



Research Article - (2023) Volume 8, Issue 3
In Situ Saphenous Vein Bypass Grafting in Peripheral Arterial Disease of the Lower Extremities
Received Date: Oct 30, 2023 / Accepted Date: Nov 21, 2023 / Published Date: Nov 27, 2023
Copyright: ©Ã?©2023 Rasit Dinc. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Dinc, R. (2023). In Situ Saphenous Vein Bypass Grafting in Peripheral Arterial Disease of the Lower Extremities. Cardio Open, 8(3), 73-77.
Abstract
Objective: To evaluate the efficacy and safety of the valvulotome device used to cut venous valves and in situ bypass in the treatment of peripheral arterial disease (PAD) of the lower extremities.
Methods: In this study, the basic principles of in situ saphenous vein bypass are mentioned, specifically for a novel valvulotome device (NODR Valvulotome device, Invamed/ Ankara/Turkey). In this context, the effectiveness of the method was evaluated by interpreting the results of some studies on in situ saphenous vein bypass.
Results: In situ bypass has an effective rate for long-term outcomes with approximately 80%, 90% and 95% for primary patency (no evidence of restenosis with a maximum systolic rate >2.5 or sonography-based occlusion), secondary patency (patency maintained by repeated intervention after complete bypass occlusion), and limb salvage (absence of major amputations), respectively. The side effects, including vessel perforation and intramural bleeding, are very low. The technical success rate is very high. Valvulotomes are easy to use by the surgeons and provide comfort for the patients.
Conclusions: In situ bypass is effective and safe in PAD treatment. Valvulotome provides ease of use for surgeons and comfort for patients.
Keywords
Peripheral Artery Disease (PAD), Valvulotomy, In Situ Vein Bypass, Great Saphenous Vein, NODâ?? Valvulotome
Introduction
Lower extremity peripheral artery disease (LE-PAD) is a cir- culation problem of the lower extremities that is progressive in nature [1]. This disease is a high burden on the public health system due to the increased risk of major cardiovascular events, high rates of morbidity, and an important cause of poor quality of life [2]. Atherosclerosis is the major cause of peripheral ar- terial disease (PAD). It most commonly affects the arteries that supply blood to the legs and feet. Although the clinical manifes- tation of PAD is generally benign, it can progress to life-threat- ening critical limb ischemia (CLI), which requires revascular- ization intervention [3]. Revascularization is achieved by open surgical techniques such as bypass grafting or endarterectomy, or by endovascular methods such as stenting or angioplasty [4]. Endovascular methods are preferred to surgical techniques due to their minimally invasive properties. However, they are most effective for more localized occlusions in larger arteries. Open surgical techniques are considered when the blockage is too se- vere or endovascular methods are not feasible due to the lesion site [5]. Leg veins are commonly used for bypass grafting in PAD. However, the leg veins have multiple valves that direct blood flow to the heart, in the opposite direction of the arteri- al system. Therefore, they cannot be used directly as grafts. To overcome this challenge, reversed vein bypass or in situ bypass methods are used (Figure 1, A and B) [6,7].
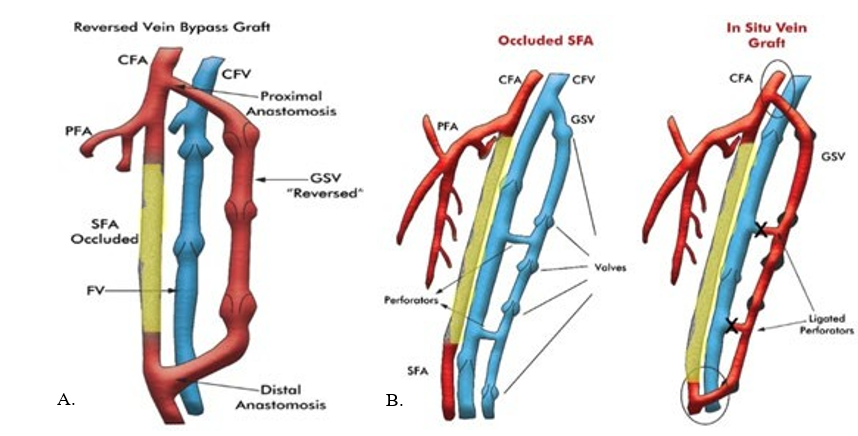
Figure 1A: Reversed Vein Bypass
Figure 1B: In Situ Vein Bypass Graft [8].
This review article focuses on the in-situ bypass treatment of PAD in the lower extremities, with a brief emphasis on other revascularization strategies.
Methods
In this study, the basic principles of in situ saphenous vein by- pass are mentioned in order to bring the reader's attention, spe- cifically to the ![]() Valvulotome device, developed Invamed (Ankara, Turkey). In this context, the effectiveness of the meth- od was evaluated by interpreting the results of some studies on in situ saphenous vein bypass.
Valvulotome device, developed Invamed (Ankara, Turkey). In this context, the effectiveness of the meth- od was evaluated by interpreting the results of some studies on in situ saphenous vein bypass.
Basic Principle of In Situ Veinous Bypass and Valvulo- tomy
In situ vein bypass is to anastomose a vein to an adjacent artery by keeping it in its original vascular bed. Only the proximal and distal ends are mobilized in this technique. The other length of the vein used for bypass is left in its original anatomical position [8]. This appears to provide a higher patency and a higher rate of vein utilization. However, this procedure has special technical challenges. For this reason, valve leaflets are cut separately to allow blood to flow downward valvulotomes. Valvulotomes are catheter-based surgical devices that are used to cut and disable venous valves. This provides a solution to direct blood flow in the grafted vein segment in the same direction as the artery [9]. The tributaries and perforators of the vein are also ligated by valvulotomes. The large and small end of the vein anastomosed to the large and small end of the artery, respectively (Figure 1B) [8].
Technical Considerations for ![]() Valvulotome
Valvulotome
The![]() Valvulotome (Figure 2) allows an easy endovascular incision of the venous valves. The hydrophilic coating facilitates the intravenous insertion with minimal risk of intimal damage. It uses a long flexible catheter with a recessed cutting blade at the tip to destroy venous valves. It is well-positioned because of the unique self-sizing nitinol wire and self-centering pulley. In addition to these, it provides optimum valve cutting thanks to the four blades on-the-wire (OTW).
Valvulotome (Figure 2) allows an easy endovascular incision of the venous valves. The hydrophilic coating facilitates the intravenous insertion with minimal risk of intimal damage. It uses a long flexible catheter with a recessed cutting blade at the tip to destroy venous valves. It is well-positioned because of the unique self-sizing nitinol wire and self-centering pulley. In addition to these, it provides optimum valve cutting thanks to the four blades on-the-wire (OTW).
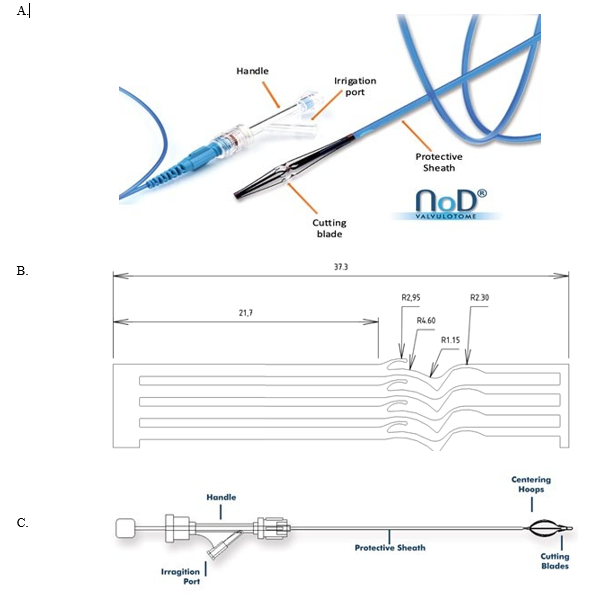
Figure 2A: Fundamental parts of ![]() Valvulotome
Valvulotome
Figure 2B: Four cutting OTW* blades, enabling effective valve cutting,
Figure 2C: Schematic demonstration of common parts of![]() and LeMaitre Valvulotome devices.
and LeMaitre Valvulotome devices.
*OTW: on-the-wire
Procedural Step
To destroy the valves of the vein, the valvulotome is inserted into the vein at its distal end with the catheter guide and then guided to the proximal end. After the blades are placed above the valve, the valvulotome opens and the valves are destroyed by the retracting motion of the blades. Then the valvulotome blades are closed and the device is taken out of the saphenous vein.
Results
According to reports from studies on valvulotomes, the esti- mated rates of long-term outcomes rates (> six months) of the studies used in situ bypass are approximately 80%, 90% and 95% for primary patency (no evidence of restenosis with a peak systolic rate >2.5 or occlusion based on sonography), second- ary patency (patency maintained by repeated intervention after complete bypass occlusion), and limb salvage (absence of major amputations), respectively [9-11]. In addition to the technolog- ical characteristics that make the valvulotomes easy to use and provide comfort, the technical success and the arterial-veinous end anastomosis rate are very high. Side effects, including vessel perforation and intramural bleeding, are very low.
Discussion
Delaying revascularization for PAD causes serious clinical con- ditions, including ischemia, gangrene, and can require leg am- putation [4,12]. Both the severity of the disease and the anatom- ical location of the PAD strongly influence the revascularization strategy [13]. Optimal management is determined by a multi-disciplinary team evaluation [4,12]. Especially during the treat- ment of long segment occlusions or heavily calcified arteries, endovascular treatment methods can cause some complications such as arterial rupture, arterial dissection, distal embolization, and access site injuries [14]. Due to such adverse events and the infeasibility for some lesions, peripheral bypass surgery still plays an important role in endovascular age [15]. On the other hand, early complications, such as postoperative cardiovascular events, wound complications, and late complications, such as anastomotic aneurysms, graft infections, and abdominal adhe- sions, are sometimes encountered in open surgical interventions [13,16].
An alternative strategy is to use leg veins with dysfunctional valves. The reverse vein bypass approach is one of the methods to disable the valves. In this method, the length of the saphenous vein surgically removed from the leg is reversed and implanted as a bypass by ligating and cutting its perforators and tributaries. However, the valves are not excised (Figure 1A) [8]. Of the al- ternative strategies, another approach is the in-situ bypass meth- od, which commonly uses valvulotomes [9]. Some commercial valvulotomes are available for the in-situ bypass. The ![]() Valvulotome is technologically and operationally similar to the LeMaitre Valvulotome (LeMaitre Vascular, Burlington, MA, USA), another commercial valvulotome device. Their self-siz- ing and self-centering close to the targeted valve provide ease of use for surgeons, high safety, and comfort for patients. During the intervention, damage to the vein intima is minimal due to the special design of the blade, and the valve leaves are cut traumat- ically without tearing. The devices contain a hydrophilic coat- ing on the protective sheath to improve push ability by reducing friction.
Valvulotome is technologically and operationally similar to the LeMaitre Valvulotome (LeMaitre Vascular, Burlington, MA, USA), another commercial valvulotome device. Their self-siz- ing and self-centering close to the targeted valve provide ease of use for surgeons, high safety, and comfort for patients. During the intervention, damage to the vein intima is minimal due to the special design of the blade, and the valve leaves are cut traumat- ically without tearing. The devices contain a hydrophilic coat- ing on the protective sheath to improve push ability by reducing friction.
Various studies have demonstrated in situ bypass, meanwhile the valvulotome, is effective for patency and limb salvage. In the LIMBSAVE registry, a multicenter study using the LeMaitre Valvulotome, primary patency, secondary patency, and limb sal- vage were reported to be 78.1%, 92.1%, and 94.7%, respective- ly, at six-month follow-up. The study also reported the method was safe and technically successful [9]. Bergmark et al also re- ported a significantly higher patency (84%) after six months for the in-situ technique [10].
In a meta-analysis study, Guo et al found that the long-term pa- tency of in situ bypass grafting was similar to reverse grafting [17]. In situ bypass grafting has even been reported to be su- perior for some subgroups, such as femoropopliteal bypass. In another study by Shah et al, the 30-day patency rate was 96%, while the cumulative secondary patency was 91% and 81% at 1 and 5, respectively [11]. Limb salvage rates using in situ bypass were 97% and 95% at 1 and 5 years, respectively. The in situ technique has several advantages over the reverse technique: for example, reduction in the number of interruptions (lower risk of dehiscence/infection at the surgical site); less manipulation of lymphatic structures (lower risk of postoperative lymphedema); lower risk of saphenous nerve damage (lower risk of postoper- ative dysesthesia); shorter intervention time; less manipulation of the great saphenous vein (lower risk of stenosis during fol-low-up); and better anastomotic congruence (better circulatory dynamics), shorer hospital stay (decreased rate of major wound infection) and faster patient recovery [9,17].
Conclusion
Revascularization plays an important role in PAD therapy. De- lay in revascularization may be associated with serious clini- cal conditions. The revascularization method is determined by a multidisciplinary team evaluation. To use valvulotome for in situ bypass is effective and safe. It also provides ease of use for surgeons and comfort for patients.
Declaration of Conflicting Interests
Rasit Dinc is the president of INVAMED Company (Ankara, Turkey).
Ethics Approval Statement
This manuscript, which is a review article, does not include stud- ies with human or animal participants.
Authors Contribution
Rasit Dinc designed, conceptualized, searched for data, wrote and finalized.
References
- Djerf, H., Svensson, M., Nordanstig, J., Gottsäter, A., Falkenberg, M., & Lindgren, H. (2021). Editor's Choice– Cost effectiveness of primary stenting in the superficial femoral artery for intermittent claudication: two year results of a randomised multicentre trial. European Journal of Vas- cular and Endovascular Surgery, 62(4), 576-582.
- Members, W. C., Gerhard-Herman, M. D., Gornik, H. L., Barrett, C., Barshes, N. R., Corriere, M. A., ... & Wijeysun- dera, D. N. (2017). 2016 AHA/ACC guideline on the man- agement of patients with lower extremity peripheral artery disease: Executive summary. Vascular medicine (London, England), 22(3), NP1-NP43.
- Conte, M. S., Bradbury, A. W., Kolh, P., White, J. V.,Dick, F., Fitridge, R., ... & for the Joint, G. W. G. (2019). Global vascular guidelines on the management of chronic limb-threatening ischemia. European Journal of Vascular and Endovascular Surgery, 58(1), S1-S109.
- Albayati, M. A., & Shearman, C. P. (2013). Peripheral arte- rial disease and bypass surgery in the diabetic lower limb. Medical Clinics, 97(5), 821-834.
- Tran, B. (2021). Assessment and management of periph- eral arterial disease: what every cardiologist should know. Heart, 107(22), 1835-1843.
- Donaldson, M. C., Mannick, J. A., & Whittemore, A. D. (1991). Femoral-distal bypass with in situ greater saphe- nous vein. Long-term results using the Mills valvulotome. Annals of surgery, 213(5), 457.
- Dardik, H., Vazquez, R., Silvestri, F., Ibrahim, I. M., Suss- man, B., Kahn, M., & Wolodiger, F. (1995). Experience with a new valvulotome for lower-extremity revasculariza- tion procedures by the in situ method. Cardiovascular Sur- gery, 3(2), 193-197.
- Schwarz, W., Nozick, J., Richmand, D., Rodgers, B., Simp-son, A., Argila, C., & Honickman, S. (1986). The in situ saphenous vein bypass graft: radiologic aspects. American journal of roentgenology, 146(3), 605-608.
- Troisi, N., Blasis, G. D., Salvini, M., Michelagnoli, S., Se- tacci, C., & LIMBSAVE Registry Collaborative Group. (2021). Preliminary six-month outcomes of LIMBSAVE (treatment of critical Limb IscheMia with infragenicular Bypass adopting in situ SAphenous VEin technique) regis- try. Vascular, 29(4), 589-596.
- Bergmark, C., Johansson, G., Olofsson, P., & Swedenborg,J. (1991). Femoro-popliteal and femoro-distal bypass: a comparison between in situ and reversed technique. The Journal of Cardiovascular Surgery, 32(1), 117-120.
- Shah, D. M., Darling 3rd, R. C., Chang, B. B., Fitzgerald,K. M., Paty, P. S., & Leather, R. P. (1995). Long-term results of in situ saphenous vein bypass. Analysis of 2058 cases. Annals of surgery, 222(4), 438.
- Reinert, M., & Kupczyk, P. (2023). Akuter peripherer Ge- fäßverschluss. Die Radiologie, 63(1), 3-10.
- Hiramoto, J. S., Teraa, M., de Borst, G. J., & Conte, M. S. (2018). Interventions for lower extremity peripheral artery disease. Nature Reviews Cardiology, 15(6), 332-350.
- Nordanstig, J., Behrendt, C. A., Bradbury, A. W., de Borst,G. J., Fowkes, F. G. R., Golledge, J., ... & Norgren, L. (2023). Peripheral arterial disease (PAD)–A challenging manifesta- tion of atherosclerosis. Preventive Medicine, 107489.
- Ram, N. (2023). Peripheral arterial disease (PAD) in diabet- ics: diagnosis and management-a narrative review. JPMA. The Journal of the Pakistan Medical Association, 73(3), 621-626.
- Topfer, L. A., & Spry, C. (2016). New technologies for the treatment of peripheral artery disease. 2018 Apr 1. CADTH Issues in Emerging Health Technologies. Ottawa (ON): Ca- nadian Agency for Drugs and Technologies in Health, 172.
- Guo, Q., Huang, B., & Zhao, J. (2021). Systematic review and meta-analysis of saphenous vein harvesting and graft- ing for lower extremity arterial bypass. Journal of Vascular Surgery, 73(3), 1075-1086.