
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Case Report - (2021) Volume 6, Issue 4
Idiopathic Intracranial Hypertension: Description of an Atypical Case
2SC Anestesia e Rianimazione Ospedale San Paolo Savona, Italy
3SC Malattie Infettive Ospedale San Paolo Savona, Italy
4SC Oculistica San Paolo Savona, Italy
5SC Radiologia diagnostica San Paolo Savona, Italy
Received Date: Nov 06, 2021 / Accepted Date: Nov 12, 2021 / Published Date: Nov 19, 2021
Copyright: ©Siri Laura, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Siri Laura, Gaiero Alberto, Maritano Lorenza, Vaira Massimo, Anselmo Marco, Polvicino Mario, Calia Stefano, Gaggero Roberto, Cohen Amnon. (2021). Idiopathic Intracranial Hypertension: Description of an Atypical Case. Int J Women's Health Care, 6(4): 232-235.
Abstract
Background: When dealing with severe and worsening headache with oculomotor dysfunction, it is necessary to take into account the possibility of idiopathic intracranial hypertension (IHH), though it is a rare condition. We present an atypical case of IHH in a 4-year-old patient with no apparent risk factors.
Methods: IHH was diagnosed by exclusion, by ocular fundus examination, liquor cerebrospinalis examination, anatomical cerebral magnetic resonance imaging (MRI) and MR angiography (MRA). At the onset of symptoms, the patient was treated with a diuretic and steroid therapy.
Results: After one year of medical therapy, we observed headache recurrence with positive ophalmological assessment and positive cerebral MRI. Medical treatment was deemed ineffective and it was necessary for the patient to undergo surgical intervention.
Conclusion: We report a case of severe and chronic headache with oculomotor dysfunction in a young, pre-adolescent patient. This case is atypical because of the young age of the patient, and it being refractory to medical therapy. This case confirms that when dealing with severe headache in young patients, it is necessary to take into account any rare cause of symptomatic headache.
Keywords
idiopathic intracranial hypertension, headache, papilledema, acetazolamide, steroids, ventriculoperitoneal shunt
Introduction
Headache is a frequent reason-consulting physician in pediatric patients. Headaches appear in about 37-51% of patients young-er than 7 years and about 57-82% of patients under 15. Chron-ic headaches are more infrequent, with 2.5% of kids under 7 and 15% of teenagers under 15 suffering from this ailment. Most of these cases are either idiopathic headaches, mainly migraines, with respect to tension-type headaches. However, when dealing with chronic headaches it is necessary to exclude any secondary causes of headache by detailed diagnostic exams, since the treatment may significantly differ.
Case Study
D. (a 4-year-old child) was admitted to our Hospital Emergency Room with a chronic daily headache. His clinical and family his¬tory was negative for any neurological diseases. His cognitive and motor development was normal and regular. His mother report¬ed that D. suddenly showed a monolateral exotropia affecting the right eye; this problem disappeared after a couple of hours. In the same week D. presented with a severe headache, whose intensity decreased after the administration of analgesic drugs. In the fol¬lowing days the headache occurred several times, accompanied by Chronic headaches are more infrequent, with vomiting, tiredness, sleepiness, and both apathy and nervousness. D. was admitted again to the Emergency Room for another visit. His vital signs were normal but the child appeared suffering and soporose. Phys¬ical neurological examination was within normal limits and the patient was afebrile. A clinical examination of the motor and sen- sory system was normal. Tone, power and reflexes in all four limbs were also normal; there was no neck stiffness and Kerning’s sign was negative. Coordination was normal, the sensory system and the cranial nerves were normal too. No significant findings were revealed in further systemic examinations. Fundoscopy revealed bilateral papilledema. Routine full blood count and biochemistry did not show any abnormality.
Enzyme-linked immunosorbent assay (ELISA) of the patient’s se-rum was negative for Herpes Simplex virus (HSV), Citomegalo-virus (CMV), Epstein-Barr virus (EBV) and toxoplasma. A brain computed tomography (CT) scan was performed and was normal. Cerebrospinal fluid chemistries and cytology were normal as well. However, an increase in liquor pressure was found. Brain magnetic resonance imaging (MRI) revealed an arachnoidal space of optical nerve dilation (Fig.1). The electroencephalogram (EEG) revealed slow posterior bilateral waves without paroxysmal signs (Fig.2).
<img src="https://www.opastpublishers.com/scholarly-images/1867-69d87b3ae5185-idiopathic-intracranial-hypertension-description-of-an-atypi.png" width="400" height="200">
Figure 1: Brain MRI: bilateral distention of the perioptic sub-arachnoid spaces
<img src="https://www.opastpublishers.com/scholarly-images/1867-69d87b6b7aa78-idiopathic-intracranial-hypertension-description-of-an-atypi.png" width="400" height="200">
Figure 2: Electroencephalogram: bilateral posterior slow wave complexes
With these tests, we excluded venous sinus thrombosis, and made presumptive diagnosis of idiopathic intracranial hypertension based on opthalmologycal and MRI findings. Treatment with acetazolamide 20mg/Kg/daily was initiated without any side effects. However, on the 6th day after treatment initiation, headache and papilledema had not resolved. Therefore, we complemented the treatment with intravenous hydrocortisone 1 mg/kg/daily followed by oral prednisolone. In the following days, D. did not present headache; ophthalmoscopic examination showed a slight swell¬ing of the right disc but visual acuity and visual evoked potentials (VEP) were normal. After D. was discharged from the hospital, this therapeutic regimen was continued for 3 months. After stopping the administration of acetazolamide and prednisolone, D. accused headache and photophobia, while a new neurophtalmological as¬sessment and EEG were both negative. The headache decreased again after the administration of analgesic therapy. 12 months later the patient was re-admitted to the hospital with headache, nausea, and vomiting. A neurophalmological assessment revealed bilater¬al optic disc edema. MRI revealed minimal arachnoidal space of optical nerve dilation. Diuretic therapy and high doses of steroids were ineffective. After 2 months of medical treatment, the patient developed glucose intolerance. Some improvement was observed after repeated lumbar puncture. Since the patient was refractory to medical therapy, it was finally decided to perform surgical treat¬ment in the form of a ventricular-peritoneal shunt. This treatment effectively resolved the symptoms.
Discussion
Idiopathic Intracranial Hypertension (IIH) is a term commonly used to describe the association of intracranial pressure without clinical laboratory or radiological evidence of an intracranial, space-occupying lesion. The incidence of IIH is variable and it ranges from 0.57 to 2/100.000 in the general population. IHH is a rare entity in pediatric patients.
Known as benign intracranial hypertension or pseudotumor cere¬bri, IIH is a diagnosis of exclusion made in the presence of pap¬illedema, normal neuroimaging and cerebrospinal fluid analysis, but with an elevated cerebrospinal fluid pressure. The diagnosis of IIH is suspected based on the patient’s and family history, and the clinical examination. To correctly diagnose IIH it is necessary to perform neurologic examination, ophthalmoscopy, visual field assessment, ocular motility examination and brain MRI with ve-nography.
Previously, the modified Dandy criteria were used for this diagno¬sis in both adults and children (Tab 1). However, Raangwala and Liu proposed new criteria to aid diagnosing for pseudotumor cere¬bri in prepuberal children, as presentation in this population can be quite different compared to adolescents and adults.
Tab 1- IIH Diagnostic criteria – Modified Dandy criteria
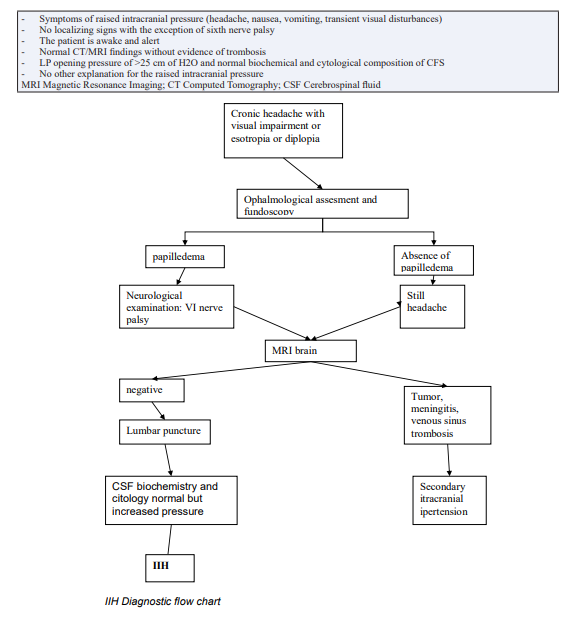
The pathophysiology of IIH is not clear: there are many hypothe¬ses on the development of this condition, including alterations in liquor absorption and production, cerebral edema, abnormalities in cerebral vasomotor control and cerebral blood flow, and venus obstruction. Risk factors for the development of IHH are obesi¬ty, adolescent age, and female sex, intake of high dose Vitamin A derivatives (e.g. isotretinoin for acne), long-term tetracicline use, steroid and hormonal contraceptives.
The most common presenting symptom is a severe headache, worsening in the morning and being exacerbated by the Valsal-va maneuver. The other manifestations are: exotropia, horizontal diplopia, caused by cranial nerve VI palsy, decreased visual acuity or blurring central vision caused by papilledema, nausea and vom¬iting. The most significant physical finding of IIH is bilateral disc edema secondary to the increased ICP.
The pseudotumor cerebri is usually a self-limited condition but a delay in treatment can lead to optic atrophy and blindness. Medical treatment with acetazolamide in association with corticosteroids has been applied with success. It is rarely necessary to perform serial lumbar punctures, lumboperitoneal or ventriculoperitoneal shunt, subtemporal decompression or optic nerve sheath fenestra-tion.
Conclusion
In conclusion, our case can be considered atypical as it involved a young child without any risk factors for IHH. This demonstrates that when presented with a case of severe and recurring headache, even in children, it is necessary to follow an accurate diagnostic protocol, in order to exclude any cerebral tumors, encephalithis, hydrocephalus and venous sinus trombosis. The diagnosis in¬volves several professionals: the neuropediatrician, ophtalomolo-gist and neuroradiologist. Regarding the therapy, our patient re¬quired a combined regimen with acetazolamide and steroids. Once we suspended the treatment with steroids, the headache recurred, without any other associated symptoms. A relapse was confirmed and steroids were not prescribed again.
After 12 months, the patient presented again with episodes of se¬vere headache with ophtalmoscopy and neuroimaging positive for IIH. Since in this case medical therapy was ineffective in the first place, surgical treatment was deemed necessary. The long-term follow-up confirmed that the correct therapeutic approach includ¬ed surgical treatment, leading to a complete recovery as well as a prevention from severe and permanent complications such as pro¬gressive blindness from postpapilledema and optic atrophy [1-10].
References
- The International Classification of Headache Disorders, 2nd edition (2004) Cephalalgia 24: 9-160.
- Skau M, Brennum J, Gjerris F, Jensen R (2006) what is new about idiopathic intracranial hypertension? An updated review of mechanism and treatment. Cephalalgia 26: 384-399.
- Thurtell MJ, Wall M (2013) Idiopathic intracranial hypertension (pseudotumor cerebri): recognition, treatment, and ongoing management. Curr Treat Options Neurol 15: 1-12.
- Binder DK, Horton JC, Lawton MT, et al. (2004) Ideopathic intracranial hypertension. Neurosurgery 54: 538-552.
- Lee A, Wall M (2010) Idiopathic intracranial hypertension (pseudotumor cerebri): epidemiology and pathogenesis.
- Algahtani HA, Baeesa SS, Obeid TH, Abuzinadah AR (2007) Idiopathic intracranial hypertension. Atypical presentation. Saudi Medical Journal 28: 762-765.
- Lee A, Wall M (2010) Idiopathic intracranial hypertension (pseudotumor cerebri): prognosis and treatment.
- Silberstein SD, McKinstry RC (2003) The death of idiopathic intracranial hypertension? Neurology 60: 1406-1407.
- Skau M, Brennum J, Gjerris F, Jensen R (2006) What is new about idiopathic intracranial hypertension? An updated review of mechanism and treatment. Cephalalgia 26: 384-399.
- Friedman DI, Jacobson DM (2004) Idiopathic intracranial hypertension. J Neuroophthalmol 24: 138-145.