
International Internal Medicine Journal(IIMJ)
ISSN: 2837-4835 | DOI: 10.33140/IIMJ
Impact Factor: 1.02



Research Article - (2024) Volume 2, Issue 8
Insights into Readmission Trends Following Inpatient Chemotherapy for Acute Lymphoblastic Leukemia: A 30-Day Analysis
2St. Joseph Medical center, Department of Hematology Oncology, AZ, USA
Received Date: Jul 26, 2024 / Accepted Date: Aug 25, 2024 / Published Date: Aug 28, 2024
Copyright: ©Â©2024 Silpa Choday, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Silpa, C., Diana, Z., Anthony, Y., Miguel, G. (2024). Insights into Readmission Trends Following Inpatient Chemotherapy for Acute Lymphoblastic Leukemia: A 30-Day Analysis. Int Internal Med J, 2(8), 01-05.
Abstract
Introduction: Acute lymphoblastic leukemia (ALL) has significant morbidity due to its aggressive course and intensive treatment protocols. Understanding the patterns of readmission after inpatient chemotherapy is crucial for optimizing patient care and resource allocation.
Methods: We conducted a retrospective analysis of the National Readmission Database among ALL patients who underwent inpatient chemotherapy between 2016 and 2020. We examined trends in 30-day readmission rates, factors associated with readmission, and outcomes such as remission and relapse.
Results: A total of 22,483 admissions were analyzed. Of these, 72.5% (16,294) experienced readmission. Notably, the trend in readmission rates declined between 2016 to 2020, dropping from 76.1% to 66.3%. Among the 16,294 readmissions, 3,607 achieved remissions, 10,637 has stable disease and 2,051 had relapsed disease (P<.001). The mean age at remission was at 18.9 years, while non-remission and relapse occurred at older ages (32.2 and 31 years, respectively, P<.001). In terms of insurance, private insurance had the highest readmission rate at 48%, followed by Medicaid at 35%, and Medicare at 12% (P<.001). The odds ratios indicated significant differences: Elective readmissions had a significantly higher risk compared to non-elective readmissions (4.01, 95% CI 3.44 - 4.67, P<.001), Additionally, patients achieving remission had a lower risk of readmission compared to those not achieving remission (0.52, 95% CI 0.42 - 0.64, P=.003), and. relapse (0.52, 95% CI 0.42 - 0.64, P<.001).
Conclusion: Our study highlights factors such as relapsed disease, insurance status, elective admissions, and age were associated with higher readmission risk. These findings emphasize the importance of targeted interventions to reduce the rates of readmission and improve outcomes in ALL patients.
Keywords
Acute Lymphoblastic Leukemia, ALL, remission, Remission, Readmissions, Trends, Inpatient Chemothera, NRD
Introduction
Acute lymphoblastic leukemia (ALL) is a type of acute leukemia marked by chromosomal translocations and somatic mutations that drive leukemogenesis, a hematological malignancy originating from B- or T-lymphoid progenitor cells [1]. ALL is increasingly recognized as a genetically diverse disease, with numerous new genetic subtypes leading to more precise risk stratification. Although most cases of ALL are diagnosed in children, the incidence exhibits a bimodal pattern, peaking in children under age 5 and again around age 50 [2]. Advances in research and treatment for adult ALL are progressing rapidly, especially for Philadelphia chromosome-positive disease, which has significantly improved outcomes [3]. However, older patients often face poor-risk biology and reduced tolerance to chemotherapy, resulting in lower remission rates and overall survival. Regardless of age, patients with relapsed or refractory ALL have very poor prognoses [4]. This study examined readmission patterns following inpatient chemotherapy, which is crucial for optimizing patient care and resource allocation.
Methods
The study analyzed hospital readmissions for ALL in the US. The complete dataset was obtained from the NRD spanning 2016 to 2020 using the ICD-10 codes. This extensive, comprehensive database encompasses national hospital discharges. It is meticulously maintained as an integral component of the healthcare cost and utilization project (HCUP) by the Agency for Healthcare Research and Quality (AHRQ). This sample includes community, general hospitals, and academic medical centers but excludes long-term facilities. Hospitals were divided based on geographic region, urban vs. rural location, teaching status, ownership, and number of beds. NRD accounts for around 60 percent of U.S. hospitalizations reported in the American Hospital Association (AHA) Annual Survey Database. A multivariate logistic regression analysis was used to calculate the predictors of in-hospital mortality, LOS, and total hospital costs (THC) following adjustment for age (included in the study are adults >18 years), sex, race, grouped with Charlson comorbidity index, insurance type, mean annual household income, and hospital characteristics. The calculation of total hospital costs involved utilizing HCUP Cost-to-Charge Ratio files. Cost is adjusted for inflation using Consumer Price Index (CPI) for medical care services in the U.S., all urban consumers, chained, with 2020 as the reference point. Institutional review board approval was not needed for this database study as the de-identified data is publicly available on the HCUP website.
Results
The study analyzed 22,483 patients with ALL to determine various characteristics and their correlation with remission status and relapse rates. There are a total of 16,282 readmissions, and a decreasing trend in readmission rates has been observed from 3,481 to 3,036 [Table 1]. The mean age overall was 29.2 years. Patients in remission had a mean age of 18.9 years, those who did not achieve remission had a mean age of 32.2 years, and those who relapsed had a mean age of 31.0 years. The difference in age across groups was statistically significant (p < 0.001). Female patients constituted 42% of the overall population, 43% of those in remission, 42% of those not achieving remission, and 41% of those relapsing (p = 0.432) [Table 2].
Age Categorization data:
Ages 2-10: 28% overall, 43% in remission, 25% not achieved remission, 18% relapse.
Ages 11-18: 19% overall, 30% in remission, 16% not achieved remission, 19% relapse.
Ages 19-40: 20% overall, 12% in remission, 20% not achieved remission, 32% relapse.
Age >41: 33% overall, 15% in remission, 39% not achieved remission, 32% relapse.
The distribution across age was statistically significant (p < 0.001).
Insurance: Medicare: 12% overall, 6.0% in remission, 12% not achieved remission, 17% relapse.
Medicaid: 35% overall, 44% in remission, 32% not achieved remission, 36% relapse.
Private: 48% overall, 45% in remission, 50% not achieved remission, 42% relapse.
Other: 5.7% overall, 5.3% in remission, 5.9% not achieved remission, 5.6% relapse.
Insurance type differences were significant (p < 0.001).
Hospital Bed Size:
Small: 10.0% overall, 13% in remission, 9.3% not achieved remission, 8.8% relapse.
Medium: 14% overall, 18% in remission, 13% not achieved remission, 13% relapse.
Large: 76% overall, 70% in remission, 78% not achieved remission, 79% relapse.
Bed size differences were significant (p = 0.008). Hospital Teaching Status: Metropolitan teaching: 96% overall, 96% in remission, 96% not achieved remission, 96% relapse.
Metropolitan non-teaching: 3.5% overall, 3.6% in remission, 3.5% not achieved remission, 3.4% relapse.
Non-metropolitan: 0.6% overall, 0.4% in remission, 0.7% not achieved remission, 0.3% relapse.
Hospital teaching status differences were not significant (p = 0.743).
Elective Admission: 66% overall, 71% in remission, 65% not achieved remission, 65% relapse (p = 0.001).
Readmission in 30 Days: 72% overall, 75% in remission, 74% not achieved remission, 63% relapse (p < 0.001).
|
Characteristic |
Overall N = 22,483 |
2016 N = 4,578 |
2017 N = 4,487 |
2018 N = 4,562 |
2019 N = 4,277 |
2020 N = 4,578 |
|
Readmitted |
|
|
|
|
|
|
|
No |
6,188 (27.5%) |
1,096 (23.9%) |
1,125 (25.1%) |
1,198 (26.3%) |
1,227 (28.7%) |
1,542 (33.7%) |
|
Yes |
16,294 (72.5%) |
3,481 (76.1%) |
3,362 (74.9%) |
3,365 (73.7%) |
3,050 (71.3%) |
3,036 (66.3%) |
Table 1: Yearly trends of Readmission
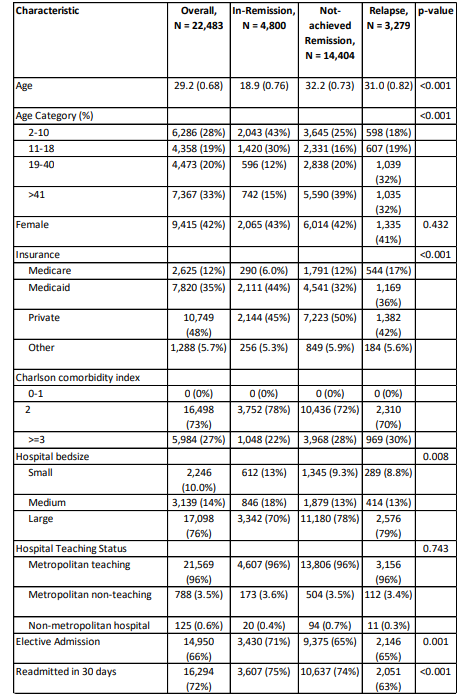
Table 2: Baseline Characteristics of Study Population Stratified by Remission Type
Discussion
The study's analysis of 22,483 readmissions reveals significant trends and factors. The overall readmission rate of 72.5%, with a notable decline from 76.1% in 2016 to 66.3% in 2020, suggests improvements in healthcare practices and interventions aimed at reducing readmissions over time. The treatment of ALL has made great progress over the past 40 years. New combination therapies, including advanced BCR: ABL1 TKIs and new antibodies, are challenging the need for long, intensive chemotherapy and stem cell transplants [5].
Age and Disease Status
The relationship between age and remission or relapse outcomes is particularly noteworthy. Patients achieving remission were younger, with a mean age of 18.9 years, compared to those not achieving remission and those relapsing, who had mean ages of 32.2 and 31 years, respectively. This suggests that younger patients may have better recovery prospects due to a combination of factors such as better overall health, quicker recovery times, and potentially more aggressive or effective treatment regimens.
Unfortunately, adults with ALL didn’t keep up with those of pediatric population. Even though about 85% of adults achieve complete remission (CR) with treatment, their 3-year event-free survival (EFS) and overall survival (OS) rates are below 45% [6,7]. In contrast, treatment for children with ALL has improved greatly, with 95% reaching complete remission and 80% to 85% achieving 5-year event-free survival [8-10].
Insurance Status
Insurance status emerged as a significant predictor of readmission rates, with private insurance holders experiencing the highest rate at 48%, followed by Medicaid at 35%, and Medicare at 12%. This disparity may reflect differences in access to care, socioeconomic status, and the comprehensiveness of coverage. Privately insured patients might be more likely to seek readmission for ongoing or recurrent issues due to better coverage, whereas Medicare and Medicaid patients might face barriers to accessing care that could prevent frequent readmissions.
Elective vs. Non-Elective Readmissions
The study's findings that elective readmissions had a significantly higher risk compared to non-elective readmissions are important for healthcare planning. Elective readmissions often result from planned surgeries or procedures that require post-operative care, indicating a need for better discharge planning and follow-up care to manage post-procedure complications and reduce the need for readmission. This underscores the necessity of targeted interventions to manage elective admissions more effectively.
Remission and Relapse
Patients achieving remission demonstrated a lower risk of readmission compared to those not achieving remission and those experiencing relapse. These findings underscore the critical importance of achieving remission in chronic disease management, as it significantly reduces the likelihood of subsequent hospital admissions. A treatment plan using blinatumomab and ponatinib with chemotherapy free regimen led to an 85% complete remission rate and a 90% estimated 3-year survival rate. This may reduce the need for stem cell transplants. For younger patients with pre-B Philadelphia chromosome- negative ALL, adding blinatumomab and inotuzumab to the initial treatment has improved the 3-year survival rate to 85% across all risk levels [11].
Regardless of age, relapse is a major problem for many patients. Adults with ALL relapses more often, probably because their disease is more severe. However, new treatments like monoclonal antibodies, innovative immunotherapies, and kinase inhibitors for specific genetic types are showing promising results. These advancements are bringing new hope and better outcomes for patients with ALL [12].
Hospital and Patient Characteristics
Factors such as hospital size, teaching status, and patient demographics also influenced readmission rates. Medicare patients had higher odds of readmission compared to those with private insurance, indicating that older adults or those with disabilities might have more complex healthcare needs, increasing the risk of readmission. However, differences in readmission rates between small and large hospitals and between teaching and non-teaching hospitals were not statistically significant, suggesting that other factors may play a more substantial role in readmission risks.
The idea of measurable residual disease has improved how we predict outcomes and make treatment decisions. Treatment for ALL has changed dramatically with new targeted therapies. These include tyrosine kinase inhibitors (TKIs) for BCR-ABL1, monoclonal antibodies like rituximab for CD20, antibody-drug conjugates like inotuzumab ozogamicin for CD22, bispecific antibodies like blinatumomab, and chimeric antigen receptor (CAR) T-cell therapy like tisagenlecleucel for CD19 [13]. These therapies target specific genes and cell markers, representing major breakthroughs in managing ALL [14].
Conclusion
This study provides valuable insights into the factors influencing readmission rates, highlighting the importance of targeted interventions, especially for elective procedures and chronic disease management. Patient characteristics, including advanced age, poor performance status, and hyperleukocytosis, are all recognized as adverse risk factors predicting poor outcomes of chemotherapy. The associations with age, insurance status, and remission outcomes offer critical areas for healthcare providers and policymakers to focus on to further reduce readmissions and improve patient care.
Declarations
Acknowledgements: None
Institutional Review Board Approval: Not needed as the data has been collected from public databases.
Ethics Approval and Consent to Participate: Not applicable.
Consent for Publication: Not applicable.
Availability of Data and Material: Data has been collected from the Nationwide HCUP database https://hcup-us.ahrq.gov/ databases.jsp.
Conflict of Interests: The authors declare that they have no competing interests.
Financial Disclosures/Funding: Not applicable.
Informed Consent: Not applicable
Authors' Contributions: SC as the first author analyzed and interpreted the data, generated tables, and graphs, wrote most of the sections, and was a major contributor to writing the manuscript. DZ and AY as a second and third author analyzed the data and was a contributor to the discussion section of the manuscript. MG as a senior author reviewed the article and made necessary changes to the manuscript. All authors read and approved the final manuscript.
References
- Chen, Y., Li, J., & Zhao, Z. (2021). Redox control in acute lymphoblastic leukemia: from physiology to pathology and therapeutic opportunities. Cells, 10(5), 1218.
- Sant, M., Allemani, C., Tereanu, C., De Angelis, R., Capocaccia, R., Visser, O., ... & HAEMACARE Working Group. (2010). Incidence of hematologic malignancies in Europe by morphologic subtype: results of the HAEMACARE project. Blood, The Journal of the American Society of Hematology, 116(19), 3724-3734.
- Gavralidis, A., & Brunner, A. M. (2020). Novel therapies in the treatment of adult acute lymphoblastic leukemia. Current hematologic malignancy reports, 15, 294-304.
- Fielding, A. K., Richards, S. M., Chopra, R., Lazarus, H. M., Litzow, M. R., Buck, G., ... & Medical Research Council of the United Kingdom Adult ALL Working Party and the Eastern Cooperative Oncology Group. (2007). Outcome of 609 adults after relapse of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study. Blood, 109(3), 944-950.
- Jabbour, E., Short, N. J., Jain, N., Haddad, F. G., Welch,M. A., Ravandi, F., & Kantarjian, H. (2023). The evolution of acute lymphoblastic leukemia research and therapy at MD Anderson over four decades. Journal of Hematology & Oncology, 16(1), 22.
- Kantarjian H, Thomas D, O’Brien S, et al. Long-term follow-up results of hyperfractionated cyclophosphamide,vincristine, doxorubicin, and dexamethasone (Hyper- CVAD), a dose-intensive regimen, in adult acute lymphocytic leukemia. Cancer. 2004; 101: 2788 - 2801.
- Larson, R. A., Dodge, R. K., Linker, C. A., Stone, R. M.,Powell, B. L., Lee, E. J., ... & Schiffer, C. A. (1998). A randomized controlled trial of filgrastim during remission induction and consolidation chemotherapy for adults with acute lymphoblastic leukemia: CALGB study 9111. Blood, The Journal of the American Society of Hematology, 92(5), 1556-1564.
- Pui, C. H., Relling, M. V., & Downing, J. R. (2004). Acute lymphoblastic leukemia. New England Journal of Medicine, 350(15), 1535-1548.
- Pui, C. H., Campana, D., Pei, D., Bowman, W. P., Sandlund,J. T., Kaste, S. C., ... & Relling, M. V. (2009). Treating childhood acute lymphoblastic leukemia without cranial irradiation. New England Journal of Medicine, 360(26), 2730-2741.
- Larsen, E. C., Devidas, M., Chen, S., Salzer, W. L., Raetz, E.A., Loh, M. L., ... & Carroll, W. L. (2016). Dexamethasone and high-dose methotrexate improve outcome for children and young adults with high-risk B-acute lymphoblastic leukemia: a report from Children’s Oncology Group Study AALL0232. Journal of Clinical Oncology, 34(20), 2380- 2388.
- Jabbour, E., Short, N. J., Jain, N., Haddad, F. G., Welch,M. A., Ravandi, F., & Kantarjian, H. (2023). The evolution of acute lymphoblastic leukemia research and therapy at MD Anderson over four decades. Journal of Hematology & Oncology, 16(1), 22.
- DeAngelo, D. J., Jabbour, E., & Advani, A. (2020). Recent advances in managing acute lymphoblastic leukemia. American Society of Clinical Oncology Educational Book, 40, 330-342.
- Samra B, Jabbour E, Ravandi F, Kantarjian H, Short NJ. Evolving therapy of adult acute lymphoblastic leukemia: state-of-the-art treatment and future directions. J Hematol Oncol. 2020 Jun 5;13(1):70.
- Jabbour, E., Pui, C. H., & Kantarjian, H. (2018). Progress and innovations in the management of adult acute lymphoblastic leukemia. JAMA oncology, 4(10), 1413-1420.