


Research Article - (2023) Volume 1, Issue 2
Indigenous Knowledge and Perception Toward Mental Illnesses Within Goma City in Democratic Republic of Congo
2Department of Internal Medicine, Faculty of Human Medi- cine, University of Goma (UNIGOM), Democrati, Republic of the Congo
3Department of Psychiatry, School of Medicine, College of Health Sciences, Makerere University Kampal, Uganda
4Department of Plant Sciences, Microbiology and Biotech- nology, School of Biological Sciences, Colle, Uganda
Received Date: Aug 12, 2023 / Accepted Date: Sep 14, 2023 / Published Date: Oct 12, 2023
Copyright: ©Â©2023 Samuel Kule Kyolo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Kyolo, S. K., Bbosa, G. S., Odda, J., Mwebaza, N., Kibendelwa, Z. T., et al. (2023). Indigenous Knowledge and Perception Toward Mental Illnesses Within Goma City in Democratic Republic of Congo. Transl Med OA, 1(2), 56-67.
Abstract
Background: Prevailing wars for more than two decades have been associated with the increased burden of mental illness- es (MIs) in North-Kivu province (NKP), in Democratic Republic of Congo (DRC). The community perception of this claim has, however, not been fully documented.
Aims: To assess the knowledge and perception of Goma city residents on MI and their associated factors.
Methods: Cross sectional study, was conducted among 610 selected community residents including key informants of Goma city from April to July 2021. Quantitative data from semi-structured interviews was analyzed using descriptive statistics and binary logistic regression, while data from Focus group discussions (FGDs) were analyzed using qualitative thematic analysis.
Results: Among residents of Goma city, rates of correct recognition of MIs namely schizophrenia, anxiety, depression and neurodevelopment disorders varied: 96.6%, 29.7%, 39.5% and 14.3%, respectively. The major causes of MIs perceived by respondents were spiritual (67.5%) and substance abuse (56.7%). Qualitative data from FGD’s revealed three major themes for poor perception of MI among residents as indigenous names of various MIs, reason of preferring traditional medicine versus conventional medicine (CM) and challenges faced in management of MIs using CM. Furthermore, demo- graphic factors such as education, religion, occupation and age were not statistically significant (p�?0.05) in predicting one’s odds of MI perception among Goma city residents.
Conclusion: The findings revealed that residents of Goma city have poor knowledge and perception on MIs regardless of education, religion, occupation and age.
Keywords
Indigenous, Knowledge, Perception, Mental Illnesses, Goma City Residents
Introduction
Mental disorders remain among the top ten leading causes of trouble worldwide, with no evidence of global reduction in the burden since 1990 [1]. Despite of the effort provided by WHO to reduce the burden, the prevalence of MIs in sub-Saharan African countries particularly due to wars and conflicts remains high [2]. Overall, in many sub-Saharan countries, amidst constrained small health budgets, less than 1% is reported to be spent on mental health, and a lot of which is misused at institutional care [3]. In DRC where there is persistent wars and conflicts, the prevalence of depression and anxiety have been reported to be 22% and 13-23% in most affected provinces especially in NKP and more so in Goma city as compared to other provinces in the country [4,5]. In these provinces, the major risk factors to MIs include; exposure to war and its collateral effects such as poverty, torture, refugee camps, human trafficking, loss of family members, stress of immigrants adapting to a new culture, sexual abuse, among many others [6].
The mental illnesses in DRC have been ranked among the top global mental health burden [7]. The problem is further aggravated by poor health infrastructure. The North-Kivu province has only one psychiatrist for a population of 1.1 million [8]. Psychiatric nurses and psychologists are limited in the country, and the primary healthcare personnel do not treat MI, so many people with MIs have no access to conventional treatment [9]. The situation is similar in many other sub-Saharan African countries where there is limited number of mental health professionals, low investment, stigma in the local communities and many others and this has led to allopathic practitioners shun taking mental health as a career option [4].
Majority of the indigenous Eastern Congolese communities believe that most cases of MIs have been reported to be of supernatural causes including sorcery, curses, punishment, etc. [10]. Thus, many Congolese believe that ‘’in the case of sorcery, one should go to a Traditional Health Practitioner (THP) and in the case of bad spirits, one has to chase the spirit away by praying and practicing rituals in the church, and in the cases that do not have a supernatural cause, one should go to the hospital’’ [11]. The limited access to professional mental healthcare, in addition to prevailing cultural beliefs have led to Goma city residents to use alternative spiritual and THPs, some of whom employ abusive practices such as chaining patients, physical abuse and food deprivation as well as use of herbs with no valid scientifically proven evidence [12].
It has been further reported that the concept of mental health disorders is determined by many factors, including the historical context, cultural influence, low level of scientific knowledge and capacity to carry out scientific inquiry, level of education in certain circumstances amongst others [13]. Despite of increased prevalence of MIs in NKP, less is known on Goma city community perception toward MIs due to negative impact of war conflict on mental health, scarcity of psychiatric services and cultural influence. This study sought to find out knowledge and perception towards MI among Goma city residents and their associated factors.
Methodology
Study Design
This was a community based cross-sectional study. Both quantitative and qualitative study designs were employed using semi-structured interviews, open ended key informant interviews and FGDs.
Study Area
The study was conducted in Goma city, capital of NKP located in eastern part of DRC from April to July 2021. Overall, the city has multi tribal population of 1.1 million urban habitants and has an area of 66,452 Km². The city has two communities, Goma and Karisimbi which are subdivided into 7 and 11 quarters respectively (Figure1) [14]. Each quarter of the community is subdivided into cells with several streets. The community of Goma is located in the South of Goma city, and has an area of 28.754 Km2 and hosts almost all political, administrative and economic businesses. On the other hand, the community of Karisimbi is located in the North of Goma city and has an area of 37.698 Km2. The community is essentially residential and has population of 622,105 habitants [15]. Data on community knowledge, perception of MIs and related symptoms were collected from the community of Karisimbi. It is residential and hosts a population with low income thus living in poverty and for them to meet their healthcare needs, they utilize alternative medicine especially in form of medicinal plants (MPs). Several studies conducted in Goma city have reported the use of herbal medicines in the community [16]. Focus group discussions were held in hospital of specialized medicine and traditional medicine (TM) centers located both in Goma and Karisimbi communities. Key informants’ opinions were sought from conventional health practitioners (CHPs) on community knowledge and perception toward MIs as well as knowledge about indigenous treatment of MIs from THP’s in the city.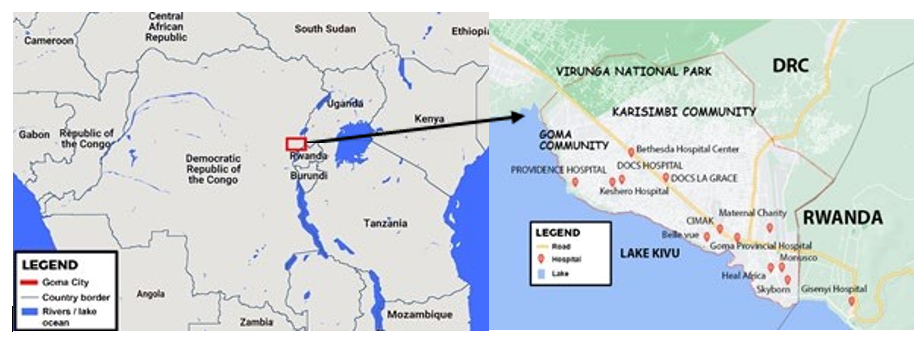
Figure 1: Map, showing the Study Setting Adapted from Operational Vulnerability Index map of Goma (Evaluating population vulnerability to volcanic risk in a data scarcity context, 2021)
Study Population
Both adult male and female residents of Goma city, aged between 18 years and above, as well as hospitals registered by directorate of health of NKP were involved in the study.
Selection Criteria of Respondents
Firstly, for the resident community, only consenting respondent that were neither THPs nor CHPs were included in the study. Secondly, for key informant’s access, among hospitals registered by directorate services of NKP to provide specialized health care (SPHC) within Goma city including MIs, only those consenting for participation were included in the study. Thirdly, medical doctors, psychologists and nurses from the selected hospitals, providing SPHC including MIs in Goma city, only willing and consented staff members were included in the FGDs. Finally, we selected THPs dealing in MIs management within Goma for the FGDs. Overall, respondents who did not consent and those who were absent at the time of data collection were excluded from the study.
Sample Size Determination
Single proportion formula was used to determine sample size of Goma city residents recruited in the study for the semi-structured interview (Singh, 2014), where n1 was the initial sample size, considering a confidence level of 95%, an estimated overall proportion of good perception about MIs management of 50% and a precision of 5%.
n1=(1.962X 50(1-50))/52
= 376.48
The sample size n2 were calculated after using a finite population correction, where N was the total number of target population, especially, population of community of Karisimbi that is 622,105 of inhabitants and considering that 55.18% of population of DRC has age range between 18 years and above (Annuaire de statistique, 2014). We obtained the total number of corrected target population as follows: 0.5518 X 622 105= 343 278 habitants, thus:
To obtain a final sample size of respondents that met inclusion criteria, n2 was multiplied by 1.5 to account for the clustering effect and adding a 15% of non-response rate. Thus, final sample size = (376.07 X 1.5) + (376.07 X 0.15) = 620 residents of Karisimbi community that met inclusion criteria. Furthermore, sample size of CHP and THP in one FGD was n=10 of those who met selection criteria in line with Anita et al. The sample size of hospitals providing specialized health care including MIs was the total number of those that satisfied selection criteria.
Sampling Procedure
A multistage sampling procedure including geographical cluster, stratified random and snowball sampling were used. First, the community of Karisimbi of Goma city was divided into 11 quarters according to administrative map from City Town Hall (all quarters were included in the study). The second stage consisted selection of 2 cells of interest in each quarter by simple random sampling, considering administrative list of cells obtained from the Town Hall. The third stage involved the selection of 4 streets of interest in each selected cell by simple random sampling considering list of streets got from the Town Hall. Fourth, the strata were based on gender of participants, especially individuals in community non-THP and non-HCP; from 4 streets previously selected, male and female respondents were randomly selected. The fifth stage was selection of household residents from selected streets, each consisting of about 60–80 household units. The households were enumerated in each selected street and were then randomly selected to give 7 households by street that was required to meet the desired sample size (about 57 households in each quarter) of n=620 residents that satisfied inclusion criteria. Resident who satisfied selection criteria were approached for participation in each selected household. The age-order method was used to identify the potential respondent and no replacement was made [17]. The sixth stage involved the selection of THPs dealing in MIs within Goma city by snowball method using information given by residents of Karisimbi community. Furthermore, selection of hospitals providing SPHCs including MIs in Goma city for FGDs was by expert sampling method based on selection criteria. This was followed by expert sampling, using information from directorate of health services of NKP that was used to select CHPs working in hospital. Finally, Elderly Traditional Health Practitioners (ETHPs) expert in management of MIs by snowball sampling based on information given by other THPs were selected.
Procedure of Data Collection
Permission to collect data from individuals in Goma city was got from the Directorate of Health Services in Goma city. Secondly, permission was got from administrative leaders before any interaction with prospective respondents. Thereafter researcher interacted with prospected respondent through face to face interview following four steps; especially: (1) Interaction with each selected residents of Karisimbi community who documented their knowledge, perception on MIs, and THPs dealing in MIs management; (2) Interaction with each FGDs including selected CHPs to obtain their opinion on MIs frequency among patients and its management by CM and by TM, (3) Interaction with each FGD including THPs to select ETHPs expert in management of MIs; and (4) Interaction with ETHPs for obtaining common medicinal formulation. Overall, researcher started their interaction with each prospective respondent by first explaining the aims and objectives of the project in order to solicit their consent and cooperation before any data were gathered.
Data Collection Tools
For quantitative study, data from selected residents of Karisimbi community, were collected through face to face semi-structured interviews by using interview schedule translated into French and local language (Kiswahili). For qualitative study, data were collected through FGD using interview guide translated into French and local language (Kiswahili). The interview schedule related to selected residents of Karisimbi community involved domains including socio-demographic data, knowledge and perception on MIs, and THP dealing in MIs. While the interview guide related to FGDs including CHPs had 8 themes. The themes included socio-demographic data; opinion of CHPs on MIs commonly managed in CM; common MIs among patients according to most affected age group and gender; nomenclature of MI by indigenous residents of Goma city; types of management commonly used in CM in Goma city; reason of preferring TM vs CM and challenges faced by the CHPs in the use CM to manage MIs. Interview guide involving THP included three domains including socio-demographic data, ETHPs expert in management of MIs in Goma city and formula used in MIs management respectively.
Validity and Reliability of Data Collection Tools
To ensure the validity of interview schedule and interview guide and in order to obtain the content validity, the tools were revised by 5 experts including; pharmacologist, psychiatrist and statistician. The reliability analysis of interview schedule was done by test-retest reliability using data from the pilot study. So, Pearson’s correlation coefficient formula for estimation of reliability was done according to Sramah & Bora (2012) with r= 0.84. Reliability of interview guide was measured though dependability and conformability as suggested by Guba and Lincoln for qualitative research.
Data Management and Analysis
Data were entered in excel 2016 and then transferred to SPSS statistical package version 17 for analysis. The data were subdivided by section according to various domains involved in the study; each section had a separate file. An electronic data base (excel) was created in which data were entered and this was continuously updated. Data were double entered for accuracy. The data base information necessary to answer our research questions were exported to the SPSS statistical package for analysis. Raw data were cleaned scrutinizing the completed research instruments to identify and minimize, as far as possible, errors, incompleteness, misclassification and gaps in the information obtained from the respondents. Having cleaned, the data were coded following the process including developing a pretested and verified code book. Quantitative data were analyzed using both descriptive statistics and binary logistic regression to determine perception of Goma city residents on MI and its associated factors. A proportion ÃÃÂ???50% was considered as good or reported by majority while proportion ÃÃÂ???50% was considered as poor or reported by minority of respondents. Qualitative transcribed data using Microsoft Word 2018 were closely studied according to the following steps: (1) identifying the main themes communicated by respondent, (2) assigning codes to the main themes, (3) classifying responses under the main themes, (4) content analysis of responses of main themes.
Ethical Consideration
The study was approved by research committee of the Department of Pharmacology and Therapeutics, and the School of Biomedical Sciences Research and Ethics Committee at Makerere University College of Health Sciences with approval protocol number SBS-841. The background, procedure and the aims of the study were communicated orally to all respondents. Assurance was given to all participants that information would be kept confidential, participation in study is voluntary, they my freely decide to withdraw from the study at any time and that no payment would be given for participating. Anonymity was maintained throughout the study, all respondents were not identified by name in any report or publication. All respondents gave their informed consent in writing, prior to participation. The study was conducted in accordance with the Helsinki declaration on use of human subjects in research.
Results
During data Processing Respondent rate of 98.4% was yielded; 610 out of 620 interview questionnaires were selected for analysis, 10 respondents were excluded due to gross incompleteness. Focus group discussions involving THP and HCP included 10 respondents and 6 selected ETHPs who were approached for documenting common formula used in drug preparation for MI.
Socio Demographic Characteristics of Respondents
About half (50.5%) of respondents, non-CHPs and non-THPs (n=610) were female, more than 50.0% of respondents were 28 years old and above; 40.8% were peasant and majority (51.5%) of them had education status of secondary school and were protestant by religion. Majority of respondents in FGDs including CHPs were male (n=24/40, 60%), 72.5% of whom were 28 years old and above, 55.0% of whom were nurses and had dealt in MIs management for 6 years and above. On the other hand, the majority of THPs (65.1%) were male with secondary school level of education. All ETHPs were 47 years old and above with secondary school level of education, herbalists with ≥ 6 years of experience and 83.3% of them were male (Table 1).
Table 1: Socio Demographic Characteristic of Respondents
|
Variable |
A (n=610) |
B (n=40) |
C (n=43) |
D (n=6) |
|
F (%) |
F (%) |
F (%) |
F (%) |
|
|
Age |
||||
|
18-27 |
167(27.4) |
11(27.5) |
2(4.6) |
0(0.0) |
|
28-36 |
202(33.0) |
17(42.5) |
12(27.9) |
0(0.0) |
|
37-46 |
145(23.8) |
9(22.5) |
14(32.6) |
0(0.0) |
|
47-55 |
73(12.0) |
2(5.0) |
11(25.6) |
4(66.7) |
|
56-64 |
23(3.8) |
1(2.5) |
4(9.3) |
2(33.3) |
|
Gender |
||||
|
Male |
302(49.5) |
24(60.0) |
28(65.1) |
5(83.3) |
|
Female |
308(50.5) |
16(40.0) |
15(34.9) |
1(16.7) |
|
Education level |
||||
|
Uneducated |
110(18.0) |
0(0.0) |
0(0.0) |
0(0.0) |
|
Primary school |
97(15.9) |
0(0.0) |
0(0.0) |
0(0.0) |
|
Secondary school |
314(51.5) |
4(10.0) |
29(67.4) |
6(100.0) |
|
University |
89(14.6) |
36(90.0) |
14(32.6) |
0(0.0) |
|
Occupation/Profession |
||||
|
Merchant |
226(37.0) |
- |
- |
- |
|
Government employee |
25(4.1) |
- |
- |
- |
|
Farmer |
4(0.7) |
- |
- |
- |
|
Peasant |
249(40.8) |
- |
- |
- |
|
Others |
106(17.4) |
- |
- |
- |
|
Residence |
||||
|
Goma |
0(0.0) |
14(35.0) |
9(20.9) |
1(16.7) |
|
Karisimbi |
100(100.0) |
26(65.0) |
34(79.1) |
5(83.3) |
|
Religion |
|
|
|
|
|
Catholic |
191(31.3) |
21(52.5) |
16(37.2) |
2(33.3) |
|
Protestant |
314(51.5) |
19(47.5) |
20(46.5) |
3(50.0) |
|
Muslim |
61(10.0) |
0(0.0) |
3(7.0) |
0(0.0) |
|
Traditionalist |
44(7.2) |
0(0.0) |
4(9.3) |
1(16.7) |
|
CHP status |
||||
|
Medical Doctor |
- |
13(32.5) |
- |
- |
|
Nurse |
- |
22(55.0) |
- |
- |
|
Psychologist |
- |
3(7.5) |
- |
- |
|
Ergotherapeutist |
- |
1(2.5) |
- |
- |
|
Social assistant |
- |
1(2.5) |
- |
- |
|
TH status |
||||
|
Divina diagnostician |
- |
- |
0(0.0) |
0(0.0) |
|
Herbalist |
- |
- |
43(100.0) |
6(100.0) |
|
Other |
- |
- |
0(0.0) |
0(0.0) |
|
Number of year of experience |
||||
|
<1 year |
- |
3(7,5) |
5(11,6) |
0(0.0) |
|
1 to 5 years |
- |
15(37.50) |
35(81,4) |
0(0.0) |
|
6 years and above |
- |
22(55.00) |
3(7,0) |
6(100.0) |
A: Non-Traditional Health Practitioners and non-Conventional Health Practitioners residents of Goma city; B: Conventional Health Practitioners; C: Traditional Health Practitioner; D: Elder Traditional Health Practitioners; F: frequency; -: not applicable; n: sample size; (%)=F/n
Distribution of Respondent’s Recognition of Existence of MIs Among Residents of Goma City
Majority of the respondents (85.7%) recognized that MIs exist in Goma city, 71.3 % argued that there were various categories of MIs in the city. Also, the majority (96.6%) asserted that schizophrenia is the main category of MI that existed in Goma city. However, a low proportion (29.7%) of respondents recognized existence of anxiety in Goma city; likewise, a low proportion (39.5%) recognized the existence of depressive disorders (DD). Furthermore, 14.3% of respondents recognized existence of neurodevelopmental disorders (NDD) in the city (Table 2).
Distribution of Respondent’s Perceived Symptoms of Anxiety, Schizophrenia, Depression and Neurodevelopmental Disorders Among Residents of Goma City
Among a total number of 610 respondents, the majority (86.6%) perceived bizarre behavior as major characteristic symptom of schizophrenia. However, no major symptom of DD, anxiety and NDD such as defined in CM was reported by the majority of respondents (Table 3).
Table 2: Distribution of Respondent’s Recognition of Existence of MIs Among Residents of Goma City
|
No |
Questions |
Male individuals response pattern, n=610 |
||
|
Yes |
No |
Not sure |
||
|
F(%) |
F(%) |
F(%) |
||
|
1 |
On your opinion, do MIs exist in Goma city? |
523(85.7) |
7(1.2) |
80(13.1) |
|
2 |
Are there various category of MI? |
435(71.3) |
45(7.4) |
130(21.3) |
|
3 |
Are there patients with anxiety disorders? |
181(29.7) |
37(6.0) |
392(64.3) |
|
4 |
Are there patients with schizophrenia? |
589(96.6) |
0(0.0) |
21(3.4) |
|
5 |
Are there patients with DD? |
241(39.5) |
28(4.6) |
341(55.9) |
|
6 |
Are there patients with NDD? |
87(14.3) |
47(7.7) |
476(78.0) |
F: Frequency; DD: depressive disorders; NDD: neurodevelopmental disorders; n: sample size, %=F/n
Distribution of Respondents’ Perceived Cause of MIs Among Residents of Goma city
Among 610 respondents, the majority affirmed that cause of MIs is spiritual (67.5%) or substance abuse (56.7%) (Table 4).
Distribution of Factors Associated With Perception of MIs Among Residents of Goma city
Binary logistic regression model was performed to see whether education, religion, occupation and age were associated with perception of MIs in Goma city. The overall model was found to be statistically significant (Chi-squared value 10 = 15.28, p< 0.05), with Nagelkerke R-squared value of 0.42. However, education, religion, occupation and age were found not to be statistically significant in predicting one’s odds of MI perception (p>0.05) (Table5).
Table 3: Distribution of respondent’s perceived symptoms of anxiety, schizophrenia, depression and neurodevelopmental disorders among residents of Karisimbi community
|
Mental illness |
Symptoms |
Response pattern, n=610 |
|
|
Yes |
No |
||
|
F(%) |
F(%) |
||
|
Anxiety |
|||
|
|
Persistent fear |
34(5.6) |
576(94.4) |
|
|
Persistent worry |
140(23.0) |
470(77.0) |
|
|
Increased heart rate |
14(2.3) |
596(97.7) |
|
Schizophrenia |
|||
|
|
Agitation |
256(42.0) |
354(58.0) |
|
|
Confusion |
146(23.9) |
464(76.1) |
|
|
Bizarre behavior |
528(86.6) |
82(13.4) |
|
DD |
|||
|
|
Hypersomnia/ insomnia |
26(4.3) |
584(95.7) |
|
|
Persistent sadness |
82(13.4) |
528(86.6) |
|
|
Lose of interest in enjoyable thing |
22(3.6) |
588(96.4) |
|
|
Headache |
26(4.3) |
584(95.7) |
|
|
Anger |
60(9.8) |
550(90.2) |
|
NDD |
|||
|
|
Metal disability |
36(5.9) |
574(94.1) |
|
|
Physical disability |
22(3.6) |
588(96.4) |
F: Number of response; DD: depressive disorders; NDD: neurodevelopmental disorders; n: sample size; %=F/n
Table 4: Distribution of respondents’ perceived cause of MIs among residents of Goma city
|
Risk factors/causes of MIs |
Response pattern, n=610 |
|
|
Yes |
No |
|
|
F (%) |
F (%) |
|
|
Hereditary |
250(41.0) |
360(59.0) |
|
Spiritual |
412(67.5) |
198(32.5) |
|
Trauma |
234(38.4) |
376(61.6) |
|
Political and social unrest |
56(9.2) |
554(90.8) |
|
Substance abuse |
346(56.7) |
264(43.3) |
|
Disease/infections |
50(8.2) |
560(91.8) |
|
High IQ |
198(32.5) |
412(67.5) |
|
Poor diet/malnutrition |
6(1.0) |
604(99.0) |
|
Unknown |
4(0.7) |
606(99.3) |
|
Warm season |
4(0.7) |
606(99.3) |
IQ: Intelligence quotient; F: Number of response; n: sample
size; %=F/n
Table 5: Binary Logistic Model for Associated Factors with community’s Perception of MIs in Goma City
|
Variable |
Chi-squared value (1) |
p-value |
OR |
CI |
|
Occupation |
0.01 |
0.92 |
0.99 |
0.81-1.21 |
|
Religion |
0.04 |
0.85 |
0.98 |
0.80-1.21 |
|
Age |
2.10 |
0.15 |
0.93 |
0.84-1.03 |
|
Education |
0.10 |
0.76 |
1.04 |
0.84-1.28 |
OR: Odds ratio, CI: Confidence interval
Mental Illnesses Commonly Managed in CM within Goma City
Schizophrenia, anxiety, DD, NDD and mania were reported by respondents in FGDs as MIs managed at specialized hospitals in Goma city. All FGDs reported that schizophrenia and complicated cases of others MIs are referred to specialized center in mental health named ‘’Santé Mental’’ located in Goma, NK province.
Table 6: Emergent themes from Qualitative Analysis of FGD: Proposed Most Affected Age Group and Gender
|
Mental illness |
Age group (year) |
Gender |
|
Schizophrenia |
18-35 |
Male |
|
Anxiety |
18-35 |
Female |
|
Depression |
18-40 |
Female |
Common MIs Among Patients According to Most Affected Age Group and Gender
Male individuals of 18 to 35 years old were reported by FGD to be the most affected by schizophrenia. The gender and age group reported to be the most affected by anxiety were females from 18 to 35 years old. Also, females from 18 to 40 years old were reported to be the most affected by DD (Table 6).
Nomenclature of MI by Indigenous Residents of Goma City
Focus group discussions including CHPs reported how residents in Goma city communities termed various categories of MIs when they seek help from hospital. The local terms used were contextually defined according to indigenous residents of Goma city. Responses of FGDs were summarized in Table 7. The first category was termed ‘’mazimu’’ (Swahili) which meant bad spirits characterized by bizarre behaviors. All FGDs reported that indigenous people believed that patients with ‘’mazimu’’ were possessed by malevolent spirits, cursed or punished by ancestors or God. According to CHPs in FGDs, patients with ‘’mazimu’’ were found to suffer from psychosis when they were admitted in hospital. The second category of MI was termed ‘’woga’’(Swahili) which meant intense fear characterized by ‘’malali ya moyo’’ (Swahili), ‘’tension’’ (French), or sumu (Swahili) which meant increased heart rate, high blood pressure or poisoning respectively. According to FGDs, patients admitted in hospital with ‘’woga’’ were diagnosed with generalized anxiety disorder (GAD). The third category was termed ‘’mateso’’ (Swahili) which was translated as social unrest or trauma. Respondents in FGDs reported that residents of Goma city characterized ‘’mateso’’ by some symptoms including ‘’anoréxie’’ (French), dépassé (French) and ‘’indifférent’’ (French) which meant anorexia, being overwhelmed and loss of interest for enjoyable things respectively. Focus group discussions reported that people with ‘’mateso’’ were found to suffer from major DD when they were admitted in hospital. The fourth category was termed ‘’ulozi’’ (Swahili) which meant sorcery characterized by ‘’shindikana’’ behavior (Swahili) which meant insolent, gang member or street urchin. Focus group discussion reported that patients admitted in hospital with ‘’ulozi’’ disease were found to suffer from mania when seeking help from hospital. The last reported category was ‘’kiwerere’’ (Swahili) which meant idiot characterized by Kizengi (Lingala) which meant stupid behavior. According to FGDs, kiwerere patients were diagnosed as having NDD when their parents sought help from hospital.
Table 7: Emergent themes from Qualitative Analysis of FGD: Indigenous Names of Various MIs in Goma City
|
Mental illnesses |
Cited local name |
Symptoms |
|
Schizophrenia |
Mazimua, |
Bizarreb |
|
Anxiety |
Bogaa, sumua |
Malali ya moyoa, tensionb, |
|
Depression |
Matesoa, dépasséb |
Anoréxieb, depasséb, indifférenceb, |
|
Mania |
Bulozia, |
Shindikanaa |
|
Neurodevelopmental disorders |
Kiwelewelea, |
Kizengic |
a: Local name in Congolese Swahili; b: local name in French; c: local name in Lingala
Types of MIs Management Commonly Used in CM in Goma City
Responses from FGDs are summarized in Table 8. Participants in FGDs reported conventional antipsychotic drugs, psychotherapy and socio professional occupation as common type of management for schizophrenia; conventional anxiolytic drugs, conventional antidepressant drugs, psychotherapy and prayer as common treatment of anxiety; and conventional antidepressant drugs and prayer for treatment of DD. However, participants reported rehabilitation as common method for management of NDD in Goma city.
ost Preferred Mode of Treatment for MIs by Residents of Goma City
Traditional medicine was cited by all participants in FGD as the most preferred of mode of treatment of MIs in Goma city.
Reason of Preferring TM Versus CM
Participants in focus groups reported that indigenous residents in Goma city prefer TM as a form of treatment for some reasons including the fact that: (1) THP reveal the cause of MI, (2) Residents of Goma city have poor of knowledge on MIs, (3) People in Goma city believe that MI are caused by evil spirits or curse, (4) Management used in TM is adapted to all diseases, (5) There is claim that patient recover fully from MI with TM than CM.
Table 8: Emergent themes from Qualitative Analysis of FGD: Commonly Types of Management Used for MIs in CM in Goma City
|
Mental illnesses |
Cited type of MI management in CM in Goma city |
|
Schizophrenia |
Conventional antipsychotic drugs, psychotherapy, socio-professional occupation |
|
Anxiety |
Conventional anxiolytic and antidepressant drugs, psychotherapy, prayer |
|
Depression |
Conventional antidepressant drugs, prayer |
|
Neurodevelopmental disorder |
Rehabilitation |
Selected Formula Used in Treatment of MIs in Goma City DRC
Interviewed ETHPs (n=6) reported two MPs including Euphorbia abyssinica (J.F.Gmel), Musa parassidiaca, for psychosis, two MPs including Arachis hypogaea L. and Cleome gynandra L. for anxiety as well as Conyza sumatrensis (Retz) E.Walker for depressive disorders. Information on their scientific name, local name, family, part used, quantity, drug preparation and dosages are summarized in Table 9.
Table 9: Common Formula used in Treatment of MI
|
A. Formula for psychosis |
|||
|
Plant scientific name |
Local name |
Part used |
Quantity |
|
Euphorbia abyssinica (J.F.Gmel) (Euphorbiaceae) |
Kiduha |
Leaves |
10drops of sap |
|
Musa paradisiaca L. (Musaceaea) |
Ndizi, |
Juice from fruits |
1 to 3 Ndizi |
|
Preparation |
|||
|
Extract raw sap from E. abyssinica (J.F.Gmel) leaves |
|||
|
Extract raw juice from M. paradisiaca fruits |
|||
|
Mixt 10 drops of the extracted raw sap of E. abyssinica (J.F.Gmel) with 30ml of the M. paradisiaca L fruit juice |
|||
|
Dosage |
|||
|
By oral route: |
|||
|
Adult: 2 soup spoons 3 times per day during 20 days |
|||
|
Child: 1 tea spoon 3 times per day during 20days |
|||
|
B. Common formula for anxiety |
|||
|
Arachis hypogaea L. (Fabaceae) |
Kalanga |
Leaves |
10 to 20 leaves |
|
Cleome gynandra L. (Capparaceae) |
Musovyo |
Leaves |
5 Leaves |
|
Preparation |
|||
|
Infuse 10 to 20 leaves of A. hypogea L. dry leaves in 1 glass of water |
|||
|
Crush about 5 fresh leaves of C. gynandra L. and extract juice |
|||
|
Dosage |
|||
|
By oral route: A. hypogea L.: ½ glass per day |
|||
|
By nasal route: C. gynandra L.: Instil 2 drops into the nostrils or eyes 2 times per day |
|||
|
C. Common formula for depression |
|||
|
Conyza sumatrensis (Retz) E.Walker, (Asteraceae) |
Kavingande |
Leaves |
About 5 leaves |
|
Preparation |
|||
|
Crush about 5 leaves of C. sumatrensis (Retz) E.Walker to extract juice, or |
|||
|
Boil about 20 leaves of C. sumatrensis (Retz) E.Walker in 1 glass of water to obtain decoction |
|||
|
Dosage |
|||
|
Nasal or ocular route: 2 or 3 drops per day during 3 weeks |
|||
|
Oral route: ½ glass of decoction once per day during 3 weeks |
|||
Challenges that Face HCP in the use CM to Manage MI
Major Challenges reported by FGD included: (1) Poor perception of Goma city resident toward MI leading them to delay for conventional treatment, (2) Lack of evidence on the effectiveness and safety of practices used by THP in management of MI, (3) Lack of collaboration between TM and CM in management of MI.
Opportunities Envisaged by HCP in Future for Management of MI
All FGD suggested collaboration between CM and TM of Goma city for effectiveness of management of MI.
Discussion
The majority of responds that were neither HCP nor CHP recognized schizophrenia as MI in Goma city. However, a low proportion of respondents recognized anxiety, DD and NDD as MI (Table 2). This trend was similarly reported by Benti et al. in communities of Gimbi town, Ethiopia, where the proportion of respondents who recognized schizophrenia as MI was 94.9% and the proportion of respondents who recognized anxiety as MI was low [18]. Also, Jingyi et al. and Wang mental health literacy studies among residents in Shanghai, anxiety was misclassified by respondents [19]. However, a study done by Reavley et al. in Australian communities found that the proportion of respondents who recognized schizophrenia and depression were 37.0% versus 96.6% in the current study [20]. Difference in findings could be justified by the fact that MI literacy differs from a culture to another [21]. Despite the difference, results suggested that residents of Goma city had poor knowledge on DD, anxiety and NDD.
Bizarre behavior was the major symptom of schizophrenia perceived by the majority of respondents. However, major symptoms of DD, anxiety and NDD were reported at low proportions by respondents (Table 3). Likewise, the result of the study reported by Ventevogel et al. showed that people of Butembo city, located from about 380 Km, were able to describe psychotic disorders as a syndrome of severe behavioral disturbances [21]. The study done by Jingyi et al. in Shangai reported that 41.0% of most people consider symptoms of anxiety as normal [19]. Also, the study done by reported that residents of Butembo, in NKP understood persistent sadness as an adaptive reaction to a situation of distress rather than as a MI [4]. This result suggested that respondents had poor perception of symptoms of anxiety, DD and NDD as MI.
The major causes of MIs in Goma city perceived by the majority of respondents were malevolent spirits and drug abuse (Table 4). Similar perceptions were reported by Benti et al. in Gimbi Town, western Ethiopia, where majority of the respondents attributed the cause of MIs to supernatural causes like evil spirit, God’s punishment, and witchcraft [18]. Regarding substance abuse, DRC has been reported to be the most producers of Cannabis sativa, plant reported to be associated with psychosis, across African continent [23]. The fact that residents of Goma city attributed MIs to spiritual cause suggested their poor knowledge and perception toward the condition.
Education, religion, occupation and age were not statistically significant in predicting one’s odds of MI perception (Table 5). This means that any resident of Goma city perceived the same causes of MIs regardless of education, religion, occupation and age. This was similar to what was reported in Iraq and India with no significant association found with age regarding the community’s view of MI [24,25]. However, this finding was not in agreement with the studies done in Agaro town and Nigeria that found out that perception of MIs correlated with educational level [26,27]. It has been reported that religion is a significant factor in mental health and it was perceived to have both positive and negative impact on perception of MI [28]. However, the study was limited to Christian populations in USA that could be socio-culturally different from Goma city population.
In FGD, MIs were perceived by CHP as defined according to American Psychiatric Association whereas, residents of Goma city that were neither HCP nor CHP perceived MIs according to their socio-cultural background [29]. Schizophrenia, anxiety, depression, neurodevelopmental disorders and mania were reported by FGD as MIs managed at specialized hospitals in Goma city. Focus group discussions reported the existence of the five MIs including schizophrenia, mania, anxiety, DD and NDD as common in Goma city unlike residents that were neither HCP nor CHP of Goma city whom the majority recognized schizophrenia as the commonest MIs in the city but ignored mania, anxiety, DD and NDD as MI in the city. This finding suggested poor knowledge of MI by residents of Goma city. Male individuals of 18 to 35 years old were reported by FGD to be the most affected by schizophrenia. The gender and age group reported to be the most affected by anxiety were females from 18 to 35 years old. Also, females from 18 to 40 years old were reported to be the most affected by DD. WHO reported similar result that depression and anxiety disorders are more common among females than males [30].
To be possessed by bad spirit and bizarre behavior were reported by FGD participants as word used by mental ill patient’s family during medical consultation to name or characterize schizophrenia. Fear; increased heart rate; high blood pressure and poisoning were reported by participants in FGDs as words used by patients to nominate anxiety. Social unrest or trauma, anorexia, loss of interest for enjoyable things and being overwhelmed were reported as names or characteristics of depression. Also, sorcery; gang member or street urchins were reported by participants in FGD as words used in Goma communities to nominate a person with mania. Furthermore, word idiot and stupid was reported by respondents as the name and characteristic of NDD in indigenous residents of Goma city. This finding suggested that Goma city residents had their own terms to perceive and recognize MIs and their symptoms. This could be their traditional diagnostic tool in relation to use of herbal medicine. There is need however to harmonize and obtain evidence based diagnosis of MIs in the city. Somewhere, residents of Goma city did not recognize those symptoms as MIs. Similar findings were reported by Spinosa (2016) as reported before, in Butambo culture aforementioned symptoms of depression and anxiety are rather an expression of someone not doing well and being overwhelmed by the tasks of life. Also, this finding suggested poor perception of MIs in the city.
Participants in FGD reported prayer among common methods for management of MIs in Goma city. The finding regarding prayer suggested the positive role of religion in management of MIs in the city which have been reported by others authors in previous studies [31]. Traditional medicine was cited by all participants in focus groups as the most preferred of mode treatment of MIs in Goma city. Indeed, it has been reported that more than 80.0% of population of African countries relies on TM for the care of various ailments including MIs [32]. WHO has acknowledged the contributions of TM to prevention and management of various ailments in developing countries [33]. In current study, all FGD participants suggested collaboration between CM and TM in future for management of MIs. Also, among common MPs reported by ETHP to treat MIs in Goma city, A. hypogea has been reported with sedative activity affects suggesting its use against MIs. However, little is known on MPs including E. abyssinica, M. parassidiaca, C. gynandra and C. sumatrensis suggesting the exploration of their psychopharmacological activities in further studies. As study limitation: To reduce the complexity of the questionnaire, case vignette based standardized questionnaire which explains cases like schizophrenia, major depressive disorder, epilepsy, and generalized anxiety disorder was not used in data collection. Further studies are needed to access knowledge and perception of Goma city population toward MIs [34-36].
Conclusion
Finding of the study proved poor knowledge and perception of Goma city resident toward MIs. The poor perception of Goma city population was not associated with age, education level, religion and education level that suggested the role of education of sociodemographic categories on MI. Also, the study suggested collaboration between CM and TM for effectiveness of MIs management.
Authors Contributions
SKK, GSB and EK designed the study. SKK and ZTK coordinated data collection. SKK developed the coding framework, undertook data analysis and wrote the manuscript. EK, GSB, JO, NM and NN contributed to the conceptual framework and reviewed the manuscript at several stages. All authors read and approved the final manuscript.
Acknowledgements
I am grateful to Dr. Godfrey Bbosa and Dr. John Odda of the Department of Pharmacology & Therapeutics of Makerere University, College of Health Sciences, Profesor Zacharie Tsongo Kibendelwa of Faculty of Human Medicine, University of Goma, in Goma city/DRC, Dr. Esther Katuura of School of Biological Sciences, College of Natural Sciences of Makerere University, all Doctoral committee members of Makerere University including, Associate Professor Noeline Nakasujja and Dr. Norah Mwebaza, and all Ethical Committee members.
Declarations
Conflicts of Interest
The authors declare no conflicts of interest regarding the publication of this paper.
Ethics Approval/Ethics Standards
This research project was approved by research committee of the Department of Pharmacology and Therapeutics, and the School of Biomedical Sciences Research and Ethics Committee at Makerere University College of Health Sciences with approval protocol number SBS-841. The manuscript does not contain clinical studies or patient data. The study was conducted in accordance with the Helsinki declaration on use of human subjects in research.
Consent to Participate
Informed consent was obtained from all individual participants including in the study.
Availability of Data and Material
Raw data are available as additional supporting files.
Funding
The authors received no financial support for the research, authorship and publication of this article.
References
- GBD 2019 Mental Disorders Collaborators. (2022). Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet Psychiatry, 9(2), 137-150.
- Rockhold, P., & McDonald, L. (2009). The hidden issue in international development aid: health and disability in conflict-affected settings in sub-Saharan Africa. Journal for Disability and International Development, 1, 4-11.
- Daar, A. S., Jacobs, M., Wall, S., Groenewald, J., Eaton, J., Patel, V., ... & Ndetei, D. (2014). Declaration on mental health in Africa: moving to implementation. Global health action, 7(1), 24589.
- Espinoza, S. (2016). Barriers to mental health treatment within the Congolese population.
- Vivalya, B. M., Vagheni, M. M., Gumisiriza, N., Kitoko,G. M. B., Piripiri, A. L., & Kaputu-Kalala-Malu, C. (2020). Implementing of mental health services in an area affected by prolonged war and Ebola disease outbreak: case of North-Kivu province, Democratic Republic of Congo. PAMJ-One Health, 1(8).
- Dossa, N. I., Hatem, M., Zunzunegui, M. V., & Fraser, W.(2014). Social consequences of conflict-related rape: Thecase of survivors in the Eastern Democratic Republic of Congo. Peace and Conflict: Journal of Peace Psychology, 20(3), 241.
- On'okoko, M. O., Jenkins, R., Miezi, S. M. M., Andjafono,D. O. L. E., & Mushidi, I. M. (2010). Mental health in the Democratic Republic of Congo: a post-crisis country challenge. International Psychiatry, 7(2), 41-43.
- Kyolo, S. K., Bbosa, G. S., Odda, J., Mwebaza, N., Kibendelwa, Z. T., Nakasujja, N., & Katuura, E. (2023). Indigenous knowledge and perception toward mental illnesses within Goma city in Democratic Republic of Congo.
- Bartlett, P., Jenkins, R., & Kiima, D. (2011). Mental health law in the community: thinking about Africa. International journal of mental health systems, 5(1), 1-7.
- Piwowarczyk, L., Bishop, H., Yusuf, A., Mudymba, F., & Raj, A. (2014). Congolese and Somali beliefs about mental health services. The Journal of nervous and mental disease, 202(3), 209-216.
- Canada: Immigration and Refugee Board of Canada (IRBC),R. D.C. (2012, June. 14). République Démocratique du Congo (RDC), information sur le traitement réservé aux personnes ayant des troubles de santé mentale. (IRBC, Éd.) Consulté le 2022.
- Eaton, J., Des Roches, B., Nwaubani, K., & Winters, L. (2015). Mental health care for vulnerable people with complex needs in low-income countries: two services in West Africa. Psychiatric Services, 66(10), 1015-1017.
- Njenga, F. (2007). The concept of mental disorder: an African perspective. World Psychiatry, 6(3), 166.
- Michellier, C., Kervyn, M., Barette, F., Syavulisembo, A. M., Kimanuka, C., Mataboro, S. K., ... & Kervyn, F. (2020). Evaluating population vulnerability to volcanic risk in a data scarcity context: The case of Goma city, Virunga volcanic province (DRCongo). International journal of disaster risk reduction, 45, 101460.
- INS-Nord-Kivu. ( 2016). Goma et ses avenues. Division Provincial du Plan, Goma.
- Namegabe, EPDNN (2008). Factors influencing the choice of care at the household level in the city of Goma (DRC) Cases of 369 households living in FSDC/ULPGL partnership sites.
- Kumar, R. V. (2013). Respondent selection methods in household surveys. Jharkhand Journal of Development and Management Studies, Forthcoming.
- Benti, M., Ebrahim, J., Awoke, T., Yohannis, Z., & Bedaso, A. (2016). Community perception towards mental illness among residents of Gimbi town, Western Ethiopia. Psychiatry journal, 2016.
- Wang, J., He, Y., Jiang, Q., Cai, J., Wang, W., Zeng, Q., ... & Zhang, M. (2013). Mental health literacy among residents in Shanghai. Shanghai archives of psychiatry, 25(4), 224.
- Reavley, N. J., & Jorm, A. F. (2011). Recognition of mental disorders and beliefs about treatment and outcome: findings from an Australian national survey of mental health literacy and stigma. Australian & New Zealand Journal of Psychiatry, 45(11), 947-956.
- Amuyunzu-Nyamongo, M. (2013). The social and cultural aspects of mental health in African societies. Commonwealth health partnerships, 2013, 59-63.
- Ventevogel, P., Jordans, M., Reis, R., & de Jong, J. (2013). Madness or sadness? Local concepts of mental illness in four conflict-affected African communities. Conflict and health, 7(1), 1-16.
- Laudati, A. A. (2016). Securing (in) security: relinking violence and the trade in cannabis sativa in eastern Democratic Republic of Congo. Review of African Political Economy, 43(148), 190-205.
- Sadik, S., Bradley, M., Al-Hasoon, S., & Jenkins, R. (2010). Public perception of mental health in Iraq. International journal of mental health systems, 4(1), 1-11.
- Salve, H., Goswami, K., Sagar, R., Nongkynrih, B., & Sreenivas, V. (2013). Perception and attitude towards mental illness in an urban community in South Delhi-A community based study. Indian journal of psychological medicine, 35(2), 154-158.
- Deribew, A., & Tamirat, Y. S. (2005). How are mental health problems perceivedby a community in Agaro town?. Ethiopian Journal of Health Development, 19(2), 153-159.
- Adewuya, A. O., & Makanjuola, R. O. (2008). Lay beliefs regarding causes of mental illness in Nigeria: pattern and correlates. Social psychiatry and psychiatric epidemiology, 43, 336-341.
- Papaleontiou-Louca, E. (2021). Effects of religion and faith on mental health. New ideas in psychology, 60, 100833.
- Roehr, B. (2013). American psychiatric association explains DSM-5. Bmj, 346.
- World Health Organization. (2017). Depression and other common mental disorders: global health estimates (No. WHO/MSD/MER/2017.2). World Health Organization.
- Tepper, L., Rogers, S. A., Coleman, E. M., & Malony, H. N. (2001). The prevalence of religious coping among persons with persistent mental illness. Psychiatric services, 52(5), 660-665.
- Abbo, C., Odokonyero, R., & Ovuga, E. (2019). A narrative analysis of the link between modern medicine and traditional medicine in Africa: a case of mental health in Uganda. Brain research bulletin, 145, 109-116.
- Abdullahi, A. A. (2011). Trends and challenges of traditional medicine in Africa. African journal of traditional, complementary and alternative medicines, 8(5S).
- Adane, M., Mengistie, B., Kloos, H., Medhin, G., & Mulat,W. (2017). Sanitation facilities, hygienic conditions, and prevalence of acute diarrhea among under-five children in slums of Addis Ababa, Ethiopia: Baseline survey of a longitudinal study. PloS one, 12(8), e0182783.
- (RDC) Cas de 369 Ménages vivant dans les sites de partenariat de la FSDC/ULPGL. https://hal-auf.archives- ouvertes.fr/hal-00871877
- Singh, A. S., & Masuku, M. B. (2014). Sampling techniques & determination of sample size in applied statistics research: An overview. International Journal of economics, commerce and management, 2(11), 1-22.