



Research Article - (2021) Volume 6, Issue 1
Improved Patient Outcomes by Normalizing Sympathovagal Balance: Midodrine and Parasympathetic and Sympathetic Monitoring
2Murray Waitzer Endowed Chair for Diabetes Research, Professor of Medicine/Pathology/Neurobiology, Director of Research & Neuroendocrine Unit, Eastern Virginia Medical School, The Strelitz Diabetes Center, 855 W. Brambleton Ave, Rm 2018, Norfolk, VA, USA
3Neuro cardiology Research Corporation, LLC, Wilmington, DE, USA
4Sr Medical Director and CTO, Physio PS, Inc, USA
5Parasympathetic & Sympathetic Nervous System Consultant, Franklin Cardiovascular Associates, PA and Autonomic Dysfunction and POTS Center; Neuro cardiology Research Corporation, LLC, Wilmington, DE, CTO and Sr. Medical Director, Physio PS, Inc., Atlanta, GA, USA
Received Date: Jan 20, 2021 / Accepted Date: Feb 02, 2021 / Published Date: Mar 10, 2021
Copyright: ©Joseph Colombo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Nicholas L DePace, Aaron I Vinik, Cesar R Acosta, Jeysel M Pinales, Michael Yayac, Joseph Colombo (2021) Improved Patient Outcomes by Normalizing Sympathovagal Balance: Midodrine and Parasympathetic and Sympathetic Monitoring. Cardio Open, 6(1): 103-110.
Abstract
A function of the Parasympathetic and Sympathetic (P&S) nervous systems is to maintain proper tissue perfusion, including of the heart and brain upon head-up postural change standing. Orthostatic dysfunction (OD) is associated with pooling of blood in the lower extremities, insufficient vascular support of the heart, and poor brain perfusion. Abnormal P&S responses to standing help to guide therapy for the individual patient. Midodrine is often the primary recommendation to correct P&S dysfunction upon standing. P&S Monitoring (Physio PS, Inc, Atlanta, GA) differentiates OD-subtypes in 2727 cardiology patients, serially tested. P&S Monitoring non-invasively, independently, and simultaneously measures P&S activity, including the normal P-decrease followed by an S-increase with head-up postural change (standing). S-Withdrawal (SW) and P-Excess (PE) are two types of autonomic dysfunction that are associated with OD. SW differentiates OD from Syncope (an S- excess with stand, e.g. Vasovagal Syncope). PE often masks SW by inflating the S-response to stand. OD based solely on BP and HR responses to provocation remains difficult to differentiate, especially early in its development and difficult to track upon follow-up. The latter is important to ensure relief of not only the abnormal BP response to stand (e.g. Orthostatic Hypotension) or HR (e.g. Postural Orthostatic Tachycardia Syndrome) but the SW or PE as well. SW underlies the majority of Dysautonomia patients with lightheadedness (whether masked or not, 82.0%, p=0.0061). Midodrine relieves SW and ultimately Lightheadedness and associated symptoms within 9 months (75.4%, p=0.0323). P&S Monitoring provides more information, enabling earlier and more specific diagnosis and therapy for improved patient outcomes. P&S dysfunction upon standing may be most well relieved by very low doses of oral vasoactive medications such as Midodrine (Proamatine), Mestinon (Pyridostigmine), or Northera (Droxidopa). In this study we focus on Midodrine.
Abbreviations
↓PCBP: A decrease in stand (Postural Change) blood pressure
(BP) as compared with rest
CVD: Cardiovascular Disease
LH: Light Headedness
OD: Orthostatic Dysfunction
OH: Orthostatic Hypotension
OHtn: Orthostatic Hypertension
OIS: Orthostatic Intolerance Syndrome
OVVS: Orthostatic Vasovagal Syncope
P&S: Parasympathetic and Sympathetic
PE: Parasympathetic Excess
POTS: Postural Orthostatic Tachycardia Syndrome
SW: Sympathetic Withdrawal
Introduction
Abnormal Parasympathetic and Sympathetic (P&S) responses to head-up postural change (standing) lead to Orthostatic Dysfunc- tion (OD), which may underlie lightheadedness (LH) due to pool- ing of blood in the lower extremities and insufficient perfusion of the heart and brain [1,2]. LH is often the first, and most debilitat- ing, symptom of OD [3-6]. Assessing OD and its various forms with only BP and HR often results in misdiagnoses, late diagno- ses, excess medication, and poor outcomes. Assessing OD with P&S Monitoring provides more information and may improve diagnostic yield, individualize therapy plans, and improve patient outcomes.
Normal P&S responses to standing start with a decrease in Para- sympathetic activity (P-activity) immediately followed by an increase in (alpha-) Sympathetic activity (αS-activity) Figure 1. P&S causes of OD include α-Sympathetic Withdrawal (αSW, Figure 2, typically associated with (pre-clinical) Orthostatic Hy- potension), β-Sympathetic Excess (βSE, Figure 3, typically asso- ciated with (pre-clinical) Syncope), and Parasympathetic Excess (PE, Figure 4, typically associated with (pre-clinical) Vasovagal Syncope) upon standing [7]. PE often masks SW, a condition typ- ically associated with both (pre-clinical) Orthostatic Hypotension and (pre-clinical) Vasovagal Syncope at the same time in the same patient [5].
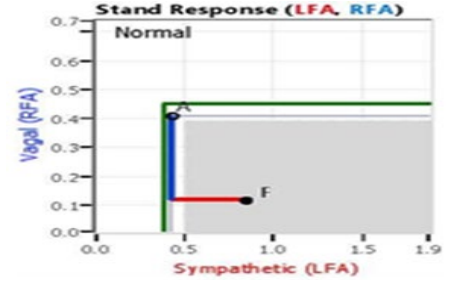
Figure 1: Normal Stand Response. Starting from the resting Baseline state (‘A’), first the Parasympathetics decrease and then the Sympathetics increase ending with the stand state (‘F’).
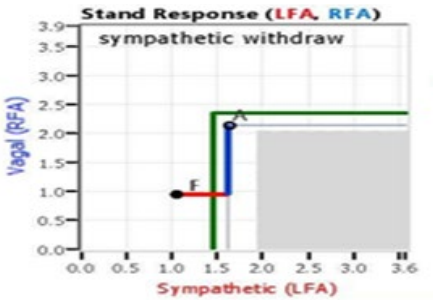
Figure 2: Sympathetic Withdrawal upon Standing. Starting from the resting Baseline state (‘A’), first the Parasympathetics decrease (normally) and then the Sympathetics also decrease (abnormally) ending with the abnormal stand state (‘F’).
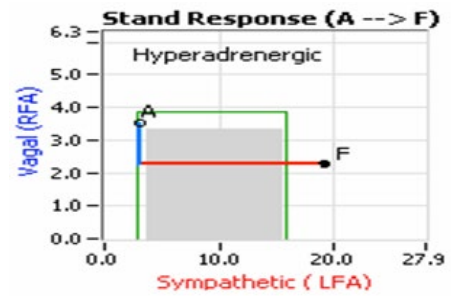
Figure 3: Sympathetic Excess upon Standing (a “Hyperadrener- gic” response). Starting from the resting Baseline state (‘A’), first the Parasympathetics decrease (normally) and then the Sympathet- ics increase excessively ending with the abnormal stand state (‘F’).
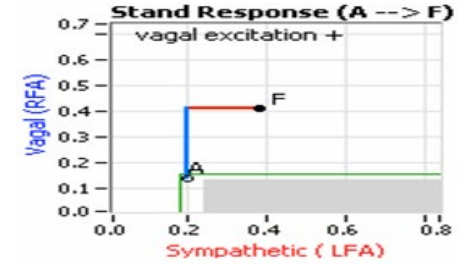
Figure 4: Parasympathetic Excess (PE) upon Standing. Starting from the resting Baseline state (‘A’), first the Parasympathetics in-crease (abnormally) and then the Sympathetics increase (normal- ly) ending with the abnormal stand state (‘F’). PE upon standing may inflate the Sympathetic response, thereby masking Sympa- thetic Withdrawal and as a result Orthostatic Dysfunction.
OD continues to be challenging to differentiate and diagnose (es- pecially early in its development), in part because both autonomic branches should be dynamically changing in a coordinated man- ner. Currently, diagnoses are based on BP and HR responses. Both BP and HR are affected by both P&S branches. Unfortunately, au- tonomic measures are of the whole system and require assumption and approximation to theorize underlying P&S activity, further confounding diagnosis. As a result, positive diagnoses require a sufficient progression of the disorder to satisfy current diagnos- tic assumptions. Detecting and differentiating abnormal P&S re- sponses is more information that may improve differential diag- noses, further specify and individualize treatment, and improve patient outcomes. Midodrine (Proamatine) is an oral vasoactive used as a vasopressor and anti-hypotensive agent. In a large car- diology cohort, low-dose Midodrine was utilized more frequently than standard therapy to relieve OD and reduce LH. This is a ret-rospective study.
Methods
From a database of 3670 consecutive, serial patients, 943 were omitted due to a high burden of ectopy. The remaining patients, 2727 (50.5% Female, average age 57 years, age range 12 to 100 years) were followed with more than one P&S Monitoring assess- ment over four (4) years (an average of 3.3 tests per patient). The mean time between P&S tests is 143 days. Patients average body mass index at baseline is 29.8 #/in2. Patients (Table 1) carry di- agnoses of cardiovascular disease (CVD) or a condition at high risk of future CVD, such as hypertension (32.7%), heart failure (35.2%), history of MI (16.2%), type 2 diabetes (36.2), renal dis- ease (17%), or COPD (8.7%). Patients were on standard therapy and under routine care. Patients demonstrating SW were screened for supine hypertension and high resting BP. If their resting BP was less than 160/90 mmHg, and they did not demonstrate su- pine hypertension, they were prescribed 2.5 mg, Midodrine, qd, titrated to tid slowly. If SW was reversed, the stand BP response normalized, and symptoms relieved, weaning the Midodrine was considered.
Table 1: Cohort description and hemodynamics at baseline testing.
|
Age |
%# |
%F |
BMI |
HR |
sBP |
dBP |
FRF |
EF-a |
EF-l |
EF-h |
FRS |
RRS |
BRR |
|
<20 |
1.6 |
45.5 |
24.8 |
78.5 |
109.9 |
68.1 |
0.19 |
67.0 |
67.0 |
67.0 |
0.0 |
0.0 |
54.5% |
|
20-29 |
4.3 |
52.2 |
26.3 |
76.0 |
114.4 |
72.4 |
0.18 |
62.2 |
55.0 |
74.0 |
0.6 |
0.0 |
46.1% |
|
30-39 |
6.4 |
56.7 |
32.0 |
76.1 |
118.1 |
76.6 |
0.18 |
67.9 |
50.0 |
78.0 |
6.1 |
0.0 |
42.1% |
|
40-49 |
16.4 |
51.6 |
32.2 |
75.3 |
121.2 |
77.8 |
0.19 |
62.7 |
25.0 |
83.0 |
9.0 |
0.0 |
41.6% |
|
50-59 |
25.0 |
47.2 |
31.3 |
72.1 |
125.4 |
77.0 |
0.19 |
60.9 |
20.0 |
85.0 |
15.7 |
3.6 |
43.0% |
|
60-69 |
25.0 |
48.2 |
30.9 |
69.5 |
130.1 |
74.0 |
0.19 |
59.8 |
12.0 |
82.0 |
20.8 |
10.6 |
47.5% |
|
70-79 |
14.3 |
51.3 |
29.3 |
68.3 |
131.3 |
70.2 |
0.20 |
59.6 |
20.0 |
87.0 |
24.8 |
12.2 |
59.8% |
|
80-89 |
6.2 |
59.3 |
27.2 |
66.6 |
139.9 |
68.7 |
0.21 |
60.9 |
21.0 |
84.0 |
27.0 |
29.5 |
67.7% |
|
>89 |
0.7 |
70.0 |
24.5 |
65.7 |
151.1 |
69.4 |
0.19 |
50.5 |
46.0 |
55.0 |
24.8 |
32.1 |
70.0% |
|
Total |
100.0 |
50.5 |
30.5 |
71.6 |
126.6 |
74.5 |
0.19 |
60.8 |
12.0 |
87.0 |
19.4 |
17.6 |
48.3% |
|
% = percent; # = Number; F = Female; BMI = Body Mass Index (#/in2); HR = Heart Rate (bpm); sBP = systolic Blood Pressure (mmHg); dBP = diastolic BP (mmHg); FRF = Fundamental Respiratory Frequency (Hz); EF = Ejection Fraction (%); a = average; l = minimum (low); h = maximum (high); FRS = Framingham Risk Score (%); RRS = Reynolds Risk Score (%); BRR = Baroreceptor Reflex Dysfunction. Total percentages based on entire population. Age range percentages based on individual parameter total. |
|||||||||||||
Patients also demonstrating PE (which often masks SW) were treated with
(1) Coreg, history-dependent if autonomic neuropathy or cardio- vascular disease was diagnosed and no Bradycardia, otherwise
(2) 10 mg Nortriptyline qHS. Patients were also strongly recom- mended proper daily hydration and electrolytes as needed to build volume, and compression stockings to provide immediate relief. If patients were not responsive to Midodrine, then adjunctive or alternative oral vasoactive were prescribed. These patients were omitted from the study.
P&S function was assessed noninvasively using P&S Monitoring from Physio PS, Inc. (Atlanta, GA) software (ANX 3.0 autonomic function monitor). It computes simultaneous independent mea- sures of P&S activity based on continuous, time-frequency anal- ysis of heart rate variability (HRV) with concurrent, continuous time-frequency analysis of respiratory activity (RA) [5]. Clinical data collected include Heart Rate (HR), Blood Pressure (BP), and P&S activity from five minutes seated rest to five minutes of active standing (equivalent to tilt-table testing [8]).
OD is differentiated by BP and HR as Orthostatic Hypotension (OH), Postural Orthostatic Tachycardia Syndrome (POTS), Ortho- static Vasovagal Syncope (OVVS), Orthostatic Intolerance Syn- drome (OIS), and rarely Orthostatic Hypertension (OHtn). PE may be co-morbid and confound diagnoses based on BP or HR alone. Upon head-up posture, these conditions are defined in the follow- ing manner.
1. OH is defined as a BP decrease of more than 20/10 mmHg. SW would confirm OH and help to direct therapy.
2. Pre-clinical OH, with P&S measures, is defined as SW with a BP decrease of more than 5/0 mmHg.
3. POTS is defined as a standing tachycardia of more than 120 bpm or an increase in HR of more than 30 bpm from sitting to standing. SW would confirm POTS and helps to direct ther- apy.
4. Pre-clinical POTS, with P&S measures, is defined as SW with an HR increase of more than 20 bpm.
5. OVVS is defined as PE (which is the Vagal component) with stand SE (which is associated with Syncope). The PE may inflate the S-response to stand, thereby masking SW. PE and SW may be treated simultaneously such as with low dose an- ticholinergics and Midodrine, respectively. Often PE must be treated first to unmask SW.
6. OHtn is defined as a BP increase of more than 30 mmHg sys- tolic. SW would confirm OHtn and help to direct therapy.
7. Pre-clinical OHtn, with P&S measures, is defined as SW with a BP increase of more than 20 mmHg.
8. OIS is a diagnosis by omission with SW and normal BP and HR responses. In clinical cases, SW confirms OD.
Midodrine is known to relieve SW and normalize the α-S-response to postural change [5, 9, 10]. Midodrine hydrochloride was created by Japanese pharmacologist in the mid-1980s. It forms an active metabolite, desglymidodrine, an α1-agonist. Then, it wields its ac- tions via stimulation of the α-adrenergic receptors of the arteriolar and venous vasculature, generating an increase in vascular tone and rise of BP. Therefore, as a vasopressor, it may be beneficial for patients with OD (OH, OVVS, OHtn, or OIS) or syndromes that are attributed to a variety of etiologies such as diabetes, car- diac disease, and autonomic dysfunction. Moreover, Midodrine’s mechanism of action suggests that it ameliorates symptoms related to hypotension, and dysfunction-weakness, syncope, blurred vi- sion, chronic fatigue, and brain fog-without cardiac stimulation, as well as OD. Midodrine comes in 2.5-mg, 5-mg, and 10-mg doses, with a half-life of 3-4 hours. Due to this short half-life, patients are usually prescribed to take the medication tid (or in the morning in cases of POTS, when POTS symptoms seem most prevalent. The most common reported side effects of Midodrine to include: paraesthesia and pruritus, mainly of the scalp and goosebumps, supine and sitting hypertension, chills, urinary urge, urinary re- tention, and urinary frequency. Titration of the medication is an option, especially if patients are sensitive to the side effects. SW helps to differentiate OD from Syncope (differentiated as an SE upon standing). However, Dysautonomia (e.g. SW) does not ac- count for all causes of OD, e.g. vascular valve dysfunction not due to SW.
Tilt-table testing is currently accepted as a standard of autonomic testing, including for causes of POTS, Syncope, and LH. It can be useful for certain diagnoses, such as Cardiogenic Syncope. However, there are numerous other conditions associated with Dysautonomia for which tilt-table testing does not provide use- ful clinical information. The stand challenge, in the clinical study, is a postural change challenge equivalent to tilt-testing [5,6]. The stand challenge is a physiologic activity. It is inherently safer and more comfortable for the patient, arguably leading to more reliable results [6]. The stand challenge enables autonomic testing to be performed in smaller clinics, and has a shorter time requirement.
Beat-To-Beat Blood Pressure (bbtBP, or in more simple form, Pulse Wave Velocity) is also a standard for autonomic testing. While btbBP is simpler to implement than tilt-table, it is often used in conjunction with tilt-table and, like tilt-table results, requires macroscopic waveform assessment. Both are qualitative, subjec- tive assessments, even in the hands of experts, and once the wave- forms are no longer visible to the human eye, no further analyses are possible. Furthermore, increased Parasympathetic (or Vagal) activity improves the appearance of HRV (via improved Respira- tory Sinus Arrhythmia) or btbBP. Once the improvement appears as perfect synchrony, P-activity is normalized. However, P-activ- ity may also be excessive, with no difference in the amount of Respiratory Sinus Arrhythmia. This is the reason behind the lack of an upper bound to the normal range for HRV-based P-activity. P&S Monitoring is quantitative and objective and utilizes frequen- cy domain analyses beyond the visual range. This is a retrospec- tive, observational study. Patient testing and clinical outcomes measures were collected as an authorized part of the subject’s care and treatment given their clinical history. All data were handled according to HIPPA regulations. Data were analyzed, statistically, with SPSS v 22.0, with the null hypothesis indicating significance at p ≤ 0.050.
Results
Within this database at baseline, 1053 (38.6%) complained of LH (Table 2), 832 (79% of those with LH) were not of Vestibular etiol- ogy (they had negative Vestibular or Balance studies). At baseline, patients within the LH population were prescribed medications that are known to affect LH, including vasodilators (3.6%), min- eralocorticoids (1.4%), diuretics (11.7%), and alpha-1 adrenergic agonists (Midodrine, 3.6%). Those already on Midodrine were ti- trated higher, to tid, as needed. Most on mineralocorticoids (Flud- rocortisone) were weaned and switched to Midodrine according to the protocol. All who were prescribed diuretics and demonstrated SW were weaned to lower doses of the diuretic, if not weaned totally.
Table 2: Baseline (Test 1, or T1) and follow-up (T2 & T3) diagno- ses as percentages of the population with corresponding therapies prescribed as percentages of the population. The percent of light- headed patients (LH) is of the total population. The remaining percentages are of the T1 LH population. The p-values are from comparing Test 1 to Test 2 and Test 1 to Test 3.
|
% |
Test 1 |
Test 2 |
p |
Test 3 |
p |
|
LH |
38.6 |
23.7 |
0.0678 |
8.5 |
0.0341 |
|
HA |
37.5 |
26.9 |
0.0626 |
10.8 |
0.379 |
|
Mig |
11.3 |
10.2 |
0.0950 |
3.1 |
0.0489 |
|
HTN |
44.1 |
41.2 |
0.0923 |
26.1 |
0.0432 |
|
OH |
40.6 |
43.6 |
0.0922 |
10.9 |
0.0227 |
|
OHtn |
2.4 |
1.8 |
0.0892 |
1.8 |
0.0667 |
|
OIS |
34.5 |
35.1 |
0.0596 |
10.6 |
0.0274 |
|
POTS |
1.5 |
1.2 |
0.0815 |
1.2 |
0.0515 |
LH: lightheadedness; HA: headache; Mig: migraine; HTN: hy- pertension; OH: Orthostatic hypotension; OHtn: Orthostatic hy-pertension; OIS: Orthostatic intolerance; POTS: Postural Ortho- static Tachycardia Syndrome
Symptom Relief Takes Time
Of the LH patients, 37.5% complained of Headache, 11.3% com- plained of Migraine, and 44.1% are diagnosed with resting Hyper- tension (HTN). After introducing low dose, α-adrenergic agonist (Midodrine) therapy, there was a 38.3% decrease in the reports of LH, with a 28.3% decrease in complaints of Headache, 9.7% decrease in complaints of Migraine, 6.6% decrease in patients demonstrating resting HTN, 7.4% increase in patients demonstrat- ing OH, 25.0% decrease in patients demonstrating OHtn, 1.7% increase in patients demonstrating OIS, and a 20.0% decrease in patients demonstrating POTS. None of the changes from the base- line test (T1) to the first follow-up test (T2) are statistically insig- nificant (p>0.050).
After another (approximately) four months of low dose, α-adrener- gic agonist therapy, on average, only 8.4% of the patients (a 64.7% decrease, p=0.0341) continued to complain of LH (Table 2), with 10.8% complaining of Headache (a 59.9% decrease, p=0.0379), 3.1% complaining of Migraine (a 69.6% decrease, p=0.0489), 26.1% demonstrating resting HTN (a 36.7% decrease, p=0.0432), 10.9% demonstrating OH (a 75.0% decrease, p=0.0227), 1.8% remain with OHtn (no significant change), 10.6% demonstrating OIS (a 69.8% decrease, p=0.0274), and 1.2% remain with POTS (no significant change). The changes between first and second fol- low-up testing (T1 & T2) are significant (p<0.05), except for those patients demonstrating OHtn and POTS.
P&S Change Precedes Hemodynamic Changes
At baseline, 36.5% of the LH cohort demonstrated a resting SE, as indicated by a high Sympathovagal Balance (SB, Table 3). Of the LH patients, 58.6% demonstrated SW (with or without a de- crease in BP upon standing), 40.6% demonstrated a decrease in stand (postural change) BP as compared with rest (↓pcBP), 37.5% demonstrated both SW and ↓pcBP (both, SW specifically with a decrease in BP upon standing), 44.1% demonstrated PE, and 23.4% demonstrated both SW and PE. These patients’ baseline BP averaged 143/78 mmHg at rest and 130/73 upon standing.
Table 3: Baseline (T1) and follow-up (T2 & T3) changes in au- tonomic and hemodynamic responses resulting from changes in therapy listed in Table 1. The p-values are from comparing Test 1 to Test 2 and Test 1 to Test 3.
|
% |
Test 1 |
Test 2 |
P |
Test 3 |
p |
|
Hi SB |
36.5 |
35.6 |
0.0937 |
13.5 |
0.0461 |
|
SW |
58.6 |
36.0 |
0.0435 |
12.7 |
0.0290 |
|
↓pcBP |
40.6 |
43.6 |
0.0922 |
10.9 |
0.0227 |
|
Both |
37.5 |
27.0 |
0.0693 |
9.9 |
0.0358 |
|
PE |
44.1 |
24.2 |
0.0414 |
9.7 |
0.0310 |
|
SW+PE |
23.4 |
22.5 |
0.0986 |
9.0 |
0.0338 |
|
rBP |
143/78 |
141/77 |
0.1444 |
133/75 |
0.0243 |
|
pcBP |
130/73 |
127/75 |
0.0916 |
136/77 |
0.0456 |
Both: concurrent SW and ↓pcBP (see below, SW specifically with a decrease in BP upon standing); pcBP: blood pressure (BP) during the postural change (pc, i.e., stand) challenge (in mmHg); ↓pcBP: a decrease in BP from rest to stand (abnormal, in mmHg); PE: Parasympathetic excess (an abnormal increase in Parasympa- thetic activity from rest to a Sympathetic challenge, i.e., Valsalva or stand, in bpm2); rBP: resting BP (in mmHg); SB: Sympathova- gal Balance (the ratio of resting Sympathetic to Parasympathetic activity, unitless); SW: Sympathetic withdrawal (a decrease in Sympathetic activity from rest to stand, abnormal, in bpm2), with or without a decrease in BP upon standing.
Follow-up test results, after 4 (±0.8) months of low-dose, α-adren- ergic agonist therapy, included a 2.5% decrease in patients demon- strating high SB (Table 3), a 38.6% decrease in patients demon- strating SW (with or without a decrease in BP upon standing), a 7.4% increase in patients demonstrating ↓pcBP, a 28.0% decrease in patients demonstrating both SW and ↓pcBP (SW specifically with a decrease in BP upon standing), a 45.1% decrease in patients demonstrating PE, a 3.8% decrease in patients demonstrating both SW and PE, a 2.3% decrease in patients’ average resting BP, and a 1.4% decrease in patients’ average standing BP. Only the decreas- es in patients demonstrating SW or PE are statistically significant (p<0.05).
After another 4 (±1.1) months of low-dose, α-adrenergic agonist therapy, on average, only 13.5% of the patients (a 62.1% decrease, p=0.0461) continued to demonstrate high SB, 12.7% persist with SW (a 64.7% decrease, p=0.0290), 10.9% persist with ↓pcBP (a 75.0% decrease, p=0.0227), 9.9% persist with both SW and ↓pcBP (a 63.3% decrease, p=0.0358), 9.7% persist with PE (a 59.9% de- crease, p=0.0310), and 9.0% persist with both SW and PE (a 60.0% decrease, p=0.0338). Their resting BP averages 133/75 mmHg, a 5.7% decrease (p=0.0243), and their standing BP averages 136/77 mmHg, a 7.1% increase (p=0.0456). The changes between the first and second follow-up testing (T1 & T2) are significant (p<0.05).
Sympathetic Withdrawal Effects Resting Blood Pressure
The data in Table 4 are presented to demonstrate the association between OD and resting BP. At baseline, 11.8% of the LH subpop- ulation present with SW and elevated or high, resting BP (>140/90 mmHg). On average, they demonstrate a 1.1 bpm2 decrease in S-activity (ΔS) from rest to stand, indicating SW. Their average resting BP is 141/75 mmHg, and they demonstrate an average 4.8/5.6 mmHg decrease in BP (ΔBP) upon standing. At baseline, 12.1% of the LH subpopulation present with a drop in stand BP (↓pcBP) and elevated or high resting BP (>140/90 mmHg). On average, they demonstrate a 1.0 bpm2 increase in Sympathetic ac- tivity from rest to stand, a normal response. Their average resting BP is 126/72 mmHg, and they demonstrate an average 22.9/4.4 mmHg decrease in BP upon standing. The LH subpopulation that presents with both SW and a ↓pcBP with elevated or high resting BP (>140/90 mmHg) accounts for 6.1% of the cohort. On average, they demonstrate a 1.2 bpm2 decrease in S-activity from rest to stand (SW). Their average resting BP is 127/74 mmHg, and they demonstrate an average 6.7/3.8 mmHg ↓pcBP. Upon follow-up, after 4 (±0.8) months of low-dose, α-adrenergic agonist therapy, there is a slight (10.7%) decrease in patients demonstrating SW (with or without a ↓pcBP) with high resting BP (Table 4). On aver-age, they now demonstrate a 1.2 bpm2 increase in S-activity from rest to stand, a normalized response. Their average resting BP is down to 139/74 mmHg, and they demonstrate a more normal, av- erage change in BP (-2.9/0.9 mmHg) upon standing. The subpopu- lation of LH patients that demonstrated a ↓pcBP with high resting BP increased to 12.7%. They demonstrated a 1.1 bpm2 increase in S-activity from rest to stand, a normal response. Their average resting systolic BP is increased (128/69 mmHg), and they demon- strate an improved, but still abnormal, average ↓pcBP (-15.4/-4.0 mmHg). The subpopulation of LH patients that demonstrated both SW with a ↓pcBP with high resting BP increased to 7.3%. They demonstrated a 0.2 bpm2 decrease in S-activity from rest to stand, a normal response. Their average resting BP is decreased (124/69 mmHg), and they demonstrate an improved, but still abnormal, average ↓pcBP (-3.9/2.6 mmHg). None of these changes are statis- tically significant (p>0.050).
Table 4: Dizzy and lightheaded patients also presenting with Hypertension at baseline, with follow-up responses to therapy. The p-values are from comparing Test 1 to Test 2 and Test 1 to Test 3.
|
HTN |
SW |
↓pcBP |
Both |
|
|
T1 |
% |
11.8 |
12.1 |
6.1 |
|
ΔS |
-1.1 |
1.0 |
-1.2 |
|
|
rBP |
141/75 |
126/72 |
127/74 |
|
|
ΔBP |
-4.8/-5.6 |
-22.9/-4.4 |
-6.7/-3.8 |
|
|
T2 |
% |
10.6 |
12.7 |
7.3 |
|
ΔS |
1.2 |
1.1 |
-0.2 |
|
|
rBP |
139/74 |
128/69 |
124/69 |
|
|
ΔBP |
-2.9/0.9 |
-15.4/-4.0 |
-3.9/2.6 |
|
|
p |
0.0952 |
0.0933 |
0.1000 |
|
|
T3 |
% |
4.2 |
3.6 |
2.4 |
|
ΔS |
2.0 |
2.2 |
1.6 |
|
|
rBP |
131/72 |
122/65 |
121/63 |
|
|
ΔBP |
6.4/3.2 |
-7.5/-2.7 |
5.5/-0.1 |
|
|
p |
0.0412 |
0.0329 |
0.0375 |
|
%: percent of cohort; ΔS: change in Sympathetic activity from rest to stand (in bpm2); rBP: resting BP (in mmHg); ΔBP: change in BP from rest to stand (in mmHg). See Table 2 for more abbre- viations.
After another 4 (±1.1) months of low-dose, α-adrenergic agonist therapy, only 4.2% of the LH population persists with SW and high resting BP, a 60.4% decrease (p=0.0412, Table 4). They demon- strated a 2.0 bpm2 increase in S-activity from rest to stand, a nor- malized response. Their average resting BP is decreased (131/72 mmHg), and they demonstrate a normalized, average increase in stand BP (6.4/3.2 mmHg). Only 3.6% of the patients that demon- strated a ↓pcBP with high resting BP persisted (p=0.0329). They demonstrated a 2.2 bpm2 increase in S-activity from rest to stand, a normal response. Their average resting BP is decreased (122/65 mmHg), but they persist with a ↓pcBP (average -7.5/-2.7 mmHg).Only 2.4% of the patients that demonstrated both SW with a ↓pcBP and high resting BP persisted (p=0.0375). They demonstrated a 1.6 bpm2 increase in S-activity from rest to stand, a normalized response. Their average resting BP is decreased (121/63 mmHg), but they persist with a slightly abnormal ↓pcBP (average 5.5/- 0.1 mmHg). All of these final changes are statistically significant (p<0.05).
Parasympathetic Excess Upon Standing Masks Sympa- thetic Withdrawal
The data in Table 5 are presented to demonstrate the association between OD and PE (the abnormal P-response to an S-challenge, i.e. stand). At baseline, 16.7% of the LH subpopulation present with SW and PE. On average, they demonstrate a 10.6 bpm2 in- crease in P-activity from rest. Their average resting BP is 130/74 mmHg, and they demonstrate an average 9.4/4.2 mmHg ↓pcBP. At baseline, 22.5% of the LH subpopulation present with a drop in BP and PE. On average, they demonstrate a 12.8 bpm2 increase in P-activity from rest, an abnormal response. Their average resting BP is 133/75 mmHg, and they demonstrate an average 15.6/4.2 mmHg ↓pcBP. The LH subpopulation that presents with both SW and a drop in BP with PE accounts for 7.2% of the cohort. On av- erage, they demonstrate a 6.4 bpm2 increase in P-activity from rest. Their average resting BP is 136/77 mmHg, and they demonstrate an average 30.5/13.4 mmHg ↓pcBP.
Table 5: Dizzy and lightheaded patients also presenting with Parasympathetic excess at baseline, with follow-up responses to therapy. The p-values are from comparing Test 1 to Test 2 and Test 1 to Test 3.
|
PE |
SW |
↓pcBP |
Both |
|
|
T1 |
% |
16.7 |
22.5 |
7.2 |
|
ΔP |
10.6 |
12.8 |
6.4 |
|
|
rBP |
130/74 |
133/75 |
136/77 |
|
|
ΔBP |
-9.1/-4.2 |
-15.6/-4.2 |
-30.5/-13.4 |
|
|
T2 |
% |
10.3 |
17.3 |
5.1 |
|
ΔP |
7.5 |
12.1 |
6.0 |
|
|
rBP |
129/75 |
131/75 |
137/78 |
|
|
ΔBP |
-6.2/-4.2 |
-8.5/-1.0 |
-7.3/-1.8 |
|
|
p |
0.0502 |
0.0481 |
0.0525 |
|
|
T3 |
% |
10.0 |
15.4 |
5.0 |
|
ΔP |
-13.1 |
-13.0 |
-13.0 |
|
|
rBP |
119/72 |
127/75 |
127/77 |
|
|
ΔBP |
9.9/1.3 |
-14.5/-4.5 |
-10.8/-3.5 |
|
|
p |
0.0497 |
0.0356 |
0.0500 |
|
ΔP: change in Parasympathetic activity from rest to standing, an abnormal response (in bpm2). See Table 3 for more abbreviations.
Upon follow-up, 4 (±0.8) months of low-dose, α-adrenergic ago- nist therapy, there is a 38.3% decrease in the number of patients demonstrating SW with PE (p=0.0502, Table 5). On average, they now demonstrate a 7.5 bpm2 increase in P-activity from rest, a more normal response. Their average resting BP is down to 129/75 mmHg, and they demonstrate a less abnormal, average, change in BP (-6.2/-4.2 mmHg) upon standing, albeit still markedly abnor- mal. The subpopulation of LH patients that demonstrated a ↓pcBP with PE decreased to 17.3%, a 23.1% decrease (p=0.0481). They demonstrated a 12.1 bpm2 increase in P-activity from rest, an ab- normal response. Their average resting BP decreased to 131/75 mmHg, and they demonstrate an improved, but still abnormal, av- erage change in stand BP (-8.5/-1.0 mmHg). The subpopulation of LH patients that demonstrated both SW with a ↓pcBP with PE de- creased to 5.1%, a 29.2% decrease (p=0.0525). They demonstrated a 6.0 bpm2 increase in P-activity from rest, an abnormal response. Their average resting BP increased to 137/78 mmHg), and they demonstrate an improved, but still abnormal, average change in stand BP (-7.3/-1.8 mmHg).
After another 4 (±1.1) months of low-dose, α-adrenergic agonist therapy, 10.0% of the LH population persists with SW and PE, a 40.1% decrease (p=0.0497, Table 5). They demonstrated a 13.1 bpm2 decrease in P-activity from rest, a normalized response. Their average resting BP is decreased to 119/72 mmHg, and they demonstrate a normalized, average increase in stand BP (9.9/1.3 mmHg). Of the patients that demonstrated a ↓pcBP with PE, 15.4% persisted with PE (p=0.0356). On average, they demonstrated a 13.0 bpm2 decrease in P-activity from rest, a normalized response. Their average resting BP is decreased to 127/75 mmHg, but they persist with a ↓pcBP (average -14.5/-4.5 mmHg). Of the patients that demonstrated both SW with a ↓pcBP and PE, 5.0% persisted with PE (p=0.0500). They demonstrated a 13.0 bpm2 decrease in P-activity from rest, a normalized response. Their average resting BP is decreased to 127/77 mmHg, but they persist with an abnor- mal ↓pcBP (average -10.8/-3.5 mmHg). All of these final changes are statistically significant (p<0.050).
Secondary Symptoms Relieved
Headache and Migraine are often included with complaints of LH and reduced with a relief of LH (Table 2). Strong recommenda- tions for proper daily hydration (specifically water consumption with electrolytes) greatly facilitate the relief of both LH and Head- ache or Migraine. Relief from proper hydration helps to point to poor brain perfusion as the source of Headache or Migraine in these patients. The pharmaceutical relief of LH with Midodrine also relieves Headache or Migraine associated with LH. Elevated or high, Resting BP is often involved with LH (Table 2) and may influence the choice of therapy. However, relieving LH may also, eventually, relieve HTN associated with elevated or high, resting BP associated with LH. It has been suggested that high BP associ- ated with LH may be compensatory. High BP associated with LH may be an attempt to prevent symptoms of LH due to abnormal ↓pcBP. The proposed theory is that with resting BP (1) elevated to levels higher than required to maintain cerebral perfusion upon standing, plus (2) the amount of the abnormal decrease in stand BP response, results in (3) the sum being a BP that maintains suffi- cient brain perfusion even when ↓pcBP due to OD. These patients typically become more LH if the high BP is treated as the primary disorder (i.e., with anti-hypertensive).
There seems to be a delay in the relief of symptoms (Table 2, e.g., HTN, OH, OIS). This may be the result of a multi-step, physiolog-ic process initiated by treating the underlying P&S dysfunction: normalizing P&S activity normalizes vascular function, which then normalizes OD and resting BP responses, normalizing brain perfusion, thereby relieving Headache or Migraine (if related). By normalizing brain perfusion, symptoms of “brain fog,” fatigue, cognitive difficulties, depression, or depression-anxiety symptoms are also relieved [11]. Table 3 provides evidence of this multi-step process. Resting BP remains relatively high, as does SB (indicat- ing a resting SE), which likely underlies the high resting BP into the first follow-up (T2). Meanwhile, the α-adrenergic agonist ther- apy has more immediate effects, causing significant improvements in SW and PE (upon standing). Therefore, it seems as if the SW or PE is first normalized, then stand BP, and the resting responses (SB and BP) are normalized (see T3, Table 3). Often, PE masks SW by inflating stand S-responses in response to the stand PE. As the stand P-levels are reduced, the S-levels do not respond as much, and SW, if it existed, is unmasked.
Discussion
At baseline, patients that demonstrate PE and no evidence of SW, but with an abnormal BP or HR response to standing, tend to have their SW masked by PE (87.5%). These and the rest of the SW pa- tients that also presented with high resting BP were found to have their resting BP normalized organically shortly after the SW was normalized. This suggests that their high resting BP was compen- satory for the SW and associated lack of an increase in BP upon standing. Relieving SW eventually normalized the associated ab- normal BP and HR responses, organically. This, in turn, eventual- ly also relieved many secondary symptoms associated with poor coronary or brain perfusion, and did so organically, assuming no end-organ effects
Conclusion
Autonomic dysfunction with the postural change indicated as ab- normal P or S responses during stand are primarily associated with symptoms of LH. It may also underlie secondary symptoms such as Headache or Migraine, resting HTN, and possibly Depression and Depression-Anxiety syndromes and associated symptoms. Resting HTN seems to be a possible compensatory mechanism to counter SW, ensuring sufficient cerebral perfusion upon standing. As a result, this form of HTN may be difficult to manage, or labile, as the system attempts to defeat HTN therapy to maintain suffi- cient cerebral perfusion. Abnormal P or S responses during stand may be associated with poor cerebral perfusion due to a lack of coordination between the lower vasculature and the heart. In these cases, the lower vasculature does not properly support the heart in delivering blood to the brain. Low-dose α1 adrenergic agonist (i.e. Midodrine) seems to reverse the stand autonomic dysfunction, and (with time) relieve associated symptoms, including resting HTN, Headache or Migraine, and, perhaps, Depression and Anxiety that results from poor cerebral perfusion. P&S Monitoring provides a second measure of OD, helping to further specify OD and thereby, therapy and response to therapy. It also enables earlier detection and diagnosing of pre-clinical states that may lead to earlier inter- vention, fewer side-effects (e.g., falls and conditions secondary to falls, and brain-fog), and improved patient outcomes.
Data Availability
Data are from patient records and files and are therefore HIPAA protected. Therefore, data availability is limited. You may contact the corresponding author to request access and limited access may be granted.
References
- Italo Biaggioni, Roy Freeman, Christopher J Mathias, Phillip Low, L Arthur Hewitt, et al. (2015) Randomized withdraw- al study of patients with symptomatic neurogenic orthostatic hypotension responsive to droxidopa. Hypertension 65: 101- 107.
- Arnold AC, Raj SR (2017) Orthostatic Hypotension: A Prac- tical Approach to Investigation and Management. Can J Car- diol 33: 1725-1728.
- Vinik AI, Maser RE, Mitchell BD, Freeman R (2003) Diabetic Autonomic Neuropathy. Diabetes Care 26: 1553-1579.
- Vinik AI, Maser RE, Nakave AA (2007) Diabetic cardiovas- cular autonomic nerve dysfunction. US Endocrine Disease 2-9.
- Vinik A, Ziegler D. Diabetic cardiovascular autonomic neu- ropathy. Circulation. 2007; 115: 387-397.
- Vinik AI, Erase T (2013) Diabetic autonomic neuropathy. Handb Clin Neurol 117: 279-294.
- Colombo J, Arora RR, DePace NL, Vinik AI (2014) Clinical Autonomic Dysfunction: Measurement, Indications, Thera- pies, and Outcomes. Springer Science and Business Media.
- Bloomfield DM, Kaufman ES, Bigger JT, Fleiss J, Rolnitzky L, et al. (1997) Passive head-up tilt and actively standing up produce similar overall changes in autonomic balance. Am Heart J 134: 316-320.
- Lin YF, Wang JY, Denq JC, Lin SH (2003) Midodrine im- proves chronic hypotension in hemodialysis patients. Am J Med Sci 325: 256-261.
- Cheshire WP (2019) Chemical pharmacotherapy for the treat- ment of orthostatic hypotension. Expert Opin Pharmacother 20: 187-199.
- Colombo J, Murray GL, Pinales JM, Acosta C, Lill R, et al. (2020) Parasympathetic and sympathetic nervous system monitoring and anxiety-like symptoms: Improved differenti- ation and improved outcomes. Cardio Open 5: 19-25.