


Research Article - (2024) Volume 8, Issue 1
Incidence Trends and Risk Factors of Alcohol-Specific Deaths
Received Date: Feb 27, 2024 / Accepted Date: Mar 18, 2024 / Published Date: Mar 25, 2024
Copyright: ©Â©2024 Kari Poikolainen. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original authors and source are credited.
Citation: Poikolainen, K. (2024). Incidence Trends and Risk Factors of Alcohol-Specific Deaths. J Addict Res, 8(1), 01-04.
Abstract
A simple but questionable view holds that alcohol-related mortality is directly and closely related to the total consumption of alcohol in a country. To study how uniform this relationship is, trends and changes by age and diagnosis in alcohol-specific deaths were studied in Finland between the years 2007-2022, a period when both alcohol consumption and alcohol-specific mortality showed a decreasing trend. Alcoholic liver disease mortality trends deviated markedly from those for the other diagnoses. Among those aged 64 years or less, there was a consistent decreasing trend for the other categories while liver disease showed a slight increase after the initial decrease. Among the population aged 65 years or more both liver disease and other groups showed an increasing trend. Alcohol poisoning decreased in both age groups. Mortality in all other diagnostic groups decreased in the younger age group and increased in the older group. Age-adjustment or gender did not explain differences. The different mortality trends were not consistent with the assumed uniform effect of alcohol consumption on alcohol-related harms. Other risk factors than alcohol may play a significant role. These are discussed and need to be considered to yield better estimates than the simplistic assumption of a 100 % attributable fraction of alcohol in these diagnoses.
Keywords
Alcohol-Specific Mortality, Liver Disease, Alcohol Poisoning, Cardiomyopathy, Mental Disorders
Introduction
Alcohol-specific deaths are a group of etiologic diagnoses, that is, alcohol is mentioned in the disease name as a causal agent. A common view is that the total consumption of alcohol in a country determines how much harm is caused by drinking alcoholic bever¬ages. If the above total consumption model is true, alcohol-related harms should move in concert with alcohol consumption over cal¬endar time. This should be most evident for alcohol-specific deaths since these deaths are considered to be 100 % caused by alcohol [1]. All deaths in the categories comprising alcohol-specific diag¬noses should follow a similar trend. The present analysis shows that this was not the case even if the overall trends in both total al¬cohol consumption and alcohol-specific mortality suggest the op¬posite in Finland, where alcohol consumption decreased steadily from 12 to 9 liters of 100% alcohol per capita and alcohol-specific mortality from 40 to 30 deaths per 100 000 of the population be¬tween the years 2007-2022.
Methodology
Alcohol-specific deaths were studied in Finland between the years 2007-2022. The above period was chosen since the trends of both alcohol consumption and alcohol-specific mortality started to de¬crease, after reaching a peak in the year 2007. Data were derived from the StatFin database kept by Statistics Finland (https://pxda-ta.stat.fi/PxWeb/pxweb/en/StatFin/). The three-digit ICD-10 codes were F10, G312, G4051, G6 21, G721, I426, K292, K70, K860, K852, 0354, P043, Q860 and X45. These are underlying causes of deaths, that is the disease or injury initiating the train of morbid events. Contributory causes of death were not included, because their causal role is unknown. The European standard population (ESP2012) was applied for age adjustment. Both age-adjusted and crude mortality showed a closely correlated decreasing trend, Be¬cause adjustment did not make any notable difference, the actu¬al mortality rates for both genders combined will be presented. The proportion of male deaths was predominant (77 %) and male mortality was closely correlated with the respective female rates (r=0.87).
Results
Alcoholic liver disease was the largest group and its mortality trends deviated from the other diagnoses. Among those aged 64 years or less, there was a consistent decreasing trend for the other categories while liver disease showed a slight increase after the initial decrease (Figure 1). Among the population aged 65 years or more both liver disease and other groups showed an increasing trend (Figure 2). Alcohol poisoning was the next largest group, decreasing among both age groups. Mortality in other diagnostic groups decreased in the younger age group and increased in the older group (Table).
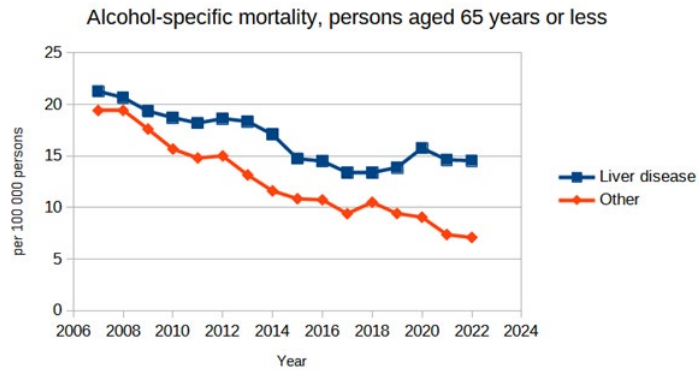
Figure 1: Alcohol-Specific Mortality, per 100,000 Persons Aged 65 Years or Less, in 2007-2022 in Finland
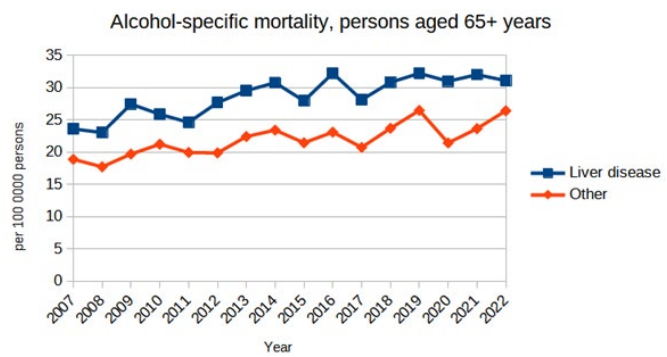
Figure 2: Alcohol-Specific Mortality, per 100,000 Persons Aged 64 Years or more, in 2007-2022 in Finland
|
|
Liver disease (K70) |
Alcohol poisoning (X45) |
Mental disorders (F10) |
Cardiomyo-pathy (I426) |
Other |
Total |
|
Under 65 years of age |
|
|
|
|
|
|
|
No. of deaths 2007 |
948 |
503 |
106 |
96 |
143 |
1796 |
|
Change % 2007 to 2022 |
-34.4 |
-80.3 |
-36.7 |
-57.3 |
-32.9 |
-48.6 |
|
65 years of age or older |
|
|
|
|
|
|
|
No. of deaths 2007 |
197 |
68 |
43 |
23 |
40 |
371 |
|
Change % 2007 to 2022 |
+103.5 |
-55.9 |
+320.9 |
+47.8 |
+137.5 |
+98.4 |
Table: Number of Alcohol-Specific Deaths (ICD-10 Codes) in 2007 and Percent Change from 2007 to 2022 by Age Group
Discussion
The alcohol-specific mortality trends were different for the liver disease group and the rest, as well as for the two age groups, those less than 65 years and those 65 years or older. Alcohol-specific deaths are a category of etiologic diagnoses, that is, alcohol is mentioned in the disease name as a causal agent. Therefore, al¬cohol is assumed to be a necessary cause. Not a sufficient cause, since death is caused by many factors. Alcohol may, or may not, be the decisive factor. The accuracy in ascertaining these deaths depends on the judgment of the cause-of-death determination and is often unknown. Attributions to alcohol may be under or over-es-timated. Each revision of the ICD has provided more diagnoses with alcohol etiology which may have increased the number of alcohol-specific deaths.Other risk factors than alcohol may be re¬lated to alcohol-specific deaths. These have been earlier studied in toto (deaths and hospitalizations of all diagnoses). In addition to alcohol intake, smoking and marital status were found to increase the risk of occurrence [2]. However, focusing on the risk factors of separate diagnostic entities is likely to be a more elaborate strate¬gy, but remains underutilized.
Risk factors for liver disease may include hepatitis infections, smoking, obesity, proton-pump inhibitor medication to decrease stomach acidity, malnutrition, some environmental poisons, like aflatoxin, and perhaps genetic factors [3,4]. C-type lectin (min-cle) may contribute to inflammation and fibrosis once the intesti-nal barrier becomes leaky in the advanced stages of chronic liver disease [5]. Notably, in a large series of biopsy-confirmed alco-holic liver disease patients, the presence of excess weight for at least 10 years was a risk factor for cirrhosis, alcoholic hepatitis, and steatosis and consumption of 20 cigarettes/day has been found to relate to 4-fold risk increase among women in England [6,7]. Coffee consumption has decreased the risk of cirrhosis [8,9]. Fa¬tal alcohol poisoning is alcohol-induced, but adequate evidence is often unavailable. The average lethal blood alcohol concentration is about 0.5 % but variation depends on innate and acquired tol¬erance. The blood alcohol level may decrease from the maximum concentration to the postmortal level for many hours between the onset of drinking and the moment of death. The time from the peak to the moment of death is seldom known [10,11]. Psychoactive drugs and conditions inducing inhalation of vomit complicate the ascertainment. Therefore, determining the underlying cause of death must often be based on a probability estimate after ruling out other possible causes.
The group alcohol-related disorders in the mental, behavioral, and neurodevelopmental disorders (ICD-10 chapter F10) is heteroge¬neous. It includes alcohol-related intoxication, abuse, dependence, withdrawal, dementia, psychotic disorder, and several alcohol-in-duced mental disorders, such as anxiety and depression, among others. Alcohol dependence may be the pivotal disorder that leads to several others. Risk factors and developmental causal paths for alcohol dependence are many and varied [12]. Major possible risk factors, either externalizing or internalizing mental problems, have been found in about 50 % of a large Swedish representative sample [13]. Cardiomyopathies comprise a heterogeneous group of diseases, often of genetic origin or caused by several heart and circulatory conditions (acquired cardiomyopathy). The main types are hypertrophic, dilated, and arrhythmia-induced cardiomyop¬athies [14]. In Finland, approximately one-third of hypertrophic cardiomyopathy is explained by the four most common genetic variants [15].
The role of alcohol as a causal agent is difficult to ascertain be¬cause both self-reports and reports from significant others are inaccurate, usually underestimate alcohol intake (but sometimes overestimate it) and variations in inaccuracy may be great [16-18]. Therefore, the under-representation of alcohol-specific deaths among deaths is sometimes suspected. In the present series, this does not seem likely since the proportion of alcohol-specific liver disease deaths (ICD-10 code K70) was as much as 86 % of all liver disease deaths (K70–K76). Other possible explanations for these observations exist. The age-group differences suggest that younger birth cohorts may drink less, have healthier drinking patterns, or have fewer other risk factors. Unfortunately, the present data are too sparse for further study of this possibility. Cause-of-death di¬agnostics could differ, but it is not likely because no major changes in the organization and personnel of cause-of-death examination have been observed during this short observation period. The asso¬ciation between alcohol-specific deaths is commonly thought to be linear, causal, and strong. Consequently, decreasing the total con¬sumption is assumed to decrease harm. Decreasing consumption by tax hikes and limitation of supply of the beverages is thought to be strong and is marketed as a ”best buy”, by WHO and several other organizations [19]. This appealing and simple view seems to be false because of contrary scientific evidence [20]. The present findings support the latter view, suggesting that other risk factors are important.
Conclusion
While ”alcohol-specific” subcategories of disease and injury en-tities may be useful for basic cause-of-death statistics, differences in the present study call for studies on the other risk factors than alcohol in these subgroups. These should be considered if we want better estimates than the crude assumption of a 100 % attributable fraction of alcohol on the role of alcohol in these diagnoses. Diag¬nostic entities should not be split into alcohol-related and not-re-lated etiologic categories in such studies.
References
- Stockwell, T. (2019). Finnish alcohol policy at the crossroads: the health, safety and economic consequences of alternative systems to manage the retail sale of alcohol. Centre for Addictions Research of BC, University of Victoria.
- Poikolainen, K., Paljärvi, T., & Mäkelä, P. (2011). Risk factors for alcohol-specific hospitalizations and deaths: prospective cohort study. Alcohol and Alcoholism, 46(3), 342-348.
- Hart, C. L., Morrison, D. S., Batty, G. D., Mitchell, R. J., & Smith, G. D. (2010). Effect of body mass index and alcohol consumption on liver disease: analysis of data from two prospective cohort studies. BMJ, 340.
- Wang, J., Wu, Y., Bi, Q., Zheng, X., Zhang, J., & Huang,W. (2020). Adverse outcomes of proton pump inhibitors in chronic liver disease: a systematic review and meta-analysis. Hepatology International, 14, 385-398.
- Schierwagen, R., Uschner, F. E., Ortiz, C., Torres, S., Brol,M. J., Tyc, O., ... & Klein, S. (2020). The role of macrophage-inducible C-type lectin in different stages of chronic liver disease. Frontiers in Immunology, 11, 507261.
- Naveau, S., Giraud, V., Borotto, E., Aubert, A., Capron, F., & Chaput, J. (1997). Excess weight risk factor for alcoholic liver disease. Hepatology, 25(1), 108-111.
- Liu, B., Balkwill, A., Roddam, A., Brown, A., & Beral, V. (2009). Separate and joint effects of alcohol and smoking on the risks of cirrhosis and gallbladder disease in middle-aged women. American Journal of Epidemiology, 169(2), 153-160.
- Klatsky, A. L., & Armstrong, M. A. (1993). Alcoholic beverage choice and risk of coronary artery disease mortality: do red wine drinkers fare best? The American Journal of Cardiology, 71(5), 467-469.
- Corrao, G., Lepore, A. R., Torchio, P., Valenti, M., Galatola, G., D’amicis, A., ... & Provincial Group for the Study of Chronic Liver Disease. (1994). The effect of drinking coffee and smoking cigarettes on the risk of cirrhosis associated with alcohol consumption: a case-control study. European Journal of Epidemiology, 10, 657-664.
- Poikolainen K. (1977). Alcohol poisoning mortality in four Nordic countries. Vol. 28. Forssa: Finnish Foundation for Alcohol Studies.
- Poikolainen, K. (1984). Estimated lethal ethanol concentrations in relation to age, aspiration, and drugs. Alcoholism: Clinical and Experimental Research, 8(2), 223-225.
- Poikolainen K. (2020). Perfect drinking and its enemies. Second, updated and revised edition. Kindle Direct Publishing.
- Kendler, K. S., Ohlsson, H., Sundquist, J., & Sundquist,K. (2022). Risk for mood, anxiety, and psychotic disorders in individuals at high and low genetic liability for bipolar disorder and major depression. JAMA Psychiatry, 79(11), 1102-1109.
- British Heart Association. (2023). Cardiomyopathy. (11 January 2024. date last accessed).
- Jääskeläinen, P., Vangipurapu, J., Raivo, J., Kuulasmaa, T., Heliö, T., Aalto-Setälä, K., ... & Kuusisto, J. (2019). Genetic basis and outcome in a nationwide study of Finnish patients with hypertrophic cardiomyopathy. ESC Heart Failure, 6(2), 436-445.
- Poikolainen, K., & Kärkkäinen, P. (1983). Diary gives more accurate information about alcohol consumption than questionnaire. Drug and Alcohol Dependence, 11(2), 209-216.
- Alanko, T. (1984). An overview of techniques and problems in the measurement of alcohol consumption. Research Advances in Alcohol and Drug Problems, 209-226.
- Knibbe, R. A., & Bloomfield, K. (2001). Alcohol consumption estimates in surveys in Europe: comparability and sensitivity for gender differences. Substance Abuse, 22(1), 23-38.
- WHO. (2023). More ways, to save more lives, for less money: World Health Assembly adopts more Best Buys to tackle noncommunicable diseases. (7 January 2024. date last accessed).
- Snowdon, C. (2022). Testing the total consumption model of alcohol. Economic Affairs, 42(3), 442-452.