
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2019) Volume 4, Issue 1
Impact of Action II Petite Lady Laser Machine in the Treatment of Urinary Incontinence and Sexual Dysfunction in Female
Received Date: Jan 21, 2019 / Accepted Date: Jan 28, 2019 / Published Date: Feb 14, 2019
Copyright: ©Najwa Alfarra, Waleed Altaweel. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background and Aims: Urinary incontinence & sexual Dysfunction is very common among female. It causes social or hygienic problem. Urinary incontinence is the uncontrolled leakage of urine. This condition affects about a third of the female population and is more common in women than in men5. Recently the Action II Petite Lady laser has attracted attention for urinary incontinence and sexual dysfunction as non-invasive way that is aimed at awakening a woman’s sensuality by tightening up their vaginal canal. The current study evaluated the clinical efficacy of the Action II Petite lady laser on the treatment of sexual dysfunction and urinary incontinence in females.
Subjects and Methods: Thirty woman with Urinary incontinence & sexual Dysfunction, ages from 25 – 55 year were treated for four sessions two weeks apart between the first three sessions and one month apart between the third and fourth session with a 2940 nm Er: YAG via 90° and 360 scanning scopes. PFX2 assessments were performed at baseline, one –month post treatment and at 2 months’ post-treatment for vaginal muscle power. FSFI questionnaires were answered pre-post intervention, and bladder diaries were used. Subjective satisfaction was assessed about sexual satisfaction.
Results: All subjects successfully completed the study with no adverse events. Significant improvement in vaginal muscle power was seen in all subjects at 2 months’ post-procedure based on the PFX2 values, sexual satisfaction as assessed by the subjects themselves 57.7% very satisfied and 42.3% moderately satisfied. The comparison between the means of the considered parameters before and after the treatment showed a very significant difference in reducing the symptoms of stress incontinence.
Conclusions: Er: YAG laser treatment for urinary incontinence and sexual dysfunction produced significant improvement. With multicast delivered in the multiple micro pulse modes via 90 and 360scanning scopes, nonsurgical Er: YAG laser treatment was pain-free, safe, side effect free, easily tolerated and effective.
Keywords
Multishotmicropulse Mode, Vaginal Tightening, 90° Scanning Scope, Sexual Satisfaction, Collagen sis, Tissue Remodeling.
Introduction
Vaginal relaxation Syndrome (VRS) is defined as laxity of the vaginal wall. It can result in loss of friction and sexual satisfaction for both a women and her partner, often referred to as “loose vagina”. Urinary incontinence is another problem associated with VRS, either of the stress or urge type, and can be mildly irritating or totally debilitating [1]. Different types of VRS treatment options exist from noninvasive approaches to invasive surgical procedures. For the noninvasive approaches, behavioral techniques (bladder training, scheduled toilet training, pelvic floor exercises can tighten up relaxed musculature in the pelvic floor, electrical stimulation, and biofeedback). However, although these are noninvasive options, the effectiveness is somewhat limited and the latency period temporary, requiring continuous follow up. Surgical procedures, is more invasive and has a higher risk of complications such as: down time for recover, risks associated with the scar formation or nerve damage than noninvasive therapies, but it can also provide a long term solution in severe cases. The laser has recently been added to the treatment of VRS as a safe technique of treatment, because it is incision less and virtually painless with no cutting bleeding or statures. Recovery is extremely quick without need for the use of analgesics or antibiotics. Studies confirmed that Er: YAG (2940nm) is an effective safe and comfortable treatment option for symptoms relief in patient with urinary incontinence because it limits damage depth with particular wavelengths having high water absorption [2].
Identification and description of the investigational device
The Action II is a solid state Er: YAG laser emitting laser energy at the wave length of a 2940 nm at which water is the main chromospheres, with this wavelength having the highest absorption rate in water among the usual lasers used in surgery and medicine. Given the high water content of skin and soft tissue, this makes the Action II system ideal for any indication requiring ablation or vaporization of skin. The Er: YAG laser can remove skin almost cell layer by cell layer with 5-20 um precision. In addition, because its absorption rate in water limits penetration of the Er: YAG laser beam into tissue, the thermal damage in the target tissue is limited to a few um. As a result, the post-treatment repair process is much faster following ER: YAG ablation and the probability of complications (erythematic, pigmentation) is low. Precise Er: YAG laser ablation can provide excellent feathering between the treated and untreated tissue, can precisely shave areas of hyperplasic skin and help with atrophic areas promoting the synthesis of collagen in the areas around targeted skin [2].
Laser system
The laser system used was the Action II Er: YAG delivering a wavelength of a 2940 nm. When fitted with dedicated vaginal scanning scopes (Petite Lady System) the laser can be operated in the multiple micro pulse mode (pulse width of 250 us, selectable number of multiples), or in the long- pulsed mode (1000ms, single pulse). There were two scopes comprising the dedicated vaginal scanning scope system (Figure 1). One scope delivered a 360 ring – shaped beam with an approximate beam width at target of 2-3 mm (Petite 360), and the other delivered around-shaped 90 beam with an approximate beam width at target of 5 mm (Petite 90), both scopes being supported in the vagina by a specially designed guide (Figure 2). In general, for the 360 scope the supporting guide is inserted, and then the scope is fully inserted into the guide. The body of the scope is marked with 2.5 mm gradations. The laser parameters are set including the multiple pulse option, the laser is fired, the probe is withdrawn by 1 gradation (2.5 mm) marked on the probe body, and the process repeated for the entire length of the vaginal canal. Multiple passes may be made. For the 90 scope in the treatment of urinary incontinence, following insertion of the supporting cage the probe is inserted with the active part of the scope at the 12 O’clock position. The laser is fired, and the scope turned to the 2 O’clock position, fired again, then turned to the 10 O’clock position and fired again. The scope is withdrawn by 2 gradations (5 mm), return to the 12 O’clock position, and the process is repeated for the required number of passes. To treat the entire vaginal wall with the 90 scope, however, for each set of shots the active part of the scope is set at the 12 O’clock, then 2 O’clock, 4 O’clock, 6 O’clock, 8 O’clock and 10 O’clock positions, the scope is withdrawn by 2 gradations, and the process repeated [2].

Figure 1: The 360 scanning scope (left) and the 90 scanning scope (right)
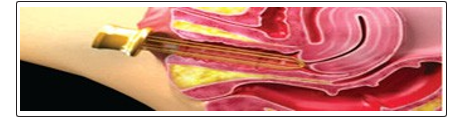
Figure 2: Illustration showing the guide for the scopes inserted in the vagina
Methods
In this prospective study, single center study, 30 patients suffering from stress urinary incontinence and sexual dysfunction underwent treatment with a 2940 nm Er: YAG Laser (Action II petite lady). A study was approved by the ethics committee of King Faisal Specialist Hospital and Research Center, Saudi Arabia.
Sample Size
The published paper by Ivan7 stated that: “The average ICIQ-UI score before the treatment was 11.3 points (p<0.05), the second measurement at 1 month was 7.4, at 3 months 7.6, and at 6 months 8.0 (p<0.05)”. We used average ICIQ-UI score before the treatment (11.3) and after treatment (8.0) for the calculation of the sample size. For type I error of 5% and power 80% and estimated standard deviation of 3.0, the calculated sample is 30 subjects.
The inclusion criteria were included married, not pregnant, without having undergone any major pelvic floor or post-delivery surgical procedure within the last 6 months to the commencement of the study. Urinary incontinence confirmed by aerodynamic, having sexual dysfunction with grade one or two cystocele/rectocele or uterus. The exclusion criteria were pregnant women. Women with neuromuscular diseases or women with prolapsed stage 111 and 1V.
At the initial consultation visit 30 patients were examined to determine their suitability according to the above inclusion and exclusion criteria. All patients submitted to treatment had passed inclusion criteria and had provided written informed consent forms. All patients testified to suffering from urinary incontinence and sexual dysfunction, and expressed their desire to improve their sign and symptoms. The patients aged were between 25-55 years old with sexual dysfunction in stress incontinence confirmed by patient history and aerodynamic study. The patients’ average body mass index was 24.15 (range 19.25-30.49) and Five subjects had given birth twice, fifteen fourth, five sixth, two seven, and three had undergone eight deliveries. Seven patients had caesarian section delivery; the rest of them had vaginal delivery. The patient’s demographics and relevant histories are given in (Figure 3).
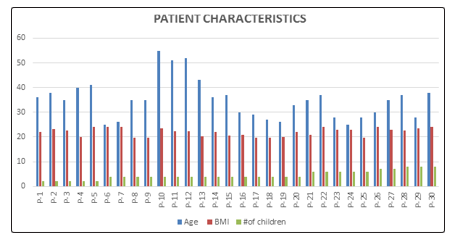
Figure 3: Patient characteristics. BMI, Body mass index
The quality of life in the area of sexuality was examined with the Female Sexual Function Index (FSFI) Arabic validate version by (Anis, et al. 2011), these questions were answered by the patient before they commence the treatment and after 10 weeks of completing the treatment.
For the measurement of vaginal muscle power, the PFX2 was used, and bladder diary. The muscle power was measured before, after one month of treatment and two months after the last session of treatment. The bladder diary was completed before, after one month of treatment and two months after the last session.
Treatment procedure
The anterior vaginal wall was treated by Er: YAG laser (2940nm) (Action II petite lady). Immediately before the laser treatment the patient’s vaginal canal was thoroughly washed and the disinfecting solution carefully dried off and removed from the mucosa. Next a specially designed laser speculum was introduced into the patient’s vagina to serve as a guide for the laser beam delivery system. Er: YAG90 scope used as multiple micro pulse mode, three multi-shot setting, pulse width of 250 and 1.7 J/shot. The three passes were delivered along the entire length of the vaginal canal in each treatment session. For each set of the shots the active part of the scope was set at the 12 O’clock the laser is fired and the scope is withdrawn by 2 graduation 5mm the process is repeated, then repeat the same process at 2 O’clock, 4 O’clock, 6 O’clock, 8 O’clock, and 10 O’clock, these positions were selected to treat the entire circumference of the vaginal wall. In session 3 and 4 an additional 2 passes /session were delivered with 360 scope in long-pulsed mode pulse width of 1000ms (1S), 3.7 J/Shot. Protocol called for four treatment sessions two weeks apart between the first three sessions and one month apart between the third and fourth session.
Results
A total of 30 patients with stress incontinence and sexual dysfunction were recruited. All 30 patients underwent the Er: YAG laser treatment. Before the treatment, FSFI and the PFX2and bladder diary were performed. At the 1-month follow up, the PFX2and bladder diary were performed with all 30 patients. A total of 30 patients underwent a 10 weeks follow up. The average treatment time was 25 minutes. The sensation of pain and discomfort was monitored during the treatment. Less than half of the patients assessed the Er: YAG laser treatment as totally painless, while the others reported very mild pain or burning sensation during the treatment. Patients returned to their routine activities immediately after treatment, and no adverse effects were reported. Patients were only requested to restrain from sexual activities for a period of 48 hours after each of the treatment sessions.
PFX2 Measurement
Reading of all subjects was compared at base line, one-month after treatment and 2 months after the final session. Improvement was seen in all PFX2 scores (Figure4). Before the intervention: seven patients had score 8, six had score 7, ten had score 5, five had score 4 and 2 had score 3. After one-month of treatment six patients had score 9, six had score 8, eleven had score 7, six had score 4, and one had score 3. Post intervention: twenty-three patients score 12, five score 10 and two score 8. (76.6% max. improved, 16 % moderately improved, 7.4% min. improved). (Figure 5).
Figure 4: PFX2 (Pelvic Floor Exercise)
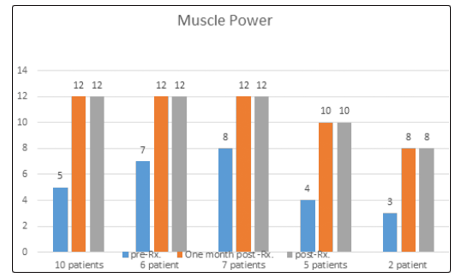
Figure 5: Vaginal muscle power at baseline as assessed by PFX, one-month post treatment and after two months of treatment
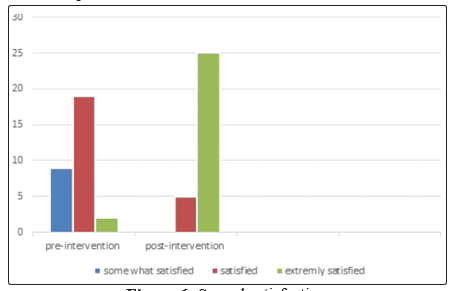
Figure 6: Sexual satisfaction
Patient sexual satisfaction was self-rated using the following scale: dissatisfied, 0; somewhat satisfied, 1; satisfied, 2; extremely satisfied, 3.
Bladder Diaries
The study was designed on the basis of three variables. The dependent variables were number of used pads, urge and urethral orifice control during coughing, sneezing, laughing, and walking. The dependent variables were measured before and after treatment (Table 1). The comparison between the means of the considered parameters before and after the treatment showed a very significant difference in reducing the symptoms. See figure 7, Table 1.
The used pads were dramatically decreased after treatment; indicate the efficacy of treatment tools on solving patient’s problem, to become dry. The high percentages of improvement indicate great changes of patient lifestyle after treatment intervention. The changes of stooping activities (cough, sneezing, laughing), physical activities (walking), and number of used pads indicate a quality of life for the patient with incontinence.
Table 1: pre and post average for all 30 patients
|
Variables |
Pre mean+/-STD |
Post mean +/- STD |
Minimum value |
Maximum value |
|
Cough |
3.4+/-5.5 |
0.1+/- 0.5 |
0 |
14 |
|
Sneezing |
1.9 +/- 4.3 |
0.0+/- 0.1 |
0 |
14 |
|
Laughing |
3.0+/-5.7 |
0.2+/- 0.6 |
0 |
14 |
|
Walking |
2.7+/-6.0 |
0.0+/- 0.1 |
0 |
21 |
|
Urge |
4.0+/- 5.6 |
0.1+/- 0.3 |
0 |
21 |
|
Pad |
12.6+/- 17.1 |
1.8 +/- 5.5 |
0 |
49 |
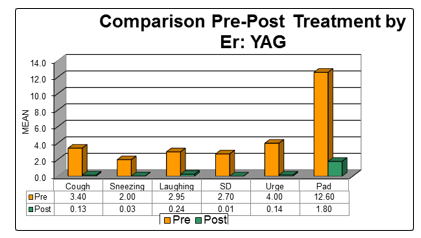
Figure 7: Evaluation parameters before and after the treatment
Questionnaire
All patients responded to the FSFI questionnaires before and after the treatment. An FSFI analysis of their sexuality showed that pre-intervention 8.3% of them had high desire for sex, 70% said it was moderate, 18.3% said it was low, and 3.3% said it was very low. Further, just 1.8% said they almost always experienced sexual arousal, 6.8% said most times, 39.6% said sometimes, 47.5%said a few times while 4.3% said almost never. Looking at the other responses based on the FSFI, the results showed 4.3% of women experiencing lubrication problem (they found it extremely difficult to lubricate during sexual activity), 37.5% of the women can sometimes lubricate during sexual intercourse, 35.8% of the women were able to maintain their wetness during sexual intercourse to the end just a few times, 1.6% found it very difficult to maintain wetness during sexual activity until the end, while 20.8% found it not difficult to maintain wetness during sexual intercourse until the end. The ability to achieve orgasm was also affected; 35.5% were able to reach orgasm sometimes during intercourse, 11.1% most of the times, while 36.6% they found it slightly difficult, 3.5% found it difficult, and 13.3% never reach orgasm during sexual activity. Overall sexual satisfaction was also affected with 34.5 % of the women finding their sexual relationship either moderately satisfied or 45.6% equal dissatisfied with satisfied. 20% of the women experiencing pain during sexual intercourse at the time of penetration, 46.6% experiencing moderate pain at the end of intercourse, and 21.1% experiencing quite a bit of pain at the beginning.
Post-intervention analysis showed that 86.6% of the women had a high to very high desire for sex, 10% said sometimes, and 3.4% had said few times. Furthermore, 69.1% said they almost always experienced sexual arousal, 29.1% said sometimes, and 1.6% said few times. Regarding lubrication during the intercourse, the result showed 78.3% of the women were able to maintain their witness during sexual activity until the end without difficulty, 7.5%of the women can sometimes lubricate during sexual intercourse, 8.3% said few times, and 2.5% said very difficult. The ability to achieve orgasm was improved; 82.2% were able to reach orgasm almost always during intercourse, 11.1% said sometimes, and 6.6% found it difficult. Overall sexual satisfaction was also improved 57.7% of the women finding their sexual relationship very satisfied, while 42.3% of them find it moderately satisfied. 32.2% of women had no pain with intercourse, while 65.3% of them had few times pain after the intercourse, 2.5% of them had pain most of the times.
Discussion
The patient with stress incontinence and sexual dysfunction the initial management involves a variety of noninvasive interventions, including behavioral therapy, electrical stimulation, and pelvic floor muscle exercises (PFMEs). These therapies do require patient’s motivation and time commitment. There have been several trials that demonstrate improvement and satisfactory cure rated in patients adhering to a strict program of behavior modification and pelvic floor muscle tones. Patient compliance and motivation, however, are essential to successful results [3]. The questionnaire responses showed that women are unlikely to carry out regular pelvic floor exercises except for a short time after childbirth or when prompted by urinary symptoms [4].
Various surgical techniques are still the mainstream of vaginal repairs. “There are quite some articles describing various techniques of vaginal repair [5, 6]. Claiming good results and low levels of complications. Prado et al. reported satisfactory improvement of sexual satisfaction in 74% of patients submitted to surgical narrowing of pelvic floor muscle weakness, similarly Moore &Milks further confirmed on the positive impact of prolapsed repair on sexual satisfaction [7, 8]. However, all of these surgical therapies are associated with risks of serious adverse effects and require relatively long recovery periods, side effect of anesthesia and restraining from sexual activities during this period. For example, in Prado’s paper, patients were requested to restrain from sexual activities for a period of six weeks after the surgery [7].
There have been several trials to design a new procedure that would overcome the side effects of surgical repair and at the same time improve the vaginal relaxation but with no adverse effects and with a short period of recovery time. Among several invasive procedures, we found the Er: YAG laser (2940nm) (Action II petite lady) treatment to be much safer technique, which attract our attention and we decided to do the prospective study with the aim to evaluate its efficacy and safety on urinary incontinence patients with sexual dysfunction, because it does not have any adverse effects, minimal discomfort, return to normal sexual activities within 48 hours after the treatment compared to any other of surgical procedures. In a paper describing another minimally invasive laser therapy for vaginal tightening treatment performed with a fractional ablative CO2 laser, Gasper et al reported several cases of bleeding, pain and burning [9]. Also according to their method description (3 sessions, 60 days apart) one can conclude that quite a long time had to pass before patients’ could return to normal sexual activity.
As already mentioned, Prado et al also reported 6 weeks of restraining from sexual activities as well as two minor surgical complications [7]. For pain management they used spinal or general anesthesia. Common occurrences in surgical treatment for vaginal relaxation syndrome are anesthesia side effect, dyspareunia, wound infection, post-op suture adhesions, or bleeding. By using a non-surgical approach, such as the Er: YAG laser (2940nm) (Action II petite lady) treatment will avoid all of these unusual side effects.
We found the Er: YAG laser (2940nm) (Action II petite lady) treatment quick and easy to perform in ambulatory care clinic. The duration that required completing the laser treatment session will be from 25-30 minutes. We are aware that this prospective study has several shortcomings include the relatively small size of the study group, the lack of a control group, and the short follow up time. However, we believe that the results will be obtained from this study will be confirmed in further studies that will follow shortly.
Conclusion
The prospective study about the impact of action petite lady (Er: YAG laser) treatment showed that an excellent efficacy in improvement of vaginal tightness with minimal patient discomfort during the treatment sessions and no adverse effects. Further prospective studies are in preparation, which would include the use of additional assessment tools like a perineometer and some additional validated questionnaires. Also longer period of follow ups up to 30 months are planned [10-13].
References
- Davila G. W (2011) Nonsurgical outpatient therapies for the management of female stress urinary incontinence: long-term effectiveness and durability. Advanced Uro 2011: 1-14.
- Lee S (2014) Treatment of Vaginal Relaxation Syndrome with an Erbium: YAG Laser Using 90 and 360 Scanning scopes: Pilot Study& Short –term results. Laser Ther 23: 129-138.
- Rovner ES, Wein AJ (2004) Treatment options for stress urinary incontinence. Reviews in urology 6: S29-47.
- Isherwood PJ, Rane A (2000) Comparative assessment of pelvic floor strengthening using a perineometer and digital examination. BJOG: an international journal of obstetrics and gynaecology 8: 1007-1011.
- Liu S, Cen Y, Liu Q (2009) Improvement of vaginal relaxation by vaginal narrowing technique with double suturing, Ch.J. ReparReconstr.Surg, 23:1456-1458.
- Li PC, Zhao MX, Duan CW, Chen B, Li Q, (2011) A modified method to treat vaginal relaxation, Ch.J. Aesth. Med 16.
- Pardo JS, Sola DV, Ricci PA, Guiloff EF, FreundlichOK (2006) Colpoperineoplasty in women with a sensation of a wide vagina, Acta Obstetric et Gynecology 85: 1125-1127.
- Moore RD, Miklos JR (2010) Vginal Rejuvenation and Cosmetic vaginal surgery , textbook of female urology and urogynecology,. edition, informa healthcare. 3rd Chapter 104: 1056-1074.
- Gaspar, A, Addamo. G, Brandi. H (2011) Vaginal fractional CO2 laser: a minimally invasive option for vaginal rejuvenation. Amer. J. of Cos. Surg 28: 156-62.
- Anis T, Gheit SA, Saied HS, Alkherbas SA (2011) Arabic translation of female sexual dysfunction index validation in an Egyption population. J. sex Med 8: 3370-3378.
- Christopher J. K, Paul D. P (2014) Incontinence is treatable — even curable — for both men and women.
- Cresswell. T (2004) Place: a short introduction. BlackwellPublishing Ltd.
- Ivan Fistonic, GuštekŠtefica, Fistonic (2012) Nikola Minimally invasive laser procedure for early stages of stress urinary incontinence (SUI). J. of the Laser and Health Academy 2012:67-74.