
Journal of Ophthalmology & Clinical Research(JOCR)
ISSN: 2573-9573 | DOI: 10.33140/JOCR
Impact Factor: 1.3


Mini Review Article - (2025) Volume 9, Issue 1
Injecting Liquid Antiseptic beneath the Conjunctiva for Inflammatory Red Eye
Received Date: Jan 10, 2025 / Accepted Date: Feb 17, 2025 / Published Date: Mar 04, 2025
Copyright: ©©2025 Karan R. Aggarwala, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Aggarwala, K. R., Engel, H., Ritch, R. (2025). Injecting Liquid Antiseptic beneath the Conjunctiva for Inflammatory Red Eye. J ophthalmol Clin Res, 9(1), 01-04.
Abstract
Many types of inflammatory red eye have been described in standard textbooks written and published the world over, for training ophthalmology resident doctors and optometric physicians, but the inflammatory acute red eye patient may suddenly appear at a general clinic where nurses can be found, but not eye doctors. In this review paper we summarize a management strategy and formalized protocol that can be used in a general clinic by trained nurses and also by certified emergency medical technicians, EMTs. The reading list at the end should serve you well to better understand and better implement your own custom stratagem. What method you choose, depends on what antimicrobial antiseptic agents can be obtained in your geographic region and which ones might be easily purchased for your medical emergency room or casualty clinic.
Introduction
Many types of inflammatory red eye have been described in standard textbooks written and published the world over, for training ophthalmology resident doctors and optometric physicians, but the inflammatory acute red eye patient may suddenly appear at a general clinic where nurses can be found, but not eye doctors. In this review paper we summarize a management strategy and formalized protocol that can be used in a general clinic by trained nurses and also by certified emergency medical technicians, EMTs. The reading list at the end should serve you well to better understand and better implement your own custom stratagem. What method you choose, depends on what antimicrobial antiseptic agents can be obtained in your geographic region and which ones might be easily purchased for your medical emergency room or casualty clinic.
What Do I See?
Your patient has one or both eyes red and appearing slightly swollen, but visual function is not affected, and there is mucous and pus at the eyeball edges. Pain is not reported as a symptom, and when you ask, the patient says neither eye has had any episode of recent stabbing pain. The patient does not have skin lesions on the hands, forearm, feet, ankles, or shins, and also does not show sign of one or more cold sores above, below, or to the side of, the lips and mouth region. You can safely bet that this is a non-viral infection of the anterior ocular membrane, the conjunctiva. The membrane sits loosely upon the white sclera. Be careful not to touch the cornea, because it has many pain receptors and the patient may get startled.
What First Shall I Do?
First, you disinfect the surface of the facial skin at the cheeks and side temples, and frontal brow region, but also the ear lobe cartilage flap, the pinna, on both sides. Do not use alcohol swab wipes— they tend to dry the facial skin and sensitize the eyelid margin, causing tears to overflow. Use a gauze bandage wetted with tap water if you do not have sterile solution, and gently exfoliate as you clean.
Next What Shall I Do?
Find the contact information of the clinic or eye doctor that is situated nearest to you and nearest to the patient who has arrived placing his trust in your hands.
What Questions Must Be Asked?
To get essential information for an acutely inflamed eye, interview the caregiver or the patient, asking these history questions:
A. Is the patient chronically constipated?
B. Does the patient suffer migraine headaches?
C. Did the patient have any recent episode of severe abdominal cramps?
D. Was the person assaulted in a street fight or in a domestic brawl?
E. Did the patient have a slip and fall at work or at home or elsewhere?
F. Does the patient use any eye drops that might be contaminated with bacteria or toxins?
G. Did the patient recently bend forward and downward, or did she perform a yoga headstand or did he lift any heavy objects?
H. Does the patient have a regular eye doctor, OD, or MD, they have seen recently?
I. Does the patient suffer throat irritation and does he use anti-histamines?
J. Has the patient any lung infection with or without chronic cough?
K. Does the patient have nasal congestion, or nasal discharge?
L. Has the patient found her sputum to be yellow or greenish- yellow?
M. Is the patient taking steroid medication eye drops or prednisone pills or injections?
N. When climbing 2 flights of stairs, is there pain at the left or right knee or at the ankle joints?
Cabinet Inventory
3. Do we have reliable vendors for silver nitrate, chlorhexidine, povidone iodide; soframycin, natamycin, and such?
4. Can we stock 7 liters of distilled water?
5. Can we obtain 4 glass bottles, 2 pipettes, 3 droppers, and 12 empty vials?
6. Do have eye pressure lowering eye-drops?
7. Do we have contact lens re-wetting drops?
8. Have we any drops that are antibiotic for gram positive bacteria? Gels? 9. Do we have drops or gel ointments for gram negative bacteria?
10. Does our cabinet stock antifungal eye drops? Ointments?
And These Workspace Questions:
1. Above what workspace counter do we install a UV lamp?
2. Can we purchase empty glass bottles and pipettes and droppers and vials?
3. How many gallons of distilled water should we hold at any given time?
4. Who among us, can be trained and authorized to prepare medications?
Antibiotics Questions
1. Can we locate a vendor to supply us with natamycin?
2. From where do we get soframycin?
Antiseptic questions
1. Is my clinic equipped with 10 percent or 5 percent povidone iodide?
2. From what vendor can we acquire antiseptic solution such as chlorhexidine? 3. Where can we get silver nitrate for the clinic?
In Summary
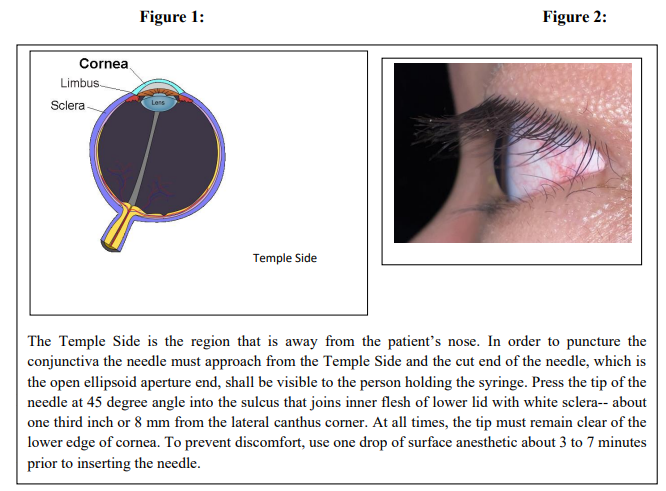
Like Hemingway, if you are an ambulance driving EMT, or a student, enrolled to become a nurse, you may already know how to fill a 10 ml syringe. So now please learn to press-fit upon the nozzle, a 22 gauge needle so as to inject perhaps 3 ml of antiseptic liquid toward resolving conjunctivitis. Soon you may find a happy patient, because you acted in good time [1-25].
Acknowledgement
The authors are keen that such methods be learned and implemented on a wider scale, and for this we have firm resolve from India [Aditya Goyal, OD MS] and South Africa [Kovin Naidoo, OD PhD] and the West Coast USA [Richard C. Hom, OD, PhD] and would you kindly address this to your colleagues, so we find time to support you.
References
- Dorairaj, S., Liebmann, J. M., & Ritch, R. (2007). Quantitative evaluation of anterior segment parameters in the era of imaging. Transactions of the American Ophthalmological Society, 105, 99.
- Lapuerta, P., & Schein, S. J. (1995). A four-surface schematic eye of macaque monkey obtained by an optical method. Vision research, 35(16), 2245-2254.
- Patel, D. V., Zhang, J., & McGhee, C. N. (2019). In vivo confocal microscopy of the inflamed anterior segment: A review of clinical and research applications. Clinical & Experimental Ophthalmology, 47(3), 334-345.
- Singh, S., Jakati, S., Shanbhag, S. S., Elhusseiny, A. M., Djalilian, A. R., & Basu, S. (2021). Lid margin keratinization in Stevens-Johnson syndrome: review of pathophysiology and histopathology. The Ocular Surface, 21, 299-305.
- Bonini, S. (2021). The red eye. European Journal of Ophthalmology, 31(6), 2843-2849.
- Timlin, H., Butler, L., & Wright, M. (2015). The accuracy of the Edinburgh red eye diagnostic algorithm. Eye, 29(5), 619-624.
- Bertolini, J., & Pelucio, M. (1995). The red eye. Emergency medicine clinics of North America, 13(3), 561-579.
- Pettey, J. H., Mifflin, M. D., & Olson, R. J. (2015). Study of the acute effects of povidone–iodine on conjunctival bacterial flora. Journal of Ocular Pharmacology and Therapeutics, 31(10), 627-630.
- Awwad, S., Mohamed Ahmed, A. H., Sharma, G., Heng, J. S., Khaw, P. T., Brocchini, S., & Lockwood, A. (2017). Principles of pharmacology in the eye. British journal of pharmacology, 174(23), 4205-4223.
- Records, R. E., & Ellis, P. P. (1969, January). Subconjunctival antibiotic therapy in ophthalmology with special consideration of the penicillins and cephalosporins. In Transactions of the Pacific Coast Oto-ophthalmological Society Annual Meeting (Vol. 50, pp. 179-193).
- Tripp, G. K., Good, K. L., Motta, M. J., Kass, P. H., & Murphy, C. J. (2016). The effect of needle gauge, needle type, and needle orientation on the volume of a drop. Veterinary ophthalmology, 19(1), 38-42.
- Mascarenhas, M., Chaudhari, P., & Lewis, S. A. (2023). Natamycin ocular delivery: challenges and advancements in ocular therapeutics. Advances in Therapy, 40(8), 3332-3359.
- Hadad, R., Hedengran, A., Barnils, A., Petrovski, G., Cvenkel, B., Utheim, T. P., ... & Kolko, M. (2024). Effect of chlorhexidine, povidone-odine and betadine antiseptic eye drops on cultured human conjunctival goblet cell survival. Acta Ophthalmologica, 102(7), 773-778.
- Mohamed-Ahmed, A. H., Picken, C. A., & Kuguminkiriza, D. (2023). How to prepare chlorhexidine eye drops. Community Eye Health, 36(118), 21.
- Hui, Y. H., So, W. K. W., Ng, M. S. N., Leung, J. T. W., Ho,E. T. L., & Wong, S. S. H. (2021). Treating peritoneal dialysis catheter exit-site granulomas with chlorhexidine swabstick: A pilot study. Journal of Renal Care, 47(2), 103-112.
- Arora, R., Pande, R. K., Panwar, S., & Gupta, V. (2021). Drug-related stevens–johnson syndrome and toxic epidermal necrolysis: A review. Indian journal of critical care medicine: peer-reviewed, oficial publication of Indian Society of Critical Care Medicine, 25(5), 575.
- Isenberg, S. J., Apt, L., Yoshimori, R., Leake, R. D., & Rich,R. (1994). Povidone-iodine for ophthalmia neonatorum prophylaxis. American journal of ophthalmology, 118(6), 701-706.
- Narayanan, V., Motlekar, S., Kadhe, G., & Bhagat, S. (2014). Efficacy and safety of nadifloxacin for bacterial skin infections: Results from clinical and post-marketing studies. Dermatology and Therapy, 4, 233-248.
- Ainslie, D., & Henderson, W. G. (1958). SOFRAMYCIN ITS PENETRATION INTO THE EYE AND ITS EFFECT UPON EXPERIMENTALLY PRODUCED STAPH. AUREUS AND PS. PYOCYANEA CORNEAL INFECTIONS. The British Journal of Ophthalmology, 42(9), 513.
- Zhao, Y., & Lei, W. (2015). Retina penetration of subconjunctival ranibizumab injection in the rabbit eye. [Zhonghua yan ke za Zhi] Chinese Journal of Ophthalmology, 51(5), 356-359.
- Niederkorn, J. Y. (2002). Immune privilege in the anterior chamber of the eye. Critical Reviews™ in Immunology, 22(1).
- Bilkhu, P. S., Wolffsohn, J. S., & Naroo, S. A. (2012). A review of non-pharmacological and pharmacological management of seasonal and perennial allergic conjunctivitis. Contact lens and anterior eye, 35(1), 9-16.
- Guidotti, T. L. (1994). Occupational exposure to hydrogen sulfide in the sour gas industry: some unresolved issues. International archives of occupational and environmental health, 66, 153-160.
- Lambert, T. W., Goodwin, V. M., Stefani, D., & Strosher, L. (2006). Hydrogen sulfide (H2S) and sour gas effects on the eye. A historical perspective. Science of the total environment, 367(1), 1-22.
- Claassen, K., Dos Anjos, D. R., & Broding, H. C. (2021). Current status of emergency treatment of chemical eye burns in workplaces. International journal of ophthalmology, 14(2), 306.