
International Journal of Health Policy Planning(IJHPP)
ISSN: 2833-9320 | DOI: 10.33140/IJHPP
Impact Factor: 1.08



Case Report - (2026) Volume 5, Issue 1
Hydrocele of Canal of Nuck in Adult Females – A Series of Three Cases
2Director and HOD Radiology, Eternal Hospital, India
3Attending Consultant, General and Laparoscopic Surgery, Eternal Hospital, India
Received Date: Mar 02, 2026 / Accepted Date: Mar 27, 2026 / Published Date: Apr 06, 2026
Copyright: ©2026 Devi Shanker Malik, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Malik, D. S., Singh, M., Dhakad, B. S. (2026). Hydrocele of Canal of Nuck in Adult Females
Abstract
Hydrocele of the canal of Nuck in adult females is exceptionally rare. The canal of Nuck is the portion of the processus vaginalis in the inguinal canal in women. This is homologous to the processus vaginalis of male anatomy. Although the canal of Nuck normally disappears completely in the first year of life, if it remains patent, then it can lead to the development of an indirect inguinal hernia or hydrocele of the canal of Nuck. Ultrasonography is the preferred investigation. Magnetic Resonance Imaging (MRI) is done to confirm the diagnosis preoperatively. The treatment remains the excision of the hydrocele of the canal of Nuck. We are presenting three cases of hydrocele of the canal of Nuck in adult females, one Bilateral and two unilateral, which were treated by laparoscopic/open excision of the hydrocele with mesh repair.
Keywords
Hydrocele of Canal of Nuck, Patent Processus Vaginalis, Canal of Nuck, Female Hydrocele
Introduction
The canal of Nuck was first described by the Dutch anatomist Anton Nuck in 1691. The hydrocele of the canal of Nuck, also called the female hydrocele, is a very rare condition. Canal of Nuck is homologous to a patent processus vaginalis in males, which also predisposes to indirect inguinal hernia and hydrocele of the spermatic cord. Thus, a hydrocele of the canal of Nuck in females is equivalent to an encysted hydrocele of the cord in males [1]. The canal of Nuck is normally obliterated in the first year of life, but failure to achieve complete obliteration results in an indirect inguinal hernia or hydrocele of the canal of Nuck. The fluid in the hydrocele of the canal of Nuck is likely due to an imbalance of the secretion and absorption of the secretory membrane lining the processus vaginalis. Usually, it is idiopathic, but sometimes trauma or infection may cause disruption of lymphatic drainage, which may lead to imbalance.
Case Report
Case 1
A 45-year-old lady presented in the OPD with swelling in the bilateral inguino-labial region for the last three months. There was no history of Diabetes, hypertension, any cardiac ailment, urinary tract infection, trauma, or any infection in this region. On examination, the swellings were globular, cystic in consistency, not tender, about 4x2 cm on the left side and 3x2 cm on the right side. Her USG showed lobulated, thick-walled cystic lesions showing internal echoes, in bilateral inguinal regions measuring approximately 20x28mm on the left side and 18x34mm on the right side. Lymphangioma / Round Ligament Cyst.

Figure 1: MRI of Case 1 Showing Bilateral Hydrocele of Canal of Nuck
MRI showed lobulated tubular fluid signal intensity lesions in the left pelvic inguinolabial and right inguinolabial regions extending along the round ligaments, suggestive of hydrocele of canal of Nuck / Mesothelial cysts of the round ligament.

Laparoscopic excision of hydrocele of canal of Nuck on both sides with transabdominal preperitoneal repair was done.
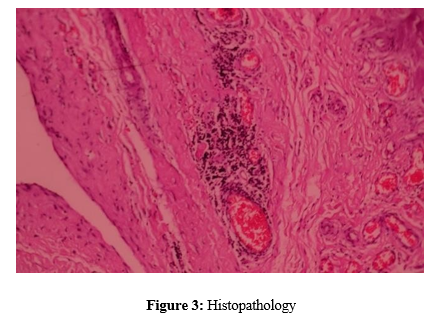
Her histopathological report revealed loose connective tissue with mesothelial lining with mild chronic inflammatory infiltrate, congestion of blood vessels, and fibrosis suggestive of Bilateral hydrocele of the canal of Nuck.
Case 2
A 35-year-old lady presented in OPD with swelling in the left inguinal region for the last 4-5 months. Earlier 2ml fluid was aspirated from it for FNAC. There is no history of DM, HT, or any cardiac ailment. She is a known case of Hyperthyroidism. On examination, it was a diffuse (not very prominent because its size had reduced after aspiration) cystic swelling in the left inguino- labial region. USG showed left sided inguinal cystic mass of 1.6x0.8cm in size with clear fluid inside and no communication with the peritoneum. There was no change with the Valsalva maneuver. Most likely Hydrocele of the canal of Nuck. FNAC shows average cellular smear predominantly acellular necrotic material along with cyst macrophages and inflammatory cells-suggestive of cystic nature of swelling.

Figure 4: MRI of Case 2nd Showing Left Sided Hydrocele of Canal of Nuck
MRI Pelvis showed fluid in the inguinal canal from deep to superficial inguinal ring-possibility of Hydrocele of canal of Nuck

Figure 5: Operative Photograph
Laparoscopic excision of Hydrocele of canal of Nuck, along with mesh repair, was done.
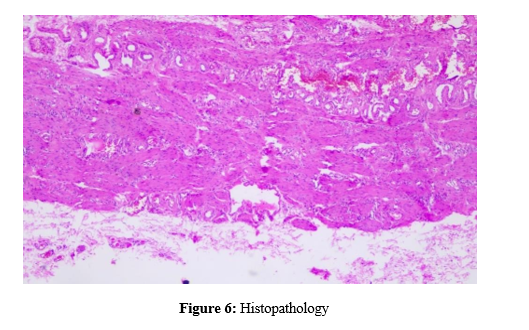
Histopathology showed loose connective tissue with congested blood vessels and a denuded, ill-defined mesothelial lining. Focal mild chronic infiltrate, fibrosis and edema suggestive of Hydrocele of canal of Nuck.
Case 3
A 41-year-old lady presented in OPD with painless swelling Right Inguino-labial region for the last one year. There is no history of DM, HT, any cardiac ailment, UTI, trauma, or any infection in this region. On examination, it was a diffuse, Globular, cystic swelling about 4x2cm in size in the right inguino-labial region. It was not tender. Signs of inflammation were absent. Lymph nodal examination was normal.

Figure 7: Ultrasonography of Case 3 Showing Right Sided Hydrocele of Canal of Nuck
USG showed evidence of Right Inguinal / Canal of Nuck Hernia containing fluid/cystic area and septation, increased during standing and Valsalva, suggestive of Hydrocele of Canal of Nuck. MRI was not done because the patient was claustrophobic and refused an MRI.
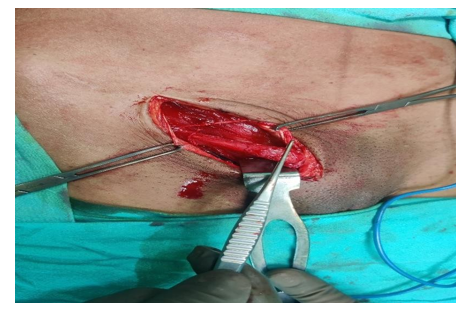

Figure 8: Operative Photograph
Open surgical excision of Hydrocele of canal of Nuck along with round ligament done. Mesh repair was done with soft prolene mesh
Histopathology showed evidence of fibroconnective tissue cyst wall lined by mesothelial cells, accompanied by inflammation and congested blood vessels, suggestive of Hydrocele of canal of Nuck.
Discussion
The canal of Nuck was first described by a Dutch Anatomist Anton Nuck in 1691. The processus vaginalis in females is known as canal of Nuck. The homologous structure in men is called the Processus vaginalis [2]. Hydrocele of canal of Nuck should always be considered in the differential diagnosis of inguinal swelling in females, along with hernia, lymphadenopathy, abscess, cyst, tumors like Lipoma, Liposarcoma, neurofibroma sarcoma, hematoma [3]. Hydrocele of canal of Nuck is usually painless, but sometimes symptoms can be acute or chronic, and infection of the hydrocele is also possible [4]. Normally, in humans, the canal of Nuck (Processus Vaginalis) completely disappears. If the Processus Vaginalis does not close, it is referred to as a Patent Processus Vaginalis (PPV). If the PPV is small and only allows fluid to pass, the condition will lead to peritoneal fluid accumulation or a (communicating) hydrocele. If the PPV is larger and allows abdominal organs to protrude, the condition is referred to as a hernia [4].
Incomplete closure of the canal of Nuck leads to the formation of a hydrocele of canal of Nuck [4]. The wall of the canal of Nuck is divided into two layers. The outer wall consists of a fibrous form of various thicknesses, including smooth muscle fibers. The inner wall consists of single-layered mesothelial cells and is a secreted layer. When the secretion and absorption of fluid become unbalanced in the secretory membrane lining the inner wall of the processus vaginalis, hydrocele of the canal of Nuck develops due to swelling of the pouch because of the collection of fluid. The hypersecretion and malabsorption of the secretory membrane can be caused by infection, injury, or inappropriate lymphatic drainage.
Imaging
The lesion might appear hypoechoic or demonstrate low-level echoes due to high protein content. When complications of the hydrocele, such as infection or haemorrhage occurs, the lesion probably shows a complex appearance with echogenic content such as a thickened wall or internal septation
USG
Ultrasound is the preferred investigation. The lesion is typically seen as a well-defined hypoechoic or anechoic mass lying superficially and medial to the pubic bone in the inguinal canal [5]. It may show cystic in appearance or with septations within the lesion
MRI
When ultrasonography is inconclusive, an MRI is used to obtain additional information about the herniated structures [1]. There is no radiation associated with this imaging modality. Its larger field of view enables a more precise anatomical relationship between the pathology in the canal of Nuck and intra-peritoneal structures. The canal of Nuck hydrocele is often hypointense on T1-weighted imaging and hyperintense on T2-weighted images. Faint internal septation can be found if there is a coexistence of an infectious or inflammatory process [1]. An MRI can also help distinguish pathologies of the canal of Nuck from other soft tissue tumours that can present as a palpable inguinal mass. However, patients need to stay still for the long scanning time, which is difficult in the case of paediatric patients.
CT Scan
A CT scan is not the first imaging modality to choose when accessing groin mass due to its radiation. However, due to its short scanning time, high availability, and the possibility of an uncertain diagnosis of inguinal hernia and other groin masses, a CT scan is commonly performed in an adult population. Another circumstance is when a patient presents with nonspecific abdominal pain at the emergency department, a CT scan would be requested to evaluate the cause of the abdominal pain, and the pathology of the canal of Nuck would be an incidental finding
Classification
Hydrocele of Canal of Nuck can be classified into three types [6].
• Type 1: There is no communication between the hydrocele and the peritoneal cavity. It mostly appears as an encysted mass without a hernia defect in children. Examples for this type are the intra-abdominal protruding forms. In adults, we assume the fascia transversalis, along with the ligamentum rotundum, is thinned out because of the hydrocele, mimicking a direct hernia [6].
• Type 2: The hydrocele communicates with the peritoneal cavity, thus mostly resulting in an indirect hernia [6].
• Type 3: The combined type has an encysted part that does not communicate with the peritoneal cavity and another that does. Its appearance resembles an hourglass and commonly causes a hernia.
• Treatment: The hydrocelectomy with mesh repair is the treatment of choice, which can be open or Laparoscopic [7].
Declarations
Authors' Contribution: Devi Shanker Malik (First author) is the main author and the corresponding author Mahipal Singh (Second author) has helped in the diagnosis of the case and B S Dhakad (Third author) has helped in the surgery and clinical follow-up of the case
Ethics Approval: Proper approval has been taken from the Ethical Committee of the hospital
Consent for publication: Written consent has been taken from the patient for publication
References
- Anderson, C. C., & Broadie, T. A. (1995). Hydrocele of the canal of Nuck: ultrasound appearance. American Surgeon, 61(11).
- Rees, M. A., Squires, J. E., Tadros, S., & Squires, J. H. (2017). Canal of Nuck hernia: a multimodality imaging review. Pediatric radiology, 47(8), 893-898.
- Fikatas, P., Megas, I. F., Mantouvalou, K., Alkatout, I., Chopra,S. S., Biebl, M., ... & Raakow, J. (2020). Hydroceles of the canal of Nuck in adults—diagnostic, treatment and results of a rare condition in females. Journal of Clinical Medicine, 9(12), 4026.
- Sarkar, S., Panja, S., & Kumar, S. (2016). Hydrocele of the canal of Nuck (female hydrocele): a rare differential for inguino-labial swelling. Journal of clinical and diagnostic research: JCDR, 10(2), PD21.
- Thomas, A. K., Thomas, R. L., & Thomas, B. (2020). Canal of Nuck abnormalities. Journal of Ultrasound in Medicine, 39(2), 385-395.
- Counseller, V. S., & Black, B. M. (1941). Hydrocele of the canal of Nuck: report of seventeen cases. Annals of surgery, 113(4), 625-630.
- Lee, S. R. (2018). Laparoscopic treatment of hydrocele of the canal of Nuck in pediatric patients. European Journal of Pediatric Surgery, 28(04), 378-382.