 kcal/kg and the protein intake was 0.8±0.25 g/kg. These values reveal that the energy and protein intake of hemodialysis patients in Turkey is much lower than the recommended level. While the potassium consumption was found to be low (65.5% of required amount) as well as the energy and protein intakes, sodium and phosphorus consumption of hemodialysis patients were higher than the recommended levels (134, 6% and 106, 1% respectively). These results may be due to the education level of the group, as most of the study group (49.5% of females, 52.5% of males) was primary school graduates [22].
Research has demonstrated that in clinical practice, food intake during hemodialysis needs to be increased. Providing nutrient or nutritional supplements during hemodialysis may be associated with improved nutritional status and reduced mortality. Nevertheless, despite these potential benefits, eating habits vary between countries, regions and clinics. It was also found that hemodialysis patients were not fed adequately on days they had dialysis. Therefore, patients should be given appropriate nutrition education and should be informed about the management of nutritional status during dialysis days.
Many studies mention the protective effect of a higher BMI in hemodialysis patients; especially patients with a BMI greater than 23 kg/m2 are less likely to have high morbidity and mortality rates [23, 24]. However, this study indicates that even if hemodialysis patients have a higher BMI, they still consume less than the recommended values for energy and protein per day. Furthermore, this research has found that patients with higher BMI consume less protein (g/kg/day).
While nutrition is important in hemodialysis patients, so is nutrition education. The elderly is more susceptible to diseases and there are various social and physiological factors that can affect their diet. For this reason, understanding of the nutritional knowledge levels in the elderly population is important. In a study conducted with 90 elderly patients over the age of 60, it was determined that 18.9% of the patients had insufficient nutrition knowledge [25]. In a study that took place in Turkey with hemodialysis patients found that the level of nutritional knowledge of the patients over 65 years of age was lower than those who were aged under 65 [26]. Kaymak (2012) found that malnutrition in hemodialysis patients was associated with old age [27]. Another study found that 26% to 77% of protein-energy malnutrition was seen in elderly individuals [28]. Similarly, we found that younger patients had a better nutritional status. It was observed that the protein intake level of the older patients was lower than the younger patients. This may be related to the nutritional status, the psychological state or the physiological state, affected by aging, or insufficient nutritional knowledge of elderly individuals, as stated in the literature.
In conclusion, the protein and energy consumption of hemodialysis patients in Istanbul/Turkey appears to be below the recommended levels. This suggests that hemodialysis patients are receiving insufficient nutrition. The decrease in protein consumption that occurs with age and BMI suggests that physical conditions affect the nutritional status of patients. Hemodialysis patients should be given better nutritional education and their nutritional status should be optimized.
Limitations
The limitations of this study were that only two nephrology clinics in Istanbul were included in the study and these clinics are not enough to represent the hemodialysis patients in Istanbul/Turkey.
References
- Alim N, Kiziltan G (2016) Kronik Böbrek Hastali ve istah. Izmir Katip Çelebi Univ. SaGlk Bilim Derg 1: 45-50.
- Akbulut G (2017) Tibbi Beslenme Tedavisinde Güncel Uygulamalar XI. Böbrek Hastaliklarinda Tibbi Beslenme Tedavisi. 1st ed Ankara Nobel Tip Kitabevleri p 43-108.
- Inker LA, Astor BC, Fox CH (2014) KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis 63: 713-735.
- Süleymanlar G, UtasC, Arinsoy T, Ates K, Altun B, et al., (2011) A population-based survey of Chronic Renal Disease In Turkey. Nephrol Dial Transplant 26: 1862-71.
- Süleymanlar G, Utas C, Arinsoy, Ates K, Altun B et.al., (2010) A population-based survey of Chronic REnal Disease In Turkey-the CREDIT study. Nephrol Dial Transplant 26: 1862-1871.
- Andrassy KM (2013) Comments on KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int 84: 622-623.
- Panaput T, Thinkhamrop B, Domrongkitchaiporn S, Sirivongs D, Praderm L, et al., (2014) Dialysis dose and risk factors for death among ESRD patients treated with twice-weekly hemodialysis: a prospective cohort study. Blood Purif 38: 253-262.
- Tufan F, Yildiz A, Dogan I, Yidiz D, Sevinir S, et al., (2015) Urea to creatinine ratio: a forgotten marker of poor nutritional state in patients undergoing hemodialysis treatment. Aging Male 18: 49-53.
- Roach LA, Lambert K, Holt JL, Meyer BJ (2017) Diet quality in patients with end-stage kidney disease undergoing dialysis. J Ren Care 43: 226-234.
- Kalantar-Zadeh K, Tortorici AR, Chen JL, Kamgar M, Lau WL, et al., (2015) Dietary restrictions in dialysis patients: is there anything left to eat? Semin Dial 28:159-168.
- Altiparmak MR (2015) Hemodiyaliz Hastalarinda Beslenme.Turkiye Klinikleri J Nephrol-Special Topics 8: 53-60.
- Beberashvili I, Azar A, Sinuani I, Kadoshi H, Shapiro G, et al., (2013) Comparison analysis of nutritional scores for serial monitoring of nutritional status in hemodialysis patients. Clin J Am Soc Nephrol 8: 443-451.
- National Kidney Foundation (2015) KDOQI clinical practice guideline for hemodialysis adequacy: 2015 update. Am J Kidney Dis 66: 884-930.
- Burrows NR, Li Y, Geiss LS (2010) Incidence of treatment forend-stage renal disease among individuals with diabetes in theU.S. continues to decline. Diabetes Care 33: 73-77.
- CanoN, Fiaccadori E, Tesinsky P, Toigo G, Druml W, et al., (2006) ESPEN guidelines on enteral nutrition: adult renal failure. Clin Nutr 25: 295-310.
- Chen J, Peng H, Zhang K, Long Xiao, 5 Zhimin Yuan, et al., (2013) The insufficiency intake of dietary micronutrients associated with malnutrition-inflammation score in hemodialysis population. PloS one 8: e66841.
- Nation Kidney Foundation (2012) KDOQI Clinical Practice Guideline for Diabetes and CKD: 2012 update. Am J Kidney Dis 60: 850-886.
- Shinaberger CS, Kilpatrick RD, Regidor DL, McAllister CJ, Greenland S, et al., (2006) Longitudinal associations between dietary protein intake and survival in hemodialysis patients. Am J Kidney Dis 48: 37-49.
- Stark S, Snetselaar L, Hall B, Beth Hall, Roslyn A Stone, etal., (2011) Nutritional Intake in Adult Hemodialysis Patients.Top Clin Nutr 26: 45-56.
- Alvarenga LDA, Andrade BD, Moreira MA, Nascimento RP, Macedo ID, et al., (2017) Nutritional profile of hemodialysis patients concerning treatment time. J Bras Nefrol 39: 283-286.
- Elmas A, Erbay Saral E, Tusrul A,sengül E, Bünül F, et al., (2012) Hemodializ hastalarÃÂ?±nda beslenme bilgi düzeyi ile klinik ve laboratuar bulgulari arasindaki ilski. Kocaeli Med J 1: 23-26.
- Kistler B, Benner D, Burgess M, Stasios M, Kalantar-Zadeh K et al., (2014) To eat or not to eat international experiences with eating during hemodialysis treatment. J Ren Nutr 24: 349-352.
- Leavey SF, McCullough K, Hecking E, Goodkin D, Port FK, et al., (2001) Body mass index and mortality in ‘healthier’as compared with ‘sicker’ haemodialysis patients: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol Dial Transplant 16: 2386-2394.
- Abbott KC, Glanton CW, Trespalacios FC, Oliver DK, Ortiz MI, et al., (2004) Body mass index, dialysis modality, and survival: Analysis of the United State Renal Data System Dialysis Morbidity and Mortality Wave II Study. Kidney Int 65: 597-605
- Allah ESA, Oraby EESES, Ibrahim RG (2015) Effect of Diet Therapy Program on Dietary Knowledge and Practice of Elderly Patients on Regular Hemodialysis. Am J Nurs 4: 131-137.
- Kocami RN, Türker PF, Köseler E, Petrone I, Di Giorgio A, et al., (2016) The Relationship between the Nutritional Knowledge Level and Nutritional Status In Hemodialysis Patients. Baskent Üni Saik Bilimleri Fak Dergisi 1: 15-31.
- Kaymak AD (2012) Hemodiyaliz Hastalarinin Yasam Kalitesi Ve Beslenme Durumlarinin Deserlendirilmesi. T Ü Saiik Bilimleri Enstitüsü Yüksek Lisans Tezi.
- de Oliveira Santin FG, Bigogno FG, Dias Rodrigues JC, Cuppari L2, Avesani CM, et al., (2016) Concurrent and predictive validity of composite methods to assess nutritional status in older adults on hemodialysis. J Ren Nutr 26: 18-25.